
Abstract
Occupational health clinicians often collect and/or interpret annual wellness biometrics for workers. It is now known that type 1 diabetes can present in stages including presymptomatic/normal glucose, presymptomatic/impaired glucose, and symptomatic/hyperglycemia. A workplace wellness screening case illustrates the concepts, along with background pathophysiology, recommendations for new staging and first degree relative screening, and implications for occupational health nurses.
Keywords
Many worksites in the United States offer annual biometric screening for employees to increase their awareness of modifiable risk factors contributing to disease and motivation to improve their personal health through primary prevention strategies. Beyond primary prevention, worksite screenings can lead to early diagnosis of previously unrecognized disease. Many times, participation in these screenings is paired with an incentive (e.g., reduced pricing on employer-sponsored health insurance); thus participation is generally robust. Healthy employees are believed to be more productive, exhibit less presenteeism, and incur fewer aggregate costs billed to employer-sponsored health insurance, which is a win-win for both employees and employers.
This article highlights a case of worksite wellness screening contributing to the identification of abnormally elevated fasting blood glucose, ultimately diagnosed as type 1 diabetes (T1D). Because the abnormal glucose was identified prior to symptoms, the individual was spared the often-antecedent life-threatening diabetic ketoacidosis (DKA), potentially saving the worker’s life and reducing costs to the company’s health insurance. The American Diabetes Association’s (ADA) recommended approach to presymptomatic staging, future directions, and implications for occupational health nurses are discussed.
Case
A 38-year-old asymptomatic Caucasian female health care worker attended an employer-sponsored biometric health screening as required for preferred health insurance pricing. Past health history was significant for “borderline gestational diabetes in one of two pregnancies,” but otherwise healthy. Family history was significant for type 2 diabetes in two grandparents, but negative for diabetes in parents and siblings. Lifestyle was significant for sedentary remote pharmacy work from home. The worker’s weight was, and had always been, normal. The worker did not report a recent increase in thirst, urinary frequency, or weight loss. Table 1 illustrates worksite biometric findings.
Initial Laboratory Values for 38-Year-Old Female
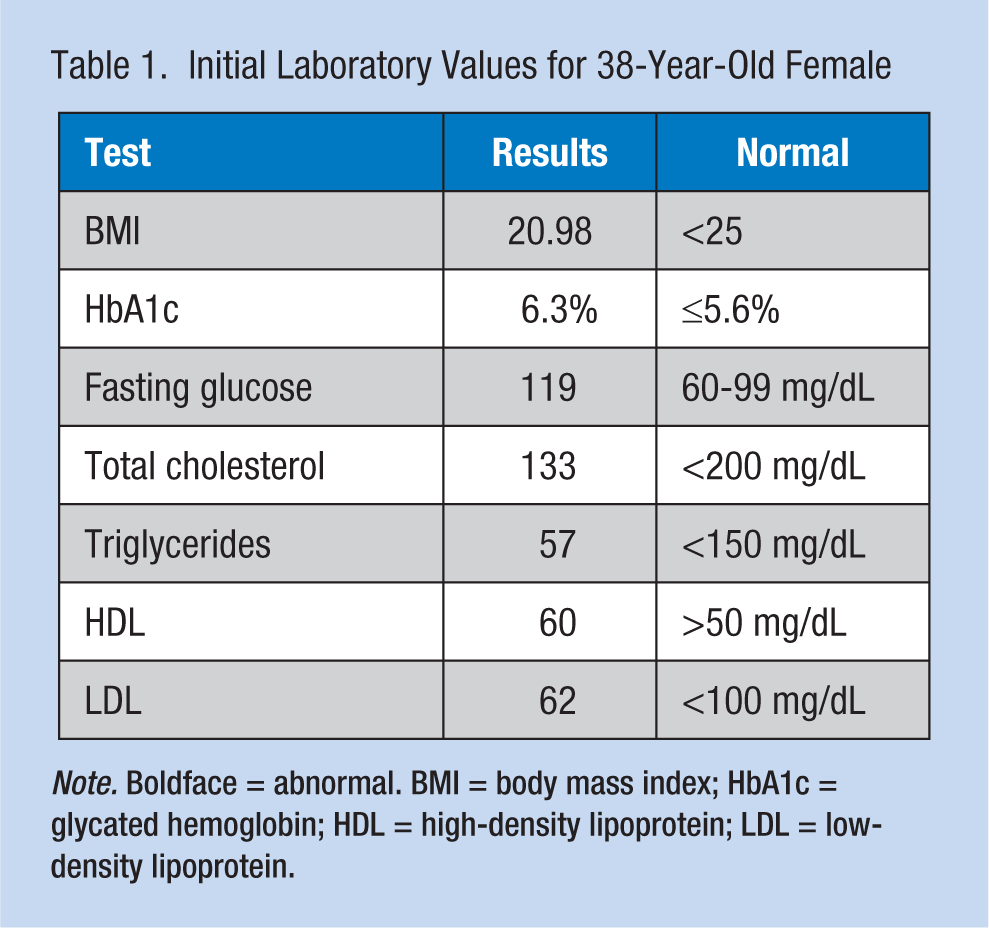
Note. Boldface = abnormal. BMI = body mass index; HbA1c = glycated hemoglobin; HDL = high-density lipoprotein; LDL = low-density lipoprotein.
