
Abstract
Cardiac events are strongly associated with line of duty deaths among firefighters. Among a convenience sample (N = 14) of volunteer firefighters, a questionnaire assessed their knowledge of cardiovascular disease before and after cardiovascular health training using evidence-based guidelines. The questionnaire explored their pattern of physical activity, awareness of their lipid levels, body mass index, as well as signs and symptoms of cardiovascular disease. Thereafter, an educational health program was conducted. Firefighters demonstrated an increase in knowledge post training, in that they were able to identify cardiovascular risk factors and personal determinants of cardiovascular disease. Occupational health providers are encouraged to educate firefighters about the seriousness of cardiovascular disease, and to implement measures to promote better lifestyle behaviors.
Keywords
Background and Significance
Cardiac events are strongly associated with line of duty deaths among firefighters, accounting for the highest occupational cardiovascular disease proportionate mortality of any occupational group (Banes, 2014; Smith, 2011). Construction workers, emergency medical workers, and police officers also engage in intense physical labor that might be preceded by periods of relative inactivity, yet the percentage of fatal cardiovascular event in these occupations is 13%, 11%, and 22% respectively (Banes, 2014; Poston et al., 2011). In 2012, the U.S. Fire Administration reported that of the 82 firefighters who died in the line of duty, 45% to 60% died of a cardiovascular event (Banes, 2014; Durand et al., 2011; Soteriades, Smith, Tsismenakis, Baur, & Kales, 2011; Yoo & Franke, 2009).
The literature strongly supports that most line of duty cardiovascular event fatalities are precipitated by work and occur in firefighters with underlying cardiovascular disease. The underlying factors include nonmodifiable risk factors such as age, gender, and familial disease history, as well as modifiable cardiovascular disease risk factors such as diabetes mellitus, high blood pressure, high blood cholesterol, high triglycerides, and obesity (Banes, 2014; Byczek, Walton, Conrad, Reichelt, & Samo, 2004; Drew-Nord, Hong, & Froelicher, 2009). Behavioral health issues, such as tobacco and alcohol use, are also associated with cardiac disease and sudden cardiac death (Yang et al., 2013). All of these health risks, in combination with handling heavy apparatus and wearing personal protective equipment weighing as much as 44 to 50 pounds, can predispose firefighters to sudden cardiac death (Banes, 2014; Farioli et al., 2014).
There has been an effort to decrease cardiovascular disease prevalence among firefighters through implementation of a nationwide program focusing on early detection and prevention, which has been deemed beneficial (Geibe et al., 2008). However, firefighters continue to be at high risk. A study by Banes (2014) examined firefighters’ cardiovascular risk behavior by conducting a 12-week low glycemic nutritional fitness program using the PHLAME (Promoting Healthy Lifestyles Alternative Models’ Effects) tool to provide both team-based and individual counseling for groups of firefighters. The PHLAME study demonstrated the positive effects of education, team, and individual interventions on body mass index (BMI), nutrition, behavior, and physical activity (Banes, 2014).
The purpose of this study was to assess volunteer firefighters’ knowledge of the risk factors associated with cardiovascular disease.
Method
Study Population
Participants included volunteer firefighters from two fire departments located in Nassau County, New York. They were contracted to receive occupational health services from Northwell Health, Occupational and Environmental Medicine of Long Island. After obtaining permission from both fire chiefs, a recruitment poster was used to inform potential participants of the study. Participation in the study was voluntary. All procedures and consent forms complied with requirements set forth by the Institutional Review Boards of Stony Brook University and Northwell Health.
Procedures
In December 2015, volunteer firefighters were invited to participate during routine annual screenings in office at Occupational and Environmental Medicine of Long Island, and on-site at two fire departments. A physical examination, including the collection of height, weight, blood pressure, cholesterol levels, and blood glucose levels, was performed. In addition, electrocardiogram was performed, and firefighters were asked to complete a self-reported 49-item questionnaire adapted by Yoo and Franke (2009) to assess their knowledge of cardiovascular disease risks. The primary investigator then asked firefighters to individually read an educational PowerPoint presentation. Finally, firefighters were asked to complete a post-survey 4 weeks later and return it by mail.
