
Abstract
Most working women do not meet current guidelines for physical activity (PA). A 12-week pilot study tested a workplace, peer modeling PA intervention. Inactive female employees from a health system were randomized to an attention control group (ACG; n = 26) or an intervention group (IG; n = 26). The ACG received health information. The IG participated in six group sessions with an active peer model and received an exercise prescription and PA information. Pre and post measures were PA (ActiGraph), Estimated VO2max (cycle ergometer), resting heart rate (HR), glucose and lipids, and cardiovascular risk. Using hierarchical linear modeling, no significant group by time effects were found. Although PA increased in both groups, F(df = 1) = 11.4, p = .002, the IG had greater improvements in fitness (VO2max, HR) and cardiovascular risk (total cholesterol, triglyceride, low density lipoprotein [LDL], calculated risk score) compared with ACG. Results support repeating this intervention in a fully powered study.
Less than 26% of working women in the United States meet current guidelines for at least 150 minutes of moderate aerobic physical activity (PA) and 2 days of muscle strengthening activities per week (Blackwell & Clarke, 2016). Most Americans (82%) do some, or all their work, at their workplaces (American Time Use Survey, 2017). Thus, leading health organizations identify the workplace as an opportune setting for health behavior interventions (Fonarow et al., 2015). Development of “health-based social networks” within workplaces is one recommended strategy to increase PA behavior among U.S. workers (Barbeau et al., 2012).
Workplace interventions targeting PA behavior and cardiorespiratory fitness (e.g., supervised exercise/training, email prompts to take the stairs, and brief stage of change counseling) have been effective (Rowland & Yates, 2017). In a few studies, peers deliver parts of multi-component interventions by providing education, or organizing and leading group PA activities. Outside the workplace, PA interventions that engage peers for social support (i.e., tangible aid, information, and emotional support) have been effective among children, older adults, and adults with cardiac diseases (Ginis, Nigg, & Smith, 2013). No workplace PA studies were found using peer modeling as a central theoretical strategy. Within the workplace, the unique effect of peers to increase PA remains unclear. Research priorities for The National Institute for Occupational Safety and Health (NIOSH; 2016) Total Worker Health® call for description of the theory(s) supporting interventions to increase understanding of why and how the intervention works. Theoretical understanding of the “peer effect” within the workplace is identified as a gap in the literature.
Most workplace PA intervention studies use the transtheoretical model to support the intervention (Rowland & Yates, 2017). The transtheoretical model explains health behavior change as a process marked by stages of readiness for change: precontemplation, contemplation, preparation, action, maintenance, and termination (Prochaska & Velicer, 1997). Another effective and recommended strategy for health behavior change interventions is self-efficacy development (Artinian et al., 2010). Self-efficacy, a central concept of social cognitive theory, can be developed through prior success, verbal persuasion, physiologic feedback, and vicarious experience (Bandura, 1998). Self-efficacy (confidence in ability) can be increased through observing someone similar succeed or fail at a given task or behavior. This observational learning, also known as vicarious experience, increases confidence (Bandura, 1998), facilitates skill acquisition, and provides feedback (Schwarzer, 2008) by attending to the behavior of a model. Vicarious experience is rarely incorporated into PA behavior interventions (Ashford, Edmunds, & French, 2010).
The purpose of this pilot study was to evaluate the feasibility and effectiveness of a 12-week workplace intervention to increase PA behavior among inactive women using active peer role models compared with an attention control group (ACG). The study aims were to: (a) assess feasibility by evaluating the number of contacted/recruited participants, number of noncompleters, time for intervention delivery, missing data, and adherence to the intervention, and (b) determine the effect of a peer modeling workplace intervention on the primary outcome of cardiorespiratory fitness, and secondary outcome of cardiovascular risk. This study addressed an additional aim of examining participants’ perceptions of the intervention, peer modeling, and PA behavior change, which is reported elsewhere (Rowland et al., 2018).
Method
This study used an experimental, randomized, two-group repeated-measures (baseline and 12-week) design to evaluate the effect of a workplace, peer modeling PA intervention. Eligible participants were randomly assigned to either the intervention group (IG) or the ACG using a statistician-generated random assignment schedule.
