
Abstract
The purpose of this study was to identify factors predicting occupational health nurses’ provision of smoking cessation services. Data were collected via a self-administered questionnaire distributed to 254 occupational health nurses in Thailand. Analysis by structural equation modeling revealed that self-efficacy directly and positively influenced smoking cessation services, and mediated the relationship between workplace factors, nurse factors, and smoking cessation services. The final model had good fit to the data, accounting for 20.4% and 38.0% of the variance in self-efficacy and smoking cessation services, respectively. The findings show that self-efficacy is a mediator that influences provision of smoking cessation services by occupational health nurses. Interventions to enhance nurses’ self-efficacy in providing smoking cessation services are expected to promote provision of smoking cessation services to workers.
Smoking is harmful due to its adverse effects on the health of smokers as well as those who inhale smoke secondhand. In Thailand, a National Statistical Office survey has shown that 10.7 million (19.9%) residents ages 15 years or older are cigarette smokers. Those of working age (25-59 years) have the highest rate of smoking (22.8%; The National Statistical Office of Thailand, 2013). Tobacco products used by residents ages 15 years or older are primarily either manufactured or hand-rolled cigarettes (49.6% and 47.0%, respectively). Pipes are less commonly used (0.3%; The National Statistical Office of Thailand, 2011). Workplaces commonly allow smoking, and smoking by cigarette-addicted employees is also common (Keeratiwiriyaporn, 2009). Several studies have shown that employees who smoke are more likely to be absent from work and exhibit less productivity than non-smoking workers (Bush & Wooden, 1995; Tsai, Wen, Hu, Cheng, & Huang, 2005; Weng, Ali, & Leonardi-Bee, 2013). Alarmed by the scientific evidence about smoking hazards, the Thai government has issued laws and regulations that prohibited smoking in the workplace (except in designated areas) to protect the health and rights of non-smokers. However, according to a survey of 74 workplaces in Thailand, some surveyed employees reported they still smoke outside the designated areas (e.g., rest rooms, near dining areas, parking areas, and outdoor areas; Keeratiwiriyaporn, 2009).
Not only has the Thai government issued smoking bans in public places, the government supports a variety of smoking cessation services in health care centers and through telephonic counseling (quit line). These services are provided by health care professionals, most commonly nurses. Nurses assist patients learn about health and other benefits of smoking cessation (Sarna & Bialous, 2013). In addition to expertise in health education and behavior change, very few Thai nurses smoke (Preechawong et al., 2014), making them role models for health promotion and the logical choice of provider for accessible and effective workplace smoking cessation services. To reduce hazards related to tobacco exposure and protect the health of employees, current practice guidelines recommend use of a smoking cessation intervention algorithm (i.e., Ask, Advise, Assess, Assist, Arrange, or 5 A’s; Fiore et al., 1996).
Variables Related to Smoking Cessation Services Provided by Nurses
Based on several prior studies (Leitlein, Smit, de Vries, & Hoving, 2013; Shelley et al., 2014), both workplace and nurse factors are known to influence the provision of smoking cessation services. Workplace factors known to influence smoking cessation services include the number of employees (Sindhu, Konggumnerd, & Wiwattanacheewin, 2014), number of smoking employees (Sarna et al., 2009), perceived organizational support (Davies, Edwards, Ploeg, & Virani, 2008), organizational policy (Braun et al., 2004), and number of health care providers (Sukbua, Kalampakorn, Kaewpan, & Powwattana, 2009).
Nurse factors known to influence smoking cessation services include seniority (Johnson et al., 2009; Sarna, Wewers, Brown, Lillington, & Brecht, 2001), education (Good, Frazier, Wetta-Hall, Ablah, & Molgaard, 2004; Gorin & Heck, 2004; Hall, Vogt, & Marteau, 2005; McEwan & West, 2001; Nagle, Schofield, & Redman, 1999; Sarna et al., 2001; Schultz, 2003), employment status (Silpasuwan, Viwatwongkasem, Phalee, & Kalampakorn, 2006; Sukbua et al., 2009), positive attitude toward smoking cessation services (Puffer & Rashidian, 2004), and in-service education and training (Borrelli et al., 2001; Wetta-Hall et al., 2005).
In addition, several barriers related to the provision of smoking cessation services have been identified, particularly barriers related to nurses’ role. Members of the American Association of Occupational Health Nurses (AAOHN) reported that they did not have necessary training or guidelines to provide smoking cessation services in their workplaces (Ganz & Campbell, 2015). Likewise, Thai nurses reported they lacked time, training, skills, and confidence for providing smoking cessation services (Preechawong, Vathesathogkit, & Suwanratsamee, 2011; Srimoragot, 2009).