Educational Intervention
The educational intervention was a 30-minute PowerPoint presentation, which described the incidence and prevalence of cardiovascular disease in volunteer firefighters and provided epidemiological details of cardiac fatalities. The PowerPoint presentation defined the major types of heart disease, described warning signs of heart attack, and factors that contribute to their development. The educational intervention discussed nonmodifiable risk factors (age, gender, familial history), modifiable risk factors (diabetes, high blood pressure, high cholesterol, high triglycerides, overweight and obesity), and behavioral health issues (physical inactivity, tobacco and alcohol use). In addition, the educational intervention explained the importance of lifestyle modification aimed at prevention and management of cardiovascular diseases, including modifying dietary habits, as well as controlling diabetes, blood sugar, and lipids and cholesterol. It also discussed the importance of maintaining regular medical check-up, complying with medications and treatment regimens, maintaining healthy weight, exercising regularly, smoking cessation, limiting alcohol consumption, and managing stress.
Measures
The questionnaire was used to assess the prevalence of self-reported cardiovascular disease, cardiovascular signs and symptoms, and cardiovascular risk factors. The 49-item questionnaire is a combination of three instruments, (a) World Health Organization Cardiovascular Disease Risk Management Package, (b) The American Heart Association’s Risk Assessment Tool, and (c) Behavioral Risk Factor Surveillance System. Cardiovascular disease signs and symptoms were assessed using questions adapted from those used in the World Health Organization Cardiovascular Disease Risk Management Package. The American Heart Association’s Risk Assessment Tool formed the basis for the assessment of cardiovascular disease risk factors, including questions regarding self-reported height and weight, fasting glucose, systolic and diastolic blood pressures, total cholesterol, low-density lipoprotein (LDL) cholesterol, high-density lipoprotein (HDL) cholesterol, and triglyceride levels. Questions assessing the presence of cardiovascular disease, and when blood pressure and blood lipids had last been assessed, were adapted from those used in the Behavioral Risk Factor Surveillance System questionnaire (Yoo & Franke, 2009).
Knowledge Scored
A construct was created from firefighters’ responses to the questionnaire; this was used to measure their awareness, or knowledge, of their cardiovascular disease risk factor values. Knowledge was a count variable, calculated by counting whether participants were aware of the following eight dichotomous values: fasting blood sugar, waist size, systolic blood pressure, diastolic blood pressure, total cholesterol, HDL, LDL, and triglycerides. Thus, knowledge scores could range from 0 (minimum, no values known) to 8 (maximum, all values known).
BMI
Standard BMI was calculated by using firefighter’s height and weight values. A BMI ≥25.0 kg/m² was used as the criterion for overweight. A BMI ≥30.0 kg/m² was used to classify a firefighter as obese.
Data Analysis
IBM SPSS Statistical Standard GradPack Version 23 for Windows (2015) was used to analyze the data. Descriptive statistics were used to assess participants’ self-reported background information, medical history, and recent health information. A Wilcoxon test was used to test whether firefighters’ knowledge of cardiovascular disease risk factors differed before and after the health educational program.
Results
Background Information
The majority of the sample was male (92.9%). The mean age of the sample was 43.4 (SD = 16.6 years). Over half of the participants (57.1%) had 6 years or more of firefighting experience. The majority (78.6%) were interior firefighters. The majority (78.6%) of participants reported smoking less than 100 cigarettes over the course of their lives. More than half of respondents (57.1%) never tried other tobacco products. Only one participant (7.1%) reported a history of carotid artery disease. Similarly, only one (7.1%) reported a history of a cardiac procedure. Two participants (14.3%) reported a history of chest pain. In addition, one participant (7.1%) reported a history of diabetes. None of the participants had experienced a heart attack, stroke, transient ischemic attack, peripheral artery disease, or family history of congestive heart disease.
