
Abstract
The transient nature of construction work makes it difficult to conduct longitudinal worksite-based health promotion activities. As part of a workplace health assessment pilot study, we worked with a commercial lunch truck company to disseminate four types of health education materials including cancer screening, workplace injury prevention, fruit and vegetable consumption, and smoking cessation to construction workers purchasing food items from the truck during their job breaks. Two weeks following the worksite assessment, we followed up with these workers to ascertain their use of the health promotion materials. Of the 54 workers surveyed, 83% reported reviewing and sharing the cancer screening materials with their families, whereas 44% discussed the cancer screening materials with coworkers. Similar proportions of workers reviewed, shared, and discussed the other health promotion materials with their family. Lunch trucks may be an effective strategy and delivery method for educating construction workers on healthy behaviors and injury prevention practices.
Keywords
Introduction
Construction workers, compared with other worker groups or industries in the United States, have documented higher levels of tobacco use (23.4% vs. 15.4%, all U.S. workers; Chin, Hong, Gillen, Bates, & Okechukwu, 2013), respiratory disease such as pneumoconiosis (10.0% vs. 5.9%, all U.S. workers; Hnizdo, Berry, Hakobyan, Beeckman-Wagner, & Catlett, 2011; National Institute for Occupational Safety and Health, Centers for Disease Control and Prevention, 2018), musculoskeletal disorders such as low back pain (31.8% vs. 25.7%, all U.S. workers Caban-Martinez et al., 2010; Yang, Haldeman, Lu, & Baker, 2016), and fatal workplace injuries (10.1% vs. 3.6%, of all U.S. workers; U.S. Department of Labor, Bureau of Labor Statistics, 2017; van der Molen et al., 2012). Although health promotion strategies among this occupational group are clearly needed, the transient nature of construction work makes it difficult to not only implement but also deliver sustainable health promotion activities to this worker group (Carley, Haas, Borcherding, & Goodrum, 2003; Lingard & Turner, 2017). Among nonunionized trades in the construction industry, which can account for 84% of the private sector construction positions in the United States and Florida (U.S. Department of Labor, Bureau of Labor Statistics, 2013), opportunities for continuing health and safety education are limited (Hnizdo et al., 2011; Viester et al., 2012), creating a need for new methods to reach this transient workforce.
Few studies have developed effective worksite health promotion strategies targeting construction workers (Viester, Verhagen, Bongers, & van der Beek, 2015). One potential promising outreach strategy is to engage with the construction worksite lunch trucks as a method to disseminate health and safety information at the jobsite. These trucks are commonly seen on commercial construction worksites catering various breakfast and lunch options to the workers during their breaks. They are privately owned trucks and operators coordinate with construction site management for catering food options to the workers during specific break times throughout the day at the jobsite. Although most commercial construction worksites differ in terms of the frequency and length of worker breaks, there is often a short morning breakfast and a lengthier midday lunch break, approximately 20 to 45 minutes in length, respectively.
In April 2010, we collaborated with a local lunch truck company to engage construction workers in Miami, Florida to (a) conduct a workplace health assessment for tobacco exposure and musculoskeletal disorders, (b) assess the use of a handheld electronic device to collect health information, and (c) assess the feasibility of the lunch truck at disseminating health promotion and safety information. Although findings for the first two objectives are presented elsewhere (Caban-Martinez, Clarke, Davila, Fleming, & Lee, 2011; Caban-Martinez et al., 2010), this research report focuses on our third objective to examine if construction workers reviewed and shared the health promotion and worksite injury prevention materials distributed via the lunch truck.
Materials and Methods
Sample and Recruitment
We partnered with a Miami-based lunch truck company that visits approximately four construction sites 2 times per day to conduct a tobacco and musculoskeletal disorders health assessment as well as deliver health promotion materials to construction workers. For this pilot project, our research team accompanied the lunch truck to two commercial constructions sites 2 times a day for 3 consecutive days. Although the truck was at the jobsite catering food to the construction workers, bilingual student interviewers engaged the workers and described the purpose of the study. A total of 57 workers, who were at least 18 years of age, were invited to participate in the health assessment. Greater details about recruitment and health assessment are described elsewhere (Caban-Martinez et al., 2011; Caban-Martinez et al., 2010). About 54 of the 57 workers approached agreed to participate in the study (participation rate = 94.7%).
