
Abstract
Background: Previous studies have discovered that the utilization of sliding sheets in patient care is a valuable technique for repositioning bedridden patients compared with traditional cotton sheets or carriers. Our aim was to examine the effects of sliding sheet usage on work-related musculoskeletal disorders and disability, perceived workload, burnout, and job satisfaction, among nurses and nursing assistants. Method: This repeated measurement study included 41 female nurses and nursing assistants from three internal medicine departments who provided direct patient care. Participants completed an eight-part questionnaire (demographics, Neck Disability Index, Quick Disability of the Arms, Shoulder and Hand Questionnaire, Modified Oswestry Low Back Pain Disability Questionnaire, BackAche Disability Index workload, burnout, and job satisfaction) 4 times during the study period: 3 months prior to the intervention, on the first day of the intervention, and 3 and 6 months after commencement of the intervention. Findings: After 3 and 6 months of sliding sheet usage, pain and disability decreased in the neck (p < .001); arms, shoulders, hands (p = .041); and lower back (p < .001), with an increase in job satisfaction (p < .001). Discussion/Application to Practice: The findings of our study indicate a clear influence of reducing work-related musculoskeletal pain and disability while increasing job satisfaction when sliding sheets are introduced into nursing practice. Occupational health nurses in health care should consider this type of low-cost intervention as a method for reducing musculoskeletal injury among direct patient care providers.
Keywords
Background
Health care workers, especially nurses and nursing assistants (Alexopoulos et al., 2011; Lövgren, Gustavsson, Melin, & Rudman, 2014; Ricco, Pezzetti, & Signorelli, 2017; Waters, Collins, Galinsky, & Caruso, 2006), suffer from high rates of musculoskeletal disorders related to patient handling (Andersen et al., 2014). Repositioning bedridden patients to promote comfort and prevent harm caused by continuous lying is a task frequently performed by nurses and nursing assistants (Resnick, 2006; Screfer, 2001). This high-risk activity frequently causes occupational injuries (Fragala, Fragala, & Pontani-Bailey, 2005; Jang et al., 2007; Nelson & Baptiste, 2006), attributed to excessive physical demands on the caregiver, due to the patient’s weight and awkward nursing postures (Nelson & Baptiste, 2006). The risk of injury can be lessened by reducing the friction between the patient and his or her bed. Hence, certain friction-reducing devices have been developed to reduce the manual force required to move these patients (Lloyd & Baptiste, 2006; Theou et al., 2011).
It has been confirmed that the methods (such as single hook method, two-person draw sheet technique) used by nursing personnel significantly affect the musculoskeletal system loading when repositioning a bedridden patient (Bartnik & Rice, 2013; Theou et al., 2011; Weiner, Kalichman, Ribak, & Alperovitch-Najenson, 2015). As repositioning is a frequent task creating a significant risk for work-related musculoskeletal pain (WRMSP) in nurses and nursing assistants (Screfer, 2001), an appropriate mechanical device is essential in assisting patient care, simultaneously preventing potential injuries to both patients and caregivers (Gonzalez, Howe, Waters, & Nelson, 2009; Koppelaar, Knibbe, Miedema, & Burdorf, 2012; Spratt et al., 2012).
In our previous study (Weiner, Kalichman, Ribak, & Alperovitch-Najenson 2017), we compared three different assistive devices aimed at finding an optimal device for reducing musculoskeletal load when moving a bedridden patient. We found that sliding sheets were the most advantageous compared with traditional cotton sheets and special carriers (the carrier was made from synthetic nylon low-friction materials, in an inflexible structure, with ergonomic handles along each side). Previous studies have supported this claim as a part of injury prevention programs (Bartnik & Rice, 2013; Fragala et al., 2005; Theou et al., 2011). Nonetheless, there is still a need to explore ways of implementing the use of the sliding sheet in the workplace, focusing on factors involved in their adoption. As previous studies indicate, the actual use of ergonomic devices is much lower than necessary (Akhtar, Afzal, Kousar, Waqas, & Gilani, 2017; Burdorf, Koppelaar, & Evanoff, 2013; Cole et al., 2006). Koppelaar and colleagues (2012) accredit these findings of little use of ergonomic devices to low availability of the equipment, in addition to lack of time and knowledge.
The aims of this study were to examine the effects of utilizing sliding sheets when repositioning a bedridden patient on WRMSP and disability, perceived workload, burnout, and job satisfaction, among nurses and nursing assistants, and the factors influencing the implementation of sliding sheet use in nursing practice. We hypothesized that utilizing sliding sheets would result in a reduction in pain intensity and improvement of functional ability. Furthermore, the sense of workload, burnout, and job satisfaction would improve after using the sliding sheets.
Method
Study Design and Sample
This was an interventional, prospective repeated measurement study of a convenience sample of nurses and nursing assistants from three internal medicine departments located at the Bnai Zion Medical Center, Haifa, Israel. Participants were included if they were a nonpregnant female who provided direct patient care, with or without musculoskeletal pain. Due to the low number of males in the patient care departments, only women were included in the study. This study was approved by the ethical committees of Bnai Zion Medical Center and Tel-Aviv University, Israel.
The Sliding Sheets
The assistive device used in the study was a reusable tubular cylindrical sliding sheet, 100-cm wide and 120-cm long. The sheet is made of synthetic nylon low-friction materials, facilitating friction between the two nylon layers when moving the patient from above the sheet. The sheet can be laundered at 80°C. The patient is positioned along the length of the sheet while in a supine position.
Data Collection
Study participants were asked to complete an eight-part questionnaire 4 times during the study period: 3 months prior to the intervention (T1), on the first day of the intervention (T2), and 3 and 6 months after the commencement of the intervention (T3 and T4).
Demographics and Working Conditions
Age, family status (married, single, divorced, widower), number of children, number of children <6 years of age, physical exercise, current smoking status, professional education, years in the profession, seniority and job function in the current department, number of shifts (8-hour shifts) per week (morning, evening, and night), and the number of bedridden patients per shift needing repositioning utilizing the sliding sheets.