Conceptual Framework
Self-efficacy, individuals’ perceptions of their own abilities to produce particular levels of performance, influences how individuals feel, think, and motivate themselves to engage in particular behaviors (Bandura, 1994). The concept of self-efficacy has been tested cross-culturally, and a relationship between self-efficacy and clinical skills (e.g., counseling ability) has been established (Bambini, Washburn, & Perkins, 2009; Goldenberg, Andrusyszyn, & Iwasiw, 2005; Preechawong et al., 2011).
In addition, Guo, Wang, and Shu (2015) examined a number of variables related to nurses’ (i.e., not limited to occupational health nurses) self-efficacy for providing smoking cessation services in Taiwan. Results revealed that relevant factors included perceived provider-related barriers in providing smoking cessation services, exposure to tobacco smoke in the workplace, nurses’ attitudes toward patient smoking, and nurses’ frequency and practical experience in providing smoking cessation services (Guo et al., 2015). Although factors related to self-efficacy have been demonstrated, the role of self-efficacy in predicting the provision of smoking cessation services by occupational health nurses has never been explored.
According to the Self-efficacy Theory, efficacy beliefs can change depending on the particular circumstance, the task, or prior experience (Bandura, 1977). To apply this concept to nurses’ provision of smoking cessation services in the workplace, self-efficacy was hypothesized to influence smoking cessation services directly. It has been inferred that workplace factors and nurse factors could influence directly and positively the self-efficacy of nurses smoking cessation services, and influence their provision of smoking cessation services directly and indirectly. The purpose of this study was to identify factors predicting occupational health nurses’ provision of smoking cessation services. This information will be useful in developing programs to enhance the effectiveness of workplace smoking cessation services.
Methods
This cross-sectional study surveyed registered occupational health nurses in the Bangkok, Thailand metropolitan region including the cities of Bangkok, Nonthaburi, Nakhon Pathom, Pathum Thani, Samut Prakan, and Samut Sakhon. Thai legislation requires that workplaces with 200 or more employees must employ at least one nurse to provide health services onsite (Ministry of Labour, 2009). A total of 420 industrial workplaces with at least 200 employees were randomly selected from the 1,647 workplaces registered through the Ministry of Industry. One registered nurse with at least 1 year of experience providing occupational health services from each selected workplace was invited by mail to participate in the study. Of the 262 nurses (62.38%) who responded, 254 provided adequate responses for data analysis.
The Ethical Review Committee for Human Research, Faculty of Public Health, Mahidol University, Bangkok, approved the study. All participants provided informed consent before participating in this study and none received any compensation for participation.
Measures
Workplace factors
Workplace factors were measured by questions about the number of employees, number of employees who smoke, and number of nurses per shift at each workplace. Employer support was measured by a single item, “Does your administrator support tobacco control?” with four response categories (highly support, moderately support, little support, and not at all). Each workplace tobacco control policy had several dimensions: organizations with smoking cessation services policies, publicizing policies, establishing a committee responsible for smoke-free policies, and providing designated smoking areas. The presence of these factors was measured by six items with yes and no responses. Sum score was used; a higher score indicated having a more well-developed tobacco control policy.
Nurse factors
Nurse factors were measured by querying respondents about age, gender, education, smoking status, employment status, years of nursing experience, occupational health nursing experience, experience in providing smoking cessation services, and smoking cessation services training.
Attitudes about smoking cessation services were measured by an instrument modified from a survey used by Sarna and colleagues (2014). Participants were asked for their opinions about smoking employees, workplace tobacco control policies, nurses’ roles in smoking cessation services, and smoking cessation interventions (i.e., Ask, Advise, Assess, Assist, Arrange). These factors were assessed by 15 Likert-scale items with five response categories (strongly agree, agree, unsure, disagree, and strongly disagree). Higher scores indicated more favorable attitudes toward smoking cessation services.
Self-efficacy related to smoking cessation services was measured by assessing the extent to which nurses were confident in providing smoking cessation interventions (i.e., 5As). Likert-scale items (n = 10) with five response categories (not at all confident to extremely confident) were used; higher scores indicated greater self-efficacy.
