
Abstract
Background:
Availability of personal protective equipment (PPE) and its effective use may influence safety climate perceptions among health care personnel (HCP). It is unclear how health care organizations can leverage the effective use of respiratory protection to engage in continuous improvement of their safety climate, which can inform opportunities for employee education and engagement.
Methods:
After using an elastomeric half mask respirator (EHMR) as their primary form of respiratory protection for several months, 1,080 HCP provided feedback in an electronic survey about respiratory protection training, confidence in EHMR use, barriers during use, and perceived safety climate. Ordinal logistic regressions were used as nonlinear models to test relationships between these variables.
Findings:
We observed that an increase in user confidence (p < .013), training content (p < .001), training formats (p < .001), and a decrease in EHMR barriers (p < .001) were associated with a statistically significant increase in proactive safety climate. In the second model, an increase in user confidence (p < .006) and training content (p < .001), and a decrease in barriers (p < .001), was associated with a statistically significant increase in compliant safety climate.
Conclusions/Application to Practice:
HCP EHMR confidence was positively associated with safety climate perceptions, underscoring the value of competency building by respiratory protection leaders prior to implementation. Because fewer barriers experienced while using an EHMR were associated with a more positive perception of safety climate, it is important to first communicate with end users about potential barriers and, second, to continue research with end users and manufacturers to improve the design of EHMRs moving forward.
Background
Proactive leadership, worker accountability, and organizational support have been referenced as characteristics of a supportive safety culture/climate to enhance the perceptions of health care personnel (HCP) on the job (Joint Commission Center for Transforming Healthcare, 2019a; Turbow & Scibilia, 2021). A culture of safety focuses on leadership commitment, safety climate metrics, and other robust tools to improve organizational processes (Chassin & Loeb, 2013; Joint Commission Center for Transforming Health care, 2019b). Safety climate, in comparison, is a narrower concept and focuses on current, shared perceptions of the workforce regarding safety policies and procedures that can influence employees’ attitudes and actions toward safety (Mearns et al., 2010; Neal & Griffin, 2004; Zohar, 2003). Safety climate dimensions previously measured in health care include leadership and management, group behaviors and relationships, communication, work/life balance, resource adequacy, and organizational commitment (including proactive and compliant processes) toward safety (Flin et al., 2006; Gershon et al., 2007; McCaughey et al., 2014). Safety climate metrics have demonstrated the predictive utility of employee proactivity and compliance at work, serving as an indicator to prevent injuries and illness (Flin et al., 2006; Neal & Griffin, 2006; Renecle et al., 2021).
The availability of personal protective equipment (PPE) and lack of effective use can negatively impact safety climate if employees perceive it to be a low priority for management (DeJoy et al., 2017; Platania et al., 2022). Conversely, a positive safety climate has been linked to general, consistent use of PPE (Arcury et al., 2013) and then more specifically, the use of respiratory protection among HCP (Rozenbojm et al., 2015). Although the association between safety climate and use of PPE in health care has been studied, the association between HCP experiences with respiratory protection and the potential impact on perceived safety climate has not been examined. This gap in research to practice is important because, although many connections exist in the literature, it is unclear how organizations can leverage the availability and effective use of respiratory protection among their workforce in a way that positively impacts employee’s safety climate perceptions to initiate other positive outcomes.
As one form of PPE, elastomeric half mask respirator (EHMR) use may also be significantly linked to safety climate or safety culture (Hines et al., 2019a, 2019b). The National Institute for Occupational Safety and Health (NIOSH)-approved EHMRs are a reusable type of respiratory protection that have been encouraged for use in U.S. health care settings by hospitals as an acceptable alternative to disposable N95 filtering facepiece respirators (FFRs; Pompeii & Hines, 2021). The integration of EHMRs is attractive for some health care settings as previous research has noted that the demand for disposable respirators within health care is likely to exceed supply during large respiratory infectious disease outbreaks (Patel et al., 2017). With the demand for single-use, disposable FFRs during pandemic outbreaks, the inclusion of reusable respirators into the workplace can mitigate issues related to shortages and inadequate protection. Consequently, EHMRs were discussed as a viable option during the COVID-19 pandemic when settings were experiencing crisis or contingency scenarios (Centers for Disease Control and Prevention [CDC], 2020). The National Academies of Science (NAS, 2019) also recommended wider use of EHMRs in health care settings around the same time.
Recently, Greenawald and colleagues (2021) highlighted the role of EHMRs in future pandemics, indicating that new models, guidance documents, procurements, and research are likely to follow suit. Despite such recommendations, this type of respiratory protection has not been used extensively in the health care field, leading to a gap in knowledge about best practices and how HCP perceive them when used on a regular basis—not only in emergency scenarios. Some studies have compared and determined that fit testing and training health care workers to EHMRs is comparable to N95 FFRs (Pompeii et al., 2020); however, there is a gap in research contributing to the organizational management and communication around such processes. It is important to address this gap as integrating EHMRs into a Respiratory Protection Program (RPP) can be daunting and, if not communicated and implemented with employees in mind, could have negative consequences on the organization’s safety climate.