The occupational health office advised the worker to schedule an appointment with a primary care provider based on the hemoglobin A1c result of 6.3%, above the normal value of up to 5.6%, and the fasting glucose of 119, above the normal value of 60-99 mg/dL (ADA, 2017). A repeat hemoglobin A1c returned at 6.2%, consistent with prediabetes. Metformin per patient request, home glucose monitoring, daily exercise, and elimination of dietary processed carbohydrates were initiated with no effect on the fasting glucose elevation. A specialist was consulted, and the worker was found to have elevated antibodies for T1D along with a low c-peptide level confirming a diagnosis of presymptomatic T1D.
Background
Islet cells of the pancreas contain beta cells responsible for endogenous insulin production. The insulin produced is in equal proportions to c-peptide. Insulin is released based on glucose levels in the bloodstream, ultimately facilitating glucose metabolism and supplying the body with energy (Ludvigsson, 2016). Without insulin, severe hyperglycemia occurs, resulting in metabolic repercussions such as significant unintentional weight loss, malnourishment, and dangerous ketogenesis (Ludvigsson, 2016).
Type I diabetes is a disease state characterized by autoimmune destruction of the pancreatic beta cells (ADA, 2017). Equally devastating is the inability for these beta cells to regenerate (Pozzilli, Maddaloni, & Buzzetti, 2015). The ADA (2017) estimated the prevalence of immune-mediated T1D at 5% to 10% of all diabetes cases. Historically, T1D has been a juvenile onset disease with the presentation typically acute. However, recent studies from Europe have suggested that at least 25%, and as many as 50%, of new T1D cases occur in adulthood (Thomas, 2016). Adult presentation can be insidious, so accurate diagnoses can be challenging in some cases (Thunander et al., 2008).
Diagnosing T1D
In many cases, T1D manifests with acute onset hyperglycemia resulting in DKA and necessitating at minimum an emergency department visit, but more often intensive care. As the case study illustrates, with widespread workplace health screenings, T1D can be identified in the presymptomatic phase, potentially saving lives. Although definitive diagnosis is beyond the scope of the typical occupational health clinic, background information about diagnostic laboratory tests can be informative.
As previously discussed, c-peptide is produced simultaneously with insulin in the body, and, therefore, a commonly used marker for insulin production in the pancreas (American Association for Clinical Chemistry, 2014). Evaluating fasting c-peptide provides a picture of the pancreas’s ability to produce insulin (low in T1D). Autoantibodies, including islet cell cytoplasmic autoantibody (ICA), glutamic acid decarboxylase-65 (GAD-65A), insulinoma-associated 2 (IA-2A), and zinc transporter 8 (ZnT8A) autoantibodies, can confirm the diagnosis, with one or more being positive in T1D (ADA, 2017). Table 2 lists these autoantibodies with their normal values.