Providing smoking cessation services
Providing smoking cessation services included nurses’ self-report of the frequency of providing smoking cessation interventions (i.e., 5As). This variable was assessed by a 10-item scale with five response categories (always, often, sometimes, rarely, and never). Higher scores indicated more frequent provision of smoking cessation services. A sample item from this instrument is, “How frequently do you assist the employee who is ready to quit smoking to set a quit date in the next 30 days?”
The instrument measuring participants’ self-efficacy regarding smoking cessation services was modified from a similar instrument used with hospital nurses (Preechawong et al., 2011); item wording was changed so the questions were more relevant to the work setting.
The instruments were reviewed for validity by three experts and subsequently revised. The revised questionnaire was then pilot tested with 30 occupational health nurses. This instrument administration confirmed that the questionnaire items were unambiguous and appropriate for a self-administered questionnaire. Selected components of the questionnaire (i.e., attitudes about smoking cessation services, self-efficacy related to smoking cessation services, and provision of smoking cessation services) were examined for internal reliability using Cronbach’s alpha. Internal reliability ranged from .839 to .962, and was deemed adequate for this study. The final survey was administered from August to October, 2015.
Analysis
Data were analyzed using SPSS V.18.0 and AMOS 18.0. Missing values and basic assumptions related to AMOS were checked before initiating the analysis. All the study variables showed normal distribution patterns with measures of skewness and kurtosis between ± 2 (George & Mallery, 2010).