The Neck Disability Index (NDI) consists of 10 items: pain intensity, personal care, lifting, sleeping, driving, recreation, headaches, concentration, reading, and work. The scores for the 10 items, with six possible answers for each questionnaire, 0 (no activity limitations) to 5 (major activity limitations), were summed up to yield a total score (0-50, with a lower score indicating lower limitations; MacDermid et al., 2009; Shashua, Geva, & Levran, 2016). The NDI has been previously proven as a valid and reliable instrument (Ackelman & Lindgren, 2002; McCarthy, Gravitt, Silcocks, & Hobbs, 2007; Ricco et al., 2017; Smedley et al., 2003) compared with the SF36 questionnaire which was used as the gold standard. The correlations between both questionnaires ranged from .447 to .659 (p < .001; Shashua et al., 2016). The test–retest reliability of the NDI was high (intraclass correlation = .93, 95% confidence limits = [0.86-0.97]). Shashua and colleagues (2016) reported that the Hebrew version of the NDI has good reliability in a test–retest examination, resulting in an intraclass correlation coefficient (ICC) of .888 (p < .001).
The Quick Disability of the Arms, Shoulder and Hand Questionnaire (QDASH) assesses six domains: daily activities, symptoms, social function, work function, sleep, and confidence. It contains two optional four-item modules that evaluate symptoms and function in people whose work requires high physical performance. Responses can range from 1 (no difficulty/not at all/not limited/none/strongly disagree) to 5 (unable/extremely/so much difficulty that I can’t sleep/strongly agree; overall score 0-55, with a lower score indicating better health/function; Beaton & Wilson, 2013; Gummesson, Ward, & Atroshi, 2006). The QDASH has been previously proven as a valid and reliable instrument. Gummesson and colleagues (2006) found that the alpha coefficient for the QDASH exceeded .9 among 34 patients with upper extremity disorders. MacDermid and colleagues (2009) found an almost perfect correlation between the QDASH and Disability of the Arms, Shoulder and Hand Questionnaire (r > .92) among 132 patients with shoulder-related disorders undergoing surgery.
The Modified Oswestry Low Back Pain Disability Questionnaire (OswestryQ) consists of 10 sections: pain intensity, personal care, lifting, walking, sitting, standing, sleeping, sex life, social life, and traveling. The scores for the 10 items, with six possible answers for each section, were 0 (no activity limitations) to 5 (major activity limitations) summed up to yield a total score (0-50, with a lower score indicating fewer activity limitations). The OswestryQ is considered the gold standard of low back functional outcome tools (AbuElhiga-Narmna & Loifer, 2005; Bar-On et al., 2005; Niscanen, 2002) and has previously been proven as a valid and reliable instrument. AbuElhiga-Narmna and Loifer (2005) found Cronbach’s alpha of .89 among 111 physiotherapy patients. Bayar, Bayar, Yakut, and Yakut (2013) found a construct validity between the Turkish (OswestryQ) and the Turkish (Roland–Morris Low Back Pain and Disability Questionnaire), r = .66-.78. Bar-On and his colleagues (2005) performed the Hebrew version of the OswestryQ and found it reliable (internal consistency of Cronbach’s α = .93) and valid while observing significant differences between the two study groups (two groups of seniors in the community with and without low back pain symptoms).
Back pain was also tested using the BackAche Disability Index (BADIX), as it includes a physical examination. The BADIX is a two-section test consisting of the BackAche Index and Back Stiffness Score. The BackAche Index which assesses five active back movements (bending forward, bending to both sides, and combined bilateral bending sideways and backward) all gauged on a 4-point Likert-type rating scale (0 = no irritation and normal end-feel to 3 = severe pain and reduced end-feel), with an overall score range of 0 to 15, with a lower score indicating less irritation. End-feel is the resistance to passive movement at the end of range of a joint (Chesworth, MacDermid, Roth, & Patterson, 1998). The morning Back Stiffness Score includes six statements: 0 = upon awakening, feeling no stiffness or back discomfort, 1 = no stiffness but back discomfort, 2 = light stiffness and back discomfort, 3 = light stiffness and back pain, 4 = severe stiffness and back pain, and 5 = the need for assistance in getting out of bed in addition to unbearable pain (overall score = 0-5, with a lower score indicating lower levels of stiffness/discomfort). The final grade was calculated from the total scores of the two sections (BackAche Index score + morning Back Stiffness Score) with an overall score of 0 to 20, with a lower score indicating better function/less stiffness and pain (Farasyn & Meeusen, 2006; Farasyn, Meeusen, Nijs, & Cuesta-Vargas, 2013).
The cultural adaptation of BADIX (Gjersing, Caplehorn, & Clausen, 2010) was performed by health professionals fluent in English and Hebrew using independent two-way translations, reviewed by an expert committee and pretested on 20 staff members at a nursing school. The reliability results were .965 for the Cronbach alpha coefficient with an ICC (95% CI) of .933 [.839-.973]. The test/retest evaluation revealed a score of r = .908. The Spearman correlation concurrent validity was p = .680 on the Roland–Morris Disability Questionnaire (Jacob, Baras, Zeev, & Epstien, 2000; Roland & Morris, 1983) and p = .570 on the OswestryQ (Bar-On et al., 2005; Roland & Faibankt, 2000).
Estimation of workload, burnout and job satisfaction was examined, with workload measures including a six-item questionnaire relating to workload level, work speed, working time, workload, amount of hard work, workload pressure, amount of effort demanded, and comprehensive work stress level, all gauged on a 7-point Likert-type rating scale (1 = not at all; 7 = very much; Karasek, 1979; Karasek & Theorell, 1990). The questionnaire has been previously proven as a valid and reliable instrument. Theis and Finkelstein (2014) reported Cronbach’s α score of .86 among 124 workers. In a cross-sectional study among 1,574 consultation physicians in Israel, the Workload Questionnaire in Hebrew was evaluated (Nirel, Goldwag, Feigenberg, Abadi, & Halpern, 2008) and found reliable and valid (Karasek, 1979; Karasek & Theorell, 1990).