Health Promotion Materials
Following the completion of the health assessment protocol (i.e., self-report questionnaire, anthropometric measurements, and biological samples; Caban-Martinez et al., 2011; Caban-Martinez et al., 2010), we provided each worker a drawstring book-bag containing Centers for Disease Control and Prevention, the National Institute for Occupational Safety and Health, and the National Institutes of Health-developed health promotion materials on the following: Tobacco exposure/smoking cessation (Centers for Disease Control and Prevention [CDC], 2017b), cancer screening (CDC, 2017a), workplace injury prevention (i.e., falls; National Institute for Occupational Safety and Health, 2017), and fruit and vegetable consumption (CDC, 2011). These health promotion materials were available in English and Spanish.
Data Collection
All 54 construction workers enrolled in the study, consented to a follow-up questionnaire that was administered via telephone or email at 2 weeks from when the research team conducted the health assessment at the jobsite. A maximum of four attempts were made to reach each of the 54 workers, with most reached after two attempts through their preferred communication mechanism.
2-Week Follow-Up Survey Instrument
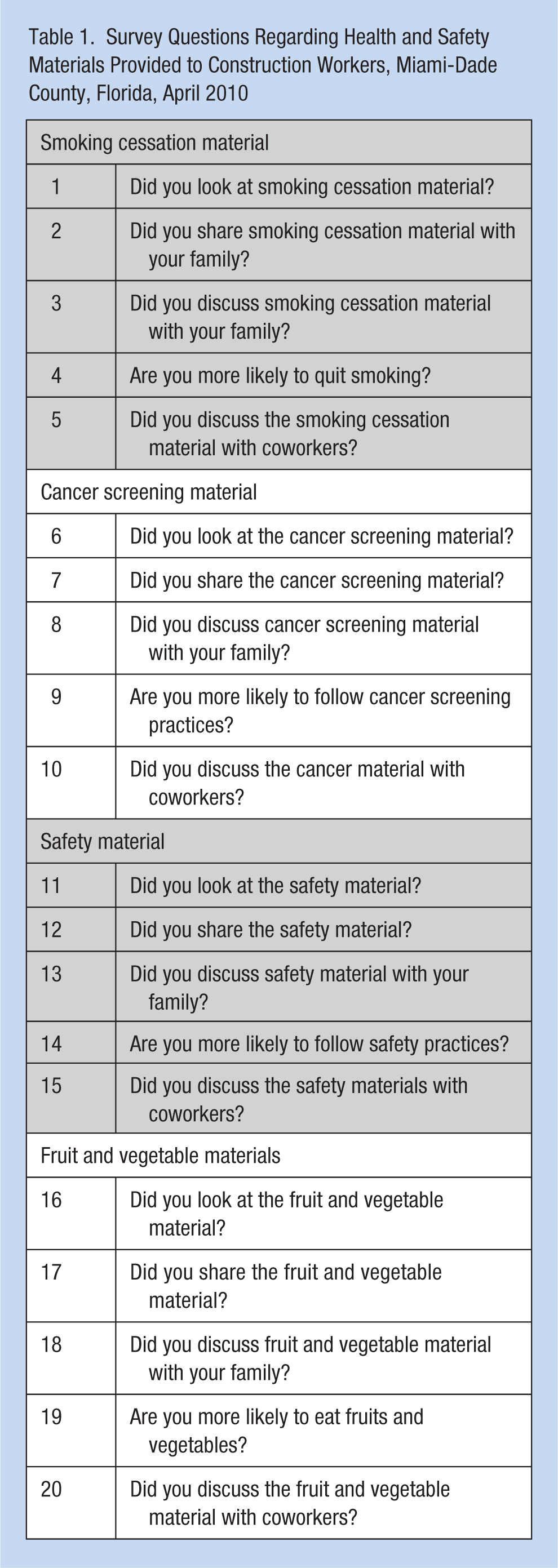
We designed and administered a 20-item follow-up survey instrument assessing review, sharing, and discussion activities by the construction workers for each of the four health promotion materials (Table 1). For each, they were asked the following: (a) if they looked at the materials, (b) if they shared the materials with any family members, (c) discussed the materials with any family members, (d) were they more likely now to practice what they reviewed, and (e) did they discuss the materials with their coworkers? The three response options for each question included the following: (a) yes, (b) no, or (c) don’t know/not sure. Each measure was adapted from the validated CDC Worksite Health Score Card (Roemer et al., 2013). The draft survey was evaluated prior to field use