Descriptive statistics (i.e., percentage, mean, standard deviations) were calculated for workplace characteristics, nurse characteristics, attitudes, self-efficacy related to smoking cessation services, and provision of smoking cessation services.
Pearson’s correlation was used to examine the relationships between study variables to establish how study variables affected each other and assist in developing the initial model. Path analysis was used to estimate a system of equations in which all of the variables were observed. The lowest Akaike information criterion (AIC), a statistic for parametric models for which parameters were established by maximizing a form of likelihood, was used to select the final model (Akaike, 1973).
Mediation, a hypothesized causal chain in which one variable affects a second variable that, in turn, affects a third variable, was tested using the causal steps approach (Baron & Kenny, 1986). In this approach, the initial predictor is associated with the outcome and proposed mediator; the mediator is associated with the outcome; and the initial predictor is associated with the outcome.
Results
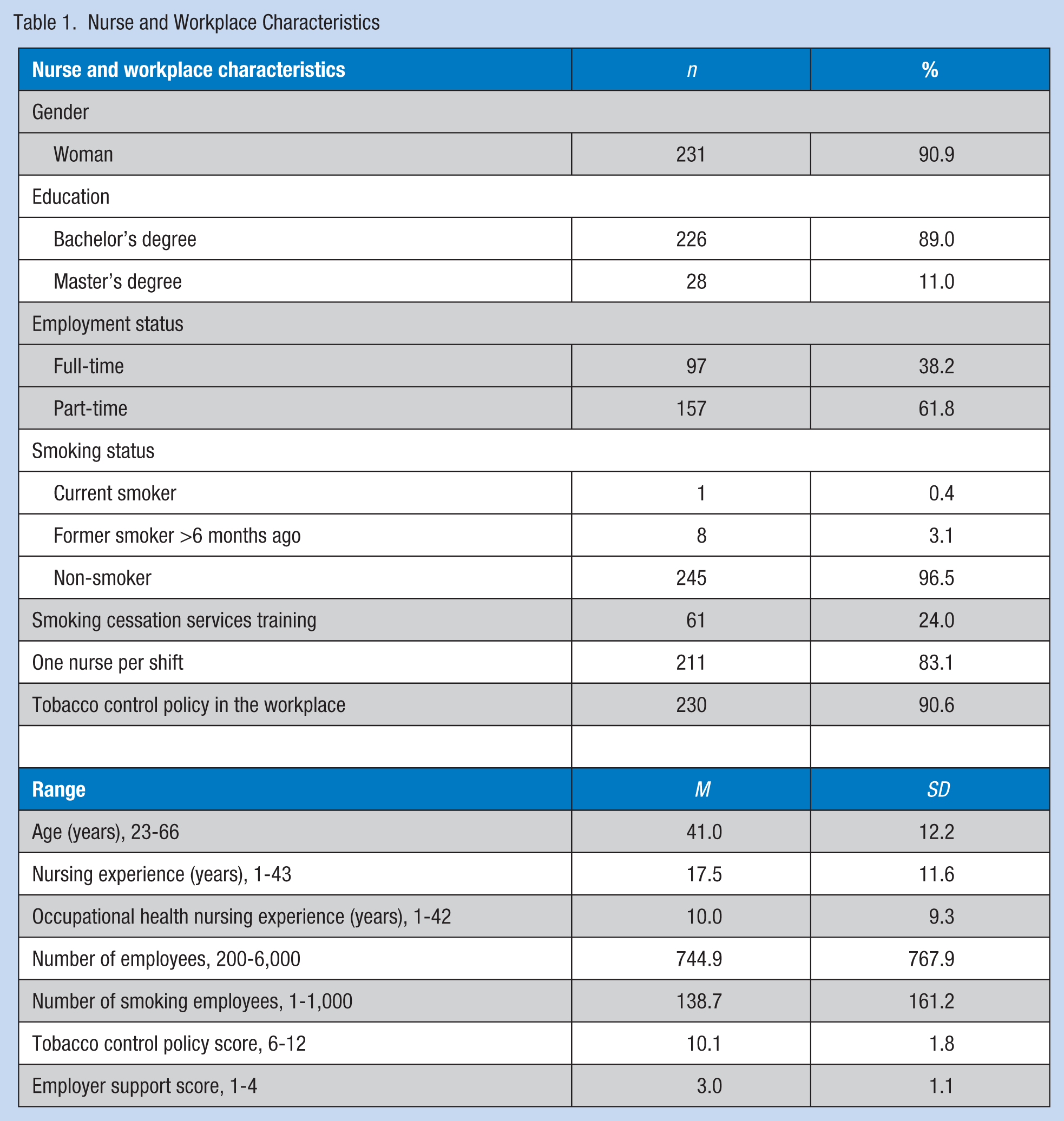
Most of the respondents were female (90.9%) with a bachelor’s degree in nursing (89.0%). Participants ranged in age from 23 to 66 years, with a mean age of 41 years. The average nursing experience was 17.5 years; average experience in occupational health nursing was 10 years. The majority (61.8%) of the participants were part-time workers, with 43.1% working fewer than 10 days per month. Overwhelmingly, most respondents (96.5%) did not smoke. Only 24% of the participants reported smoking cessation services training. Most of the participants (90.6%) worked in companies with tobacco control policies. The nurse and workplace characteristics of the respondents are presented in Table 1.
Nurse and Workplace Characteristics