The Shirom–Melamed Burnout Measurement Questionnaire was employed which included a 16-item questionnaire relating to burnout at work; it was divided into three subgroups: (a) energy level, that is, feeling tired, lack of morning energy for work, feeling physically drained; (b) vital thinking, that is, exhaustive thought, slow thinking, concentration difficulty, an unclear head and scattered feelings; (c) emotional energy, that is, fed up, running on an empty battery, feelings of detachment, difficulty relating to complicated issues, lack of sensitivity to others’ needs, such as workers or patients, no strength to invest emotionally in others, incapable of feeling sympathy toward others, mental fatigue, all gauged on a 7-point Likert-type rating scale (1 = almost never; 7 = almost always; Melamed, 2009; Melamed, Shirom, Toker, Berliner, & Shapira, 2006; Shirom, 1998). The Shirom–Melamed Burnout Measurement’s Hebrew version has been previously proven as a valid and reliable instrument. In a cross-sectional study among 1,574 consulting physicians in Israel, the Work Burnout was evaluated and found to be reliable (α = .93) and valid (Nirel et al., 2008).
The Job Satisfaction Questionnaire was employed which included a 10-item questionnaire relating to the degree of satisfaction in accordance with responsibility, freedom to choose work methods, work diversity, coworkers, physical working conditions, realization capabilities, salary level, a boss who recognizes the good performance of the worker, and working hours, all evaluated on a 7-point Likert-type rating scale (1 = very unsatisfied; 7 = very satisfied; overall score = 11-77; Bowling & Hammond, 2008; Shirom, 1998). This questionnaire has been previously proven as a valid and reliable instrument (Chanchai et al., 2016; Voss, Floderus, & Diderichsen, 2001). In a cross-sectional study among 1,574 consulting physicians in Israel (Nirel et al., 2008), this questionnaire was evaluated in Hebrew. The questionnaire was found to be reliable (α = .93) and valid (Voss et al., 2001).
Procedures
Prior to the study, the sliding sheets were assessed for durability by the hospital’s laundry facility. They were found durable, thus allowing the sliding sheets to be washed with the regular cotton sheets for infection control.
The study was performed in three phases which included 3 months per phase (Figure 1).
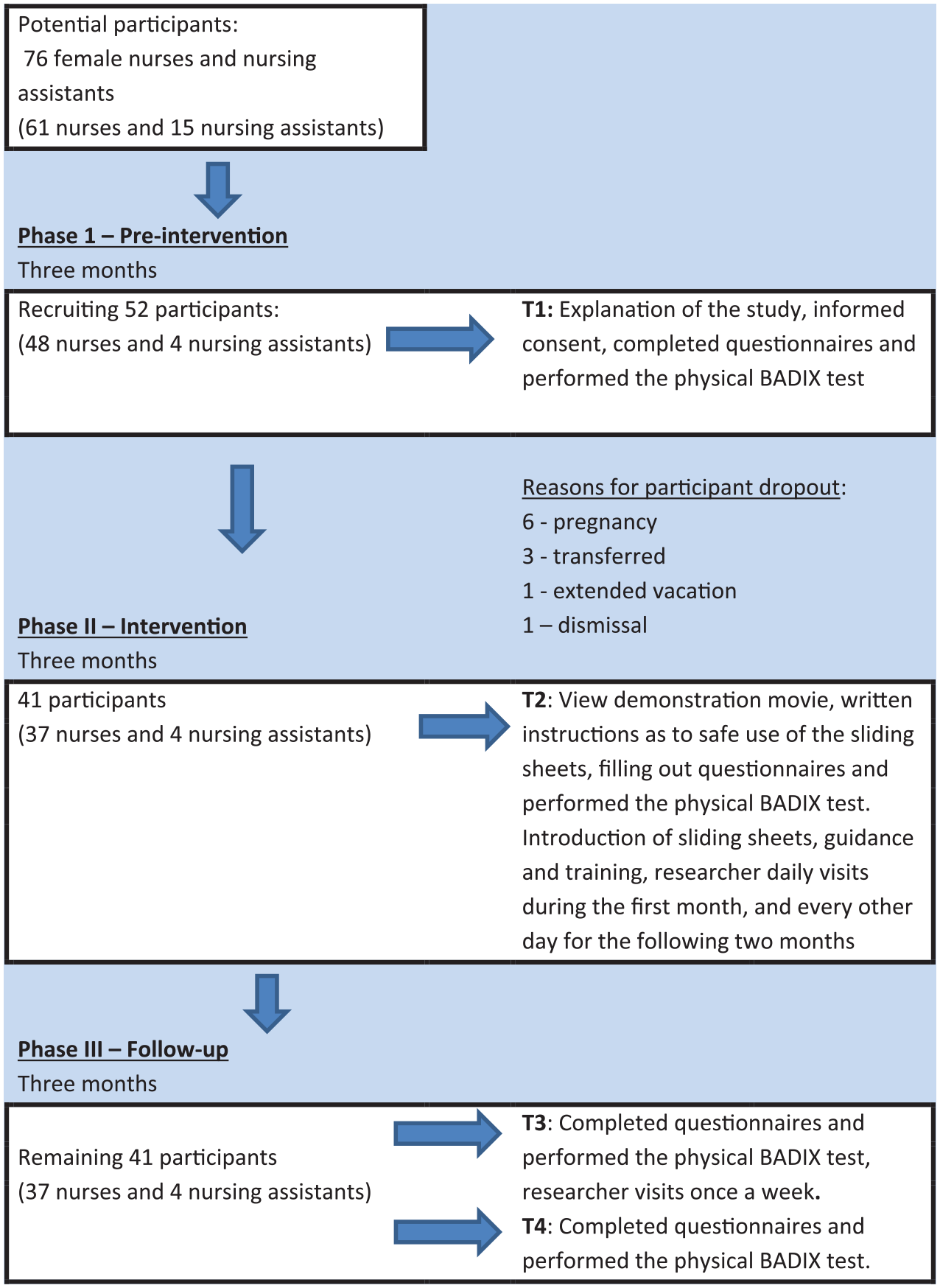
The study flow chart.