Self-Reported Recent Health Checks
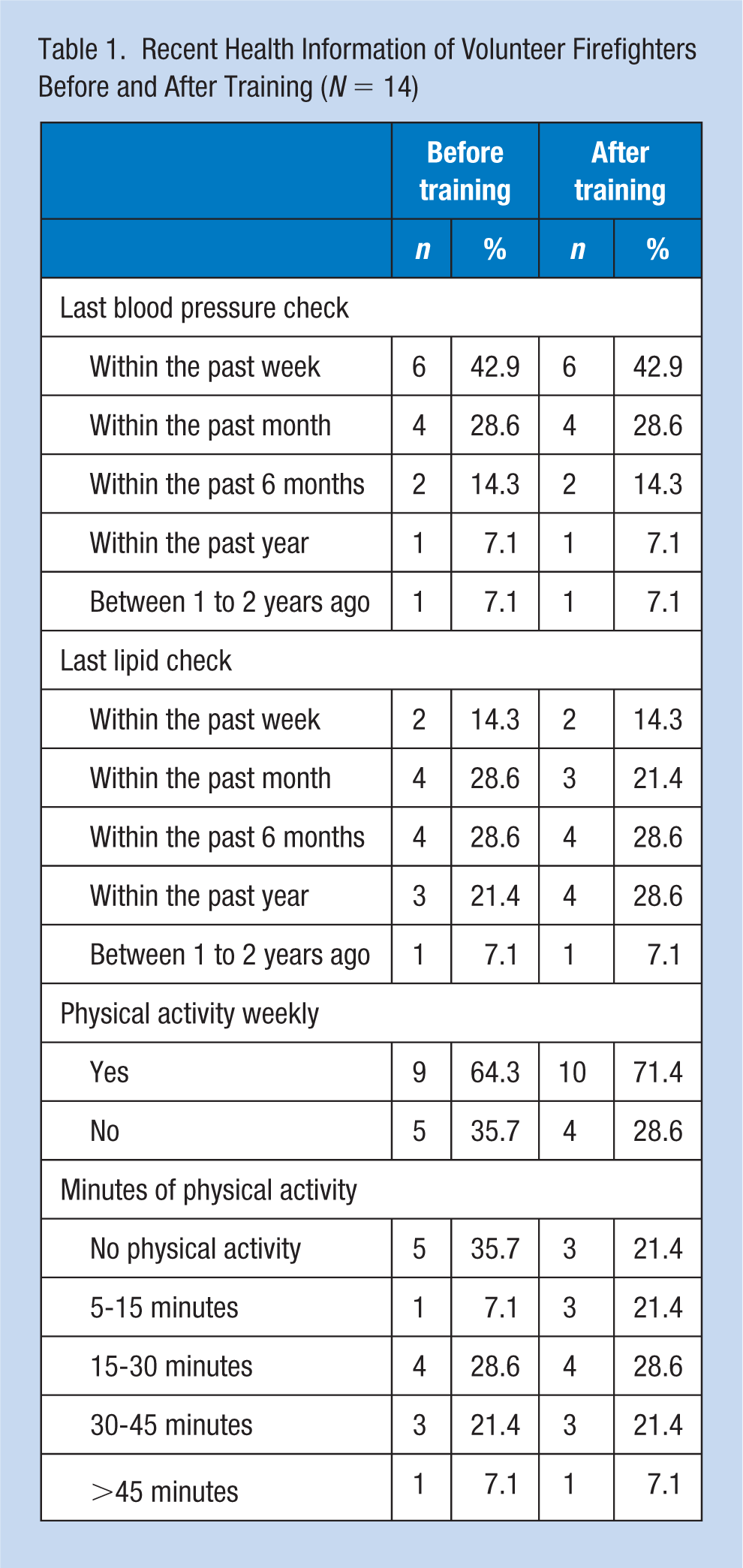
Volunteer firefighters’ (N = 14) self-reported recent health checks are presented in Table 1. The majority (pre-survey and post-survey: 71.4%) of participants reported having a blood pressure check either in the last week (pre-survey and post-survey: 42.9%) or in the last month (pre-survey and post-survey: 28.6%). The majority of the sample (pre-survey: 71.4%; post-survey: 64.3%) of participants reported having a lipid check either in the past week (pre-survey and post-survey: 14.3%), in the last month (pre-survey: 28.6%; post-survey: 21.4%), or in the past 6 months (pre-survey and post-survey: 28.6%). Most respondents reported participating in physical activity weekly (pre-survey: 64.3%; post-survey: 71.4%). Around half of the sample (pre-survey and post-survey: 50.0%) reported participating in physical activity between 15 to 45 minutes.
Recent Health Information of Volunteer Firefighters Before and After Training (N = 14)
Knowledge of Cardiovascular Disease Risk Factors
A small number of participants reported being aware of their fasting blood sugar (pre-survey: 7.1%; post-survey: 14.3%). No participants reported knowing if their waist size was greater than 40″ (for men) or 35″ (for women) in the pre- and post-surveys. In the pre-survey sample, only 57.1% of the participants knew their blood pressure compared with 71.4% of the post-survey sample. Body mass index, knowledge, blood pressure, and cholesterol before and after training among the study population are presented in Table 2. No participants knew their total cholesterol in the pre-survey sample, compared to 21.4% in the post-survey sample. None of the participants in the pre-survey sample knew their HDL, LDL, and triglyceride values, compared with 28.6% in the post-survey sample.
