
Abstract
Although small-scale enterprises (SSEs) dominate the private enterprise sector, knowledge about support for these organizations from occupational health services (OHSs) is insufficient. The aim of this research was to study OHS services provided and staff cooperation with SSEs in Norway and Sweden. In total, 87 Norwegian and 51 Swedish OHS providers answered a survey on their experiences providing requested services from and cooperation with SSEs. Based on survey questions and constructed indices, providers in the two countries were compared using independent sample t tests and non-parametric tests. Open-ended questions were analyzed using qualitative content analysis. The results showed that SSEs, particularly in industrial, construction, and trade sectors, commonly contract for Norwegian and Swedish OHSs, and these contracts have increased in the last 12 months. Norwegian providers state that SSEs request broader organizationally- based services; their Swedish counterparts request more individual-based health-related services. Improvements concerning specific strategies for OHS collaboration with SSEs may be needed.
Keywords
Approximately one third of the Norwegian and Swedish workforce employed in the private sector work for small-scale enterprises (SSEs) with less than 20 employees, approximately 95% of all private enterprises in the two countries (Statistics Norway [SSB], 2015; Statistics Sweden [SCB], 2014). In Sweden, 62% of the workforce has access to occupational health services (OHSs; Swedish Work Environment Authority, 2014). Depending on the sector, 10% to 55% of Swedish employees in SSEs have access to OHSs (Gunnarsson, Andersson, & Josephson, 2011). In Norway, approximately half of the workforce has access to OHSs (Moen, Hanoa, Lie, & Larsen, 2015), but the coverage is less in small enterprises (Josefsson & Kindenberg, 2004).
SSEs operate in many sectors but are most common in agriculture, legal and financial services, retail, construction, and manufacturing (Gunnarsson, 2010). Several studies show that the majority of SSEs pay little attention to occupational health and safety issues (Andersson & Hägg, 2006; Breucker, 2001; Hasle & Limborg, 2006) and that specific strategies are needed to focus attention on these issues in SSEs (European Agency for Safety and Health at Work, 2004). Also, several studies show that SSEs, particularly in some sectors, have an at-risk physical work environment; reasons for these hazards might be lack of understanding and problems in organizing systematic occupational health and safety management (OHSM; Bornberger-Dankvardt, Ohlson, & Westerholm, 2003; Frick, Langaa Jensen, Quinlan, & Wilhagen, 2000; Hasle & Limborg, 2006; Vinberg, 2006). Occupational health and safety management promotes the use of systematic managerial processes to detect, abate, and prevent workplace hazards. This approach has been voluntarily assumed by an increasing number of larger enterprises (Frick et al., 2000). Another reason, apart from higher exposure to physical work environment risks in SSEs than in larger companies, is the diversity of tasks performed by only a few employees (Antonsson, Birgersdotter, & Bornberger-Dankvardt, 2002). Some researchers also point out that SSEs have limited competence in creating health-promoting workplaces (Moser & Karlqvist, 2004; Torp & Moen, 2006; Wilson, DeJoy, Vandenberg, Richardson, & McGrath, 2004). Psychosocial work conditions are somewhat different from physical work conditions. In SSEs, the distance from decision-maker to employee is short; both leaders and employees have considerable control of their work tasks (Bornberger-Dankvardt et al., 2003; Lindström, Schrey, Ahonen, & Kaleva, 2000; Nordenmark, Vinberg, & Strandh, 2012; Sørensen, Hasle, & Bach, 2007). Some researchers even point out that, given the high job control and high job demands that characterize work in SSEs, one could argue that this form of employment provides prototypes of “active jobs” that can influence health positively (Stephan & Roesler, 2010).
Limited research concerning resources to support SSEs and cooperation between OHSs and SSEs has been published. However, a Swedish study of private enterprises (Schmidt, Sjöström, & Antonsson, 2011) showed that effective OHSM was a key factor in employees using OHSs. Efficient collaboration was highly dependent on a continuous dialogue between the company and the OHS, which needed to demonstrate flexibility and a willingness to adjust programs and services to meet employee needs (Schmidt et al., 2011). Both Norwegian and Swedish studies have found that OHSs were mainly used for individual health examinations and employee health care (Gunnarsson et al., 2011; Moen et al., 2015; Westerholm & Bostedt, 2004).
More research is needed about which resources OHSs are providing SSEs and how OHSs are cooperating with these enterprise groups. The aim of this study was to investigate the services OHSs are providing SSEs and OHSs’ cooperation with SSEs in Norway and Sweden by answering the following research questions:
OHS and Occupational Legislation in Norway and Sweden
In Norway, an OHS must be authorized by the Norwegian Labour Inspection Authority. Statutory criteria for authorization (Ministry of Labour and Social Affairs, 2005) include a quality assurance system and at least three full-time equivalent professionals with expertise in occupational medicine, occupational hygiene, ergonomics, psychosocial work environment, and systematic health, safety, and environment work. Some employers are obliged to have OHS because their employees are particularly vulnerable to physical or psychological illness or injury (Ministry of Labour and Social Affairs, 2005). In Sweden, the structure and organization of OHSs are described in the Work Environment Act (Ministry of Employment, 1977). In Sweden, anyone can open an OHS unit and sell OHS services with no need for official approval. However, in April 2014, the Swedish Social Insurance Agency introduced a temporary authorization procedure for OHSs to allow employers to apply for financial compensation if they are using OHSs for employees enrolled in vocational rehabilitation (Ministry of Health and Social Affairs, 2014a, 2014b). A voluntary quality system, based on ISO (International Standard Organization) 9001, has also been established, which leads to official certification issued by the Swedish Board for Accreditation and Conformity Assessment (SWEDAC; Gunnarsson et al., 2011).