To date, research linking PPE use and safety climate has made recommendations to boost access to and availability of PPE (DeJoy et al., 2017) and to improve engagement around PPE selection (Peterson et al., 2016). However, using safety climate as a dependent variable can be a reliable measure to assess improvements needed in respiratory protection design as well as implementation of new or different types of respirators via targeted trainings and interventions that seek to support HCP effective and sustainable PPE practices. To this end, we examined how the implementation of additional respiratory protection and complementary processes and trainings may impact the perceived safety climate among HCP, using EHMRs as a case example.
Methods
Two hospital systems (A and B) participated in this study. System A is the flagship academic medical center of a state university system that employs more than 9,000 staff, along with 1,300 faculty physicians and 950 residents work in this urban, mid-Atlantic hospital. System B is a member of a nine-hospital system consisting of 21,000 employees. Both hospital systems were implementing EHMRs at their locations to a subset of HCP, based on availability of EHMRs provided for the study. These hospitals were also provided resources on implementation of policies on use, cleaning, and storage of the EHMR by HCPs. Both hospital systems used different EHMR models and had been using them routinely for about 10 to 12 months when the surveys were deployed. Both EHMR models used at the time of the study and survey deployment had exhalation valves and no adaptations were made to the respirator body for use in health care. However, hospital policy did dictate that exhalation valves needed to be covered to prevent possible illness spreading from HCP to patients. This was normally achieved with a surgical mask being placed over the exhalation valve although a face shield worn over the respirator was also used.
HCPs were identified for participation by role and department to include physicians and advanced practice providers (e.g., nurse practitioners), nurses, nursing assistants, respiratory therapists, dietary services staff, environmental services staff, and facilities management personnel working in intensive care units (ICU), emergency departments (ED), operating room (OR), pediatrics, medical/surgical units, and other cohort units based on internal risk assessments by position. Between the locations, 4,676 HCPs (n = 2,419 at System A; n = 2,257 at System B) were fit tested to wear an EHMR and trained in accordance with the U.S. Occupational Safety and Health Administration (OSHA) Respiratory Protection Standard (29 CFR 1910.134). Training included how to clean, disinfect, and store their EHMR between patients and at the end of their shift. The voluntary survey link was emailed to the eligible 4,676 HCPs. The study protocols were approved by the respective Institutional Review Boards of the participating hospital systems.
Data Collection
Workers were surveyed between April and June 2021 about their training on EHMRs, confidence in use, barriers experienced during use, and perceived safety climate. A 55-question survey was developed in collaboration with NIOSH and the two participating hospitals and deployed online using REDCap (Research Electronic Data Capture; Harris et al., 2009, 2019). The survey included the following domains of interest in the current study.
Confidence in EHMR Use
This scale consisted of two questions. Respondents were asked, first, how confident they were in being able to don and doff their EHMR correctly and, second, how confident they were in being able to don and use their EHMR correctly each time they wear it. A 1 to 4 scale was used where 1 was not confident at all (can do correctly less than 25% of the time) and 4 was fully confident (can do correctly every time).
Barriers During EHMR Use
Respondents were asked to check all barriers that applied to them while wearing an EHMR from a list of 13 options: (a) it is difficult to breathe; (b) bothered by moisture buildup; (c) interferes with other PPE, such as a face shield; (d) interferes with normal eyeglasses; (e) difficulty speaking or being understood by patients; (f) difficulty speaking or being understood by trainees/residents; (g) difficulty speaking or being understood by colleagues; (h) uncomfortable to wear for less than 1 hour; (i) uncomfortable to wear for more than 1 hour; (j) feels uncomfortably warm; (k) feels claustrophobic; (l) difficulty due to hairstyle; and (m) causes skin irritation or acne. The ordinal variable for analysis was created by adding each option checked by respondents, where a higher cumulative value (up to 13 maximum) indicated more barriers encountered while using their EHMR, while a lower number (0 possible) indicated no barriers encountered while using the EHMR.
Respiratory Protection Training Content
Respondents were asked two questions including “Which of the following were training formats that you were exposed to regarding respiratory protection, in general? (Check all that apply).” The second question was specific to EHMR training: “What is included in the training you received specific to EHMRs? (Check all that apply).” Both questions posed the same eight response options: (a) why the respirator is necessary; (b) fit-testing procedures; (c) how improper fit, use, or maintenance can compromise protective effects; (d) limitations and capabilities of EHMRs; (e) how to inspect, use, and check the seals; (f) how to don and doff; (g) cleaning, storage, disposal, and maintenance procedures; and (h) cartridge or respirator change schedule. The responses for these two questions were combined to create an ordinal variable where a higher cumulative number (up to 16 maximum) indicated more thorough respiratory protection training.
Respiratory Protection Training Format
Respondents were asked to check all training formats that they were exposed to during their respiratory protection training. Eight options were provided: (a) trained exclusively when I went for fit testing, (b) lectures, (c) in-person training with trainee participation, (d) videos, (e) written study materials, (f) quizzes, (g) online training, and (h) other. For this ordinal variable, a greater number (8 maximum) designated more diverse training formats, indicating that more than one training method was used (e.g., lecture and quizzes).