Setting and Sample
The study setting was a Midwestern health system with approximately 3,500 employees, 80% of whom were female. Participant inclusion criteria were female employees between 19 years and 65 years of age, worked at least 20 hours per week, and self-reported 60 minutes or less of moderate or 20 minutes or less of vigorous PA per week. Exclusion criteria were greater than moderate cardiovascular risk (Arena, Pescatello, Riebe, & Thompson, 2014), unable to complete cycle fitness testing, pregnancy, working night shift, participating in a weight management or exercise program, and taking a beta-blocker medication.
Using G*Power (Faul, Erdfelder, Lang, & Buchner, 2007), sample size was determined under univariate repeated-measures ANOVA within-between interaction (Time × Group Effect), where alpha = .1, two groups over two time points, a sample size of 50 has 80% power to detect an effect size of f = .178, which is equivalent to a (d) of .357. The alpha level used was appropriate for a preliminary study (Hertzog, 2008). The medium effect size was consistent with workplace PA interventions using maximal oxygen consumption VO2max to measure fitness outcomes (Conn, Hafdahl, Cooper, Brown, & Lusk, 2009).
Intervention Development
The theoretical basis for the peer modeling intervention was a combination of social comparison theory (self-improvement based on comparison with others; Festinger, 1954) and self-efficacy theory (confidence in one’s capabilities to engage in a given behavior; Bandura, 1998). In this study, active peers served as role models (peer models) for successful engagement in healthy PA. The peer models were similar to participants in gender, age, occupation, and family demands. This intervention was designed to provide social comparison/vicarious experience opportunities with similar and successful peer models to increase participant confidence, motivation, and practical knowledge for self-improvement via PA.
Seven physically active female employees from the study site were recruited, interviewed, and trained to present their personal story of living an active lifestyle. Each peer model was asked to create a 20-minute PowerPoint presentation describing their experience of maintaining a minimum of 150 minutes of moderate level or greater PA per week for at least the past 6 months. Each peer model specifically described their motivation, barriers, facilitators, self-monitoring, goal setting, and technology used for PA. One peer model presented per session except for the last session when two peer models presented. Although only six sessions were scheduled, a seventh peer model was recruited in the event of a schedule conflict. Because no scheduling conflicts occurred, the extra peer model presented at the last session.
Peer Model Intervention
Following baseline testing, IG participants were privately counseled by a nurse practitioner on the results of their cycle fitness test and given an exercise prescription which included the following: (a) target (HR) range (HRmax – HRrest × % intensity desired + HRrest); (b) PA intensity based on cycle test results, 40% to 60% of HRreserve for low fit and 60% to 70% of HRreserve for moderately fit participants; (c) instruction on rating of perceived exertion (RPE) scale and encouragement to achieve a RPE of 12 to 15 for moderate intensity PA (Borg, 1982); and (d) goal to reach at least 150 minutes of moderate PA per week at prescribed target HR range and RPE range. In addition, the IG was asked to submit weekly PA logs (n = 12) documenting PA type, minutes, peak HR, and RPE during moderate PA lasting at least 10 minutes.
Over the 12-week intervention, the IG met every other week for a total of six 45-minute group lunch and learn presentations at the workplace. Each IG session was 10 minutes on PA health benefits, 20 minutes of peers presenting their PA PowerPoint story, and 10 to 15 minutes of peer questions and discussion related to PA issues. The IG learned from seven different peer models.
Attention Control Intervention
The ACG met every other week for six 45-minute group lunch and learn presentations for 12 weeks at the workplace. The ACG received general health information on diet, cancer screening, stress management, and sleep. The ACG did not receive fitness test results or an exercise prescription and were asked to maintain their current level of PA during the study.
Measures
Measures were collected at baseline and repeated at 12 weeks postintervention. An advanced practice nurse investigator, trained in fitness testing, completed all assessments and collected questionnaires in the employee fitness center.