Phase I—Pre-intervention measuring phase
During the first month, departmental staff meetings were held in the three participating internal medicine departments. An explanation of the study was given to the participants and informed consent forms were signed. The participants filled out the questionnaires and performed the BADIX test for the first time (T1).
Phase II—Intervention measuring phase
Three months after commencement of the research, with no intervention as of yet, participants filled out the questionnaires for the second time and performed the BADIX test (T2) once again. The staff were shown the type of sliding sheets to be used, a training film, guidance forms, and diaries which would be filled out as to the extent of the use of the sliding sheets. The following day, after each departmental staff meeting, the sliding sheets were distributed for use among the patients for 3 months. During these 3 months, guidance and training of the staff were carried out as follows: a daily visit during the first month and then every other day for the following 2 months. At the end of Phase II, a third meeting was held, questionnaires were filled out, and the BADIX evaluation was performed once again (T3).
Phase III—Follow-up measuring phase
Following 3 months of sliding sheet use, the participants filled out the questionnaires once again and the BADIX was performed for the fourth time (T4).
Statistical Analysis
All statistical computations were performed using the SPSS 17.0 for Windows (SPSS, Chicago, IL, USA). Descriptive statistics were performed to obtain a sample characterization. The sample size was estimated by a Power and Sample Size Calculation (PS Version 3.0, 2009) software. WRMSP and disability were the main outcome measures of the study. The QDASH was selected to present the sample size calculation as it resulted in the largest sample size. Previous findings have suggested that response differences in the QDASH among matched pairs were normally distributed with a maximal standard deviation of 20 (Polson, Reid, McNair, & Larmer, 2010). If the correct difference in the matched pairs averaged 11 (discriminant difference), a significance level of 5% (α = .5), the statistical power of 80% (β = .8) and a sample of 28 subjects were required. In light of the foregoing, a sample size of 30 participants qualified as sufficient statistical power. Because a number of outcome measures were used simultaneously, we chose to recruit 50 subjects.
Descriptive statistics were utilized to characterize the study sample. Prior to data analysis, a Kolmogorov–Smirnov test was performed on all variables. Normal distribution was found and the null hypothesis was not rejected (p < .2-.4). In addition, all variables found in the skewness test showed distribution values ranging from +1.96 > Z > to 1.96 (normal range). Repeated measurement analysis of variance (ANOVA) compared the four measurements of WRMSP and disability (tested by the NDI, QDASH, OswestryQ, and BADIX) as well as an estimation of workload, burnout, and job satisfaction. The Wilcoxon signed rank test compared the participants’ reports on the extent of sliding sheet usage at the end of the first 3 months and at the end of 6 months.
Results
During the data collection period, 76 female nurses and nursing aids (61 and 15, respectively) were employed in these departments. When the research protocol was presented at routine staff meetings, 48 nurses and four nursing assistants volunteered to participate (Figure 1). During the first 3 months, 11 nurses dropped out; hence, 41 subjects (37 nurses and four nursing assistants) were included in the statistical analysis. At baseline, only two out of the 41 subjects experienced no neck pain; nine experienced no arm, shoulder, or hand pain; and four experienced no lower back pain, which could cause functional limitations.
As shown in Table 1, the mean values of the following demographic characteristics of the population include age (37.73 ± 10.2), weight (66.21 ± 10.95), height (1.64 ± 0.05), body mass index (BMI; 24.66 ± 4.42), number of children (1.2 ± 1.12), number of children under the age of 6 (0.44 ± 0.77), years in the profession (10.95 ± 10.20), and years of work in the current workplace (7.22 ± 7.87). More than half of the subjects were physically active (58.5%), and most of them were nonsmokers (85.4%). The majority were academic registered nurses (73.2 %) with an average seniority of 10.95 ± 10.00 years.
Demographic and Occupational Characteristics of Study Nursing Staff (N = 41)
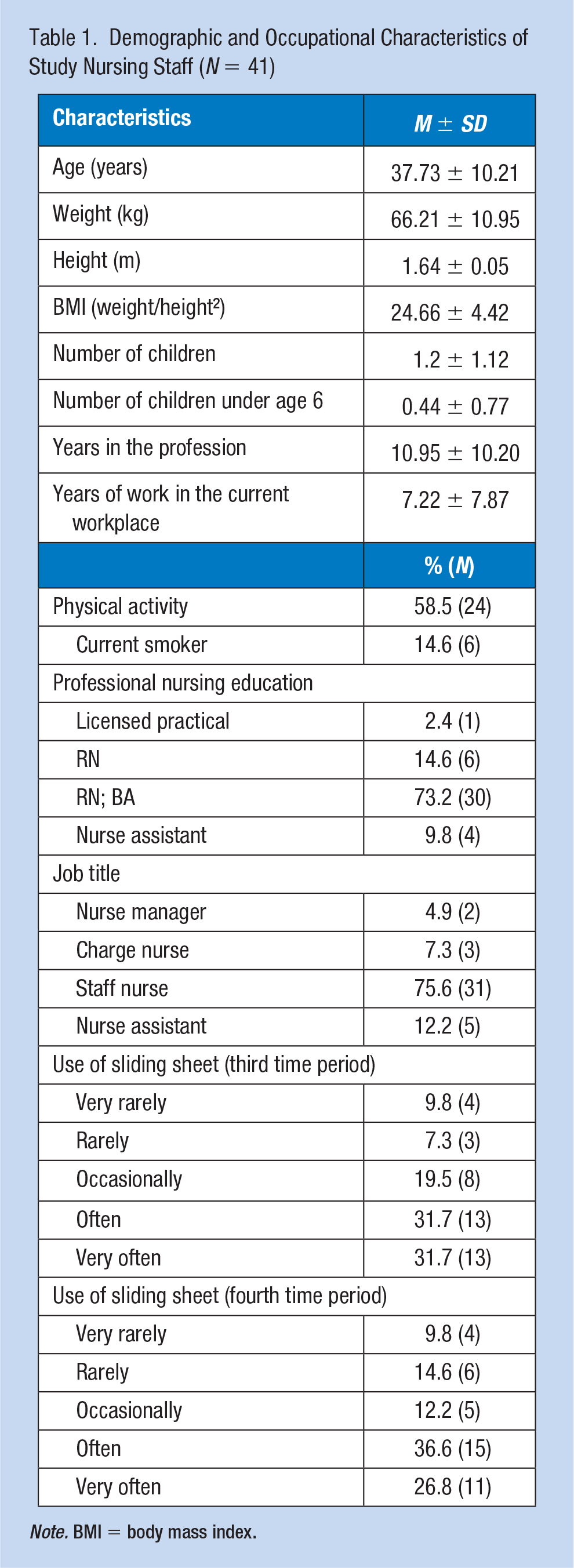
Note. BMI = body mass index.
