
Abstract
The role of the environment in harboring and transmitting multidrug-resistant organisms has become clearer due to a series of publications linking environmental contamination with increased risk of hospital-associated infections. The incidence of antimicrobial resistance is also increasing, leading to higher morbidity and mortality associated with hospital-associated infections. The purpose of this review is to evaluate the evidence supporting the existing methods of environmental control of organisms: environmental disinfection, contact precautions, and hand hygiene. These methods have been routinely employed, but transmission of multidrug-resistant organisms continues to occur in healthcare facilities throughout the country and worldwide. Several new technologies have entered the healthcare market that have the potential to close this gap and enhance the containment of multidrug-resistant organisms: improved chemical disinfection, environmental monitoring, molecular epidemiology, self-cleaning surfaces, and automated disinfection systems. A review of the existing literature regarding these interventions is provided. Overall, the role of the environment is still underestimated and new techniques may be required to mitigate the role that environmental transmission plays in acquisition of multidrug-resistant organisms.
The patient environment in healthcare settings has continually proven to harbor a reservoir of potentially harmful, and even lethal multidrug-resistant organisms (MDROs). Increased interest in the prevention of hospital-acquired infections has led to a renewed interest in tackling this growing problem for three primary reasons: a number of studies have been published not only describing the contamination of patient environments, but also linking that contamination to an increase in the risk of healthcare-associated infections (HAIs) [Fisher et al. 2012; Weinstein, 1991; Carling and Huang, 2013; Otter et al. 2013]; pathogens associated with HAIs are causing increases in mortality and morbidity due to antimicrobial resistance [Harris, 2008]; and changes in reimbursement for HAIs have caused healthcare facilities to explore environmental interventions for the reduction of HAIs [McGlone et al. 2012; Stone et al. 2010].
In this review, we summarize the data linking contamination in the environment to an increased risk of HAIs, the issues in current practices addressing the environment and the spread of MDROs, and finally, we examine emerging technologies that address enhanced environmental cleaning and outcomes. It is not meant to be a comprehensive review, but rather to shed some light on the breadth of complexity when considering the role of the environment in the spread and control of MDROs and the issues with current practices.
The link between the environment and the risk of HAIs
