
Abstract
In recent years, safe patient handling in the health care industry has been addressed by various stakeholders, but much work remains to reduce health care worker injuries, and improve safety and care quality for patients. Recently, safe patient handling in ambulatory care settings has gained attention. As health care delivery evolves, demands on ambulatory care will increase and more dependent patients will visit ambulatory care clinics. Typically, ambulatory care clinics are not equipped with appropriate safe patient handling equipment. Examination tables, standard in ambulatory care clinics, currently have fixed height and are not easily accessible. This study investigated the benefits of introducing new height-adjustable examination tables to an ambulatory care setting. The results of this study indicate that by using height-adjustable examination tables, work-related musculoskeletal disorder (WMSD) risk for caregivers can be significantly reduced.
Keywords
It is well documented that caregivers working in health care facilities are at high risk for experiencing work-related musculoskeletal disorders (WMSDs; for example, back injuries and other strains and sprains; Collins, Nelson, & Sublet, 2006; Karahan, Kav, Abbasoglu, & Dogan, 2009; Mohammed et al., 2014; Pompeii, Lipscomb, Schoenfisch, & Dement, 2009; Trinkoff, Lipscomb, Geiger-Brown, & Brady, 2002). Recent data demonstrate that this trend continues. The incident rate for overexertion type injuries among nursing assistants in 2014 was 204.6 per 10,000 full-time workers, more than 5 times greater (35.6) than for all U.S. workers experiencing this type of event or exposure (Bureau of Labor Statistics, 2015). For private industry sectors with more than 100,000 total cases, health care and social assistance had an incident rate of 121.3 cases per 10,000 full-time workers, the highest among sectors reporting. Work-related musculoskeletal disorders accounted for 39% of the total injuries and illnesses reported in the health care industry in 2014 (Bureau of Labor Statistics, 2015).
Because of the high rates of WMSDs suffered by health care workers, interventions (e.g., safe patient handling and mobility programs) have been initiated. These programs include the introduction of new technology integrated into health care equipment and facility furnishings (American Nurses Association, 2013; Owen, Keene, & Olson, 2000). Examples of new technology include mechanical patient lifts, lateral transfer aides, transfer chairs, and integrated bed systems (Nelson et al., 2006).
To date, much of the emphasis on safe patient handling and mobility efforts have been directed at acute care, long-term care, and home care (American Nurses Association, 2013). Little work has been done to evaluate and reduce risks in ambulatory care. Ambulatory care is a large and growing part of the overall health care delivery system and employs many workers. Demands on ambulatory care will continue to increase with additional pressure to reduce health care costs by reducing length of stay. More high-dependency patients, who require assistance with movement and mobility, will be seeking the services of ambulatory care providers. Caregivers who assist ambulatory care patients include physicians, physician assistants, nurse practitioners, registered nurses, licensed practical nurses, nursing assistants, physical therapists, occupational therapists, and other technicians.
Considering patient handling activities required in ambulatory care, assisting patients on and off examination tables is a frequent task, which presents risks similar to those encountered when transferring patients between bed and chair, a difficult and high risk caregiver activity (Nelson et al., 2003).
Defining the Problem
Examination tables typically found in ambulatory care have fixed height and actually are referred to as box-type tables. The normal height of these standard box-type examination tables is about 32 inches. To understand the difficulty presented by fixed-height examination tables, compare this height of 32 inches with the height of a common chair seat, which is approximately 18 inches. Figure 1 illustrates the problems encountered when patients attempt to climb on and off a fixed-height table; when in a normal seated posture, patients’ feet are well above the floor surface. This situation can be improved with a height-adjustable surface because patients can comfortably place their feet flat on the floor when transferring to the examination table. Presented with a 32-inch high fixed surface, wheelchair users and others with activity limitations must be lifted or assisted onto the table, risking a WMSD for the assisting health care worker. Figure 2 further illustrates the height differential between a fixed-height examination table and an adjustable-height table placed in a low accessible position.

Difference in foot position in relation to floor comparing fixed-height and height-adjustable examination table.

Illustrating height difference between fixed-height and adjustable-height examination tables when compared with standard seating height.
In addition to the risk of heavy lifting, further occupational risk is presented to caregivers if bending and twisting are required to examine patients positioned at a fixed height. When patients are examined on equipment with an adjustable-height feature, health care providers can elevate the equipment to a comfortable height and maintain a natural posture for the examination or procedure, eliminating static and awkward postures and further decreasing the risk of back strain or WMSDs for these health care professionals (Macdonald, 2010). Figure 3 shows a patient on an adjustable-height table, providing easy access for the caregiver.