Participants reported extensive use of sliding sheets after 3 and 6 months of usage, as demonstrated in Figure 2. After 3 months of intervention, only 16% reported utilizing the sheets “very rarely” and “rarely,” and 20% reported utilizing the sheets “occasionally.” After 6 months of usage, only 25% reported utilizing the sheets “very rarely” and “rarely,” and 12% reported utilizing the sheets “occasionally.” Approximately 64% reported utilizing the sliding sheets “often” and “very often” in both periods. No significant differences were found between the two time periods (Z = −0.536, p = .592).
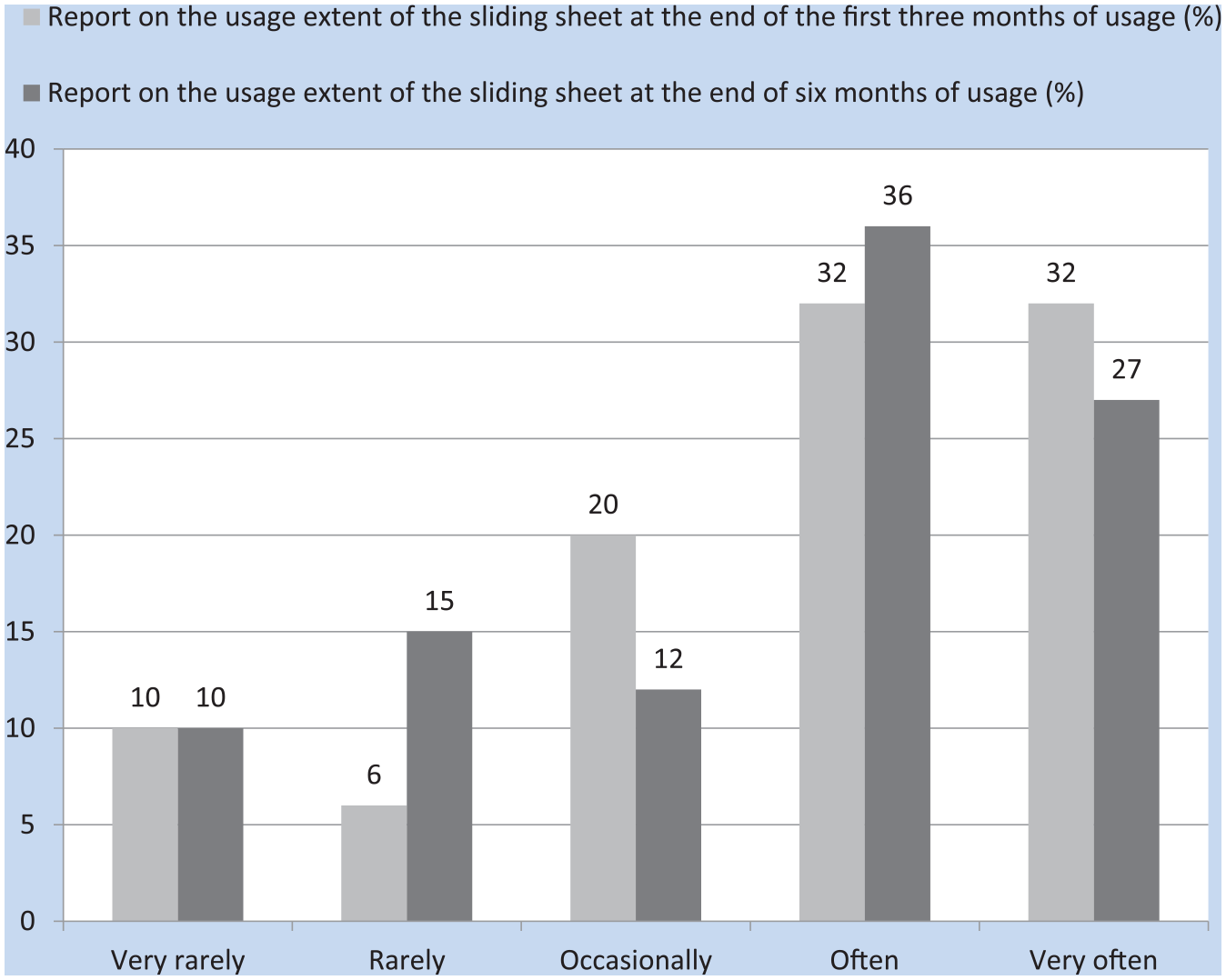
The reported usage of the slide sheet at 3 and 6 months postintervention.
The effects of using sliding sheets when moving a bedridden patient on WRMSP, disability, and psychosocial aspects among nurses and nursing assistants are shown in Tables 2 and 3. The BADIX results demonstrated significant improvement in back pain and morning stiffness, F(3, 120) = 21.72, p < .001 (Table 2), as well as the NDI which showed significant improvement in neck pain and discomfort following the intervention, F(3, 120) = 9.36, p < .001. In addition, the QDASH showed significant improvement following the intervention and follow-up, F(3, 120) = 2.84, p < .041. The OswestryQ, which measured back pain and disability, also showed significant improvement following the intervention, F(3, 120) = 11.28, p < .001. The Job Satisfaction Questionnaire (Table 3) showed significant improvement in the follow-up period, F(3, 120) = 6.68, p < .001, whereas the Workload Questionnaire and the Shirom–Melamed Burnout Measurement Questionnaire showed no significant differences between the four different measurement times, F(3, 120) = 1.09, p = .358; F(3, 120) =1.93, p = .129, respectively.