for face, content, and current validity. We administered the draft survey instrument through key informant interviews to occupational health and safety experts as well as with general labor construction workers (in English and Spanish) at the target worksites to assess interpretation of the question stems and response items. Reliability and internal consistency of the scale and its subscales were supported by respectable Cronbach’s alpha coefficients cancer screening (.95), workplace safety and injury prevention (.84), fruit and vegetable consumption (.88), and smoking cessation (.78). In addition, consistency between test–retest samples separated by 2 weeks were indicated by acceptable correlation coefficients between the scale and sociodemographic characteristics: Pearson Correlations Coefficients (.64-.72). We also collected the sociodemographic characteristics (age, race, ethnicity, material status, income, and health insurance status) reported by the workers on the baseline workplace assessment survey. Measures on sociodemographic characteristics were adapted from the validated U.S. National Health Interview Survey (Botman, Moore, Moriarity, & Parsons, 2000). Participants were mailed a US$10 gift card for completing the follow-up survey. The study protocol was approved by the University of Miami’s Institutional Review Board.
Survey Questions Regarding Health and Safety Materials Provided to Construction Workers, Miami-Dade County, Florida, April 2010
Data Analysis
Continuous variables were expressed as mean ± the standard error of the mean, and categorical variables as frequency and percent. We also conducted a subgroup analysis of construction workers who reported currently smoking tobacco to assess their review, sharing, and dissemination of the smoking cessation materials. Statistical analysis of survey data was performed with SAS 9.3 software (SAS Institute, Inc., Cary, NC, USA).
Results
Sociodemographic Characteristics