Patient on height-adjustable table that can be raised and lowered for caregiver ease of access during examination or procedure.
Administrators, chosen to respond to a survey, were asked if they skipped parts of an examination when barriers to examining patients with disabilities were encountered (Lagu et al., 2013). Forty-four percent of the administrators acknowledged that parts of an examination were skipped when barriers were encountered. Practice administrators were asked about accommodations if patients were not able to transfer to an examination table. Seventy-six percent of practice administrators indicated that patients were examined in their wheelchairs when they could not transfer to an examination table. Over 52% of practice administrators reported asking patients to bring someone with them to help with the transfer. Seventy-seven percent of practice administrators indicated that their employees were trained to lift a patient but only 4.8% of practices had a mechanical lift available to transfer patients (Lagu et al., 2013).
When a physician or other health care professional is unable to complete an appropriate examination because a patient cannot transfer to an examination or procedural table or chair, the patient may not receive all aspects of needed care. The patient could be misdiagnosed, because the health care professional may not have sufficient information. Alternatively, the patient might miss the benefit of early detection of a serious developing condition. By providing accessible examination tables, the quality of care provided to individuals with disabilities and activity limitations can be improved. In addition, the use of an accessible examination table may also reduce the frequency of using and time required for a lift team, lift equipment, or transfer assistance from staff (Macdonald, 2010).
Although height-adjustable examination tables make sense, they are currently lacking in the majority of health care facilities. In a California survey, researchers found that only 8.4% of provider sites had a height-adjustable examination table (Pharr, 2014).
Research Hypothesis
When a caregiver is required to assist a dependent patient, whether in a wheelchair or from a standing position, to a fixed-height examination table, the caregiver is at risk for a WMSD. If modifications are introduced to the design of examination tables, such as the ability to move the table up and down with automatic adjustable-height controls, the process of assisting a dependent patient to the examination table is substantially less risky for the health care worker. To investigate the occupational risk reduction that might be achieved with the introduction of height-adjustable examination tables, a study was undertaken.
The purpose of this study was to consider the risks caregivers encounter when they are required to assist dependent patients to fixed-height examination tables and then determine if and how risk might be reduced if a height-adjustable examination table was an alternative. The research question posed hypothesized that height-adjustable examination tables can facilitate the process of assisting patients of various dependency levels to examination tables and, as a result, occupational risk to caregivers will be reduced. In other words, less perceived physical exertion will be reported when a caregiver assists a patient who has mobility limitations and requires assistance to a height-adjustable examination table versus a standard fixed-height examination table.
Data Collection Instrument
Measuring perceived physical exertion is an effective technique when investigating relative risk of patient handling activities (Fragala & Fragala, 2014; Owen & Fragala, 1999; Owen, Garg, & Jensen, 1992; Winkelmolen, Landeweerd, & Drost, 1994). The validated Borg Scale for Perceived Exertion was used to evaluate caregiver subjective physical exertion required to complete the task of helping a patient to an examination table. This instrument uses a 10-point scale, ranging from 0 (no exertion) to 10 (extremely hard exertion; Borg, 1978, 1982). Reliability and validity of the Borg scale have been previously published (Borg, 1978, 1982). In addition, subjective ratings were deemed appropriate for this study for several reasons. First, prior research found no significant differences in findings using the Borg scale for perceived exertion and the more complicated, time-consuming, and labor-intensive biomechanical model methods (Owen & Fragala, 1999; Owen et al., 1992; Winkelmolen et al., 1994). Second, biomechanical models are rarely feasible in actual clinical settings where the primary objective of the setting is to provide care to patients (Fragala & Fragala, 2014). Finally, because a major objective of improving ambulatory care is to protect caregivers from overexertion, their personal perception of exertion may provide more useful data than objective assessments. The Borg Scale for Perceived Exertion is also frequently used by ergonomists and has been widely accepted in the ergonomics field (Dawes et al., 2005).
Method
Experienced caregivers performed two different tasks for assisting a 235-pound volunteer, who acted as a patient, to an examination table. The total number of recorded trials was 32 and each task was performed by an individual caregiver.