Measures of Nursing Staff’s Physical Comfort Before and After the Sliding Sheet Intervention (N = 41)
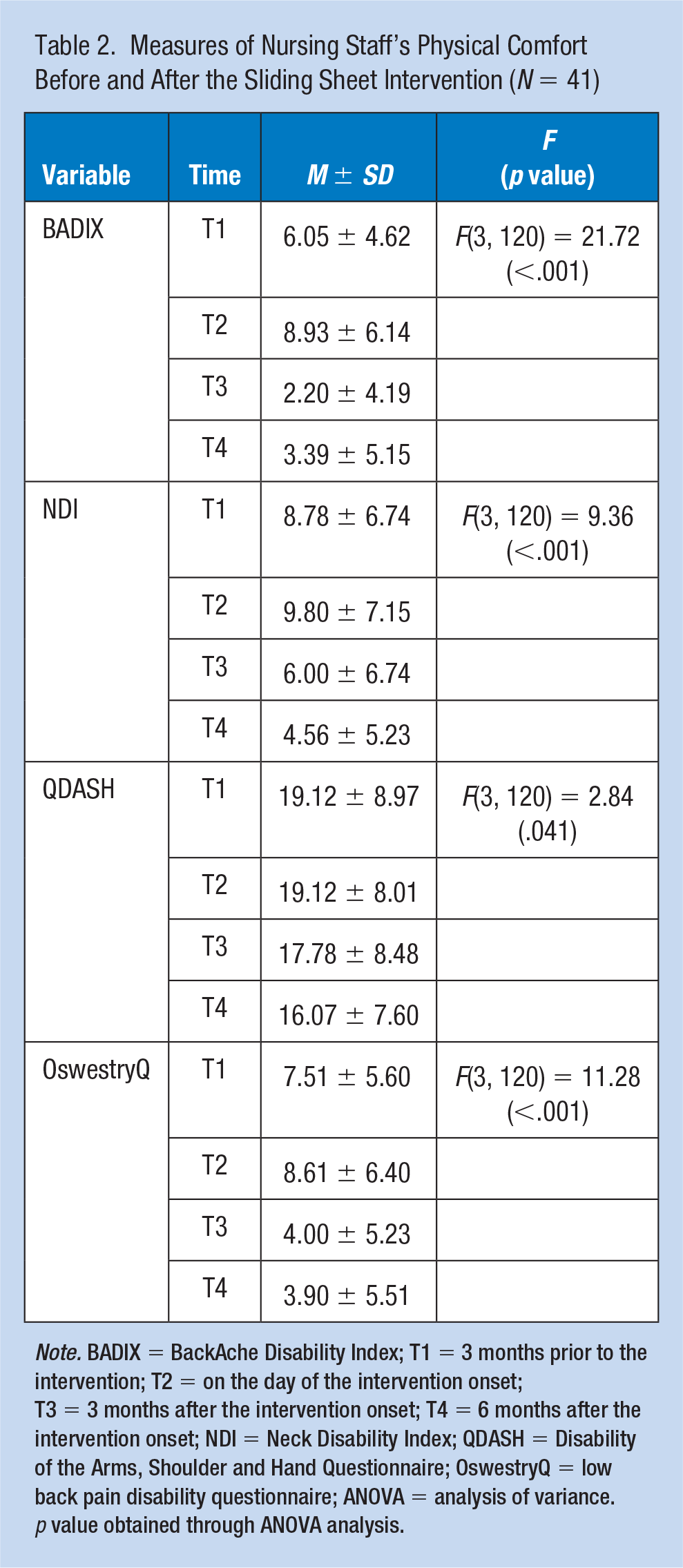
Note. BADIX = BackAche Disability Index; T1 = 3 months prior to the intervention; T2 = on the day of the intervention onset; T3 = 3 months after the intervention onset; T4 = 6 months after the intervention onset; NDI = Neck Disability Index; QDASH = Disability of the Arms, Shoulder and Hand Questionnaire; OswestryQ = low back pain disability questionnaire; ANOVA = analysis of variance. p value obtained through ANOVA analysis.