Survival in the environment
Summary of survival time versus prior room occupancy risk for healthcare-associated infections.
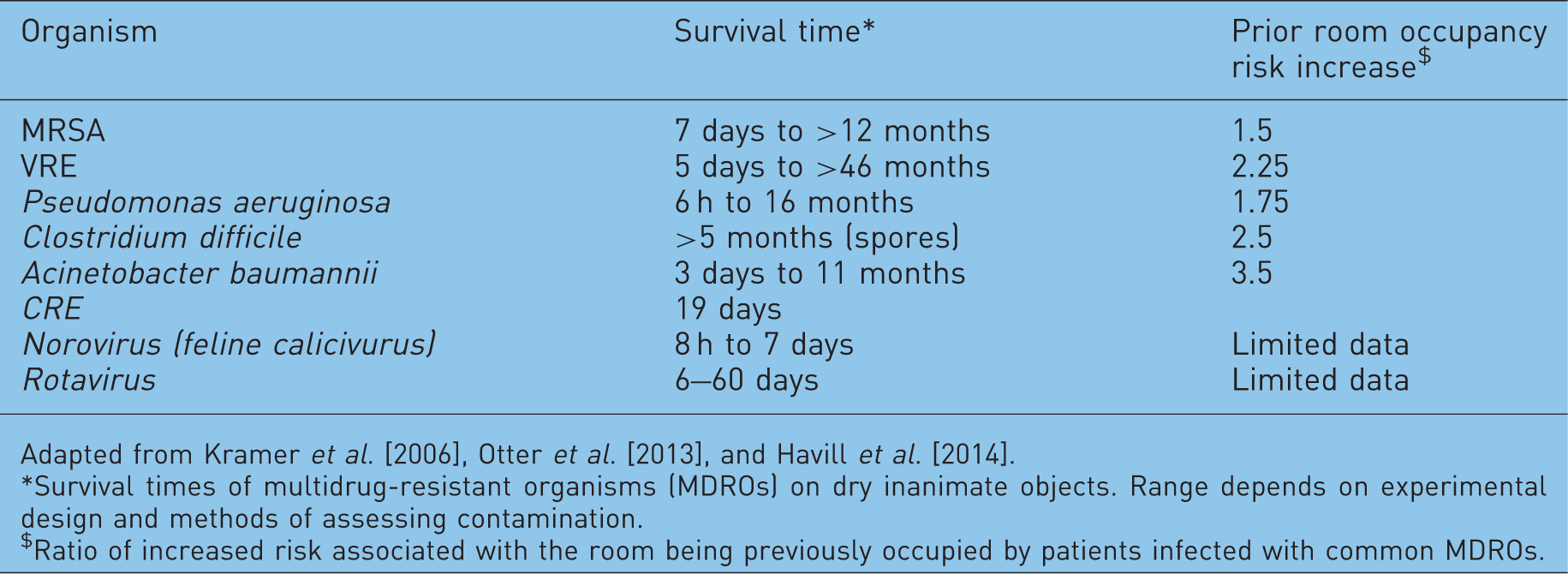
Adapted from Kramer et al. [2006], Otter et al. [2013], and Havill et al. [2014].
Survival times of multidrug-resistant organisms (MDROs) on dry inanimate objects. Range depends on experimental design and methods of assessing contamination.
$Ratio of increased risk associated with the room being previously occupied by patients infected with common MDROs.
Presence of MDROs in the patient care environment
There are numerous studies demonstrating the presence of MDROs in the patient care environment. These studies typically focus on MRSA, VRE, and C. difficile; however, Acinetobacter and norovirus are also frequently sampled. Contamination levels have been found that exceed the number of bacteria or virons necessary for the transmission of the organisms [Otter et al. 2013]. While it is not known whether the contamination levels on any individual surface will exceed the number of organisms necessary to be transmitted or cause disease, the summation of contamination in a room can pose a significant hazard to the next patient. This summation of contamination is particularly relevant when considered in conjunction with extended survival times of MDROs on hard surfaces. Multiple studies have demonstrated the presence of pathogens in the environment [Getchell-White et al. 1989; French et al. 2004; Dubberke et al. 2007; Dumford et al. 2009]; in one, MRSA was cultured from 43% of beds of individuals not known to be MRSA positive [French et al. 2004], and in another, VRE was cultured from 13% of surfaces in rooms of patients not known to be colonized with VRE [Trick et al. 2002]. Byers and colleagues concluded that 16% of hospital room surfaces contained VRE-positive samples, even though standard terminal cleaning protocols for rooms with a previous VRE-positive occupant had been followed [Byers et al. 1998]. Most likely, this contamination of rooms of unaffected patients is due to viability of organisms shed by previous occupants [French et al. 2004; Drees et al. 2008; Hardy et al. 2006], but it could also be due to horizontal transmission from healthcare workers, visitors or asymptomatic carriers [Riggs et al. 2007], as well as migration of the organisms through air flow or other means [Creamer et al. 2014; Edmiston et al. 2005]. For patients with clinical infection with MRSA or VRE, the frequency of environmental contamination with these organisms correlates with the number of culture-positive body sites [Rohr et al. 2009; Bonten et al. 1996; Boyce et al. 2007]. These patients may also shed more pathogens than those who are only colonized, especially if they have diarrhea, which may result in widespread contamination [Boyce et al. 1997, 2007; Boyce, 2007].