The volunteer patient exhibited limited mobility and, although ambulatory, had difficulty mounting a step and compromised upper body strength. Task 1 involved a traditional fixed-height examination table, with a surface height of 33.38 inches, commonly found today in many ambulatory clinics. To assist the patient mount the table, an intermediate step was provided at the foot end of the table. Task 2 employed a height-adjustable examination table with a lowest seat height of 18 inches. Immediately after conducting each task, caregivers completed written data collection sheets on which they indicated their perceived physical exertion for each body part considered.
Caregivers were instructed to assess patients’ limitations; if they felt it was unsafe or beyond their capabilities to assist the patients to the examination table, they were not required to complete the task. When caregivers determined the task was beyond their capabilities and did not complete the task of assisting the volunteer patient to the examination table, the maximum score of 10 was recorded for that trial. In eight of the 32 trials, the caregiver determined the task to be unsafe because the exertion required was extremely hard.
Data Analysis
Differences in caregiver mean perceived exertion between the tasks of assisting the patient to the examination table were evaluated using paired samples t tests for each body part (i.e., shoulder, upper back, lower back, and whole body). Analyses used Excel 2010 statistical data analysis tools including the t test paired for two sample means. Data are presented as mean plus standard deviation and percent of reduction in perceived physical exertion when the task was completed with the height-adjustable examination table.
Results
Comparing mean relative perceived exertion reported by caregivers when assisting patients to fixed-height examination tables versus height-adjustable examination tables yielded the following results:
Perceived shoulder exertion differed significantly (t = 10.30, p < .05) between assisting patients to the fixed-height examination table (5.29 ± 2.98) versus the adjustable-height examination table (.28 ± .49). The mean perceived exertion was reduced by a factor of 95% with the height-adjustable examination table.
Perceived upper back exertion differed significantly (t = 8.59, p < .05) between assisting patients to the fixed-height examination table (5.23 ± 3.39) versus the adjustable-height examination table (.13 ± .28). The mean perceived exertion was reduced by a factor of 98% with the height-adjustable examination table.
Perceived lower back exertion differed significantly (t = 10.41, p < .05) between assisting patients to the fixed-height examination table (5.73 ± 2.98) versus the adjustable-height examination table (.20 ± .46). The mean perceived exertion was reduced by a factor of 97% with the height-adjustable examination table.
Perceived whole body exertion differed significantly (t = 11.95, p < .05) between assisting patients to the fixed-height examination table (6.00 ± 2.77) versus the adjustable-height examination table (.19 ± .35). The mean perceived exertion was reduced by a factor of 97% with the height-adjustable examination table.
Results of paired sample statistics are presented in Table 1, which compares the mean of the relative perceived physical exertion reported for the 32 trials by body areas considered. These results are further displayed in Figure 4, which provides a display of reported means comparisons. When the task was completed with the height-adjustable table, note the 95% to 98% reduction in mean perceived physical exertion for all body parts and the whole body.
Comparison of Perceived Exertion (M ± SD) for Assisting Patient Onto Examination Table (n = 32)
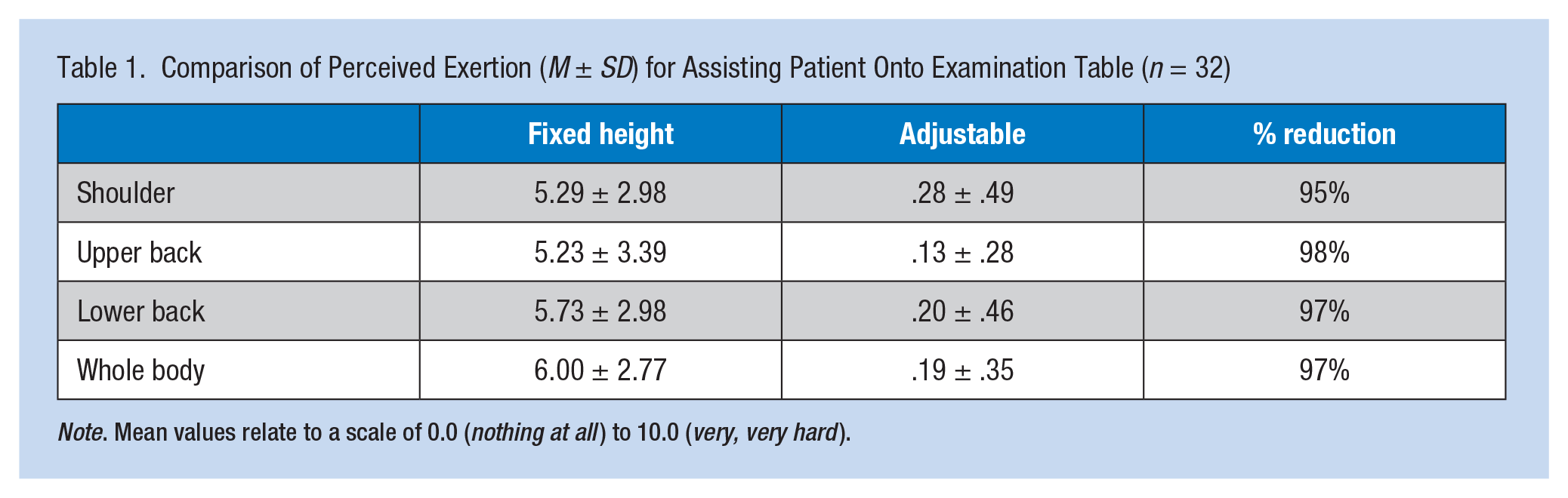
Note. Mean values relate to a scale of 0.0 (nothing at all ) to 10.0 (very, very hard ).