Safety Climate Instrument
Respondents were presented with 11 statements about their workplace using a three-option response scale from Disagree to Agree with three being a higher level of agreement with the statement, and hence a more positive perception of the safety climate. The option of Don’t Know was used as a neutral option for the questions to capture another reason why some respondents may otherwise choose to disagree or agree with the item probes (Reips, 2010). Questions were adapted from Peterson and colleagues’ (2016) PPE safety climate scale and additional questions were added to capture EHMR-specific perceptions. However, the two items that were added specific to attitudes around EHMRs were not correlated with the other nine safety climate items and consequently were removed from the scale.
Data Analysis
Prior to completing the analyses to answer the research question for this study, it was important to assess the dependent variable (i.e., safety climate) in greater detail. The nine safety climate items were used in a principal component analysis (PCA) using SPSS version 25 (IBM, 2017). The PCA produced two components with an initial eigenvalue of above 1 (4.033, 1.146) accounting for 57.5% of the variance. Examining the scree plot, component matrix, and pattern matrix, these two components were retained. However, when examining the communalities table, one item had a lower loading (0.265) in comparison with the other eight items. So, this item was removed and the PCA was run again with the remaining eight items.
To verify that the safety climate PCA was suitable for analysis, the Kaiser–Meyer–Olkin (KMO) measure of sample adequacy was checked (KMO = 0.823), passing the 0.6 value test, and the Bartlett’s test of sphericity was significant (p < .001), indicating that the PCA was appropriate to use. Looking at the total variance explained, the two components again produced an initial eigenvalue of above 1 (3.899, 1.125) but accounted for 62.7% of the variance. The component correlation between these two components was 0.493, suggesting strong correlation and reporting of the Oblimin rotation (below). Refer to the Supplemental Table 1.0 and Supplemental Figure 1.0 for the pattern matrix and scree plot with the eigenvalues for these eight components (items), which also includes the mean and standard deviation for each survey item.
Based on the pattern matrix, safety climate was characterized using two broad dimensions with the types of questions that loaded into each component being focused on proactive or compliant safety climate practices. To this end, one component was labeled proactive safety climate scale (e.g., hazards corrected, priority toward safety, supervisor safety communication; Cronbach’s alpha = .828) and the other labeled compliant safety climate scale (e.g., HCP wear respirators when required, supervisors correct workers if respirators are not worn properly; Cronbach’s alpha = .733), both of which were used as dependent variables in the analysis. Finally, because the safety climate survey responses were highly skewed to the right and homogeneous, the scale averages were recategorized into a 6-point scale to allow for greater distribution between the responses. In this case, a 1 represented the lowest perception of safety climate, whereas a 6 represented the highest perception of safety climate.
Although researchers could have retained one safety climate scale as the dependent variable, the way in which the constructs loaded provided an obvious difference in how safety climate could be ascertained as well as implications for organizational response in the future. Proactive safety climate has been discussed as general participation in some studies and examined as extra-role behaviors taken on behalf of individual employees to improve current working conditions, speaking out with ideas, and overcoming safety and health challenges (Griffin & Neal, 2000). Alternatively, a compliant safety climate is a function of not only knowledge and skills but also internal motivation and external support to comply with safety behaviors and processes (Griffin & Neal, 2000). Wearing the necessary PPE and following workplace rules are a function of compliant safety climate and emphasized by management in the workplace (Clark & Ward, 200). Previous studies have shown that these two measures of proactivity and compliance are directly responsible for, albeit in different ways, worker performance, and hence we chose to maintain their separation for the analysis (Christian et al., 2009; Neal et al., 2000).
Analyses sought to understand the relationship between EHMR knowledge in the form of training completeness and formats provided, confidence in EHMR use on a 4-point scale, and cumulative barriers experienced during EHMR use on HCP perceptions of safety climate constructs. These questions were answered using regressions within R v.4.1.2. (R Core Team, 2021). Proportional odds assumption tests were necessary to reliably perform the proportional odds models. R v.4.1.2. was used to perform a Brant test (both using Brant and proTest) to see whether the assumptions held (Brant, 1990). Because the dependent variables were ordinal values, ordinal regression models were used as nonlinear probability models to test these relationships (formulas available upon request).
Results
The survey was completed by 1,080 respondents (n = 480 System A; n = 600 System B). Most respondents had been in their current position for more than 5 years (n = 604, 56%), while 8.1% (n = 87) had been in their position for less than 1 year; 11.6% (n = 125) 1 to 2 years; and 24.2% (n = 261) for 2 to 4 years. Almost half of the respondents were nurses (n = 477, 44.5%) and worked in the ICU (n = 463, 42.9%). About a quarter (25.4%, n = 272) were physicians or physician assistants. Nursing assistant, respiratory therapist, and a technologist or therapist were other commonly held positions that were reported. Regarding education level, 18.7% (n = 167) held an associate degree, while a majority of the sample recorded a 4-year college degree (40.6%, n = 362) or graduate degree (31%, n=276) and the remaining indicated “other” or did not answer the question.
Descriptive statistics for the independent and dependent variables of focus in this study (i.e., EHMR confidence, Training, EHMR experiences, and safety climate) are shown in Table 1. Subjective findings around perceived safety climate and confidence are skewed to the right with more positive perceptions and higher confidence in donning and doffing an EHMR, which is why the scale was recalculated as described earlier.