Norwegian and Swedish laws for occupational health and safety are similar in that they require all companies to plan and implement policies regarding these issues systematically in the organization, and to work actively toward a safe and healthy work environment for their employees (Ministry of Labour and Social Affairs, 1996; Swedish Work Environment Authority, 2001).
Method
In total, 748 OHSs were identified (377 in Norway and 371 in Sweden) through official registries and the Swedish Association of Occupational Safety and Health. Exclusion criteria were as follows: OHSs without official approval from the Swedish Social Insurance Agency, contact person duplicates (where the branches have the same administrative leader), internal OHSs (e.g., OHS units in large corporate entity, state-owned corporations, private companies), and OHSs in the process of termination. Details are presented in Figure 1. After exclusions, the total Norwegian and Swedish sample consisted of 192 and 198, respectively. In total, 87 Norwegian and 51 Swedish OHSs completed the survey, a response rate of 45.3% and 25.8%, respectively, with a total response rate of 35.4%.
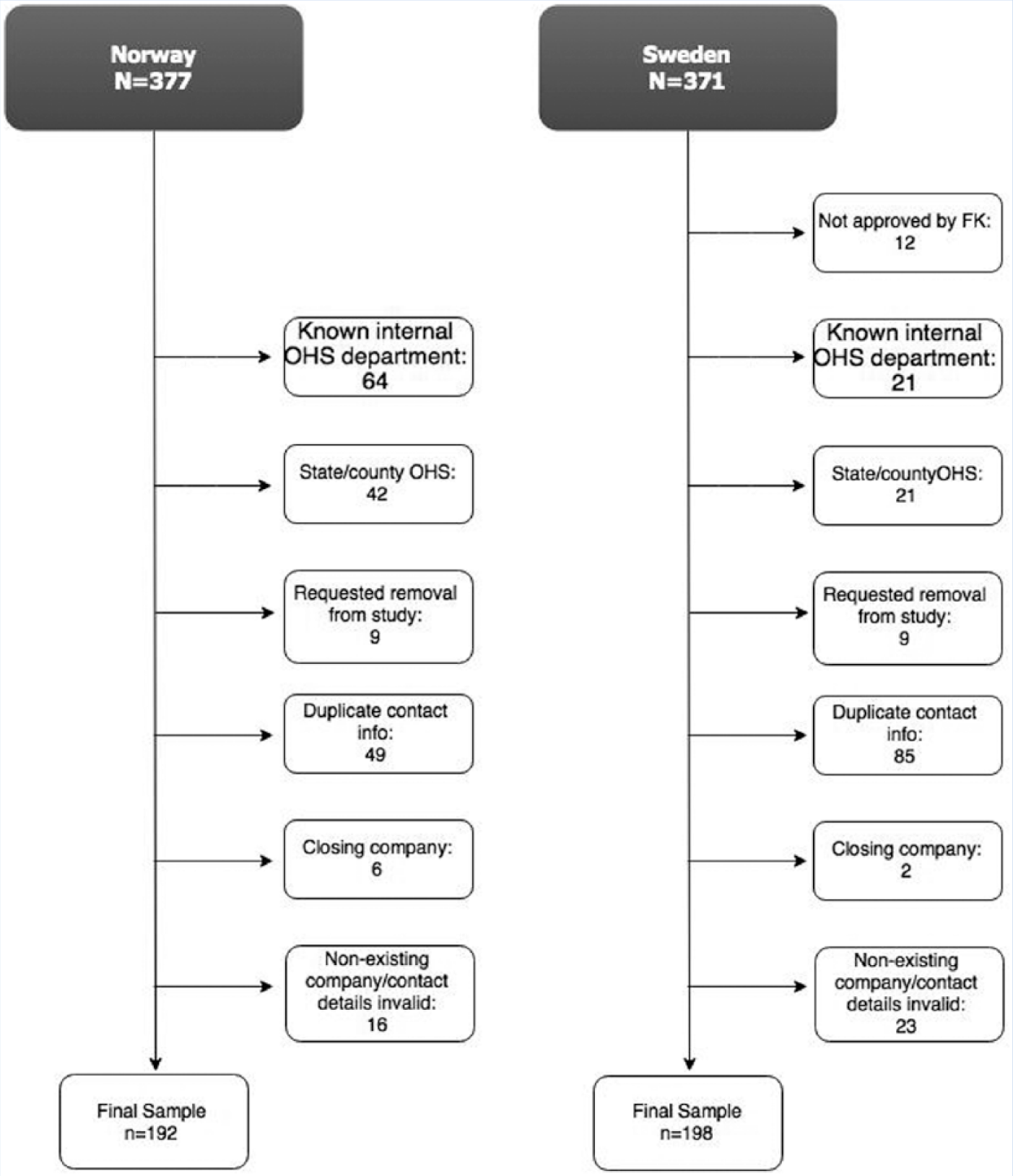
Flow chart.
The Survey
Questions were based on a recent survey from the Finnish Institute of Occupational Health, a component in developing a Finnish model of OHS practice for SSEs (Palmgren et al., 2015). The survey was translated from Finnish to Norwegian and Swedish by one of the authors with assistance from a bilingual Finn. The survey was translated back and forth twice allowing for cross-cultural adaptations as described by Beaton, Bombardier, Guillemin, and Ferraz (2000). The questionnaire was then adapted to apply to unique conditions in Norway and Sweden by removing some inappropriate questions and adding one question about which services were requested by customers. Two OHS providers in Norway and Sweden validated the final questionnaire prior to distribution.
