
Abstract
This article, the first in a two-part series, reviews and examines the components of clinical nutrition. In Part 1, the authors introduce the concept of nutrition and the role it plays in supporting healthy employees, current guidelines, and recommendations for determining healthy eating and the nutritional component of carbohydrates. In Part 2, the components of fats, proteins, vitamins, minerals, and water, and a resource guide are provided for the occupational health nurse to assist in the implementation of employee education in the area of healthy nutrition. The intent of the articles is to acquaint and inform occupational health nurses on the current guidelines for healthy eating so they can better appraise their employee population, thus creating a healthier workforce. The information provided is not all-inclusive on the topics discussed, but provides a foundation to understand the requirements for a healthier workforce.
Keywords
Occupational health nurses possess both the skills and capabilities to develop and implement workplace programs which promote healthy lifestyles. In a 2012 study, the American Association of Occupational Health Nurses, Inc. (AAOHN) surveyed 5,138 of their members to identify priority occupational health and safety issues. Forty-one percent of the members responded, and of those respondents, 61% reported health risk appraisal (HRA) priorities. Of those members, HRA priority areas included weight management/nutrition/healthy eating, physical activity, and mental health/stress management. These priorities were consistent across three industry sectors, three occupational health nurse job titles, and the smallest and largest employers (DeAngelis & Burgel, 2013), and could all be addressed through workplace health promotion programs. Health promotion has been linked to increased productivity, fewer health risks, and decreased use of health care resources (Baicker, Cutler, & Song, 2010). Therefore, it is imperative that occupational health nurses have resources necessary to educate their at-risk worker populations.
Occupational health professionals should be aware that diet reflects the variety of foods and beverages individuals consume over time in settings such as worksites, schools, restaurants, and homes (Reed, 2014). Interventions to support healthy eating and nutrition can ensure that workers have the knowledge and skills to make healthy food choices and are aware of healthier food options that are available and affordable to manage weight and prevent or manage chronic disease.
Healthy Diet
A healthy diet provides enough essential nutrients to avoid deficiencies but not excessive amounts which may increase the risk of chronic diseases or nutrient toxicities. Four of the 10 leading causes of death in the United States (i.e., heart disease, cancer, stroke, and diabetes) are associated with dietary excesses (Dudek, 2014). Individuals who are at a healthy weight are less likely to develop chronic disease risk factors, such as hypertension, obesity, and dyslipidemia (Slawson, Fitzgerald, & Morgan, 2013). A healthy diet has the potential to alleviate the high economic and personal costs of morbidity and mortality associated with these risk factors (Kochanek, Murphy, Xu, & Tejada-Vera, 2016).
Occupational health nurses should also be aware of social, cultural, and environmental factors (e.g., knowledge and attitudes, skill sets, social support, societal and cultural norms, food and agricultural policies, food assistance and programs) that influence workers’ diets (Lutz, Mazur, & Litch, 2014).
The environment and places where workers eat also appear to influence their diets (Higgs & Thomas, 2016). Because Americans spend about 30% of their lives working (Reference, n.d.), the workplace becomes influential in two ways: food availability at the workplace and as a classroom to educate employees. Availability of healthier foods can support workers in following healthful diets. Better access to retail venues that sell healthier options may have a positive impact on workers’ diets. For example, foods that are eaten away from home, such as the workplace, often have more calories and are of lower nutritional quality than foods prepared at home (U.S. Department of Agriculture, Economic Research Service [USDAERS], 2016). Marketing of food products such as “fast” and “convenient” also can influence food choices (Dimitri & Rogus, 2014). Due to the multitude of dietary influences, education by occupational health nurses is crucial to healthy living.
Those workers who eat healthy diets consume a variety of nutrient-dense foods within and across food groups, especially whole grains, fruits, vegetables, low-fat or fat-free milk or milk products, lean meats, and other protein sources. They limit the intake of saturated and trans fats, cholesterol, added sugars, sodium (salt), and alcohol as well as balancing caloric intake to meet caloric needs. A healthful diet reduces the risk factors for chronic disease and other health conditions (e.g., malnutrition, iron-deficiency anemia, heart disease, hypertension, dyslipidemia [abnormal lipid profiles], type 2 diabetes, osteoporosis, oral disease, constipation, diverticular disease, and some cancers; Grodner, Escott-Stump, & Dorner, 2016). To fully understand the impact of healthy diets, occupational health nurses must understand current recommendations and required dietary allowances for both macronutrients (fat, protein, carbohydrates) and micronutrients (vitamins and minerals). The Dietary Guidelines for Americans 2015-2020 is a critical tool which occupational health nurses can use to assist employees in learning how to make healthy food choices in their daily lives and, as a result, prevent chronic disease, prolong life expectancy, and increase productivity (Berry & Mirabito, 2011).