Descriptive Findings of HCPs Ratings of Safety Climate and EHMR Measures for Confidence in Donning/Doffing EHMRs, EHMR Barriers Experienced, and EHMR Fit Test Training Content and Format
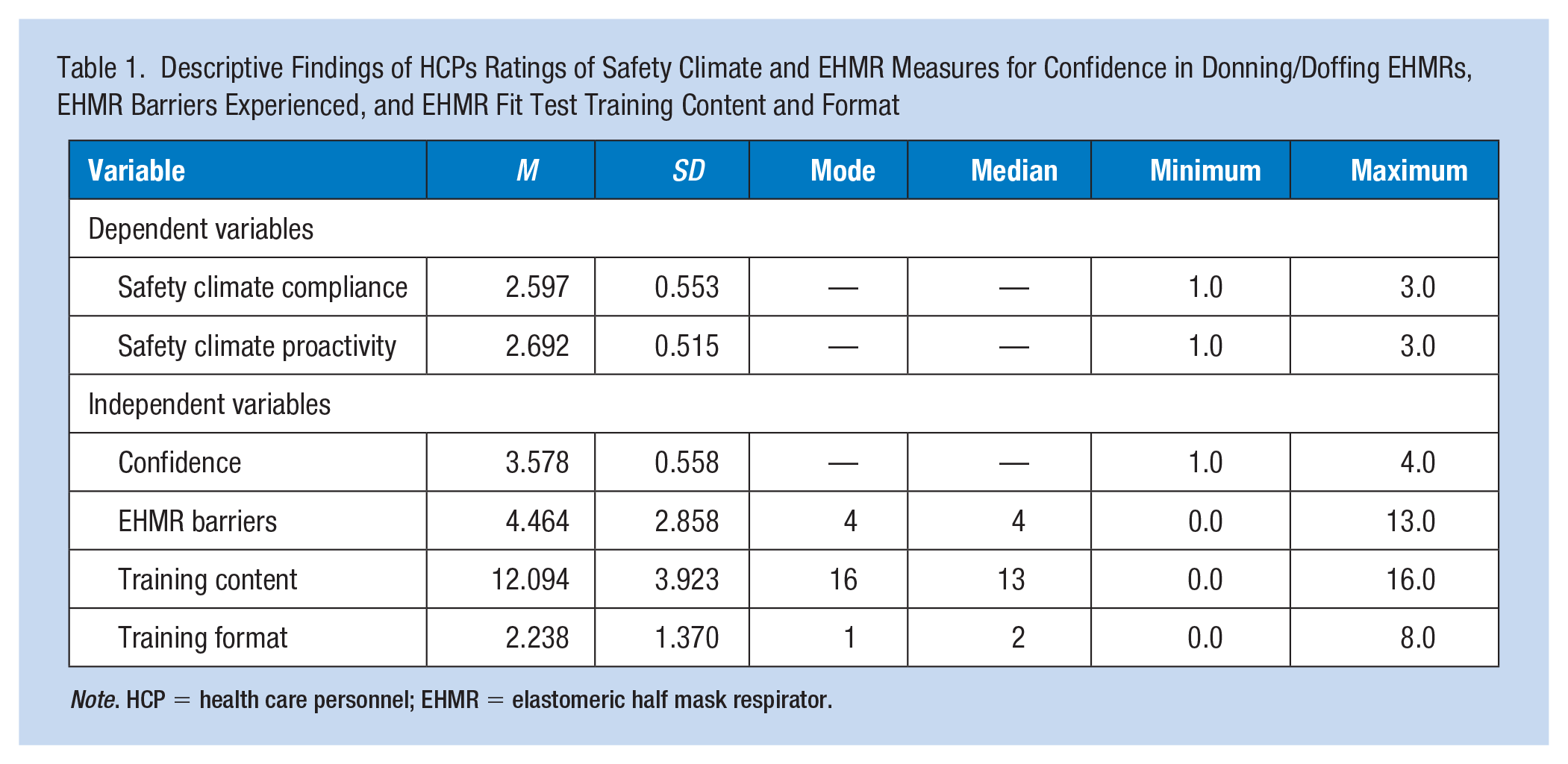
Note. HCP = health care personnel; EHMR = elastomeric half mask respirator.
Findings for the proactive safety climate model showed that the parallel regression assumption held true (chi-square = 15.46, Pr(>chi-square) = 0.75). Findings for the compliant safety climate model showed that the parallel regression assumption also held true (chi-square = 17.67, Pr(>chi-square) = 0.61). Brant tests of individual variables suggested that the assumption was not violated for both tests. These results provided confidence to proceed with the ordinal logistic regressions. In the first ordinal regression model, using the proactive safety climate scale, an increase in user confidence (p < .013), more training content (p < .001), and an increase in training formats (p < .001), and a decrease in EHMR barriers (p < .001), were associated with a statistically significant increase in proactive safety climate (e.g., hazards corrected, priority toward safety, supervisor safety communication). See Table 2 for results.