Relationships between study variables were examined using Pearson correlation coefficients (Table 2). Most independent variables were significantly correlated with self-efficacy and provision of smoking cessation services. As expected, tobacco control policy (r = .237, p < .01), employer support (r = .249, p < .01), smoking cessation services training (r = .189, p < .01), and attitude toward smoking cessation services (r = .380, p < .01) were positively related to nurses’ self-efficacy in providing smoking cessation services. In addition, tobacco control policy (r = .304, p < .01), employer support (r = .313, p < .01), smoking cessation services training (r = .232, p < .01), and self-efficacy (r = .587, p < .01) were positively related to nurses’ provision of smoking cessation services.
Pearson Correlation Coefficients Matrix of Study Variables
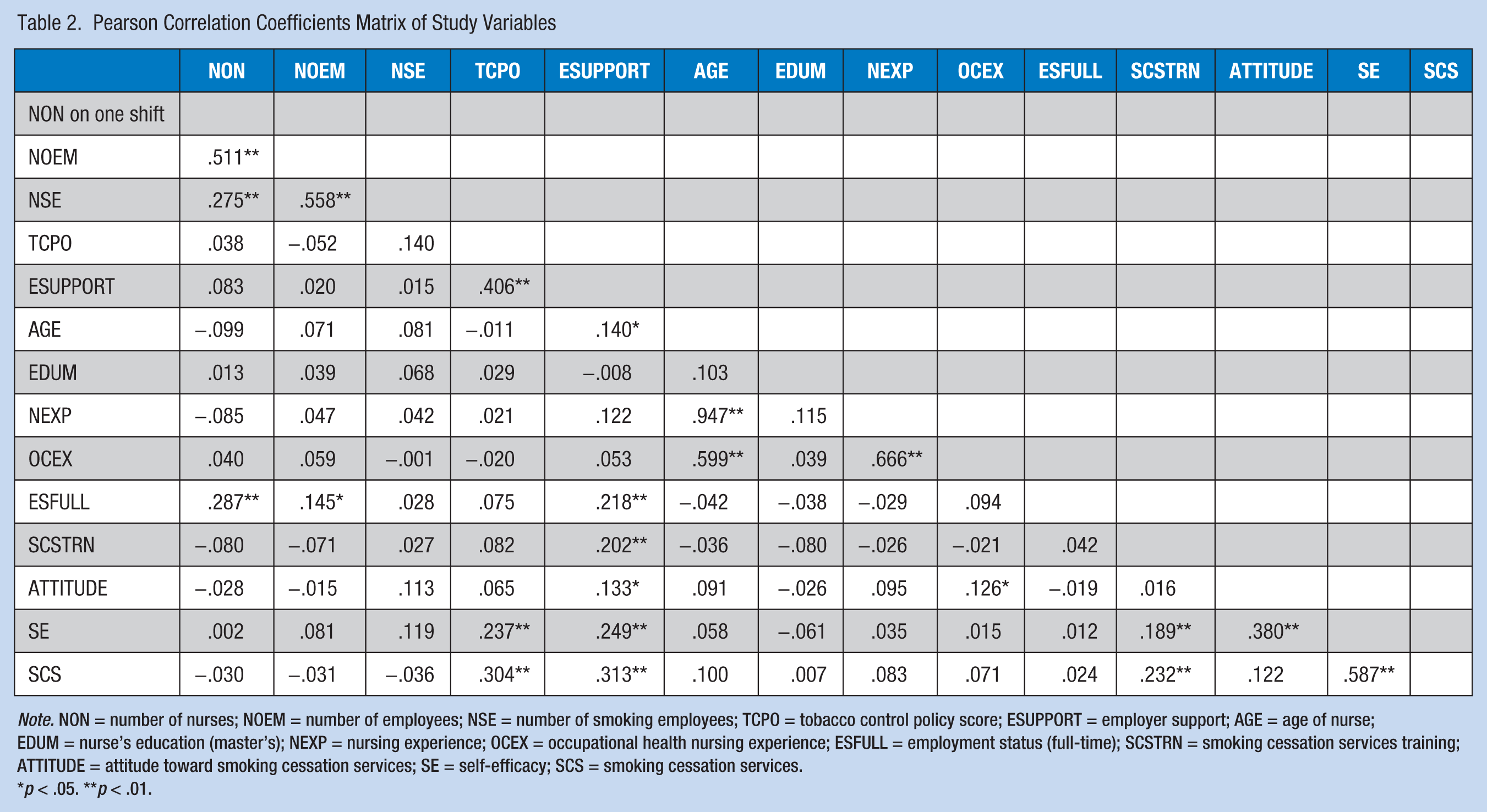
Note. NON = number of nurses; NOEM = number of employees; NSE = number of smoking employees; TCPO = tobacco control policy score; ESUPPORT = employer support; AGE = age of nurse; EDUM = nurse’s education (master’s); NEXP = nursing experience; OCEX = occupational health nursing experience; ESFULL = employment status (full-time); SCSTRN = smoking cessation services training; ATTITUDE = attitude toward smoking cessation services; SE = self-efficacy; SCS = smoking cessation services.
p < .05. **p < .01.
Construction of the Model
Variables significantly correlated with providing smoking cessation services were used to construct the model (Figure 1). This model demonstrated a good fit to the data (χ2 = 10.53, [p = .062], GFI = .99, AGFI = .94, NFI = .96, comparative fit index [CFI] = .98, root mean square error approximation [RMSEA] = .06, AIC = 42.53), accounting for 20.4% and 38.0% of the variance in self-efficacy and smoking cessation services, respectively, and was the best fit of all models tested (Table 3).