2015-2020 Dietary Guidelines for Americans
The Dietary Guidelines for Americans (Office of Disease Prevention Health Promotion [ODPHP], 2015) encourages the implementation of educational programs tailored to individuals and provides a foundation for changes to organizational practices, approaches, and policies that support healthy food choices, including places where food decisions are made (e.g., the workplace). Through the use of these guidelines and recommendations, the American workforce can become healthier. The key guidelines and website for the Dietary Guidelines for Americans (ODPHP, 2015) are displayed in Table 1.
2015-2020 Dietary Guidelines for Americans
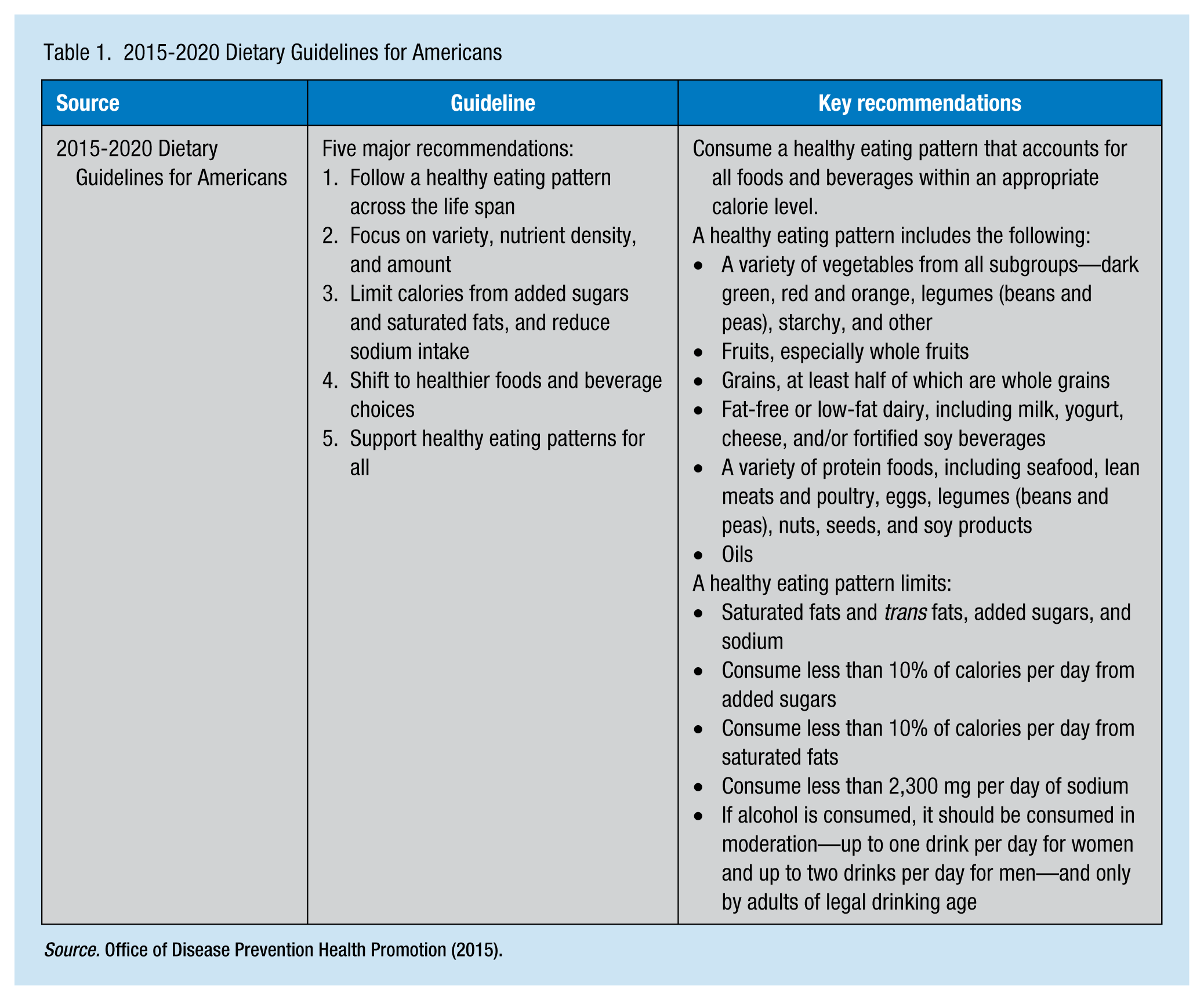
The key recommendations from the guidelines are quantitative and suggest a healthy eating pattern that includes a variety of nutrients from all subgroups (i.e., dark green, red, and orange vegetables; whole fruits, whole grains, fat-free or low-fat dairy; and a variety of protein sources). Dairy foods can include milk, yogurt, cheese, and fortified soy beverages, and protein foods including seafood, lean meats, poultry, eggs, legumes (beans and peas), nuts, seeds, and soy products.