The sample mean age of the construction workers was 42.4 years (±12.3 years), ranging from 23 to 74 years of age (Table 2). The sample was entirely male (100%, n = 54 workers), and 91% (n = 49) self-identified as Hispanic/Latino descent. About 20% (n = 10) of construction workers reported having some type of health insurance.
Sociodemographic Characteristics of Construction Workers Participating in the Workplace Health and Safety Pilot Project, April 2010 (n = 54)
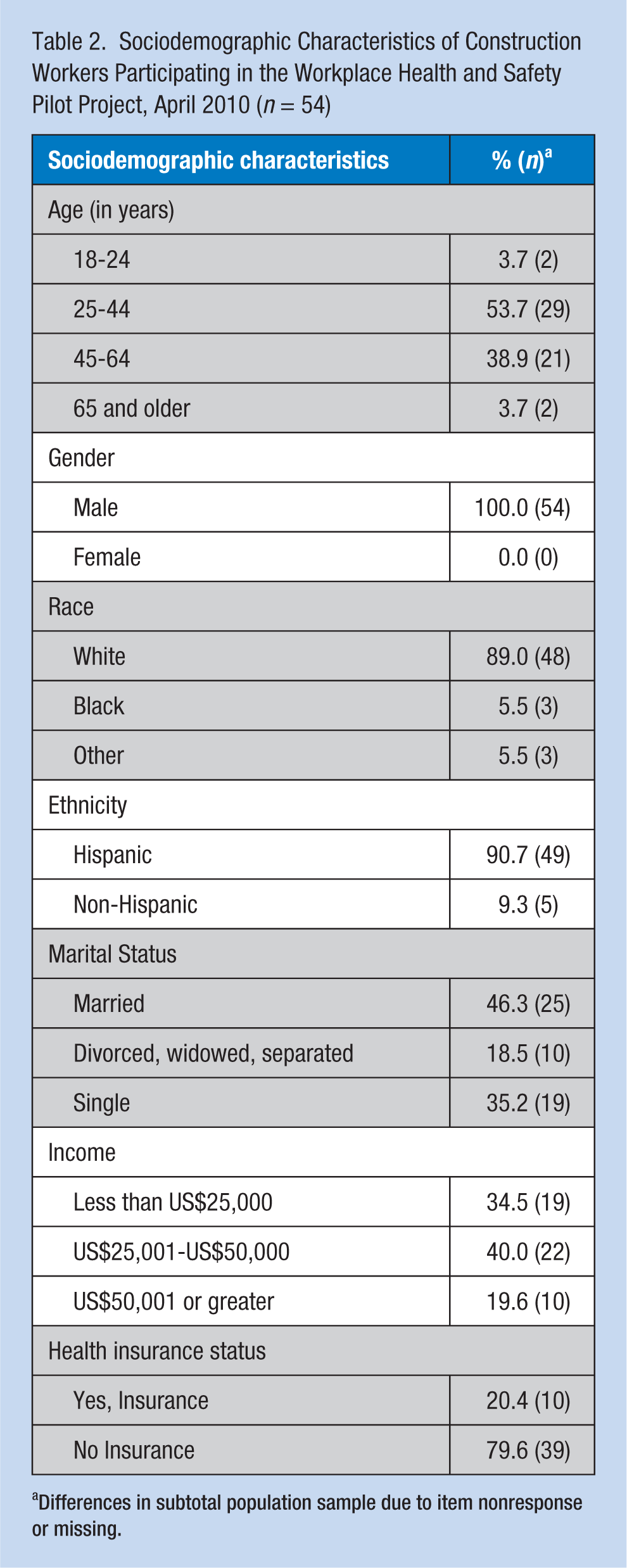
Differences in subtotal population sample due to item nonresponse or missing.
2-Week Follow-Up Survey
All 54 workers completed the follow-up survey. About 69% (n = 37) of construction workers read the materials on tobacco exposure and smoking cessation, 54% (n = 29) shared and 50% (n = 27) discussed the information with family, and 26% (n = 14) discussed the materials with coworkers. The proportion of workers reviewing, discussing, and sharing the other (i.e., cancer, injury prevention, and fruit/vegetable consumption) health promotion materials is presented in Figure 1. About 83% (n = 45) of the workers reported that they reviewed the cancer screening material, and 44% (n = 24) stated that they discussed the cancer screening materials with coworkers. More than 83% (n = 45) of workers also shared and discussed the cancer screening with their families.
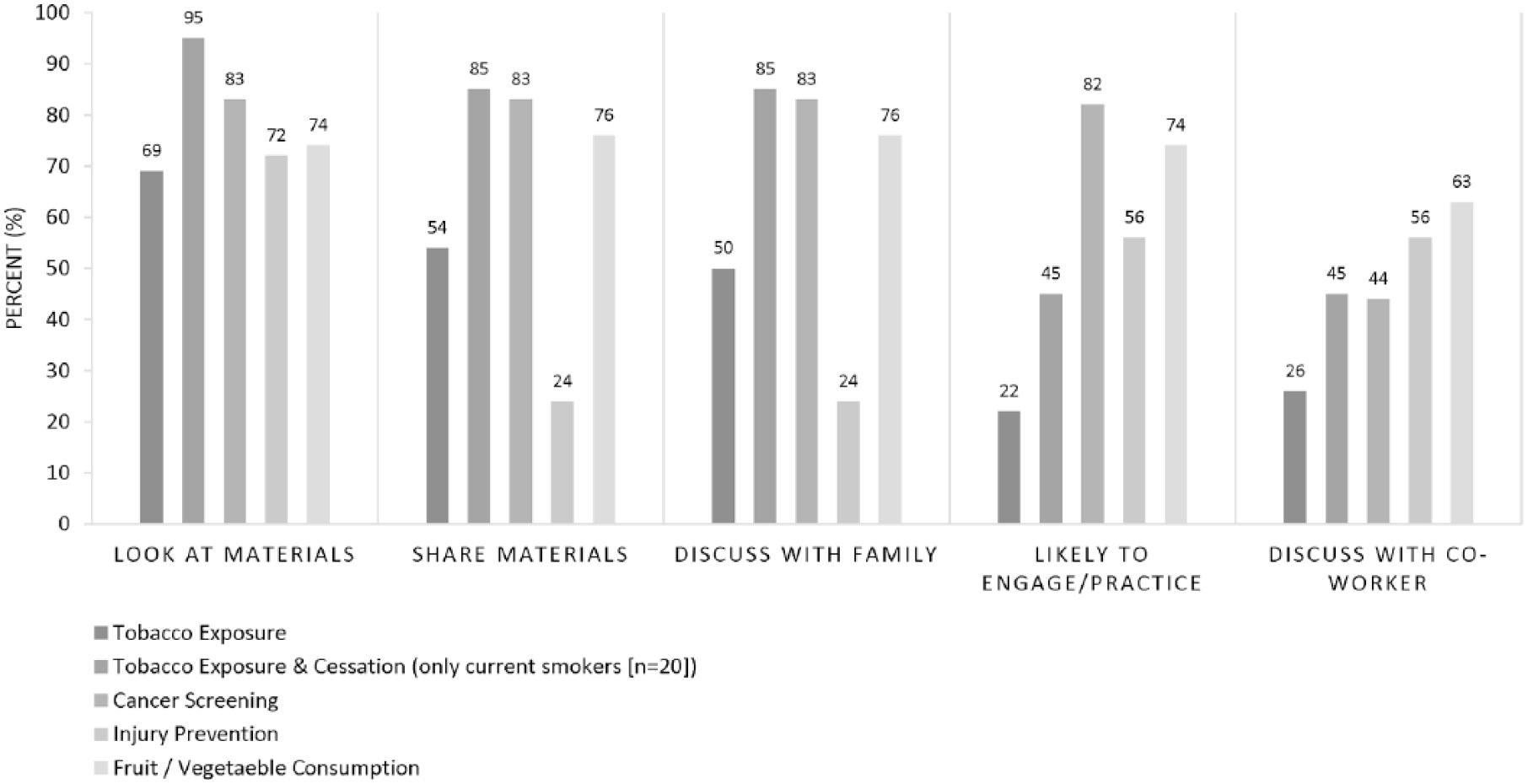
Percentage of construction workers using workplace health promotion materials at 2 weeks following distribution at the worksite via the lunch truck (n = 54).
Subgroup Analysis of Smokers
We analyzed the tobacco exposure and smoking cessation material callback response among workers in our sample who reported being current smokers (n = 20). More than 95% (n = 19) of current smokers reported reading the tobacco materials, 85% (n = 17) both shared and discussed it with family members, and 45% (n = 9) discussed it with coworkers. In addition, 45% (n = 9) of current smokers reported being more likely to quit smoking and reduce tobacco exposures as they reviewed the smoking cessation materials given to them at the lunch truck.
Discussion