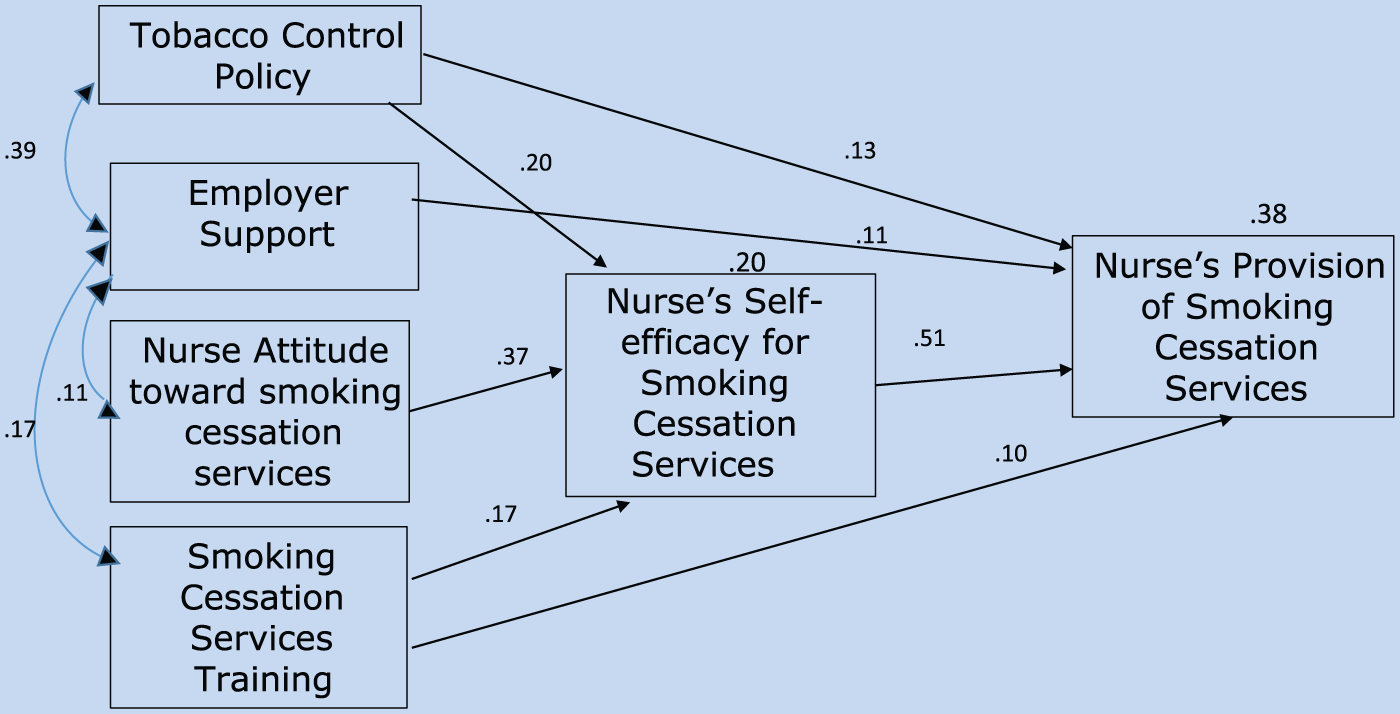
Nurses’ smoking cessation services model.
Goodness of Fit Indices for Model
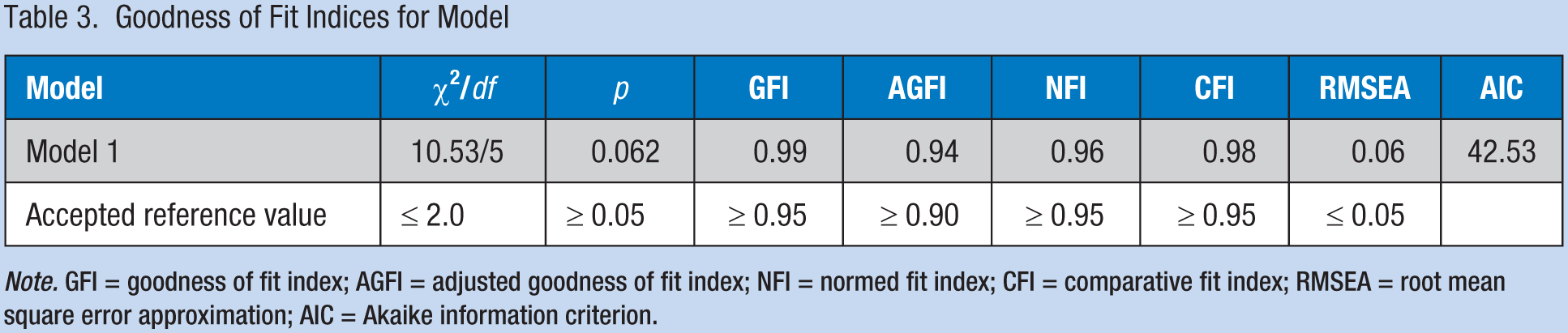
Note. GFI = goodness of fit index; AGFI = adjusted goodness of fit index; NFI = normed fit index; CFI = comparative fit index; RMSEA = root mean square error approximation; AIC = Akaike information criterion.
As expected, self-efficacy was positively related to providing smoking cessation services (β = 0.51, p < .05), and mediated some nurse factors and workplace factors that predicted provision of smoking cessation services. The standardized beta for the direct path from smoking cessation services training to smoking cessation services was 0.10 (p < .05), indicating partial mediation of self-efficacy having influence on smoking cessation services; the standardized beta for the direct path from tobacco control policy to smoking cessation services was 0.13 (p < .05), indicating partial mediation of self-efficacy. In addition, the standardized beta for the direct path from attitude about smoking cessation services to self-efficacy related to smoking cessation services was 0.37 (p < .05), but was not related to smoking cessation services, indicating full mediation of self-efficacy. The direct path from employer support to smoking cessation services was significant (β = 0.11, p < .05).