The guidelines also categorize several dietary components that should be limited so individuals can achieve healthy eating patterns within caloric limits. These guidelines recommend consuming less than 10% of calories per day from added sugars, less than 10% of calories per day from saturated fats, and less than 2,300 milligrams per day of sodium; alcohol should be consumed in moderation (i.e., up to one drink per day for women and up to two drinks per day for men) if at all and only by adults of legal drinking age (Dudek, 2014).
MyPlate
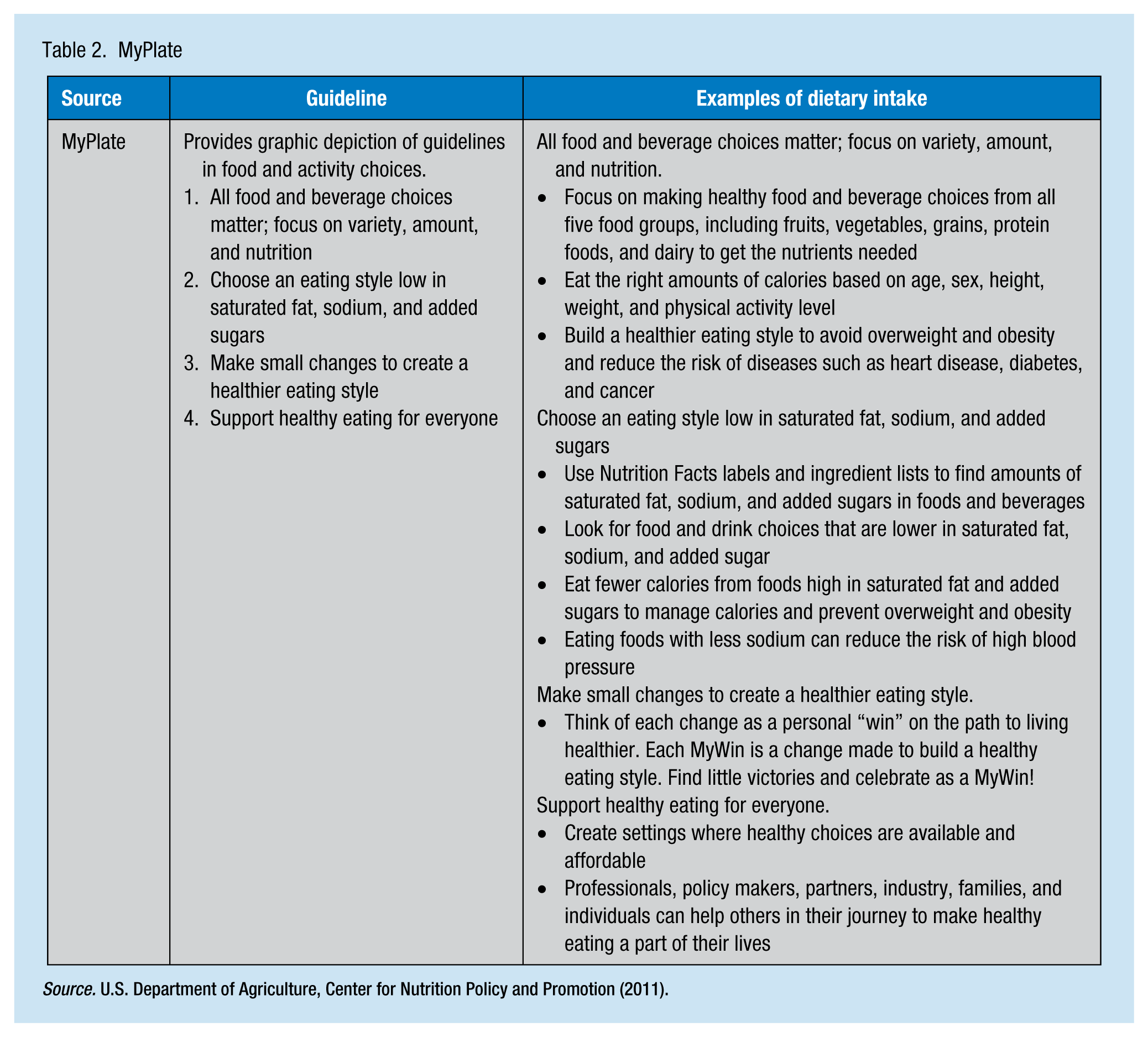
MyPlate is another tool which can be used by occupational health nurses to educate employees on healthy eating. In early 2011, MyPlate replaced MyPyramid; MyPlate is a new graphic by which the Dietary Guidelines for Americans (ODPHP, 2015) is translated into food and activity choices for healthy individuals older than 2 years of age (U.S. Department of Agriculture [USDA], Center for Nutrition Policy and Promotion, 2011). The belief is that nutrient needs should be met through food, not supplements. The graphic and its contents are designed to convey the concepts of variety, moderation, proportionality, and personalization as well as physical activity (see Figure 1).