In this pilot study comprised of predominantly Hispanic construction workers, we found that workers were willing to receive work-related health and safety information via a lunch truck during their breaks. The lunch truck provided a unique mechanism to disseminate these materials. More than three fourths of the workers sampled reported reading, sharing, and discussing the health materials with family members and coworkers. The materials most read and discussed by workers were those related to smoking cessation and cancer screening, which is consistent with trends showing high rates of smoking among construction workers, and high rates of cancer screening among Hispanics (Emmons et al., 2011; Lee et al., 2007). However, health materials on safety and injuries were read and discussed less. Although our pilot study did not assess reasons for sharing or not sharing information received, we theorized that workers may have already received some type of safety information as part of their usual worksite or orientation training, or the information we presented was not presented in an interesting enough fashion.
A few study limitations should be noted. The data collected as part of the 20-item follow-up survey are self-reported, and it is not possible to discern if the workers truly read the health promotion materials themselves or shared/discussed it with their family members. As we did not partner with the general contractor of two construction sites visited for this pilot study, we are not aware of the total number of workers on the site. It is also not possible to determine which workers use the lunch truck to consume meals at the jobsite as compared with those that might visit other local food options or bring food from home. One of the challenges in working with the lunch truck was the limited space to carry health assessment equipment and health promotion materials. Finally, the time period to engage workers (20 minutes at breakfast and 45 minutes at lunch) is hectic and limits the number of surveys and assessment activities that could be completed while allowing workers some time to eat during their break.