Volunteer Firefighter Body Mass Index (BMI), Knowledge, Blood Pressure (BP), and Cholesterol Before and After Training (N = 14)
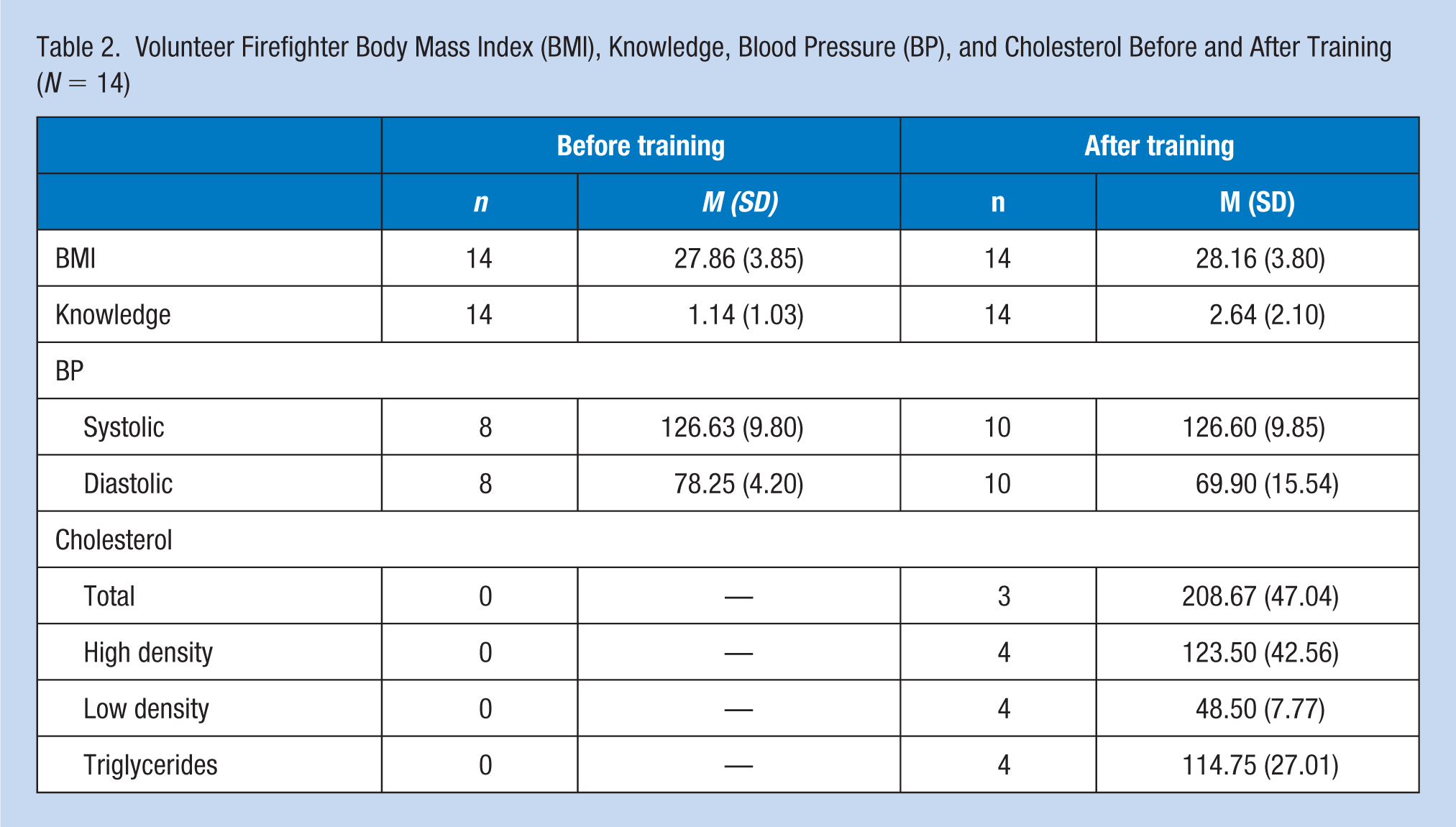
In the pre-survey and post-survey, mean systolic blood pressure was 126.63 (SD = 9.80) and 126.60 (SD = 9.85), respectively. Mean diastolic blood pressure was 78.25 (SD = 4.20) and 69.90 (SD = 15.54), respectively. Mean total cholesterol was 208.67 (SD = 47.04), post-intervention. Mean HDL, LDL, and triglycerides in the post-survey sample were 123.50 (SD = 42.56), 48.50 (SD = 7.77), and 114.75 (SD = 27.01), respectively. In addition, mean BMI in the pre-survey was 27.86 kg/m² and post-survey 28.16 kg/m².