Autoantibodies Commonly Found in T1D
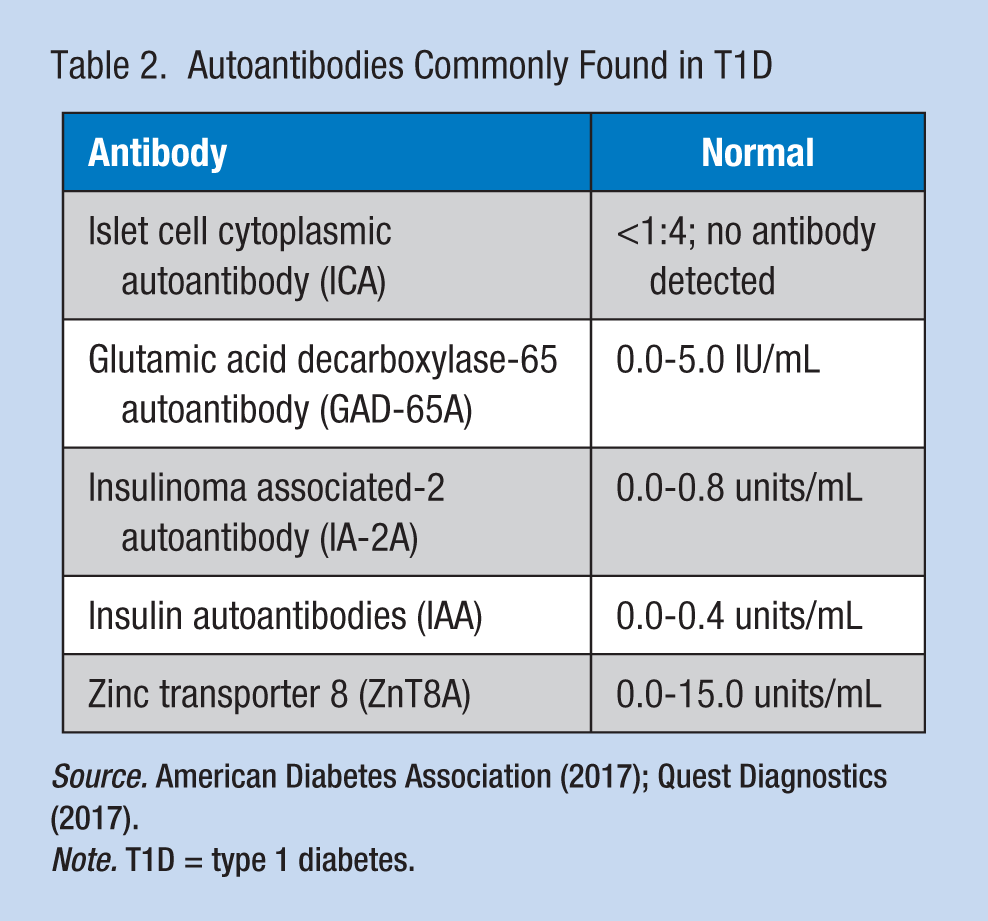
Note. T1D = type 1 diabetes.
Staging T1D
With improved detection in recent years, the ADA in 2017 published guidance for staging T1D. As illustrated in Table 3, three stages range from “presymptomatic” whereby only antibodies are positive to hyperglycemia with classic diabetes symptoms such as weight loss, thirst, and urinary frequency (ADA, 2017). Case finding for workers with Stage 1/presymptomatic T1D is recommended through autoantibody testing of first degree relatives (ADA, 2017).