The survey focused on how the providers experienced the following topics related to SSEs: organizational structure, number of customers and customers’ company sizes, range of services requested by the customer, customer-OHS cooperation and agreements, marketing, communication and cooperation, and challenges of the OHS in the future. Most of these questions had Likert-scale answers from always to never. The marketing questions had simple yes/no options, and additional marketing questions had text boxes for specifying details. The future development of OHSs to better reach SSEs was answered with 16 suggested changes; the respondents could select several answers in this section. The questions about the greatest challenges and possible solutions had optional open text boxes.
Data Collection
The survey was distributed solely via an electronic survey platform (SurveyGizmo) using e-mail invitations. The survey platform provided logical questioning, for example, a subsequent question was only visible for respondents answering “yes” to a prior question. Two reminders were sent to prospective participants a week apart.
Data Analysis
The quantitative data were tested for normality with the Shapiro-Wilks test and analyzed with independent samples t tests and non-parametric tests (Mann–Whitney U test, χ2, Fisher’s Exact test). The significance level was set at p < .05. All quantitative analyses used SPSS, version 21.0. Analysis of questions with Likert-scale answers was facilitated by combining and recoding reporting values to create fewer response categories. Response options, such as always and very often or rarely and never, were combined into fitting categories. A specific recoding of reported values was used to dichotomize responses on frequency of services requested, resulting in new categories of rarely or never and often.
Five indices were created from questions on the same topic. The response option don’t know was recoded as “missing.” Cronbach’s alpha assessed the reliability of all potential indices: Guidance and advice to SSEs (12 items, maximum possible score: 48, α = .96), OHS monitoring work ability and health (5 items, maximum possible score: 20, α = .80), SSE goals on health and OHSs (5 items, maximum possible score: 20, α = .93), Monitoring sick leave (11 items, maximum possible score: 44, α = .92), and Evaluation of OHS measures (5 items, maximum possible score: 24, α = .90). The mean and median values for the indices were compared between countries (Kvorning, Hasle, & Christensen, 2015).
All open text answers were analyzed using qualitative content analysis (Graneheim & Lundman, 2004). The answers to the question “Do you have specific industries represented among your customers?” were categorized as “industry, construction, and trades,” “catering and cleaning,” “administration and teaching,” and “health and welfare.” The open text answers about marketing were categorized as “electronic advertisement, web and social networks,” “physical advertisement,” “customer contact,” and “networking events.” The third marketing question (“Do you have a special offer for small companies?”) received only one category of responses: “special deals.” Two questions concerning problems and possible solutions were analyzed into two categories: Challenges for SSEs working with OHSM, and Changes needed.
No data were collected on individual company business strategies, and no sensitive information or company names were discernable from the data. No sensitive information about OHS clients was requested in this survey.
Results
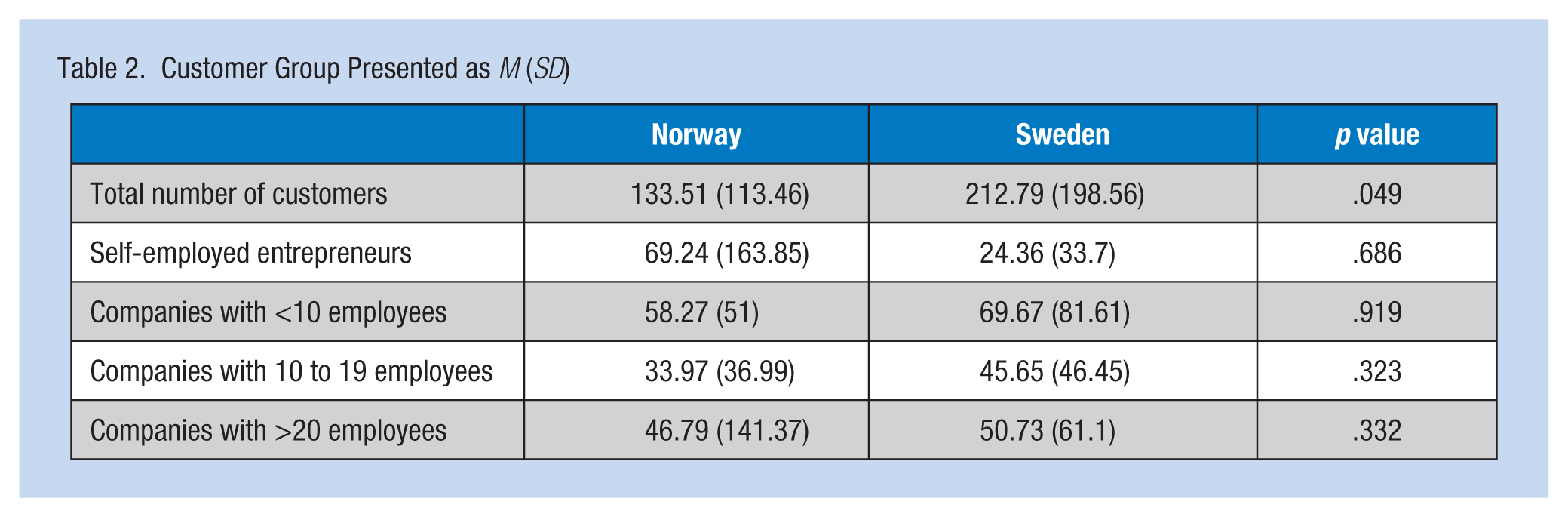
The respondents’ position and organizational structure are presented in Table 1. The respondents were mainly managing directors representing various types of privately organized OHSs. No significant differences between the two countries in terms of the respondents’ position or organizational structure were identified. The number of customers each OHS had at the time of the questionnaire ranged from 0 to 450 (M = 133.5, SD = 113.5) in Norway, and from 1 to 700 in Sweden (M = 212.8, SD = 198.6), which was a significant difference (p = .049). The question on grouping current customers by company size based on number of employees showed that the distribution was similar in both countries (Table 2).