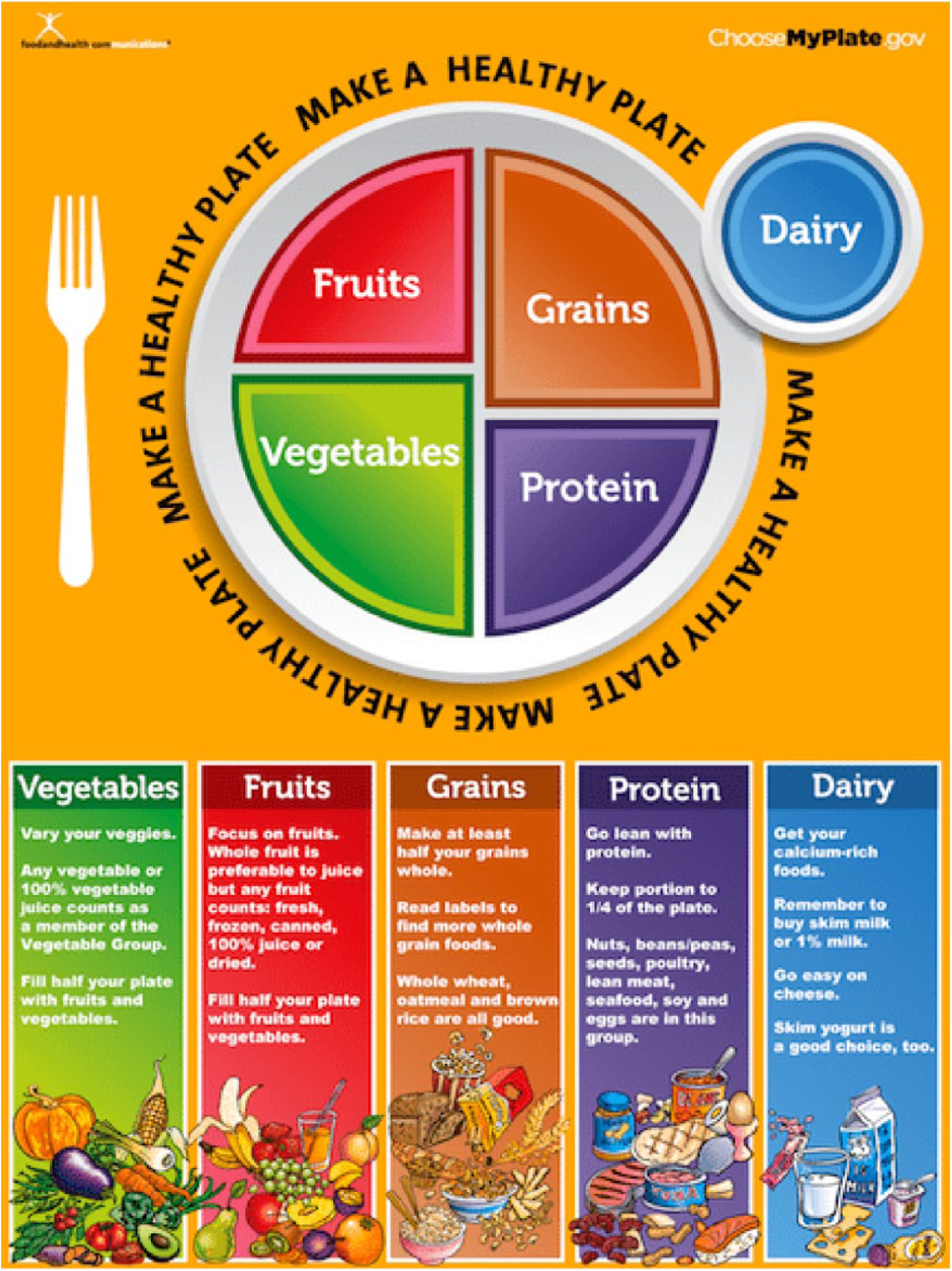
MyPlate.
The basic messages are centered on healthy choices which incorporate the five food groups and balance caloric intake with caloric expenditure to build a healthier eating style. The major guidelines of MyPlate, its website, and exemplars of dietary intake are found in Table 2. Two components of MyPlate which occupational health nurses can incorporate into health promotion programs are empty calories and serving and portion sizes. Empty calories have no nutritional value (e.g., alcohol and sugar). Only about 8% to 19% of daily calories should be empty calories, but Americans average 30% of calorie intake on empty calories (Britten, Cleveland, Koegel, Kuczynski, & Nickols-Richardson, 2012).
MyPlate
Serving size and portion size are also factors to consider with MyPlate recommendations. The MyPlate program now uses total amount per day, which estimates how many servings are in individual portion sizes. Serving size, the amount of food officially recommended, and portion size, the amount of food normally consumed, often differ (Cavanagh, Vartanian, Herman, & Polivy, 2014).
The above factors, empty calories and portion size, play a significant role in morbidity and mortality, and are two contributing factors to four of the 10 leading causes of death in the United States (i.e., heart disease, cancer, stroke, and diabetes; Kochanek et al., 2016). These statistics demonstrate the importance of a healthy diet. Worker education and counseling can increase awareness of the impact of food on overall well-being. Knowing the nutrient intake values of a healthy diet is the first step in that process. Numerous guidelines and recommendations can educate occupational health nurses, workers, and management.
Nutrient Intake Values
Although not designed as an educational tool, the Dietary Reference Intakes (DRIs) provide comparisons of estimated intake to estimated requirements. The DRIs not only advocate for nutrient levels that protect workers from nutrient deficiency diseases but also focus on reducing the risk of chronic diseases associated with dietary excesses (Dudek, 2014). The updated Recommended Dietary Allowances (RDAs), Estimated Average Requirements (EARs), Adequate Intake (AI), and Tolerable Upper Intake Level (UL) have a specific purpose, represent a specific level of intake, and are viewed as average daily intake over time, at least 1 week for most nutrients. Each area is exemplified in Table 3 to include definition, purpose, and application to practice.