Prior room occupancy risk
Prior room occupancy risk is defined as the risk conferred to a new patient based on the characteristics of the patient who occupied the room before. As expected, the presence of a positive culture for a given pathogen from the prior occupant of the room places the subsequent occupant at higher risk for acquisition of the same pathogen [Otter et al. 2013; Drees et al. 2008; Huang et al. 2006b; Nseir et al. 2011; Shaughnessy et al. 2011]. Since there is no direct contact between the two patients, this risk is associated with the environment. The VRE colonization status of the prior occupant, for example, is predictive for an increase in VRE colonization risk to the subsequent occupant [Drees et al. 2008; Nseir et al. 2011]. In a 14-month surveillance study across two intensive care units (ICUs), patients in rooms with previous VRE-colonized occupants were three times more likely to acquire VRE as those whose rooms did not house a colonized patient [Drees et al. 2008]. This pattern is also true for MRSA. Among 10,000 patients with a previous MRSA-positive infected or colonized room occupant, 3.9% acquired MRSA colonization compared with 2.9% for non-MRSA-positive rooms [Huang et al. 2006b]. Of patients who acquired C. difficile infection (CDI) after ICU admission, 11% had a CDI-positive prior room occupant compared with 4.6% who did not (p = 0.002) [Shaughnessy et al. 2011]. Furthermore, Huang et al. [2006c] found that admission to a room previously occupied by a patient with an MDRO increased the risk of the next patient by 40%. It is important to note that this increase in risk can affect not only patients admitted to rooms in which the prior occupants tested positive for a pathogen but also other patients in the facility and even patients in other facilities in a network [Lee et al. 2011]. Table 1 shows a summary of the additional risk attributed to the prior room occupant for a number of organisms.
These risks identified above represent vertical transmission of pathogens within an institution. Methods of assessing horizontal transmission continue to evolve with new applications of existing technologies. New tools are deployed to understand the interrelation between HAIs, the environment, and the sources of risk. For example, using molecular epidemiologic techniques, such as polymerase chain reaction, the identification of clonal types within species can be quantified [Bhalla et al. 2004]. This has led to the discovery of outbreaks in situations in which no indications were present by using standard infection control surveillance and definitions [Carling and Bartley, 2010].
The use of these techniques to explore clonal repetition can potentially provide new insight into the spread of pathogens within a healthcare facility over time in addition to infection control practices. It is expected that, at some point, molecular epidemiological techniques will be deployed in a routine fashion to provide insight into the transmission of organisms within a facility.
Impact of enhanced cleaning on HAIs
The risk of disease transmission attributable to contaminated surfaces in the patient environment such as bed rails, handles, and grab bars has been well defined, and there has been a clear demonstration that enhancing environmental disinfection of high-touch surfaces can lead to a decrease in HAI rates. Improved cleaning thoroughness and enhanced cleaning methods can lead to a reduction in the acquisition of HAIs. These methods include utilizing checklists to ensure that high-touch surfaces are cleaned first, double cleaning of rooms, and the addition of cleaners dedicated to high-touch surfaces [Boyce, 2007; Donskey, 2013; Dancer, 2009]. Many infection prevention guidelines have recommended the use of routine hypochlorite disinfection in place of standard disinfection to prevent transmission of C. difficile. A study of two medical wards treating older people found that the use of hypochlorite was associated with a significant decrease in hospital-associated C. difficile [Wilcox et al. 2003]. Furthermore, a study looking at the use of hypochlorite in ICUs found that it was effective at reducing infection rates when used for all discharge cleaning, and when used only for cleaning C. difficile isolation rooms [McMullen et al. 2007].
Issues with current practices
Compliance with routine and terminal cleaning
In multiple studies, researchers marked high-touch surfaces in rooms with a marker visible only under ultraviolet (UV) light in order to determine whether the surfaces had been cleaned [Carling et al. 2008a, 2008b, 2010]. In one of those studies, 1404 surfaces in 157 patient rooms were checked after routine cleaning, and only 47% of the surfaces had actually been cleaned [Carling et al. 2006b]. This result reflects the inability of hospital cleaning staff to consistently and systematically clean a room owing to time pressure, training issues, high turnover rate and other difficulties.