Demographic Data Presented as n and % (Norway n = 87, Sweden n = 51)
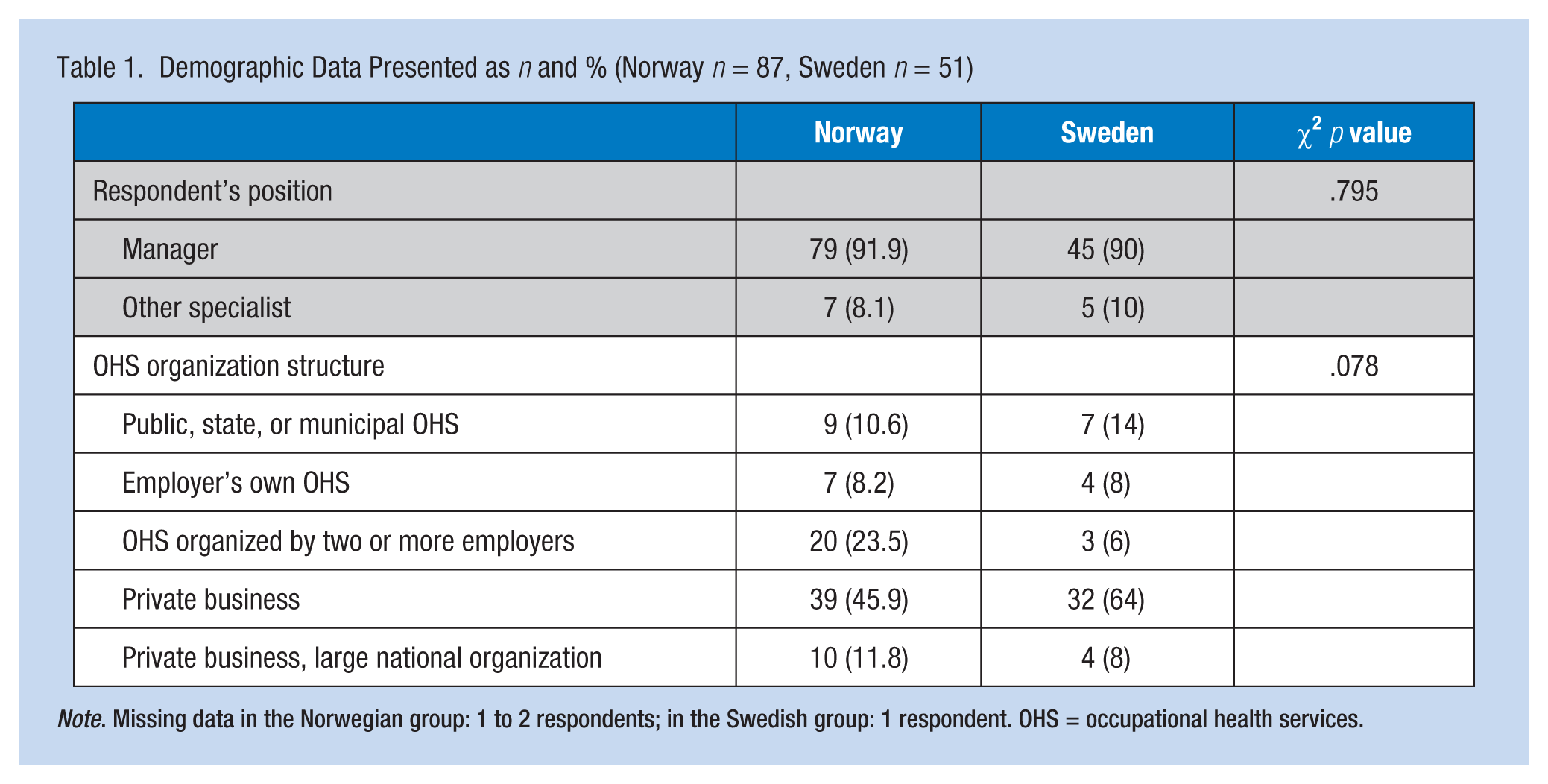
Note. Missing data in the Norwegian group: 1 to 2 respondents; in the Swedish group: 1 respondent. OHS = occupational health services.
Customer Group Presented as M (SD)
The distribution of companies during the previous 12 months had changed somewhat in both countries. In Norway, 56.1% of the respondents answered that companies with less than 10 employees had increased somewhat or greatly during the last 12 months. This group had also increased the most compared with the other customer sizes in Sweden, according to 43.6% of the respondents. The highest proportion of industrial sectors in both countries was within industry, construction, and trades (78.4% and 66.7% for Norway and Sweden, respectively). Many of the Norwegian respondents (43.2%) also had a considerable number of cleaning and restaurant/catering customers represented.
Services Requested
The services most frequently requested in Norway were assistance with occupational health and safety systems, followed by ergonomics and occupational hygiene. These services were all requested significantly more often in Norway than in Sweden. The most requested services in Sweden were individual health examinations and health care services, followed by rehabilitation services. The only two services with similar demand in both countries were education and health and lifestyle advice, which were either never or rarely requested in either country (Table 3). Analyses of the total number of requested services showed that Norwegian OHSs reported more requests for services in total (Median = 4.5) from SSEs than did Swedish OHSs (Median = 3.0).