Discussion
A proposed model of interrelationships among three factors and provision of smoking cessation services by occupational health nurses was tested. The authors hypothesized that (a) workplace factors (i.e., number of employees, number of employees who smoked, employer support, tobacco control policy, and number of nurses per shift) and (b) nurse factors (i.e., age, education, employment status, nursing experience, occupational health nursing experience, smoking cessation services training, and attitude toward smoking cessation services) would directly influence self-efficacy related to smoking cessation services and providing smoking cessation services; and (c) nurses’ self-efficacy for providing smoking cessation services would directly influence providing smoking cessation services and mediate the relationships between workplace factors and nurse factors and providing smoking cessation services.
A model describing nurses’ performance in this area was constructed, and tested using structural equation modeling. The resulting model included five variables (i.e., tobacco control policy, employer support, smoking cessation services training, attitudes toward smoking cessation services, and self-efficacy toward smoking cessation services) predicting occupational health nurses’ provision of smoking cessation services.
Self-Efficacy as a Mediator to Providing Smoking Cessation Services
Nurses’ self-efficacy related to providing smoking cessation services was a key mediator in the model, and was directly and positively related to provision of smoking cessation services. This finding supported Bandura’s proposition that self-efficacy provides the foundation for human motivation (Bandura, 1986). In addition, the mediating role of self-efficacy was supported by workplace factors (i.e., tobacco control policy), nurse factors (i.e., smoking cessation services training, attitudes toward smoking cessation services), and provision of smoking cessation services. Self-efficacy has been found to play a mediating role not only in nurse-provided smoking cessation services, but also services focused on other health-promoting behaviors provided by other health care providers. For instance, self-efficacy played a mediating role for nurse delivery of weight management services (Zhu, Norman, & While, 2013), and self-efficacy mediated the relationship between feelings of empowerment and nursing practice (Manojlovich, 2015). In addition, self-efficacy was highly correlated with providing smoking cessation services among psychiatric nurses (Guo et al., 2015).
Tobacco Control Policy and Employer Support as Significant Workplace Factors
Although several variables were predicted to be positively related to self-efficacy (e.g., number of employees, number of employees who smoke, employer support, tobacco control policy, and number of nurses per shift), only tobacco control policy and employer support were included in the final model. In this model, tobacco control policy directly and positively influenced self-efficacy, and indirectly and positively influenced smoking cessation services. Employer support directly and positively influenced smoking cessation services. This finding suggests that occupational health nurses who work in settings with tobacco control policies and employer support were more likely to provide smoking cessation services.
It is interesting that employer support directly and positively influenced provision of smoking cessation services by nurses, but did not influence self-efficacy. This finding indicates that those occupational health nurses who work in settings that have employer support were more likely to provide smoking cessation services than those without support. These findings are consistent with a study by Mosadeghrad (2014) that indicated health care quality can be improved by supportive leadership, proper planning, and effective resource management. However, a study by Caesens, Marique, Hanin, and Stinglhamber (2015) found that self-efficacy partially mediates the relationship between perceived organizational support and work engagement.
Nurse Training and Attitudes Predict Providing Smoking Cessation Services
Age, education, employment status, nursing experience, and occupational health nursing experience did not predict nurses’ self-efficacy in providing smoking cessation services. This finding was similar to the results of Guo et al. (2015) and Wetta-Hall et al. (2005), who found that age, education, and seniority of psychiatric nurses were not significantly correlated with their self-efficacy in providing smoking cessation services.
However, study results differed from those of Johnson et al. (2009), who stated that mental health care providers with more seniority exhibited more confidence in providing smoking cessation services. This finding might have been due to the fact that the nurse participants in the Johnson et al. (2009) study included 44.2% paraprofessional members in addition to professional nurses.
The results from this study showed that only two nurse factors (i.e., smoking cessation training and attitude toward smoking cessation services) predicted provision of smoking cessation services, and positively influenced self-efficacy. However, smoking cessation services training and smoking cessation attitudes also directly and positively influenced self-efficacy, indicating that those nurses with smoking cessation training and positive smoking cessation attitudes were more likely to be confident in their ability to provide smoking cessation services. This result was consistent with a study by Zhu et al. (2013) that reported perceived skills and training directly and positively influenced self-efficacy related to the provision of weight management services.