Ordinal Logit Regression Results of EHMR Confidence in Donning/Doffing, EHMR Barriers Experienced, and Fit Test Training Content and Format on the Proactive Safety Climate Component Among HCP
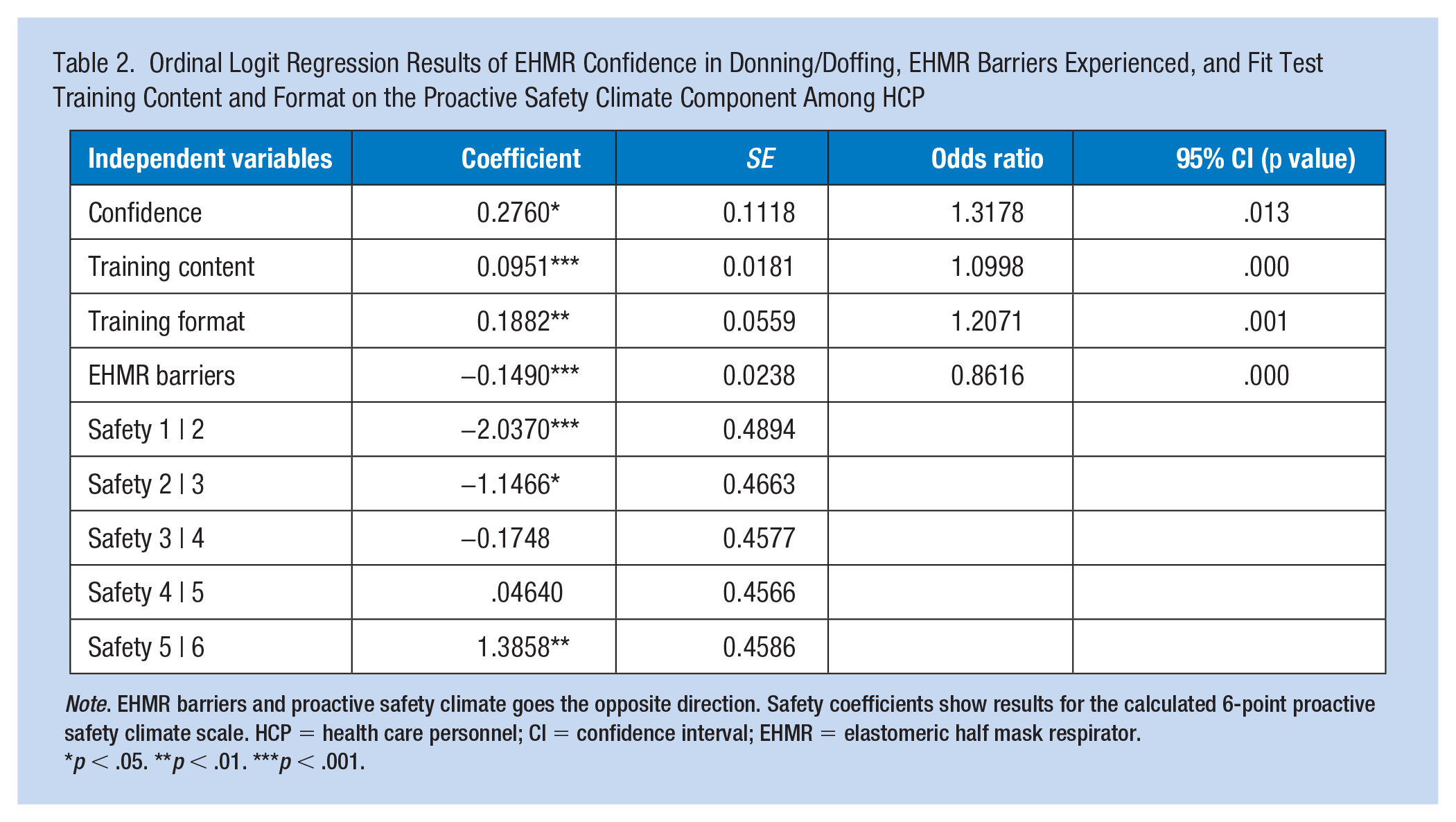
Note. EHMR barriers and proactive safety climate goes the opposite direction. Safety coefficients show results for the calculated 6-point proactive safety climate scale. HCP = health care personnel; CI = confidence interval; EHMR = elastomeric half mask respirator.
p < .05. **p < .01. ***p < .001.
Table 2 shows that the odds of HCP perceiving a positive, proactive safety climate in their organization increase by 31% for each one-unit increase in Confidence, holding all other variables constant; increase by 11% for a one-unit increase in Training content; increase by 21% for a one-unit increase in Training format; and decrease by 14% for each one-unit increase in EHMR barriers, holding others constant.
In the second model, an increase in user confidence (p < .006) and training content (p < .001), and a decrease in EHMR barriers (p < .001), were associated with a statistically significant increase in questions related to the compliant safety climate scale (e.g., HCP wear respirators when required, supervisors correct workers if respirators are not worn properly). Training formats, whether in-person, online, or a combination, were not statistically significant (p < .941) (see Table 3).