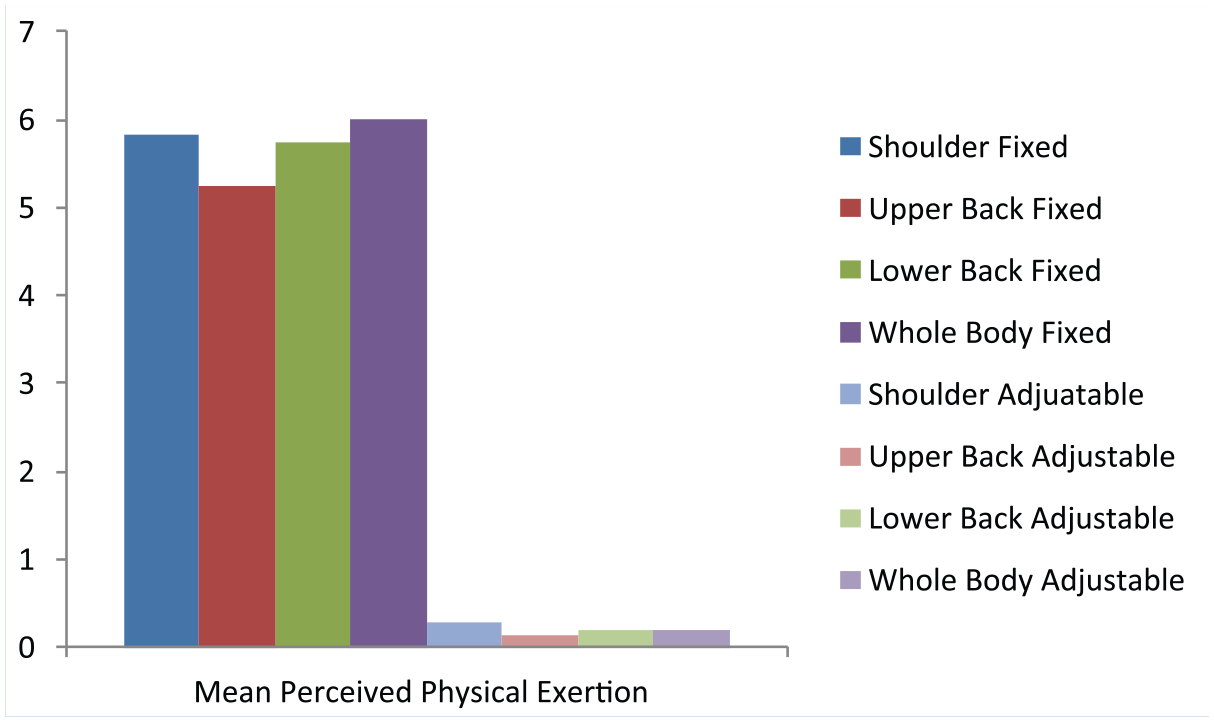
Comparison of mean perceived physical exertion.
In addition to the reduction in perceived physical exertion, application of height-adjustable examination tables could reduce actual risk based on ergonomic task assessment. A fixed-height examination table could require a lift or transfer from a low seat height to a much higher seat height. Using the National Institute of Occupational Safety and Health (NIOSH)-lifting formula to determine what might be a safe load for health care workers to lift, the recommended limit is 35 pounds for patient handling tasks. When the load exceeds 35 pounds, it is recommended that safe patient handling technology be employed (Waters, 2007). By using height-adjustable examination tables, the need to lift or transfer patients to a much higher seat height is eliminated thus creating a safer task from an ergonomics perspective.