Before the training, participants’ knowledge ranged from 0 to 4 with a mean of 1.14 (SD = 1.03) and median of 2. After the training, participants’ knowledge ranged from 0 to 6 with a mean of 2.64 (SD = 2.10) and median of 2. Thus, the range of knowledge was more restricted prior to the training. The results of the Wilcoxon test revealed that the educational program elicited a statistically significant change in knowledge (Z = −2.39, p = .017). Although the median (midpoint) knowledge score was 2.0 both pre- and post-education, seven participants had higher knowledge after the education. The other seven participants displayed no change in their knowledge.
Discussion
The purpose of this study was to assess volunteer firefighter’s knowledge of cardiovascular disease risk factors. Studies have shown that volunteer firefighters’ fatalities due to heart attack are predisposed to cardiovascular disease. An important finding of the study is that volunteer firefighters’ knowledge of cardiovascular disease appears to be low despite elevated cardiovascular disease risks. The majority of the firefighters did not know their fasting blood sugar, total cholesterol, triglyceride, HDL and LDL. In addition, most participants were unaware of their waist size. The mean BMI reflected a prevalence of obesity. A minority of firefighters engaged in the minimum recommended physical activity. On the contrary, the majority of the firefighters were aware of their blood pressure. The results reinforce that volunteer firefighters seem to be at increased risk of cardiovascular disease. Moreover, the results suggest that a brief, simple educational intervention can increase firefighter awareness of these risk factors in the short-term.
Limitations
A primary limitation of this study is the use of self-reported data, which may yield biased results. Self-reporting tends to underrepresent the true values; consequently, findings may underestimate cardiovascular disease risk factor (Yoo & Franke, 2009). Future studies could benefit from collecting verified data from patient medical records. Convenience sampling is also a limitation that may bias the results of the study due to how participants are selected. The use of random sampling in future studies could reduce this potential bias. Moreover, the low response rate to the post-survey is another restriction, which according to Eastlake, Knipper, He, Alexander, and Davis (2015) are likely not representative of the region. This contributed to a small sample size, which was also a limitation. Therefore, results may not generalize to firefighters both locally and regionally.
Implications for Occupational Health Nursing Practice
Cardiovascular disease and sudden cardiac death in volunteer firefighters remain an important public health problem. Although the response rate was low, respondents completing the heath training gained knowledge. The results are indicative that firefighters would benefit from continued education, and future firefighter-related intervention research led by occupational health nurses. Occupational health nurses can take a leadership role by encouraging firefighters to make healthy decisions, such as engaging in health-promoting activities, increasing physical activity, maintaining ideal body weight, eating healthy, smoking cessation, and reducing alcohol consumption. This study intervention was effective and feasible when conducted during routine annual screenings. Occupational health nurses can collaborate with other members of interdisciplinary teams in developing and implementing firefighter health and fitness-related policies (Byczek et al., 2004). Utilizing health surveillance strategies in collaboration with other professionals and working closely with members of the community, for example, may help change firefighters’ behavior and general health. Research indicates that involvement in voluntary work and the implementation of protective and preventive health measures may have positive impacts on one’s overall health and well-being (Kemppainen, Tossavainen, Turunen, & Franke, 2012). Future research conducted by occupational health nurses should examine the influence of broader community and policy factors on workplace fitness programs and wellness practices, as well as fire department dynamics and organizational behavior (Staley, Weiner, & Linnan, 2011).
Footnotes
Acknowledgements
The authors hereby convey sincere gratitude to the DNP faculty at Stony Brook University School of Nursing, the team at Northwell Health Occupational and Environmental Medicine of Long Island, and Dr. Warren D. Franke.
Conflict of Interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Author Biographies
Althea S. Palmer, DNP, FNP, RN, is a board-certified family nurse practitioner at Northwell Health, Long Island Jewish, New York, and an adjunct faculty in the Barbara H. Hagan School of Nursing, Molloy College, New York.
Jessica L. Yoos, MA, is a statistician at the University of Pennsylvania.