Type 1 Diabetes Staging
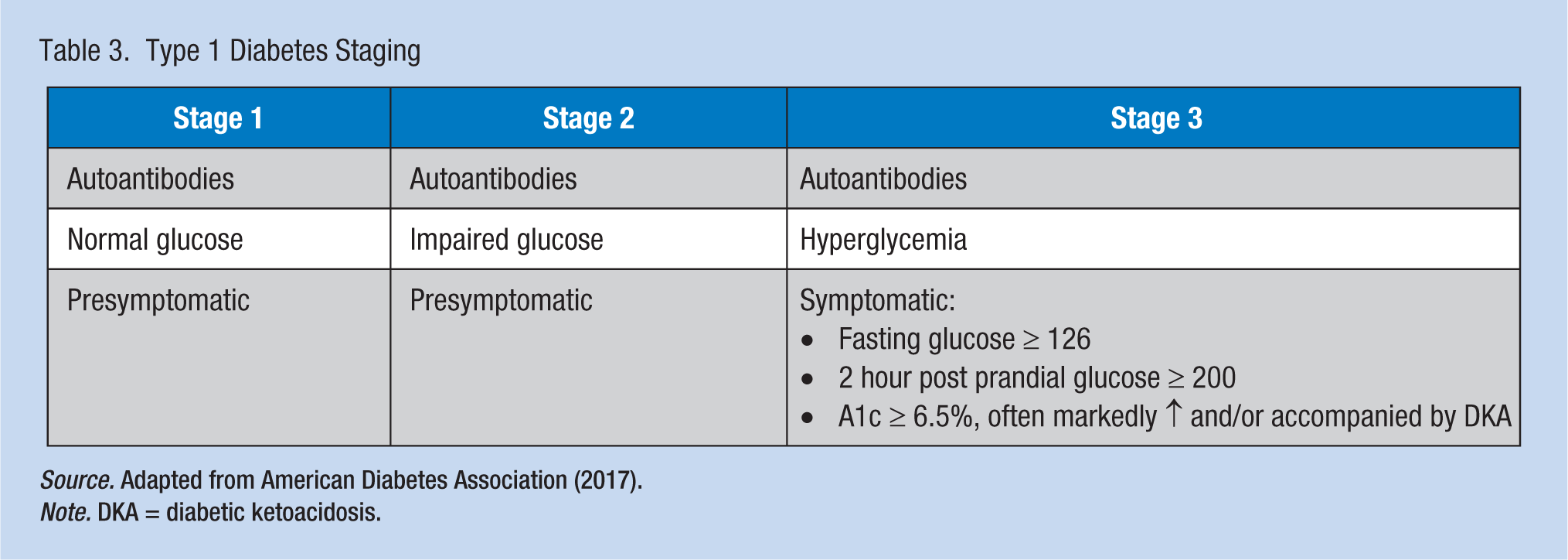
Source. Adapted from American Diabetes Association (2017).
Note. DKA = diabetic ketoacidosis.
Case, Continued
Clinical clues for typical type 2 diabetes, such as obesity and dyslipidemia, were not present in this worker, which should alert the occupational health clinician to consider other causes of abnormal glucose. This worker was identified to have Stage 2 T1D given the presence of autoantibodies, elevated glucose, and elevated A1c. Insulin therapy was initiated in the specialist’s office. Improvement in glucose control along with a slight increase in weight (which can be expected with stabilization of glucose levels) was subsequently noted. As previously indicated, the worker also had two healthy young children. Following the ADA’s recommendation to screen for autoantibodies in first degree relatives, one of the worker’s children tested positive for the GAD-65 antibody, but with normal glucose, which is consistent with Stage 1 T1D. The child did not need insulin yet, but will be monitored closely in the future for symptoms of diabetes, and, much like her mother, will likely be spared acute onset DKA given disease identification.
Future Directions for T1D
The City of Hope’s Diabetes and Metabolism Research Institute recently announced their goal to cure T1D by the year 2023 (City of Hope, 2017), which is a very ambitious, but welcomed goal as many individuals anxiously await such a cure. Researchers have investigated various pathways of autoimmune beta cell destruction; subsequent therapies targeting those mechanisms are ongoing, including one City of Hope’s foci. Single immune modulators and various combinations have been, or are being, investigated in efforts to find a cure (City of Hope, 2017; Pozzilli et al., 2015; Type 1 Diabetes TrialNet, 2017).
Implications for Occupational Health Nurses
Occupational health clinicians are both individual and workplace population health providers. Biometric workplace screenings have proven their value in identifying risks for, or monitoring, metabolic disease processes. Predictive capability now exists for T1D in high-risk individuals. Preventive capability is yet to materialize.
How do occupational health clinicians assist workers with abnormal glucose identified with biometric screening, or known T1D? A clear understanding of the pathophysiologic background and diagnostic criteria of T1D, along with the newest recommendations for screening first degree relatives can guide both primary and secondary prevention strategies. Although beyond the scope of this article, knowledge of insulin injection devices, storage, onset of action, and duration is essential. Review of workplace protocols for the treatment of hypoglycemia in the workplace is also recommended.