Equipment
The impact of the contamination of mobile medical equipment such as intravenous poles, carts, and documentation stations has not been well studied. Best-practice guidelines related to portable medical equipment recommend disinfection between uses [Healthcare Infection Control Practices Advisory Committee, 2003]. The contamination of these types of equipment and the recovery of MDROs such as MRSA on the equipment’s surfaces have been documented [Havill et al. 2011]. A systematic review of 23 studies showed that 86.8% of equipment was found to be contaminated, with an average of 82.1 colonies per surface, with known pathogens such as MRSA, Pseudomonas spp. and Acinetobacter spp. [Schabrun and Chipchase, 2006]. Furthermore, environmental sampling for C. difficile spores revealed that around 20% of mobile equipment was contaminated, including pulse oximeters, medication carts, and barcode scanners [Dumford et al. 2009]. Interestingly, contamination of medical equipment has also been tied to outbreaks of MDRO infections. For example, VRE outbreaks have been linked to contamination of rectal thermometers, ear thermometers, and electrocardiogram leads [Falk et al. 2000; Livornese et al. 1992; Porwancher et al. 1997], and an MRSA outbreak in a head and neck surgery center in the Netherlands was linked to contamination of ultrasonic nebulizers [Schultsz et al. 2003].
Current cleaning practices are often inconsistent for mobile medical equipment, with uncertainty between the nursing and environmental staff on cleaning roles, cleaning frequency, and cleaning methods. Recently, the Joint Commission has placed an increased focus on identifying clean and dirty equipment [Joint Commission, 2010].
Clothing and hand-held electronics
The clothing of healthcare workers (i.e. white coats, ties, and jackets) and gadgets (i.e. pagers, tablets, and other devices) may play a role in the spread of microorganisms, mainly MDROs. The presence of microorganisms on these items has been well documented [Munoz-Price et al. 2012; Singh et al. 2002; Goldblatt et al. 2007; Lopez et al. 2009]. Recently, the Society for Healthcare Epidemiology of America issued new guidelines to reduce the use of white coats in the clinical setting [Bearman et al. 2014]. Like mobile medical equipment, current cleaning practices for garments are often infrequent and inconsistent. However, the link between contamination on these items and HAIs has not yet been established.
Cloth surfaces
Upholstered furnishings are becoming increasingly common in patient-care areas as hospitals seek to reduce the patient’s perception of the hospital as a clinical environment. As a result, many surfaces have been introduced to patient rooms without adequate training or processes in place to assure the successful disinfection or cleaning of those surfaces. For example, curtains are often only laundered when visibly soiled. It is still unknown how much the contamination of these materials can cause horizontal spread of organisms through the hands of healthcare workers or act as a reservoir for these organisms [Trillis et al. 2008].
Solution/wipe contamination and improper application
Components of the cleaning process can rapidly become contaminated themselves. Bucket-based cleaning tools and fluids become contaminated rapidly and potentially serve as a point of transfer of pathogens from one surface to another [Healthcare Infection Control Practices Advisory Committee, 2003]. Additionally, many disinfectants require the mixing of different chemicals on site. Errors in the process lead to reduced efficacy and potential hazard for cleaning staff [Sarwar et al. 2004; Singer et al. 2006]. Mop heads and wipes, if not used correctly, also become contaminated and potentially spread pathogens from surface to surface. This has led to adoption of disposable cleaning items, such as disposable wipes. However, some studies have shown that wipes themselves can become contaminated, especially if not used according to manufacturer’s instructions. This often occurs when environmental workers use one wipe to disinfect multiple surfaces, or a greater surface area than recommended by the manufacturer [Sattar, 2010].
There is also the risk of contamination of hands when performing hand hygiene. Contamination of soap has been reported [Sartor et al. 2000], as well as contamination of the sink area [Doring et al. 1996]. One academic center removed all automatic faucets from their facility because of contamination of the aerators [Hargreaves et al. 2001].