Ordinal Logit Regression Results of EHMR Confidence in Donning/Doffing, EHMR Barriers Experienced, and Fit Test Training Content and Format on the Compliant Safety Climate Component Among HCP
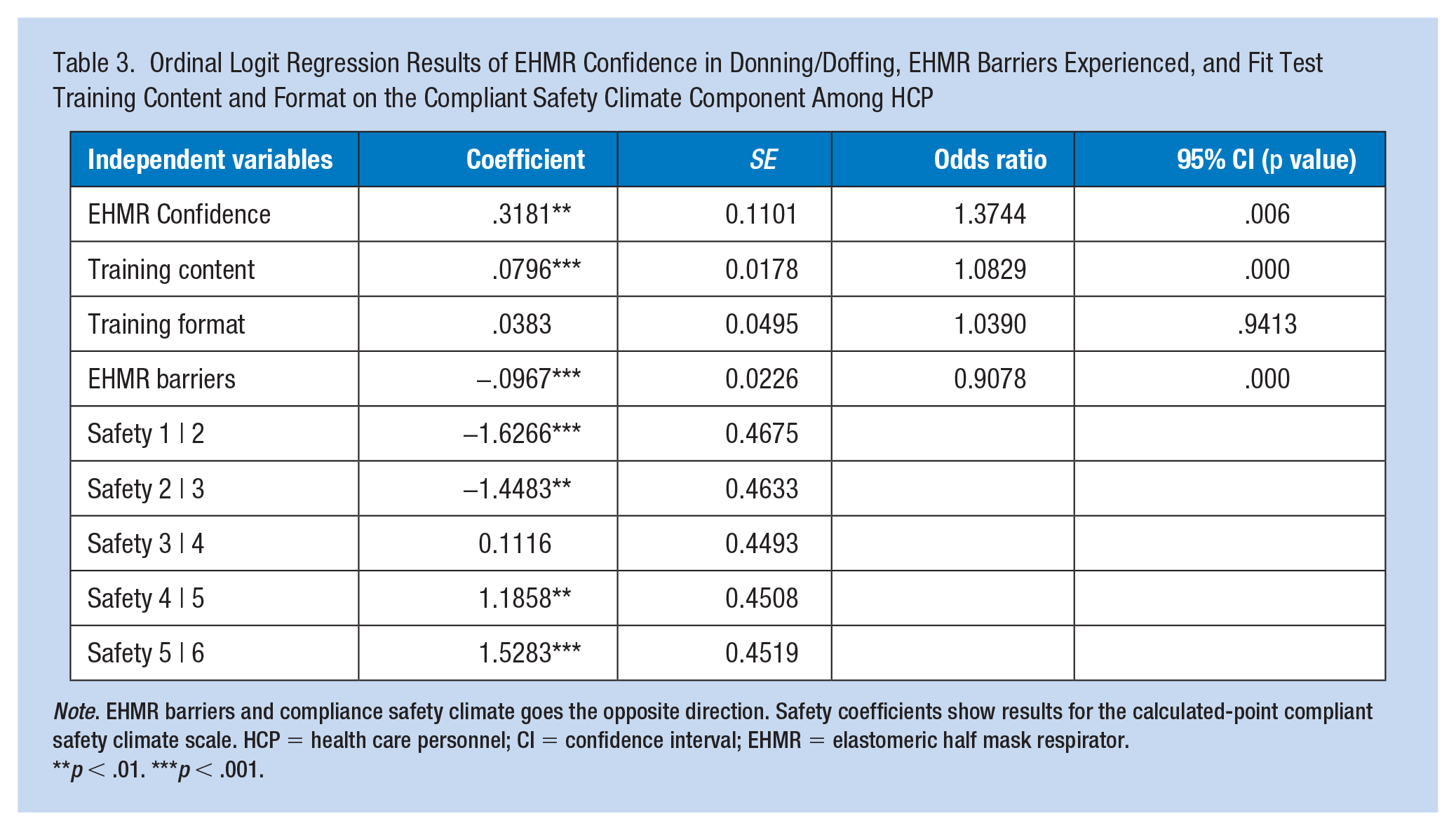
Note. EHMR barriers and compliance safety climate goes the opposite direction. Safety coefficients show results for the calculated-point compliant safety climate scale. HCP = health care personnel; CI = confidence interval; EHMR = elastomeric half mask respirator.
p < .01. ***p < .001.
Table 3 shows that the odds of HCP perceiving a positive, compliant safety climate in their organization; increase by 37% for each one-unit increase in Confidence, holding all other variables constant; increase by 10% for a one-unit increase in Training content; and decrease by 9% for each one-unit increase in EHMR barriers experienced, holding others constant.
Discussion
Research has demonstrated that increased proactivity or participation in training can be attributed to a strong safety climate (e.g., Griffin & Neal, 2000; Morrison et al., 1997). Other studies have shown the interdependence of training efforts and safety climate perceptions (McDonald et al., 2020). These results are no different in showcasing similar interdependencies of knowledge, skill building, and safety climate. Specifically, user confidence, training content, and in some cases training format were associated with the likelihood of a positive safety climate. On the contrary, cumulative barriers experienced while using an EHMR were negatively associated with HCP perceptions of safety climate. These results are important for several reasons. First, they show the importance of seeking ways to improve current EHMR designs to remove some of these barriers to use. Manufacturers can use these results and aim to improve aspects of fit and comfort. Second, measuring the safety climate within an organization is achievable, but making changes to processes, practices, and policies to improve worker perceptions is a bigger challenge on behalf of organizations and discussed more below.