Considerations for Further Research and Study Limitation
This preliminary study used a convenience sample with a relatively small number of trials. However, the number of trials was adequate to demonstrate a statistically significant difference in relative perceived physical exertion between the two tasks of assisting patients to an examination table. Although the methodology employed in this study, using relative perceived physical exertion as an indicator of occupational risk, has been shown to be valid and appropriate, other methods for evaluating risk might be considered for additional laboratory studies. For example, biomechanical modeling methods could be applied to compare forces on musculoskeletal structures while caregivers are assisting patients to an examination table. Comparing force differences generated by various tasks on musculoskeletal structures could provide additional information for determining occupational risk for injury.
Laboratory studies provide accurate information when considering relative risk of injury. However, these studies do not demonstrate whether an implemented solution actually results in fewer injuries for ambulatory caregivers. A logical next step is to evaluate the effectiveness of height-adjustable examination tables in reducing caregiver injuries via a clinical study. This clinical study could evaluate the impact of height-adjustable examination tables on occupational injury rates using a pre-/post-intervention design.
Beyond potential caregiver risk reduction, a height-adjustable examination table can have many benefits for the patient. Whether transferring from a wheelchair or assisting an ambulatory patient, a height-adjustable examination table is designed to make positioning patients on examination tables easier, more efficient, and safer for staff and patients. With an 18- to 37-inch adjustable range, the height-adjustable examination table also creates a less stressful, more controlled experience for the patient and ensures that patients’ dignity is maintained. These benefits contribute to quality of care and could be investigated in future clinical research studies using an instrument similar to the exertion scale rating tool used in this study.
As new safe patient handling and mobility solutions are developed, laboratory studies can measure risk reduction and patient benefits for specific devices or technology. Information from laboratory and clinical studies should guide the selection of equipment for clinical settings. As the value of new safe patient handling technology becomes recognized and more common in health care facilities, further research can demonstrate the effectiveness of these solutions in reducing occupational injuries and their impact on quality of care. This study and future research will support the value of and need for safe patient handling and mobility technology.
Conclusion
Results from this pilot study indicate that height-adjustable examination tables can reduce the occupational risk of assisting patients to an examination table and the process can be easier for both patients and caregivers. Caregivers reported that significantly lower perceived physical exertion was required to perform the task with a height-adjustable examination table. Greater caregiver physical exertion equates to greater stress on musculoskeletal structures and increased risk for injury (Fragala & Fragala, 2014; Owen & Fragala, 1999; Owen et al., 1992; Winkelmolen et al., 1994). This reduction in perceived physical exertion may translate to less force exerted on the musculoskeletal structure and a lower risk of injury to the caregiver.
As a result of assisting patients to an examination table, caregivers may be more likely to comply with protocols for examinations in ambulatory care settings. Compliance may translate to improved quality of care and better health care experiences for patients. This study demonstrates how examination table technology, using the concepts of ergonomics, can improve the environment of care in ambulatory care settings resulting in better outcomes for both patients and caregivers.
Applying Research to Practice
Ambulatory care is a rapidly growing segment of the overall healthcare delivery system. With increasing demands to reduce in-patient days, volume of ambulatory care visits will grow and the patient population to be seen will be more dependent. In addition to an aging population, older people with mobility limitations will be seeking care in these ambulatory care clinics. This research provides scientific evidence to those responsible for designing, building, and renovating the ambulatory care setting to benefit both patients, and caregivers. Through this research, the value of height, adjustable examination tables has been demonstrated when a significant risk reduction is achieved for the caregiver. In addition, the research suggests benefits for the patient and provides ideas and a path for future research to investigate these patient benefits.
Footnotes
Conflict of Interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The author wishes to thank and acknowledge Midmark for providing financial support for the research.
Author Biography
Dr. Fragala has 40 years of professional experience and is an international expert in the application of ergonomics to healthcare. He has been on the faculty at major universities, consulted to leading industries and government agencies, and has over 100 publications related to safe patient handling. His book entitled, Ergonomics: How to Contain On-the-Job Injuries in Healthcare, has influenced much of the work today related to healthcare ergonomics and safe patient handling programs. In recognition for his work and contributions, he was recently presented with the National Advocacy Award for Improved Caregiver Safety.