Acquired resistance to disinfectants
The persistent pressure of disinfectants on the microorganisms present in the environment may lead to the development of resistance. Many organisms already possess intrinsic resistance to common disinfectants and acquired resistance through plasmid mediated transmission is becoming more common [McDonnell and Russell, 1999]. Recurrent exposure of bacteria to chlorhexidine has been linked to higher levels of resistance [Block and Furman, 2002]. Concern about resistance to triclosan, as well as unsupported marketing claims, has led to a US Food and Drug Administration ban of the chemical [Halden, 2014]. With the rapid emergence of resistance to disinfectant, it may be prudent to assess efficacy of the disinfectant used in the facility against common clinical isolates [Kawamura-Sato et al. 2010].
Contact precautions
Contact precautions and using personal protective equipment for patients on isolation have long been a primary means of containing pathogens to a limited environment within a facility. Recent controversy suggests that contact precautions isolation may have no impact on hospital-associated MRSA infections [Gasink and Brennan, 2009; Abad et al. 2010], but other data contradict that finding [Healthcare Infection Control Practices Advisory Committee, 2007]. Patients in contact isolation are significantly less likely to have interactions with their healthcare providers for the duration of their isolation [Evans et al. 2003]. This decrease in provider contact is an additional argument for reassessing the routine use of isolation precautions. Additional strategies, such as decolonization of patients with chlorohexidine bath [Climo et al. 2013], can reduce the risk of transmission of MDROs potentially by reducing the bioburden of pathogens in the environment. Additional research into the cost effectiveness of contact precautions, routine screening, and decolonization is merited.
Hand hygiene/environment connection
International guidelines recommend performing hand hygiene procedures after coming into contact with surfaces in the patient environment [Boyce and Pittet, 2002; WHO, 2009]. In one study, hand imprint cultures were positive for one or more pathogens after contacting surfaces near 34 of 64 patients (53%) in occupied rooms and in 6 of 25 rooms (24%) that had been cleaned after patient discharge. S. aureus and VRE were the most common organisms isolated. All 12 of the VRE isolates were identified as Enterococcus faecium and 7 (35%) of the S. aureus isolates were MRSA strains [Bhalla et al. 2004].
The addition of antimicrobial chemicals to hand hygiene products was an effective method for enhancing bacteriostatic activity. However, over time, organisms have developed resistance to chemicals such as chlorhexidine and triclosan [Block and Furman, 2002; Goroncy-Bermes and Schouten, 2001]. While alcohol-based hand rubs are effective and have not shown any evidence of inducing bacterial resistance [Kampf and Kramer, 2004], they are not as effective as soap and water for hand washing for elimination of bacterial spores from the skin [Weber et al. 2003].
Suboptimal compliance with appropriate hand hygiene has been well documented. Overall, healthcare worker compliance with hand hygiene is around 40% [Boyce and Pittet, 2002]. Studies have also shown that the average hand hygiene event does not last for the recommended 15–20 s [WHO, 2009]. To better track and administer hand hygiene programs, electronic monitoring systems have been implemented. These systems use a variety of techniques to assess compliance, and reporting and behavior correction can occur in real time [Boyce, 2011]. The accuracy of electronic monitoring systems continues to improve and their use in hospitals may become more appealing.
Beyond the guidelines: emerging technologies
As more attention is focused on HAI reduction and the role of the environment in transmission, a number of technologies are emerging to reduce the risk derived from the microbial reservoir in patient care areas. Many of these technologies have been proven effective in the laboratory setting, but have an unknown impact on facility-wide HAI rates.
New disinfectant claims
Multiple products have emerged with new disinfectant claims, mostly centered on C. difficile spore kill times. Special consideration should be given to the mechanism of delivery of the disinfectant to the targeted surface and the required contact time for the chemical. Some application methods may not adequately moisten a surface for the entire contact time and long contact times may not be achievable due to the time pressures in the healthcare environment [Carling and Huang, 2013]. As we have seen above, human factors result in a high percentage of high-touch surfaces being missed in typical disinfection; that fact and the compliance of housekeeping with the use of any disinfectant, including the correct mixing of chemicals, are important factors when evaluating new products.