Measures of Nursing Staff’s Job Satisfaction—Workload and Burnout Before and After the Sliding Sheet Intervention (N = 41)
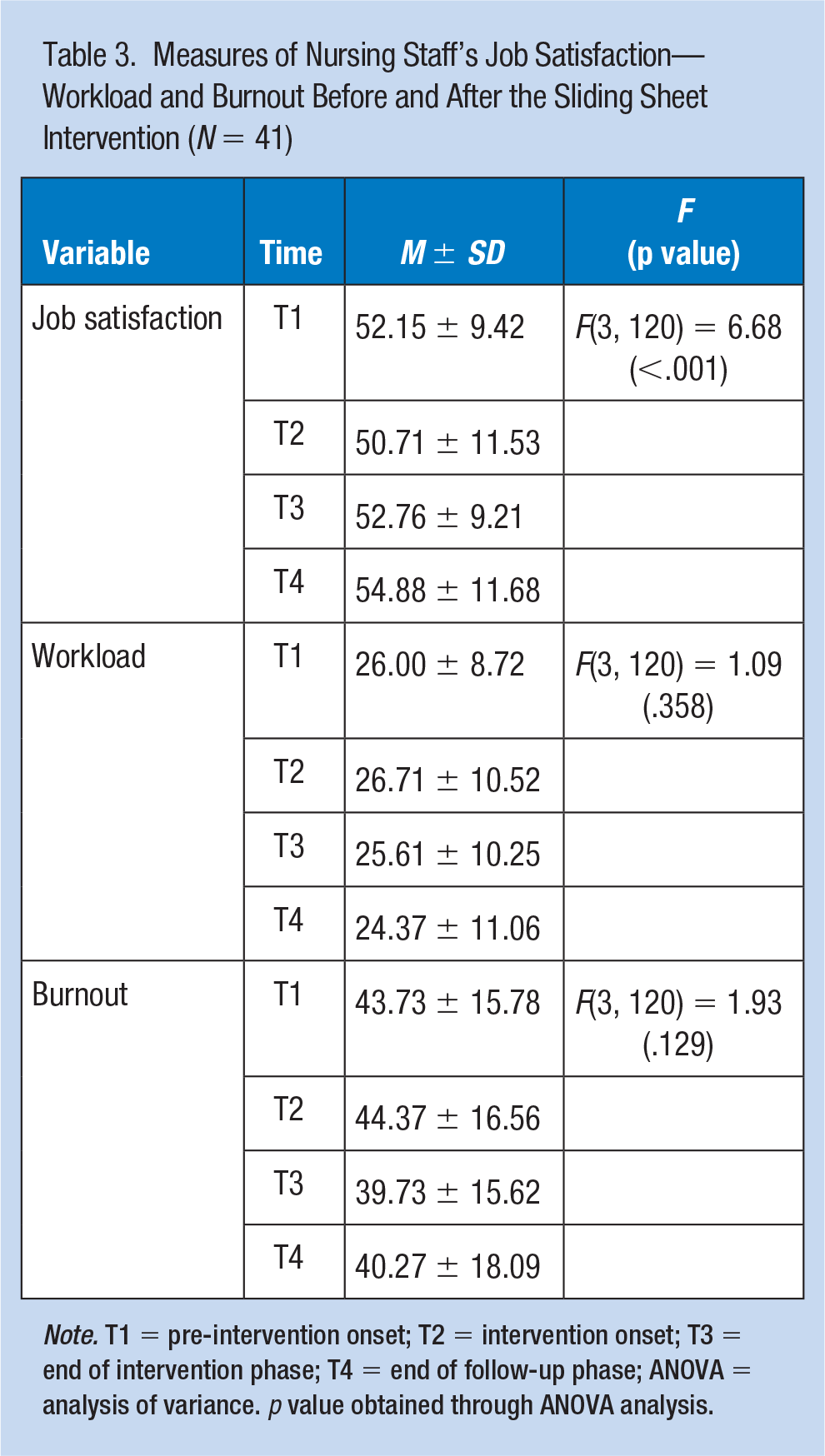
Note. T1 = pre-intervention onset; T2 = intervention onset; T3 = end of intervention phase; T4 = end of follow-up phase; ANOVA = analysis of variance. p value obtained through ANOVA analysis.
Discussion
To the best of our knowledge, the current study is the first to clinically examine the consequences of utilizing sliding sheets when repositioning bedridden patients. Utilizing sliding sheets by nurses and nursing assistants resulted in reduction in pain and disability and improved job satisfaction. Unfortunately, we are witnessing scarce use of assisting devices in the clinical field, despite their effectiveness in reducing WRMSP. The use of sliding sheets should be strongly encouraged by nurses and by administration.
Impact on Upper and Lower Back Pain and Disability
The BADIX, which includes a questionnaire and physical examination results, showed a significant decrease in back pain, disability, and morning back stiffness during the intervention and follow-up phase. These findings, reinforced by the OswestryQ, indicated a significant decrease in the level of back pain and disability. Our findings aligned with a larger study conducted among 5,017 Danish health care workers in eldercare, who had responded to baseline and follow-up questionnaires (Andersen et al., 2014), which found that persistent use of assistive devices reduced the risk of a back injury, a risk outcome of daily patient transfer. Other studies, performed under laboratory conditions, examined the effect of sliding sheet usage on back pain and disability when repositioning bedridden patients (Jäger et al., 2013; Skotte & Fallentin, 2008), reaffirming the advantages of sliding sheets during manual patient handling. Jäger and colleagues (2013) built a biomechanical model to assess the lumbar load and the potential for load reduction by applying biomechanically “optimized” transfer modes such as sliding sheets instead of “conventional” techniques. Their results showed that highest compressive force values were found for conventional performances and lowest values when sliding sheets were applied. Furthermore, Skotte and Fallentin (2008) used also a biomechanical model for calculating the net torque at the L4/L5 joint and found that friction-reducing devices like sliding sheets had even higher influence on the low backload of the caregiver than the patient’s weight and disability.
In an earlier study, Schibye and colleagues (2003) assessed the changes in the mechanical load on the lower back in a laboratory setting by using plastic bags to minimize the friction between the patient and the bed. They found a decrease in the peak torque and compression force at the L4/L5 joint when using friction-reducing devices for repositioning a supine patient toward the head of the bed. Similar conclusions were obtained by Bartnik and Rice (2013) who investigated the force required for moving a patient upward in bed using friction-reducing slide sheets versus traditional cotton sheets, which was reduced with the sliding sheet.
Influence on Neck Pain and Disability
In the current study, the NDI measures demonstrated a significant decrease in the level of neck pain and disability which resulted from the use of the sliding sheets during the 3- and 6-month follow-up periods. Our study is in accordance with a previous study, conducted by Smedley and colleagues (2003), which assessed the incidence and risk factors of neck and shoulder pain in nurses by a self-reported incidence of neck and shoulder symptoms over a 2-year period among 587 nurses who had been pain-free for at least 1 month at baseline. Their results indicated that for physical exposures at work, the highest risks were associated with specific patient handling tasks involving reaching, pushing, and pulling. Our results are also in agreement with our previous study (Weiner et al., 2017) that assessed perceived exertion of patient repositioning in bed rated by the Borg (1982) scale, and indicated a significant advantage for both neck and lower back when utilizing sliding sheets. Our findings also concur with other studies (Arsalani, Fallahi-Khoshknab, Josephson, & Lagerstrom, 2014; Drew, Kozey, & Morside, 2016; Filek, Leach-Macleod, Brims, Binsted, & Jakobi, 2010; Fragala & Fragala, 2014).