Frequency of Requests by Small-Scale Enterprises for Services Presented as n and % (Norway n = 87, Sweden n = 51)
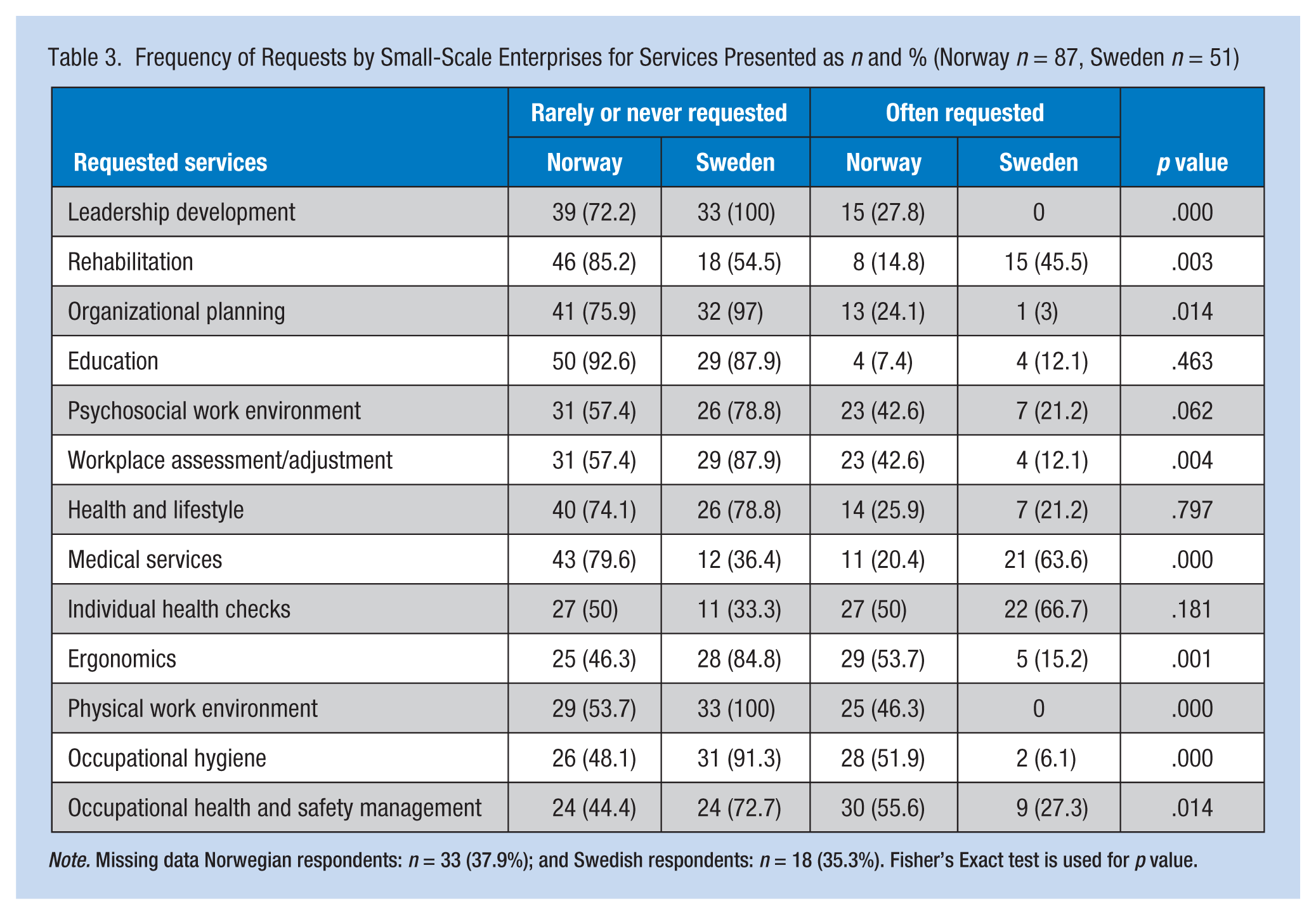
Note. Missing data Norwegian respondents: n = 33 (37.9%); and Swedish respondents: n = 18 (35.3%). Fisher’s Exact test is used for p value.
Cooperation Between OHSs and SSEs
Table 4 shows the results of the five indices. A significant difference was found in the median scores of the index regarding the frequency of Guidance and advice to SSEs (Norway: 39, Sweden: 23). Norway also recorded significantly higher mean scores on the indices SSE goals on health and OHSs (Norway: 13.5, Sweden: 7.3), Monitoring sick leaves (Norway: 32.0, Sweden: 24.8), and Evaluation of OHS measures (Norway: 13.5, Sweden: 8.5). No difference was found in the median scores of the index OHS monitoring work ability and health (Norway: 11.4, Sweden: 11.7).