Given the physical and often emotional burden of diabetes, occupational health nurses are well positioned to promote social connectedness and advocacy for workers with diabetes. Platforms for workers with T1D to stay informed, proactive, and connected include Type One Nation, Patients Like Me (2017), Type 1 Diabetes TrialNet (2017; clinical research studies), City of Hope, Juvenile Diabetes Research Foundation (JDRF; 2017), and Helmsley Charitable Trust (2017), among others. Table 4 highlights these platforms, a useful resource for occupational health nurses and affected workers.
Social, Research, and Advocacy Platforms for Type I Diabetes
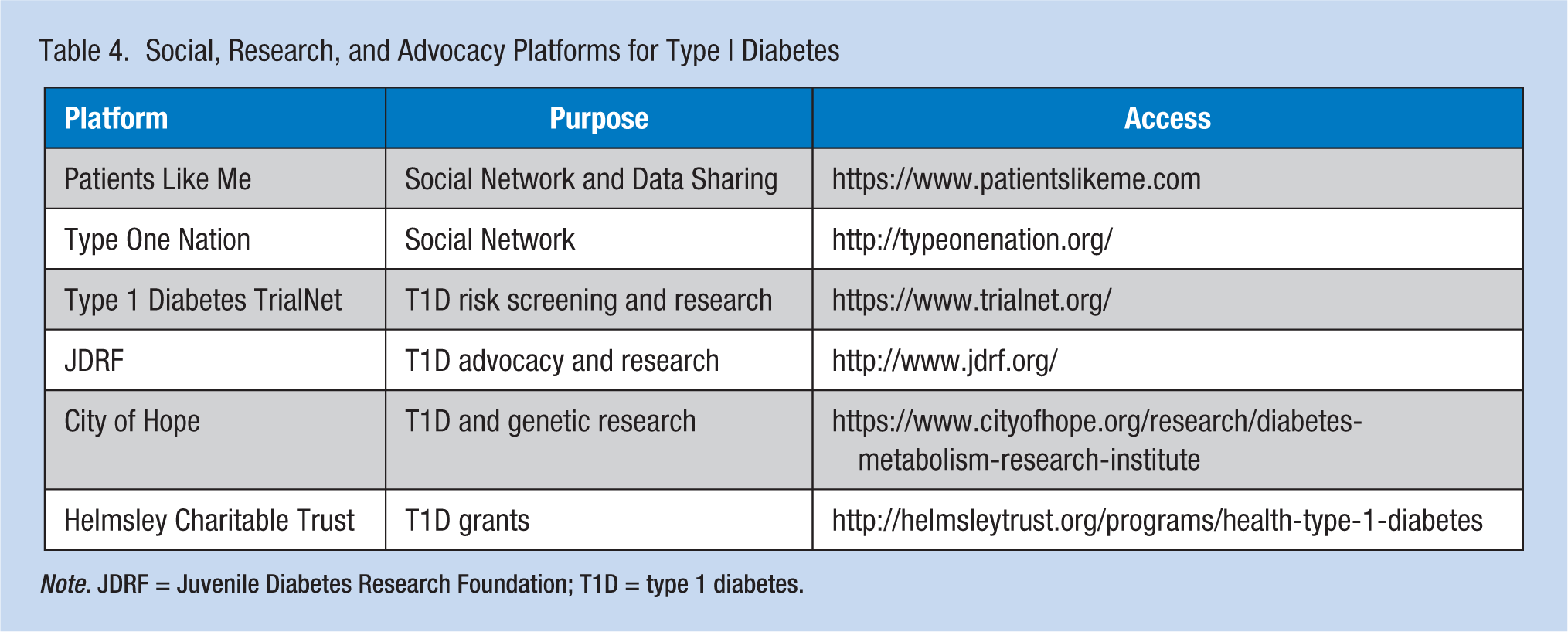
Note. JDRF = Juvenile Diabetes Research Foundation; T1D = type 1 diabetes.
Footnotes
Conflict of Interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Author Biography
Karla K. Giese is a board certified advance diabetes management (BC-ADM) diabetes specialist and director of diabetes quality in a nursing modeled, nationally accredited diabetes clinic in Albuquerque, NM. She is also an assistant professor in the DNP and MSN programs at Liberty University.