Environmental monitoring
Improving manual disinfection compliance can be accomplished, to a degree, through enhanced monitoring of the environmental workers [Carling and Huang, 2013]. Many facilities have deployed these technologies to comply with Joint Commission Standards 2013 EC.04.01.03.EP2: ‘results of data analysis [are used to] identify [and correct] opportunities to resolve environmental safety issues’. Available from http://www.jointcommission.org/Standards/ (accessed March 19, 2014).
Such practice has relied on a visual assessment of cleanliness; however, studies have identified no correlation between the visual assessment and a significant decrease in the microbiological contamination level [Carling, 2008; Carling et al. 2006a]. As a result, the visual assessment is considered an inadequate measure of monitoring environmental contamination.
More commonly accepted measures for environmental monitoring include environmental surface sampling, fluorescent marking systems and adenosine triphosphate (ATP) monitoring [Guh and Carling, 2010; Rutala and Weber, 2008]. These methods are effective because they provide immediate feedback and educational opportunities for the cleaning staff. Continuing education and reinforcement of cleaning techniques, in conjunction with environmental monitoring, is critical for providing a clean healthcare environment [Carling and Huang, 2013].
Environmental surface sampling is the current Centers for Disease Control and Prevention recommendation; however, this sampling is limited to times of outbreak rather than part of a routine practice [Sehulster and Chinn, 2003]. This protocol may change as specific sampling techniques, such as a polymerase chain reaction based system, become affordable and quick to identify. A third measure for assessment of cleanliness is ATP monitoring; however, more evidence that effectively correlates ATP levels and environmental contamination is needed [Carling and Huang, 2013].
Self-disinfecting surfaces
Surfaces with self-disinfecting properties have been emerging in the marketplace. These surfaces use a variety of approaches to achieve disinfection, including antimicrobial copper, titanium dioxide coatings, and other technologies [Salgado et al. 2013; Schmidt et al. 2013; Li et al. 2006]. The efficacy of these surfaces has been demonstrated in the laboratory, but the slow kill times and selective use of antimicrobial surfaces in hospitals have yet to show a proven impact on HAIs. Additionally, there is concern that resistance to these surfaces may develop over time as organisms are exposed to the antimicrobial mechanism over long periods. As more of these surfaces are used in healthcare settings, data will indicate whether they are effective or cost effective.
Automated disinfection systems
Enhanced environmental disinfection has been shown to have a significant impact on HAI rates [Donskey, 2013]. These enhanced cleaning methods have typically relied on additional manpower or a change in cleaning chemicals. Over the past several years, a number of automated disinfection systems that use hydrogen peroxide or UV light have entered the market. These systems vary greatly in their disinfection methods and application in the healthcare environment.
There are three commercially available technologies for the automated disinfection of rooms in healthcare environments: hydrogen peroxide vapor, mercury UV light and pulsed xenon UV light. All three technologies have been deployed in hospitals.
Economic justifications for facilities considering these types of systems should be based not only on the capital cost of the systems, but also on projected avoided costs associated with prevented infections. These projections and their costs should be based on the available medical literature. As pay for performance metrics for hospitals continue to change, the cost effectiveness of these systems may increase.
Hydrogen peroxide vapor
Reductions of healthcare-associated infections associated with automated room disinfection systems.