Results of Indices Analyses of Consultation Between OHS and SSEs Presented as M (SD) and Median
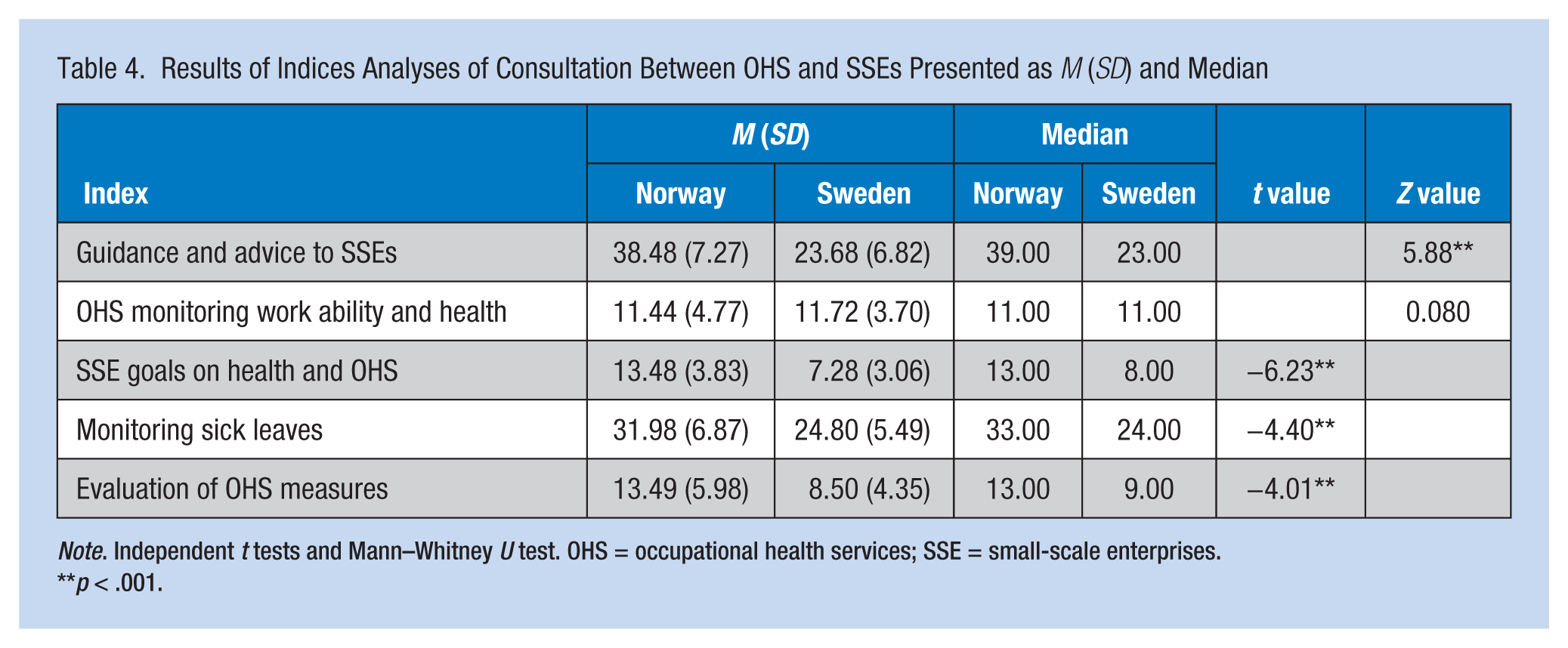
Note. Independent t tests and Mann–Whitney U test. OHS = occupational health services; SSE = small-scale enterprises.
p < .001.
Marketing
The Swedish and Norwegian OHSs were similar in terms of direct marketing to companies of any size. Half of the Norwegian (50.9%, n = 27) and half of the Swedish (54.5%, n = 18) OHSs promoted their services on the open market, with no significant difference between the countries. For those who conducted direct marketing, the preferred channels were digital (e.g., social media, e-mail, and web pages: 17.2% in Norway and 17.6% in Sweden), or direct contact with customers (e.g., meetings with or visits to customers: 18.4% in Norway and 15.7% in Sweden). Both marketing types showed no significant difference between countries. The majority of the OHSs did not specifically direct their marketing toward SSEs (83% in Norway and 75.8% in Sweden). A significantly larger proportion of the Norwegian OHSs had developed special offers for their smallest customers compared with Swedish OHSs (32.1% vs. 6.1%, respectively, p = .006).
Communication and Cooperation
More than half of the Norwegian and Swedish OHSs are rarely contracted by organizations that support the leaders of small enterprises (65.5% and 57.6%, respectively). Cooperation with projects to develop and support SSEs are somewhat more common in Norway than in Sweden, but the majority of OHSs in both countries do not participate in these projects (65.5% and 81.1% in Norway and Sweden, respectively).
Similar frequencies of contact between OHSs and their customers were found in Norway and Sweden. Almost all OHSs reported that they were in contact annually or more often; 96.3% of Norwegians and 95.7% of Swedes were in contact with their entrepreneur customers (no employees) at least once a year, and for SSEs with less than 20 employees, the yearly contact was 100% and 98%, respectively. Both Norwegian and Swedish OHSs estimated that most entrepreneurs and SSEs were satisfied or pleased with their services (Norway: entrepreneurs 97.5%, SSEs 98% were pleased; Sweden: entrepreneurs and SSEs, 100% were pleased).
The Future of OHS in Norway and Sweden
OHSs in both countries reported that to better benefit and include SSEs in the future, customers needed to become more knowledgeable about OHSs (Norway: 72.9%, n = 35; Sweden: 87.5%, n = 24). Swedish OHSs reported that increased official reimbursement from social insurance and tax deductions as well as more cooperation with trade unions would benefit SSEs as consumers of OHSs (all 53.6%, n = 15). The Norwegian OHSs wanted more standardized instructions on how to handle SSEs’ OHS needs and SSE competence in procuring appropriate OHS services (both questions 50%, n = 24).