Previous studies have offered broad recommendations such as improving leadership efforts or engaging HCP in safety activities or leadership rounds (Joint Commission, 2014; Peterson et al., 2016; Wizner et al., 2018). While such efforts can improve a culture over time, the current results show that concrete programs and initiatives can positively influence safety climate perceptions in a shorter time span, which can subsequently support participation in consistent PPE practices among HCP. Consequently, there are areas in which health care administrators, infection prevention and control specialists, and respiratory protection program managers can focus on prior to integrating PPE into the work environment. Specifically, the predictors used in this analysis reveal the importance of accurate training and resources and successfully relaying this information to HCP not only to build confidence in using EHMRs but also to create realistic expectations with their use.
Implementation Practices to Support HCP EHMR Confidence and Use
First, respondents had a high perceived confidence in donning and doffing their EHMRs. Despite the overall high average, however, the results were notable in showing that a one-unit change in HCP confidence in EHMR use significantly increased perceptions of safety climate by a higher percentage than the other study antecedents (31% for proactive metrics and 37% for compliant metrics). The HCP confidence was positively associated with both the proactive and compliant safety climate scales, underscoring the value of competency building prior to implementing respiratory protection. From a proactive safety climate standpoint, the results illustrate the importance of visible commitment to safety in the form of training quantity and quality to support HCP initiating and effectively sustaining respirator use on the job.
Regarding the compliance safety climate scale, these questions probed supervisors finding and correcting absent or improper use of respiratory protection. Other studies have shown that when lapses in respiratory protection protocols occur in hospitals, HCPs are more likely to assimilate to a lax culture (Fix et al., 2019). It is likely that the in-depth trainings provided in the current study, as rated by respondents, impacted the perceived priority toward safety modeled by the two hospital systems, including the diligence to enforce procedures discussed during the training.
Although previous research has developed training related to EHMR fit testing to include an overview of donning and doffing (e.g., Pompeii et al., 2020), incorrect doffing of respiratory protection can increase HCP and patient risk of exposure and infection (Phan et al., 2019), making this skill especially important to achieve prior to respirator use in the workplace. Research has shown that interactive training for teaching respiratory protection and other occupational safety and health information is more effective (Eckerman et al., 2002), although the results were not as conclusive on training format in the current study. Nonetheless, taking the time to provide detailed respiratory protection training prior to implementation has been recommended to improve user confidence (Eckerman et al., 2002; Rohlman et al., 2005) and is an important takeaway from the current results.
Specific to EHMRs, the NAS (2019) summarized additional implementation recommendations for on-the-job and just-in-time EHMR training. One vetted idea was to use practice champions to normalize the use of respiratory protection. Practice champions have been shown to be an effective tool for RPPs and their implementation (Rogers et al., 2009; Shaw et al., 2012) and it is possible this visible sign of organizational support for respiratory protection may prevent mental health stressors among HCP and improve confidence in the respiratory protection being offered (SøVold et al., 2021). In addition to practice champions, leadership safety values and actions are important to show that respiratory protection is a cultural norm and priority for the organization (NAS, 2019).
The results of this research must be considered within its current limitations. First, the two hospital systems that participated in this research study had already implemented EHMRs proactively at a time when very few hospital systems had done so. This proactive initiative implies these sites may already value safety climate. Similarly, the sample within the two hospitals was voluntary and is subject to self-selection bias. Those who volunteered to participate likely already have a priority toward safety, which is probably in part why the safety climate results were highly skewed and needed to be recategorized. It is possible that nonrespondents had varying views of EHMRs that may have swayed the results in some capacity.
Finally, some of the possible EHMR barriers are subject to inherent bias to the outcome being based on their job tasks (e.g., communicating with residents) or physical characteristics (e.g., wear glasses or bald). Future research should not only aim to recruit additional locations and respondents that have more diverse experiences with EHMRs but also control for some of these physical characteristics. Along these same lines, responses are subject to social desirability bias and should be considered a limitation of the data. In addition, due to the limited sample, these study results cannot be generalized to EHMR perceptions in general nor other types of respiratory protection. Finally, researchers did not aim to demonstrate equivalence in demographic distributions among the occupations nor the two hospital systems, which can be further explored in follow-up analyses to look for significant differences to inform future interventions.
Implications for Occupational Health Nursing Practice
There are several processes associated with integrating new or different forms of respiratory protection into the workplace, such as training provided to HCP, initial and cumulative experiences with the respiratory protection, and how these factors may influence subsequent behaviors. This study identified potential relationships between EHMR training experiences, confidence in use, and cumulative barriers experienced during use on HCP perceptions of safety climate. Despite the limitations to this study, there are useful takeaways that pose new implications for occupational health nursing practice. Specifically, previous research has shown that HCP may decide not to wear respiratory protection due to minimal exposure, respirators not being provided by their employer, and that others in their work area do not wear them (Wizner et al., 2018). However, with an increase of HCP exposure risks on the job, temporary protocols in place requiring respiratory protection, and the widespread distribution of respiratory protection, these barriers were not applicable for the current sample. Therefore, this study, which utilized the activities associated with implementing workplace respiratory protection (i.e., EHMRs) as predictors of perceived safety climate, helps explain more recent perceptions and trends among HCP and what organizations can do to support these perceptions.