Influence on Arms, Shoulders and Hand Pain and Disability
In our study, the QDASH measures showed a significant decrease in the level of pain and disability rates for the arms, shoulders, and hands. Lloyd and Baptiste’s (2006) laboratory study concurs with our findings, showing significantly lower force on the upper extremities during the performance of transfer tasks using friction-reducing equipment compared with regular draw sheets. Bartnik and Rice (2013) also found a reduction in the force required by the caregiver’s hands to pull a patient up in bed when using friction-reducing sliding sheets. Accordingly, it may be concluded that the use of a sliding sheet has a protective influence on arms, shoulders, and hands expressed after a prolonged period of time.
Effect of the Intervention on Psychosocial Aspects
The results of the Job Satisfaction Questionnaire indicated a significant increase in job satisfaction during the intervention phase which concurs with Zhuang, Stobbe, Collins, Hsiao, and Hobbs’s (2012) study that examined the effects of resident-transferring methods on the psychophysical stress of the personnel performing the transferring tasks. The results indicated that the psychophysical stresses on nursing assistants were significantly lower when performing resident transfers with assistive devices than when performing transfers using the baseline manual transfer method. The absence of continuity in job satisfaction during the follow-up phase (compared with that observed in the intervention phase) in the current study was probably due to the adaptation of working with the sliding sheet, whereas the other work environmental conditions, such as organizational factors, were unchanged. Improved satisfaction at the time of the intervention may be due to the intervention itself more than to the type of intervention, so further intervention such as an organizational one seems to be needed to see continuity in improving satisfaction. Schwendimann, Dhaini, Ausserhofer, Engberg, and Zuniga’s (2016) study strengthened the importance of organizational characteristics on job satisfaction.
Perception of the workload and burnout level showed no significant differences between the four measurement times. S. J. Lee, Faucett, Gillen, Krause, and Landry (2010) found that physical workload perception was not associated with safe work behavior (such as using the sliding sheet), which we also concur. Similar findings were found by Smedley and colleagues (2003) who assessed the incidence and risk factors of neck and shoulder pain in nurses. The researchers found that workplace psychosocial factors (including job demands, satisfaction, and control) were not associated with incident neck/shoulder symptoms, which is consistent with our findings.
Several limitations of this study include that the selection of hospital wards for the intervention was not randomized, and participants were selected from a convenience sample of volunteers without representation of the full nursing staff. In addition, we ascertained data through self-report which may lead to bias such as recall or social desirability bias. We originally asked participants to fill out a daily “sliding sheet usage diary”; however, it was rarely filled out, so we were not able to use these data. Future research is necessary to investigate the influence of maintaining ongoing training, management involvement, and to establish a culture that encourages the use of this type of equipment to aid in patient handling.
Conclusion
The findings of our study indicate a clear influence of reducing WRMSP and disability and increasing job satisfaction when sliding sheets are introduced into nursing practice. We conclude that the pain and disability measures used in this study are particularly sensitive to musculoskeletal monitoring in prospective study design. It appears that pain and disability monitoring are more accurate than monitoring pain alone. In light of our findings as regards the absence of continuity in job satisfaction after 6 months of intervention, we recommend maintaining an ongoing training program to establish a culture that encourages the use of equipment to aid in patient handling.
Implications for Occupational Health Practice
The findings of our study indicate a clear influence of reducing WRMSP and disability among nursing staff who used the sliding sheets, as well as an increase in job satisfaction. We included a training program in this study which fostered the adoption of safe patient handling practices. Occupational health nurses in health care are well positioned to implement this type of safe patient handling intervention, which is of low cost. All direct patient care providers could benefit from this type of intervention.
Applying Research to Practice
Previous studies have found that the usage of sliding sheets in patient care is a valuable technique in repositioning bedridden patients compared with traditional cotton sheets or carriers. Our aim was to examine the effect of sliding sheet use among nursing personnel when moving bedridden patients on physical strain and job satisfication. Among 41 female nursing staff, after 3 and 6 months of sliding sheet usage, pain and disability decreased in the neck (p < .001); arms, shoulders, and hands (p = .041); and lower back (p < .001), with an increase in job satisfaction (p < .001). The findings of our study indicate an influence of reducing pain and disability while increasing job satisfaction when sliding sheets are introduced into nursing practice.
Footnotes
Acknowledgements
The study was performed in partial fulfillment of doctoral degree requirements. The authors thank the management, the nursing staff, and the laundry staff at Bnai Zion Medical Center in Haifa for participating in the study. The authors thank Mrs. Phyllis Curchack Kornspan for her editorial services.
Conflict of Interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Author Biographies
Deborah Alperovitch-Najenson completed her physical therapy studies at Karolinska Institute in Stockholm University in Sweden in 1989. In 2005 she completed PhD studies in the Department of Anatomy and Anthropology, Tel Aviv University, and postdoc at Ben-Gurion University of the Negev in 2011. She does research in the field of Ergonomics and guides students in their thesis.
Chava Weiner completed her nursing studies at Bnai Zion (Rothschild) Hospital Nursing School in Israel in 1978 and has been the director of this school since 2008. In 2019, she completed PhD studies in the Department of Environmental and Occupational Health at Tel Aviv University.
Joseph Ribak graduated from the Tel Aviv University School of Medicine in 1974. He specialized in occupational medicine at Mount Sinai Hospital in New York 1984. He was previously a medical officer of the air and sea forces, head of Occupational Medicine at the Tel Aviv University School of Continuing Education, vice president of the Tel Aviv Medical Center for Surasky, vice president of the Israel College of the Academy, head of the Medical Institute for Road Safety, and many more. He is currently retired.
Leonid Kalichman completed his physical therapy studies at Tel Aviv University in 1995. In 2004, he completed PhD studies in the Department of Anatomy and Anthropology, Tel Aviv University, and postdoc at Boston University in the United States in 2009. Since 2008, he began an academic career in the Physical Therapy Department at Ben-Gurion University of the Negev, and from 2017 he serves as head of the department. He is the director of a Musculoskeletal Medicine Clinical Research Unit and has established a South Israel Interdisciplinary Academic Forum of Musculoskeletal Medicine (SIMM). He has published more than 160 articles in scientific journals.