According to Swedish OHSs, the least important need was cooperation with other OHS units (7.1%, n = 2) and business advisory services (14.3%, n = 4), and increasing OHS skills (14.3%, n = 4). In Norway, the least important need was to develop systems that support SSEs and the self-employed to buy OHS collectively (6.3%, n = 3), OHS cooperation in business development projects (12.5%, n = 6), and reduction of bureaucracy (14.6%, n = 7).
Qualitative Analyses
The open-ended questions, “What is your biggest challenge in working with small-scale enterprises?” and “How could these challenges be solved?” were optional; 21 Norwegian OHSs and 14 Swedish OHSs responded.
Category 1: Challenges for SSEs Working With OHSM
In this category, the OHSs identified the challenges they perceived SSEs had in working with OHSM, including financial conditions and legislation related to SSEs, and involvement and interest from SSEs in occupational health issues.
The analysis showed that in Norway, the problems most frequently addressed concerned financial or legal matters. The client lacked either finances or willingness to spend money on OHSs. For Norwegian OHSs, regulations were hindering OHS access to small customers. Several Swedish OHSs reported that SSEs received lower priority from OHSs because the amount of time or effort spent and the cost per employee were not financially beneficial for the OHSs.
The companies can’t afford to pay for extra services. Very many of the businesses are not “including workplaces” and can’t utilize these support systems. (Norwegian OHS)
In the quote, the idea of including workplaces describes a specific agreement between social partners (e.g., unions, employers, or the government) in Norwegian industry. This agreement reduces absences and the proportion of employees working at less than full capacity in the labor market. Businesses that sign this agreement receive financial incentives for meeting the above-mentioned objectives.
To the respondents, administrative and legal matters that affect OHS for the SSEs appear to be too complicated to receive priority from an unskilled leader.
A lack of competence in HSE of the leaders of small companies. Hence, the leaders think there is too much demands on “paperwork” for HSE and will not place HSE high on the agenda in busy workdays. (Norwegian OHS)
The major concern for Swedish respondents was that they experienced little SSE interest in OHSs. This problem was frequently mentioned by OHSs in Norway as well.
It’s difficult when the customer only comes to us because it is needed in their collective labor agreement. They are rarely interested in our services, they only want a paper to be able to continue their work on e.g. raising a building. (Swedish OHS) They are basically not interested in HSE. And will therefore not have time to work with it. (Norwegian OHS)
An equally substantial number of Norwegian and Swedish responses concerned SSE leaders’ lack of knowledge and skills regarding safe work environments and the role of OHS in establishing and maintaining work environments focused on health and safety.
Category 2: Changes Needed
In this category, the OHSs identified changes needed in legislation and financial support for SSEs and in the priority given to occupational health issues. Norwegian OHSs suggested that legislative changes were necessary to solve identified problems. If a company was not following the law, this should have consequences. More specific and easily available information (e.g., what business leaders/owners should know when starting a company) should be included in the law. Another important solution was developing knowledge and skills for small business owners. However, no one suggested who should be responsible for developing these skills in business leaders.
The Swedes were more careful to address how to implement solutions to identified problems. Financial assistance for SSEs or OHSs to offset the cost of occupational health and safety programs was one suggestion. New or simplified information technology (IT) tools so OHSs could assess customers’ needs quickly and package solutions were also suggested. Better communication with leaders and employee representatives was put forward to improve information flow.
Through different types of IT solutions. Look at banks that let the customer do most of the work, but still get paid for the service. (Swedish OHS)
Discussion
This study investigated OHSs provided to SSEs in Norway and Sweden. The results of this study showed that responding OHS providers reported both self-employed individuals and SSEs were customers and that this customer group had increased in number during the last year in both countries. This finding is positive, considering that earlier investigations showed that many SSEs were not affiliated with OHSs (Josefsson & Kindenberg, 2004). The fact that dominant segments in both countries were within industry, construction, and trades could be explained by specific regulations in these sectors related to work environment legislation (Ministry of Employment, 1977; Ministry of Labour and Social Affairs, 2011).
The first research question in the study was about which services SSEs request from OHSs; clear and significant differences in SSE requests exist between the countries. The same applies to the second research question of whether OHSs have developed specific measures and strategies for consulting with SSEs. Among Norwegian OHSs, the frequency with which information and guidance are provided to SSEs, how the customers’ OHS goals are handled, evaluation of OHS work and practices, and contractual agreements are significantly higher than among Swedish OHSs. In regard to the third research question about differences between Sweden and Norway concerning requests for services, cooperation, and agreements with SSEs, it seems that Norwegian OHSs are more likely to work with organizationally based services than Swedish OHSs. The Swedish OHSs work more with individually based health care services.
Explanations for these results include: The Norwegian accreditation system for OHSs has improved their quality assurance system, competence development, and staffing in occupational health and safety (Lie & Bjørnstad, 2015). The voluntary quality system in Sweden (Gunnarsson et al., 2011) focuses more on business development issues related to ISO 9001 and less on services provided by OHS. Other explanations might be a stronger focus on work organization and collaboration between researchers, employers, and employee organizations in Norway than in Sweden (Lindøe & Hansen, 2000) and the ongoing development of individual responsibility for lifestyle and health in Sweden (Abrahamsson & Johansson, 2013). However, it is noteworthy that measures related to health and lifestyle were requested from SSEs less often than other measures. This finding is in line with research showing that OHSs often work from a pathogenic perspective, instead of using a more holistic approach focusing on promoting health and preventing exposure to workplace hazards (Lydell, Hildingh, Söderbom, & Ziegert, 2015).