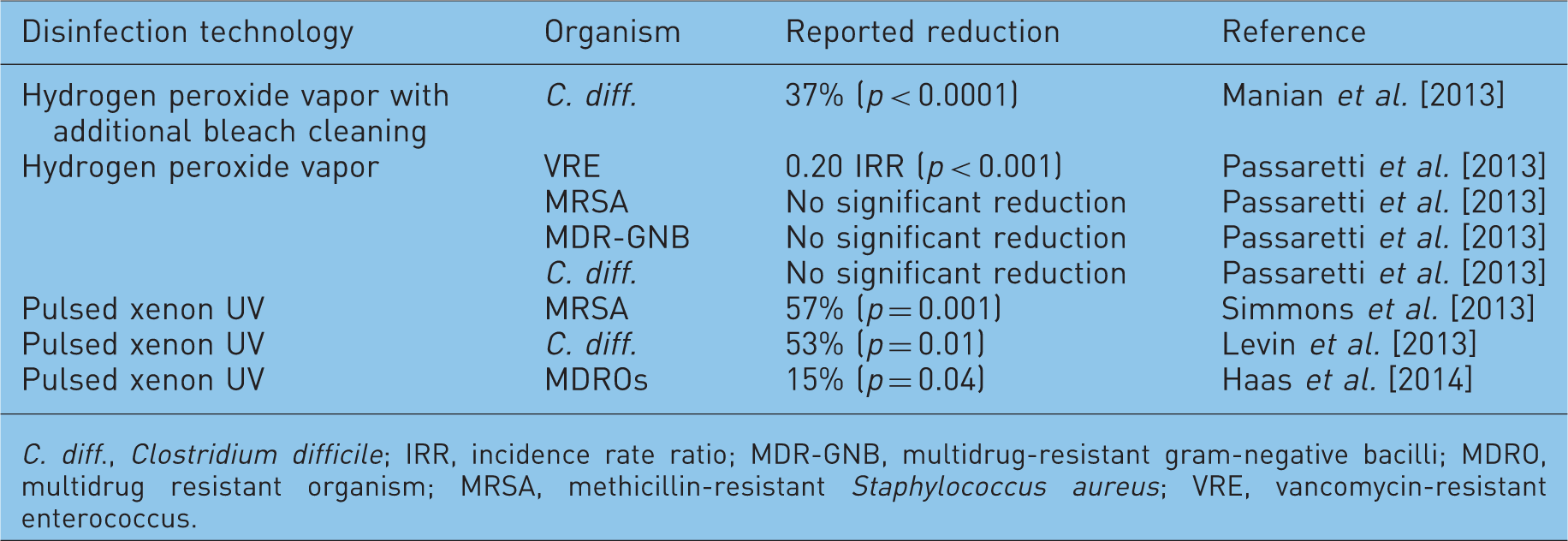
C. diff., Clostridium difficile; IRR, incidence rate ratio; MDR-GNB, multidrug-resistant gram-negative bacilli; MDRO, multidrug resistant organism; MRSA, methicillin-resistant Staphylococcus aureus; VRE, vancomycin-resistant enterococcus.
This vapor poses a potential health risk to humans; exposure can lead to irritation of the eyes, nose, throat, and lungs [BioQuell, 2010]. Because of this risk, certain measures need to be taken to appropriately seal the room prior to use of the disinfection system. This preparation includes sealing of doors and windows, as well as ventilation intakes and returns. Failure to appropriately seal the room can result in leakage of the product that exceeds recommended short-term exposure limits [Fu et al. 2012]. In addition, the time required completing the sealing and disinfection process ranges from 1.5 to 4 h, depending on the size of the room [Passaretti et al. 2013; Boyce et al. 2008; Havill et al. 2012; Holmdahl et al. 2011; Manian et al. 2013].