Reference Values for the DRI
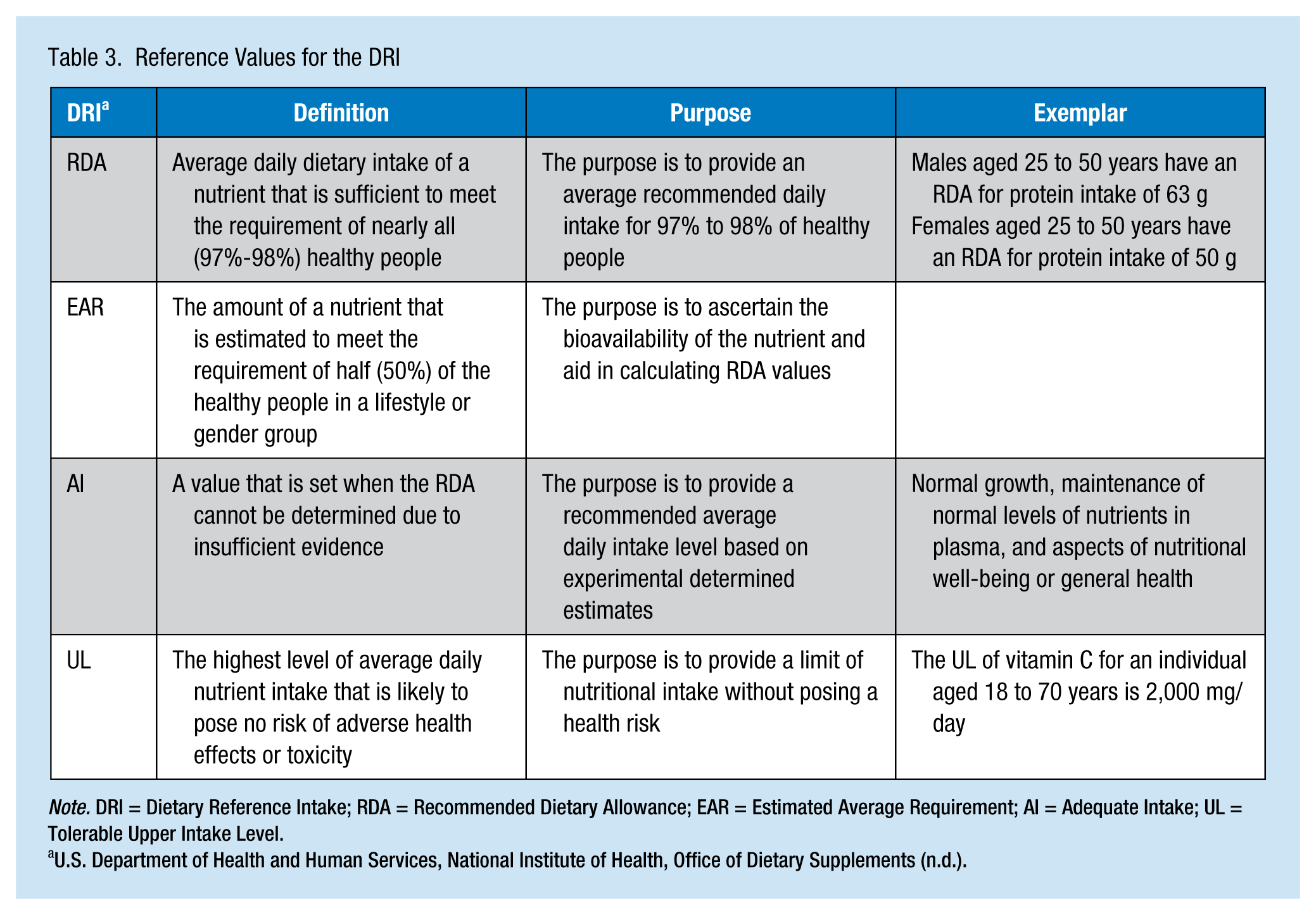
Note. DRI = Dietary Reference Intake; RDA = Recommended Dietary Allowance; EAR = Estimated Average Requirement; AI = Adequate Intake; UL = Tolerable Upper Intake Level.
These healthy eating pattern guidelines and DRI values correlate with recommended macronutrients (carbohydrates, fat, and protein) and micronutrients (vitamins, minerals, and water) needed to live a nutrient-wise, well-balanced, healthier life. Macronutrients and micronutrients will be reviewed in terms of DRIs and recommended eating patterns to improve understanding of these requirements. This information can be used in the creation of health promotion and disease prevention programs or counseling.
Macronutrients
Carbohydrates
Carbohydrates are more than just “sugar” and “starches”; carbohydrates provide the majority of calories in almost all human diets and are a class of energy-yielding nutrients that contain only carbon, hydrogen, and oxygen, hence the common abbreviation of CHO (Dudek, 2014). Carbohydrates are either simple with only one or two sugar molecules or complex with numerous sugar molecules.