The findings in this study support several occupational and environmental health nursing roles and functions, including counseling, health promotion, risk reduction, and workplace hazard detection. Occupational health nurses could collaborate with lunch truck operators to deliver specific health education and health promotion materials and resources to worker group often of low socioeconomic status and varying minority ethnicities and races (i.e., Latinos and African Americans). In partnership with the general construction firm, the lunch truck visitation period, although brief (approximately 20 minutes) at the jobsite, could create an opportunity for teachable moments for workers including using a toolbox talk format to deliver specific health education interventions such as smoking cessation, or respiratory mask use. In addition, the lunch truck visitation could allow for brief, specific workplace hazard detection such as carbon monoxide or lead screening. Taken together, these health and safety activities delivered in concert with lunch truck visitation periods could improve access and delivery of key occupational health and safety messages to the construction workforce.
Commercial construction sites are dynamic workspaces where worker entry and exit assignments change quickly (Sparer et al., 2014). The worksite lunch truck provides a new approach to engage and conduct workplace health assessment and health promotion activities that improve the health and safety of construction workers (Oude Hengel et al., 2011), particularly among workers in a nonunionized setting. The management staff of construction worksites may benefit in partnering with a lunch truck service beyond granting access rights to the jobsite and include activities to conduct health assessments (i.e., vision and hearing testing, tobacco exposure assays), and health promotion (i.e., fall prevention) information. Furthermore, research is needed to evaluate the efficacy and reach of a lunch truck health promotion activity among workers on the construction site. Health and safety activities delivered by occupational health nurses in concert with lunch truck operators could create a venue at the worksite to engage a large proportion of construction workers.
Footnotes
Acknowledgements
The authors would like to thank all the constructions workers and the construction firms that participated in the research study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Funding support to accomplish the research was largely supported by the National Institute for Occupational Safety and Health’s (NIOSH) Deep South Educational Research Center at the University of Alabama (Subcontract: 288477-10; Prime Award NIOSH T42OH008436) and NIOSH Grant K01OH010485-01.
Institution and Ethics Approval
The study protocol was reviewed and approved by the Institutional Review Board of the University of Miami, Miller School of Medicine (ID: 20090945).
Author Biographies
Alberto J. Caban-Martinez is an Assistant Professor of Public Health Sciences and Director of the Environmental and Occupational Health Lab at the University of Miami, Miller School of Medicine. He also served as Principal Investigator of the NIOSH Pilot Program Grant from the Deep South Educational Research Center at the University of Alabama at Birmingham that funded this project. He conceptualized the idea of a lunch truck model to bring health promotion and health education activities to construction worksites.
Kevin J. Moore is a research assistant in the Caban-Martinez Environmental and Occupational Health Lab, and a fourth-year MD-MPH student at the University of Miami, Miller School of Medicine, and lead aspects of the lunch truck study.
Tainya C. Clarke is a health scientist and biostatistician and volunteer health scientist at the University of Miami, Miller School of Medicine where she provides statistical guidance across construction worker research projects.
Evelyn P. Davila is a co-investigator, and volunteer scientist at the University of Miami, Miller School of Medicine. She co-lead the collection, management, and interpretation of survey and biological data collected as part of this project.
John D. Clark III is a co-investigator and volunteer scientist at the University of Miami, Miller School of Medicine. He co-lead the collection, management, and interpretation of survey and biological data collected as part of this project.
David J. Lee is Professor, and the Director of Graduate Public Health Programs at the University of Miami, Miller School of Medicine. He is a co-investigator and senior mentor in the conceptualization of the research project. He also assisted in the collection, analysis and interpretation of survey and biological data collected as part of this project.
Lora E. Fleming is Professor Emeritus at the University of Miami, Miller School of Medicine and Professor, Chair, and Director of the European Centre for Environment and Human Health at the University of Exeter Medical School. She is a co-investigator and senior mentor in the conceptualization of the research project. She also assisted in the collection, analysis and interpretation of survey and biological data collected as part of this project.