Mercury ultraviolet
Mercury systems generate monochromatic UV light, with the majority of the emitted light occurring at a wavelength of 254 nm [Harm, 1980; Rutala et al. 2010]. This wavelength of light is able to induce pyrimidine dimers in the DNA of organisms [Harm, 1980; Wang, 1976]. However, the optimum wavelength for producing pyrimidine dimers is 265 nm [Harm, 1980; Wang, 1976], which means that mercury systems induce dimers at a slower rate than the lower frequency light [Kowalski, 2009]. Published data regarding efficacy and disinfection times for mercury systems have shown reductions in vegetative organisms such as MRSA and VRE with approximately 15 min of exposure and reductions in C. difficile spores with approximately 100 min of exposure [Rutala et al. 2010; Boyce et al. 2011]. As with hydrogen peroxide systems, there are safety concerns associated with the use of UV light. Direct, prolonged exposure to UV light can result in a temporary irritation of the cornea and conjunctiva of the eye [Kowalski, 2009; Cullen, 2002]. The risk of exposure is mitigated by the use of motion sensors that shut off the device.
Pulsed xenon ultraviolet
The alternative method for production of UV light is through pulsed xenon flash lamps. These lamps utilize xenon gas to generate broad-spectrum, high-intensity UV light. Pulsed xenon technology emits light throughout the germicidal spectrum, ranging from 200 to 280 nm [Boyce et al. 2011]. As with mercury-based systems, xenon systems achieve deactivation of pathogens by inducing thymine dimers [Boyce et al. 2011]. Because pulsed xenon emits UV throughout the germicidal spectrum, it is able to induce dimers with optimum efficiency. This broad-spectrum light also allows pulsed xenon light to deactivate bacteria with three unique mechanisms: photosplitting, the creation of single- or double-strand breaks in the DNA; photohydration, the addition of a water molecule across a carbonyl group of a DNA base; and photocrosslinking, which causes abnormal bonding activity in proteins [Harm, 1980; Wang, 1976; Kowalski, 2009]. These additional mechanisms of action allow for more rapid deactivation of pathogens. Studies on the disinfection times for pulsed xenon UV show reductions for C. difficile spores and vegetative organisms within 5 min [Simmons et al. 2013; Stibich et al. 2011]. Safety concerns related to pulsed xenon UV are the same as those for mercury systems. As with the mercury systems, these risks are mitigated by implementing motion sensors that shut off the device.
When utilizing UV light for disinfection, regardless of type, it is critical to consider the enhanced efficacy associated with direct line of sight. Reflected light has been found to be substantially less effective than direct light at eliminating pathogens [Rutala et al. 2010; Boyce et al. 2011]. Separate areas such as bathrooms have been found to receive insufficient levels of disinfection when the only disinfection cycle occurs in the main patient room [Boyce et al. 2011]. To account for the poorer disinfection efficacy of reflected light, multiple positions are necessary when utilizing a UV system.
All of these systems have demonstrated an ability to reduce contamination levels in the environment. Of interest is whether this environmental reduction translates into a reduction in HAI rates. Table 2 summarizes the published data regarding infection reductions associated with use of automated disinfection systems.
Conclusion
It has been demonstrated that pathogens can survive in and be recovered from healthcare environments. Further, the risk of HAIs can be linked to the prior room occupant and lessened through environmental interventions. The issues with current practices identified here are not meant to be a comprehensive list of gaps, but rather to broaden and stimulate thinking about how the environment interacts with pathogens to produce risk for patients.
The patient environment has not received the same level of focused attention from infectious diseases researchers and infection preventionists as other areas. Now that many facilities have established good infection control practices, it is likely that additional HAI reductions will come from outside the current practices, through interventions such as automated room disinfection or molecular epidemiological investigations of clonal spread of specific pathogens.
The environment should be considered a substantial factor in infection control practices, and resources should be directed to improving our understanding of the interaction of pathogen survival, disinfection, hand hygiene, and HAI risk.
Footnotes
Funding
This research is supported in part by the National Institutes of Health through MD Anderson’s Cancer Center Support Grant CA016672.
Conflict of interest statement
RFC is a consultant for Xenex Healthcare Services; SS, CDJ, MR, JG, JS and MS are employees of Xenex Healthcare Services; SSG has no competing financial interest to declare.
Acknowledgment
The authors thank Ms Sunita C. Patterson of MD Anderson Cancer Center for editorial support.