Simple carbohydrates, monosaccharides and disaccharides, are the most common and simplest of all sugars. Monosaccharides include glucose, fructose, and galactose. Glucose, also known as dextrose, is a component of all disaccharides as well as the sugar which the body converts from all other digestible carbohydrates. The major role of glucose is to circulate through the blood providing energy to cells (Schorin, Sollid, & Smith, 2012). Fructose or “fruit sugar” is also a monosaccharide, the sweetest of all natural sugars. High-fructose corn syrup (HFCS), a form of fructose, is used heavily in food production (Ruff et al., 2015). The final monosaccharide, galactose, is not found in appreciable amounts in foods; galactose combines with glucose to form lactose. Glucose, fructose, and galactose are all absorbed without undergoing digestion.
The common disaccharides, sucrose, maltose, and lactose, are composed of two linked monosaccharides which must be reduced to monosaccharides before they can be absorbed. Sucrose, a combination of glucose and fructose, is refined to “table sugar” which can have harmful trace chemicals. All the minerals and vitamins which hold the two molecules (glucose and fructose) together are lost in the refining process. Maltose is also a disaccharide composed of two joined glucose molecules; although not found naturally in foods, the human body creates maltose from the consumption of potatoes and bread (i.e., white starches). Lactose or “milk sugar” is composed of glucose and galactose, and found naturally in milk; lactose is the least sweet of all sugars.
Complex carbohydrates, polysaccharides, include starch, glycogen, and fiber (Dudek, 2014). Plants synthesize glucose through photosynthesis and use it for energy. Leftover glucose is then stored as starch in the roots, seeds, or stems of plants; humans consume starch in plant grains. Starch is typically the foundation of all diets via potatoes, dried peas, and beans. Starches are not sweet because their molecules are too large to fit on the tongue’s taste buds.
Glycogen is an animal (including human) version of starch. It is stored in animal tissue but provides no benefit because glycogen is converted to lactic acid when animals are slaughtered. Humans store glycogen in the liver and muscles and use glycogen for energy as needed; after reducing glycogen to glucose, it is released into the bloodstream in between meals to maintain blood glucose levels (Jensen, 2012).
Fiber is generally considered a group name for polysaccharides that cannot be digested by human enzymes. The many forms of polysaccharides are commonly referred to as “roughage” because polysaccharides are found only in plants as a component of cell walls or cells themselves (Alpert, 2013). Roughage is categorized as insoluble or soluble. Soluble roughage dissolves in water, is fermented in the colon, and slows gastric emptying, which delays the rise in postprandial blood glucose and lowers serum cholesterol. Insoluble fiber does not dissolve in water and provides bulk to the large intestines. Insoluble fiber provides a laxative effect by increasing stool size and is considered dietary fiber, natural fibers found in plants, or functional fiber that has been extracted from plants that are used specifically to benefit the human body. Dietary and functional fibers are listed as total fiber on food labels. Fiber is a source of energy for the colon lining but is not considered a source of human energy overall. Fiber plays a role in decreasing the incidence of colon cancer and lowering cholesterol (Hansen et al., 2012).
Sources of Carbohydrates
Carbohydrates are found in grains, vegetables, fruits, and dairy products. Grains consist of whole grains and refined grains. Whole grains consist of the entire kernel of the grain; can be cracked, ground, or milled into flour; and are composed of three parts (i.e., the bran, endosperm, germ [embryo]). Refined grains are rich in starch but lack the fiber, vitamins, trace minerals, fats, and phytochemicals found in whole grains due to the refining process (Tosh, 2015). Examples of these include white flour, white bread, white rice, and refined cornmeal which is all then fortified (Jacques et al., 2013). When educating workers about sources of carbohydrates, whole grains should always be emphasized as a healthier option than refined grains (Mobley, Slavin, & Hornick, 2013).
Vegetables are composed of starch and some sugars which provide the majority of calories. Starchy vegetables (e.g., corn, beans, and potatoes) provide 3 times more carbohydrates than the same amount of watery vegetables (e.g., carrots, asparagus, green beans, and tomatoes). Fruits are mainly composed of sugar (mostly fructose) with small amounts of starch and minute quantities of protein providing minor calories. Exceptions to this are avocado, olives, and coconut, for which the majority of calories are from fat. The skin of fruit is also a source of essential fiber.