First, these results show that the implementation of new respiratory protection can create concerns among employees, making their experiences invaluable to introduce any new PPE effectively and efficiently. In the current study, as HCP encountered more barriers during EHMR use (e.g., moisture buildup, difficulty communicating, facial irritation), their negative perceptions of the safety climate increased. This result is not surprising, as other studies have shown that if PPE interferes with patient care, HCP compliant use is likely to suffer (Hines et al., 2020). Similarly, another study (Radonovich et al., 2009) concluded that new respirator designs were likely needed to improve HCP tolerability during long work shifts and is another area that deserves further exploration in light of the COVID-19 pandemic. Specifically, given HCP recent and increased access to EHMRs, additional research and development efforts should be supported that address the EHMR barriers being experienced among end users in health care. Addressing these barriers will not only make the increased use of EHMRs in health care more sustainable but may also significantly improve the system’s safety climate.
The development of additional EHMR models may be difficult for manufacturers at this specific point in time given the variety of new models without exhalation valves or with filtered exhalation valves that have recently been developed (Fernando et al., 2021). Regardless of current capacity, however, the results provide a call to action to consider. For example, perhaps these results provide an impetus for new entrepreneurs to enter this space or for the government to provide additional research and development support to give confidence that changes to manufacturing or production lines will yield meaningful results regarding end-user adoption. Such research may also open additional avenues of research to study the confidence that HCP and other end users have in NIOSH-approved respiratory protection.
In summary, these results further support and prompt the need to consider realistic expectations training and communication to HCPs when they receive and are fit-tested for new types of respiratory protection. Because respirator types and their individual fit are different for each person, realistic expectations about comfort and potential barriers to expect are important to know before consistent use. Future interventions and training may need to include not only the benefits, but also the common barriers experienced with types of PPE, and EHMR comfort, specifically, to avoid HCP doubt upon initial use. Unexpected negative experiences may impact HCP perceptions toward the organization’s commitment to safety. Overall, findings demonstrate that efforts to improve confidence in respirator use and training formats as well as future designs to reduce barriers to use are all high-yield targets to bolstering safety climate.
Applying Research to Occupational Health Practice
As elastomeric half mask respirators (EHMRs) become a more common type of respiratory protection used in health care settings, understanding the impact this respiratory protection has on employee experiences and perceptions becomes more critical, regardless of whether we are in a pandemic or not. In the current study, as health care personnel (HCP) encountered more barriers during EHMR use (e.g., moisture buildup, difficulty communicating, facial irritation), their negative perceptions of the safety climate increased, whereas an increase in user confidence and training perceptions was associated with an increase in safety climate. Health care organizations should consider ways that their current respiratory protection plans, and complementary training can be enhanced to support HCP experiences with EHMRs. Examples may include realistic expectations training and communication to HCPs when they receive and are fit-tested for new types of respiratory protection, as well as the use of champions on site to support the knowledge base and mastery of using EHMRs. Such activities may help avoid HCP doubt upon initial use and help the organization visibly demonstrate its commitment to safety.
Supplemental Material
sj-docx-1-whs-10.1177_21650799231164783 – Supplemental material for Examining the Impact of Elastomeric Half Mask Respirator Knowledge and User Barriers on Safety Climate Perceptions in Health Care Settings
Supplemental material, sj-docx-1-whs-10.1177_21650799231164783 for Examining the Impact of Elastomeric Half Mask Respirator Knowledge and User Barriers on Safety Climate Perceptions in Health Care Settings by Emily J. Haas, Katherine Yoon, Caitlin McClain, Margaret Sietsema, Adam Hornbeck, Stella Hines, Sricharan Chalikonda, Sara Angelilli, Hope Waltenbaugh, Paul Thurman PhD, Meghan Napoli and Rohan Fernando in Workplace Health & Safety
Footnotes
Author Contributions
All authors had substantial contribution to the completion of this manuscript to include the design of the work, acquisition of data, data analysis, and/or interpretation of the data and drafting the work or revising it critically for important intellectual content. All authors gave final approval of this submitted version.
Conflict of Interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Disclaimer
The findings and conclusions are those of the authors and do not necessarily represent the official position of the National Institute for Occupational Safety and Health, Centers for Disease Control and Prevention.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Institutional Review Board (IRB) Approval
Two separate facilities conducted this study, and each had their own IRB review the protocol of the study to occur at their location. The Institutional Review Board of Allegheny Health Network found the study exempt from IRB review (reference # 2021-034), and the University of Maryland, Baltimore (UMB) Institutional Review Board also ruled this study exempt from IRB review (reference #HP-00094424).
Human Subjects Review
The study was conducted at two different sites, and each site’s IRB reviewed the protocol for the work done at their respective location. Alleghany Health Network Research Institute’s IRB provided a certificate of exemption (2021-034 “Healthcare Worker Survey on Elastomeric Masks”), dated February 22, 2021, and the University of Maryland Baltimore’s IRB provided letter of exemption as well (HP-00094424), dated January 26, 2021.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.