Both the Norwegian and Swedish providers reported using specific strategies when consulting with their customers. A majority of the OHS units had not directed their marketing specifically at SSEs, but nearly all providers reported that they had at least annual contact with SSE customers. Efficient collaboration and a close relationship between company managers and OHSs are key factors for improving the work environment (Schmidt et al., 2011). The fact that the majority of OHS units did not participate in SSE development projects and that more than half of them only rarely consulted with organizations that support SSE leaders suggests improvement strategies. Research about the importance of networks has demonstrated forum discussions about health and safety issues can result in change (Kurppa et al., 2006; Palmgren et al., 2015). The above conclusions about cooperative strategies are in contrast to study findings that nearly all providers regarded SSEs as satisfied or pleased with OHS measures. However, a Finnish study showed that only four of five entrepreneurs and only two of three SSEs were satisfied with their OHSs (Palmgren et al., 2015).
Although some differences between countries were identified, all providers reported that SSEs needed to learn more about occupational health services, increase their collaboration with trade unions, standardize handling instructions and solicit government incentives for using OHSs. These strategies are consistent with research showing that SSEs are often unaware of services that OHSs offer and that they, therefore, do not find OHS useful (Antonsson et al., 2002; Bornberger-Dankvardt et al., 2003). It is interesting that only a few OHS providers identified that OHSs also needed to learn more about SSEs. Educational services are rarely requested in either country, but both countries have concluded that general knowledge about OHS among company leaders is poor. The question is whether OHSs have provided sufficient marketing of their services to convince SSEs that occupational health and safety is a necessary investment. It seems unlikely as only half of responding OHSs reported that they conducted direct marketing of services, and only a few directed their marketing toward SSEs. According to the OHSs themselves, SSEs are the ones lacking the skills and knowledge necessary to establish OHS policies and services in their workplaces. In the qualitative analysis, OHSs identified the challenges of working with SSEs, including financial limitations, legislative regulations, and interest in health issues.
In summary, this study demonstrated that SSEs, particularly in industry, construction, and trades, are common customers of Norwegian and Swedish OHS and that the demand for these services has increased in the last 12 months. The results point to significant differences between Norway and Sweden in regard to SSEs’ requests for services and consultations between SSEs and OHSs. Norwegian OHSs work with a more holistic approach to psychosocial and physical work environments, work organization, and leadership; Swedish OHSs work more with services focused on individual injuries and illnesses, individual health examinations, and rehabilitation. To improve OHSs in SSEs, OHS services should be marketed directly to SSEs, and closer collaboration between OHSs, SSEs, and enterprise networks is essential. The analyses also showed a need for financial incentives to increase utilization of OHS among SSEs and more competence among SSE leaders when introducing OHSM in SSEs. This study should be replicated in other countries because occupational health and safety laws and the structure and organization of OHS differ by country, and these differences can influence OHSs, consultations, and agreements with SSEs. More research is also needed about occupational health and safety issues in SSEs throughout the world. Research about occupational health and working conditions in SSEs in several countries have shown limited knowledge and skills on the part of management in regard to how to make improvements. Therefore, OHSs are needed in SSEs.
Limitations
Generalization of the results requires caution as the results are based on self-reported data from providers, which can result in bias when SSEs are not answering questions themselves. Also, the response rate differed between Norwegian and Swedish providers and was in general relatively low (35.4%). However, a strength of the study was the robust inclusion criteria and using official and branch registries to identify participants. Other strengths included the combination of quantitative and qualitative questionnaire data as well as the development and use of survey questions from similar Finnish studies (Palmgren et al., 2015).
Implications for Practice
Small-scale enterprises use OHSs less than larger enterprises and organizations in Norway and Sweden. Therefore, OHSs could develop specific strategies and services for SSE leaders on how to improve working environments and worker health in their enterprises. Preferably, OHSs should arrange networks for SSE leaders and employee representatives to discuss OHSs and health-promotion programs. A closer dialogue between OHSs and SSEs about goals and evaluation processes could also increase SSE motivation to improve working conditions and worker health. Occupational health nurses could contribute to this goal by providing care for employees in SSEs, and promoting health and safety in their workplaces.
Applying Research to Practice
Occupational health services could potentially develop specific strategies and services for small-scale enterprises (SSEs) on how to improve working environments and worker health in their companies. Preferably, occupational health services (OHSs) could arrange networks for SSE leaders and employee representatives to discuss occupational health and safety activities, worker health and lifestyle issues, and health-promotion programs. A closer dialogue between OHSs and SSEs about goals and evaluation processes could also increase SSE motivation to improve working conditions and worker health. Incentives to expand OHSs with adapted services for SSEs is another possible intervention.
Footnotes
Acknowledgements
We would like to acknowledge Aud Ramberg, Friskgården occupational health services (OHS), Norway; and Karin Mäki, Commodia OHS, Sweden, for valuable help and comments prior to data collection.
Conflict of interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The authors want to express their gratitude to AFA Insurance, Sweden, for financing the study (Dnr: 130190).
Author Biographies
Stig Vinberg is a professor at the Department of Health Sciences at Mid Sweden University. His main research interests include workplace health promotion and management, with particular emphasis on small enterprises.
Lisa Torsdatter Markussen is a research assistant at the Department of Health Sciences at Mid Sweden University.
Bodil J. Landstad is a professor at the Department of Health Sciences at Mid Sweden University and research manager at Nord-Trøndelag Hospital Trust in Norway. Her research is focused on health promoting and rehabilitating processes including workers who either are at risk of termination or already marginalized relative to work.