Dairy products such as milk contain carbohydrates which is responsible for the majority of its calories. One cup of milk provides 12 grams of carbohydrates in the form of lactose (Dudek, 2014). Cheese is lactose-free, therefore has less carbohydrates, except cottage cheese which has about 6 grams of carbohydrates per cup. Ice cream and flavored yogurt have added sugars which add to the amount of carbohydrates in the product but are empty calories.
Empty calories play a significant role in carbohydrate content in the American diet. Extra added sugars and syrups can elevate the carbohydrate content but vary by product. Soda is one example of empty calories, with 100% added sugar, meaning it is made from “straight sugar” and has no nutritional value.
Recommended Intake of Carbohydrates
The Dietary Guidelines for Americans (ODPHP, 2015) recommends that carbohydrates compose 45% to 65% of total daily calories, which translates to between 225 and 325 grams of carbohydrates a day in a typical 2,000 calorie a day diet (i.e., if four calories to each gram of carbohydrate, then approximately 900-1,300 calories of this diet would consist of carbohydrates). The RDA for carbohydrates is 130 grams for both adults and children, so the typical amount consumed by Americans is above the RDA.
The adequate range for total fiber is set at 14 grams for every 1,000 calories consumed per day (Dudek, 2014), approximately 28 grams of fiber for a 2,000 calorie a day diet. In 2014, it was found that the mean dietary fiber intake of all individuals 2 years and older in the United States, excluding breastfed children, was 16 grams per day (Hoy & Goldman, 2014), well below recommended intake. Adequate fiber intake has been linked to less risk of heart disease, cancer (specifically colon), type 2 diabetes, and obesity (Mobley et al., 2013). Therefore, fiber and whole grains should be the staple of carbohydrate consumption. Dietary guidelines recommend that adults and children consume at least one half of their grain servings from whole grains. Some tips for choosing whole grains include replacing refined grains with whole grains, choosing a ready-to-eat cereal with 5 grams of fiber or more per serving, eating dried peas and beans 2 to 3 times per week, and eating at least five servings of fruits and vegetables daily. Factors often contributing to the low intake of whole grains include consumers’ inability to identify whole grains, little awareness of the health benefits of whole grains, and the cost, taste, and unfamiliarity with how to prepare whole grains (Mobley et al., 2013).
The Dietary Guidelines for Americans (ODPHP, 2015) recommends that added sugars be limited to 10% of daily calorie intake. Added sugars account on average for almost 270 calories or more than 13% of consumed calories per day in the U.S. population. The American Heart Association (2014) suggests an added-sugar limit of no more than 100 calories per day (about six teaspoons or 24 grams of sugar) for most women and no more than 150 calories per day (about nine teaspoons or 36 grams of sugar) for most men (American Heart Association, 2014). The most common sources of added sugars in the American diet include soft drinks, cakes, cookies, pies, fruit drinks, dairy desserts such as ice cream, and candy.
One way to limit added dietary sugars is to use sugar alternatives (i.e., sugar alcohols and nonnutritive sweeteners). Sugar alcohols (e.g., sorbitol, mannitol, and xylitol) are natural sweeteners derived from monosaccharides. High consumption of these products can cause a laxative effect. Nonnutritive sweeteners are virtually calorie free, are sweeter than sugar, and do not raise blood glucose levels (Antenucci & Hayes, 2015).
Summary
This article, the first in a two-part series, reviewed the recommendations and guidelines for nutritional health as well as the first macronutrient, carbohydrate. In Part 2 of the series, the authors will discuss macronutrients (fat and protein) and micronutrients. Informational resources will also be provided to evaluate nutritional status as well as educational resources occupational health nurses can use in educating their employees about healthy eating.
Footnotes
Conflict of Interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Author Biographies
Rebecca Toothaker is an assistant professor of nursing at Bloomsburg University. She has recently published her dissertation on Millennial Nursing Students in Traditional Educational Programs.
Noreen Chikotas is a professor of nursing at Bloomsburg University. She has been a nurse educator for 20 years and has practiced as a CRNP in occupational health for more than 10 years. She has published and presented on both clinical issues and instructional strategies.