Limitations
Several study limitations merit consideration. First, although using a standardized instrument to assess smoking cessation services would add strength to the methods used in this study, the instruments were tested for psychometric properties (Casado & Thuler, 2015; Preechawong et al., 2011) and developed for health care facilities with multidisciplinary health care providers but not appropriate for use in the workplace. Resulting modifications of the original instrument limit comparisons of findings with previous studies. Second, the questionnaires were mailed to nurses at their workplaces, which led to some lost surveys and consequent reduction in sample size. Also, the study was conducted exclusively in Thailand; influencing factors may differ in other countries. Due to the cross-sectional descriptive nature of the study, causal inferences cannot be made.
Conclusions and Recommendations
This study identified workplace and nurse factors that predict occupational health nurses’ provision of smoking cessation services. The findings confirmed that self-efficacy theory is a relevant framework for understanding the relationship among workplace factors, nurse factors, and smoking cessation services. Workplace factors (i.e., employer support) directly and positively influenced smoking cessation services. Another workplace factor, tobacco control policy, directly and positively influenced self-efficacy, and indirectly and positively influenced smoking cessation services. Attitudes toward smoking cessation services directly influenced self-efficacy for provision of smoking cessation services; training influenced smoking cessation services directly as well as indirectly through self-efficacy. These findings suggest some factors (i.e., tobacco control policy and smoking cessation services training) can be modified to increase nurses’ self-efficacy and provision of smoking cessation services. Therefore, employer support via tobacco control policies, emphasizing smoking cessation services for employees, and smoking cessation services training for nurses could increase provision of smoking cessation services in the work setting.
The findings from this study suggest that interventions to increase nurses’ self-efficacy in providing smoking cessation services can be expected to enhance smoking cessation services. Consequently, development of Thai national policy directing creation and implementation of a smoking cessation services curriculum for baccalaureate nursing education and continuing nursing education can be expected to increase nurses’ knowledge and skills, and subsequently their self-efficacy in providing smoking cessation services in the workplace.
Given the benefits of training programs, effective smoking cessation services training programs for occupational health nurses should be developed, particularly in countries with high rates of smoking. Measures to improve service efficacy may also benefit provision of quality smoking cessation services which may include direct observation of smoking cessation services.
Applying Research to Practice
Occupational health nurses are in key positions to assist employees to quit smoking. To promote the services provided by occupational health nurses, self-efficacy in smoking cessation services should be enhanced. Training on how to provide smoking cessation services for employees should be developed to assure nurses’ capacity and encourage them to have positive attitudes toward employees who smoke and smoking cessation services. Attitude-based and skill-based training with an emphasis on guidelines for smoking cessation interventions (i.e., 5As) can result in increasing provision of services. In addition, employers should be aware of the benefits of tobacco control measures conducive to smoking cessation including smoke-free policies and designated smoking areas. Employees’ efforts to quit smoking should be supported as cessation not only benefits individuals but also the organization.
Footnotes
Acknowledgements
The authors thank the participating employers and nurses for their cooperation in the distribution and completion of study questionnaires.
Conflict of Interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported in part by the Tobacco Control Research and Knowledge Management Center, a research institute supported by the Thai Health Promotion Foundation.
Author Biographies
Kannikar Chatdokmaiprai is a doctoral student (major in public health nursing), Faculty of Public Health, Mahidol University, Thailand. She is also a nursing instructor at the College of Nursing, Christian University of Thailand.
Surintorn Kalampakorn is associate professor, Public Health Nursing Department, Faculty of Public Health, Mahidol University, Thailand. She is currently the president of the Occupational Health Nurses Association of Thailand and the secretariat of the Nurse Network on Tobacco Control of Thailand.
Marjorie McCullagh is professor and director of the Occupational Health Nursing Program, University of Michigan School of Nursing, USA. She also serves as a director of the University of Michigan Center for Occupational Health and Safety Engineering, which is a NIOSH Education and Research Center (ERC).
Sunee Lagampan is associate professor and head of the Public Health Nursing Department, Faculty of Public Health, Mahidol University, Thailand. She has more than 20 years experience in developing training program for nurses. She has also directed various health services evaluation projects.
Sansanee Keeratiwiriyaporn is secretary-general and program manager, Association for the Development of Environmental Quality (ADEQ), Thailand. She is currently the project manager in workplace health promotion including tobacco control funded by the Thai Health Promotion Foundation.