Cardiorespiratory fitness
Estimated VO2max is an indicator of increased PA behavior and an accepted measure of cardiorespiratory fitness. A multi-stage submaximal cycle test using the Monark 827E ergometer (Monark Exercise AB, Vansbro, Sweden) was used to estimate VO2max and metabolic equivalents (METs; Arena et al., 2014). Following a 2-minute warm-up of low resistance pedaling (0.5 kg), participants maintained a pedaling speed of 50 rpm while resistance was increased by 0.5 kg every 3 minutes. The test was complete when either 85% of max HR was reached (220 – age) or the participant requested to stop. Work rate was estimated using participant’s age-predicted max HR and HR at end of last two stages completed. Estimated VO2max was calculated using VO2max (mL/kg−1/min−1) = 1.8 × work rate (kg/m/min−1)/body mass (kg). Resting HR was also measured before the cycle test as an indicator of cardiorespiratory fitness (Kang, Kim, & Ko, 2016).
PA behavior
Moderate or greater PA (≥3 METs; Arena et al., 2014) was measured using a tri-axial accelerometer (ActiGraph GT3X, ActiGraph LLC, Pensacola FL, USA). At baseline and postintervention, all participants were instructed to wear the monitor during wake time, on the hip, for seven consecutive days. ActiLife software 6.10.2 (ActiGraph LLC, Pensacola, FL, USA) was used to evaluate PA data stored with the epoch interval set at 1 minute. Wear time validation parameters were activity threshold of 10 counts per minute, minimum of 8 hours of wear time per day, and a minimum of 3 days of valid wear time per week. Activity levels were measured in counts per minute (cpm) and defined as sedentary = 0–99, light = 100–1,951, moderate = 1,952–5,724, or vigorous = 5,725 or more (Freedson, Melanson, & Sirard, 1998). Average weekly time spent in moderate or greater PA was calculated by the sum of moderate and vigorous PA minutes divided by number of valid wear days × 7.
Blood glucose and lipids
Venous blood was collected after an 8-hour fast. A Clinical Laboratory Improvement Amendments (CLIA) and College of American Pathologists (CAP) certified laboratory analyzed serum glucose, total cholesterol, high density lipoprotein (HDL) cholesterol, low density lipoprotein (LDL) cholesterol, and triglycerides using the Vitros 5600 analyzer (Ortho diagnostics, Raritan, NJ, USA).
Lifetime cardiovascular risk
The Lifetime Cardiovascular Risk calculator (lifetimerisk.org) was used to predict the 30-year risk of fatal and non-fatal cardiovascular disease (Berry et al., 2012). To calculate risk using this tool, self-report variables included age, gender, history of diabetes, and current smoking status. Measured variables were total cholesterol, body mass index (BMI), and fitness level in METs.
Procedures
This study was approved by the University’s Internal Review Board and the study site. Informed consent, questionnaires, blood collection, measurements, and exercise testing were completed in a private area of the study site’s employee fitness center. Randomization occurred after baseline testing.
Analysis
Statistical Package for Social Sciences (2016) software (v. 24) was used to analyze demographic and study variables for group by time interaction effects. Participants were examined on an intent-to-treat basis. Variables were first screened and then non-normally distributed variables (VO2max, METs, cardiovascular risk, and ActiGraph measured PA) were log transformed. Analysis was initially planned with repeated-measures ANOVA. Participant noncompleters (IG = 9; ACG = 3) prompted a change to hierarchical linear modeling to analyze group by time interactions for the primary outcome of cardiorespiratory fitness and secondary outcome of cardiovascular risk. Because this research was a feasibility study, statistical significance was determined with a p value < .10.
Results
At baseline, the ACG and IG were similar in mean years of age (ACG M = 43 ± 8.8; IG M = 43 ± 12.4), predominately Caucasian, employed full-time, and married or partnered (Table 1). Compared with the ACG, more participants in the IG worked as clinical staff versus nonclinical staff. The IG had slightly higher self-report and measured moderate PA per week compared with the ACG; however, estimated VO2max, METs, and resting HR were nearly identical for both groups at baseline (Table 2).
Baseline Female Participant Demographics
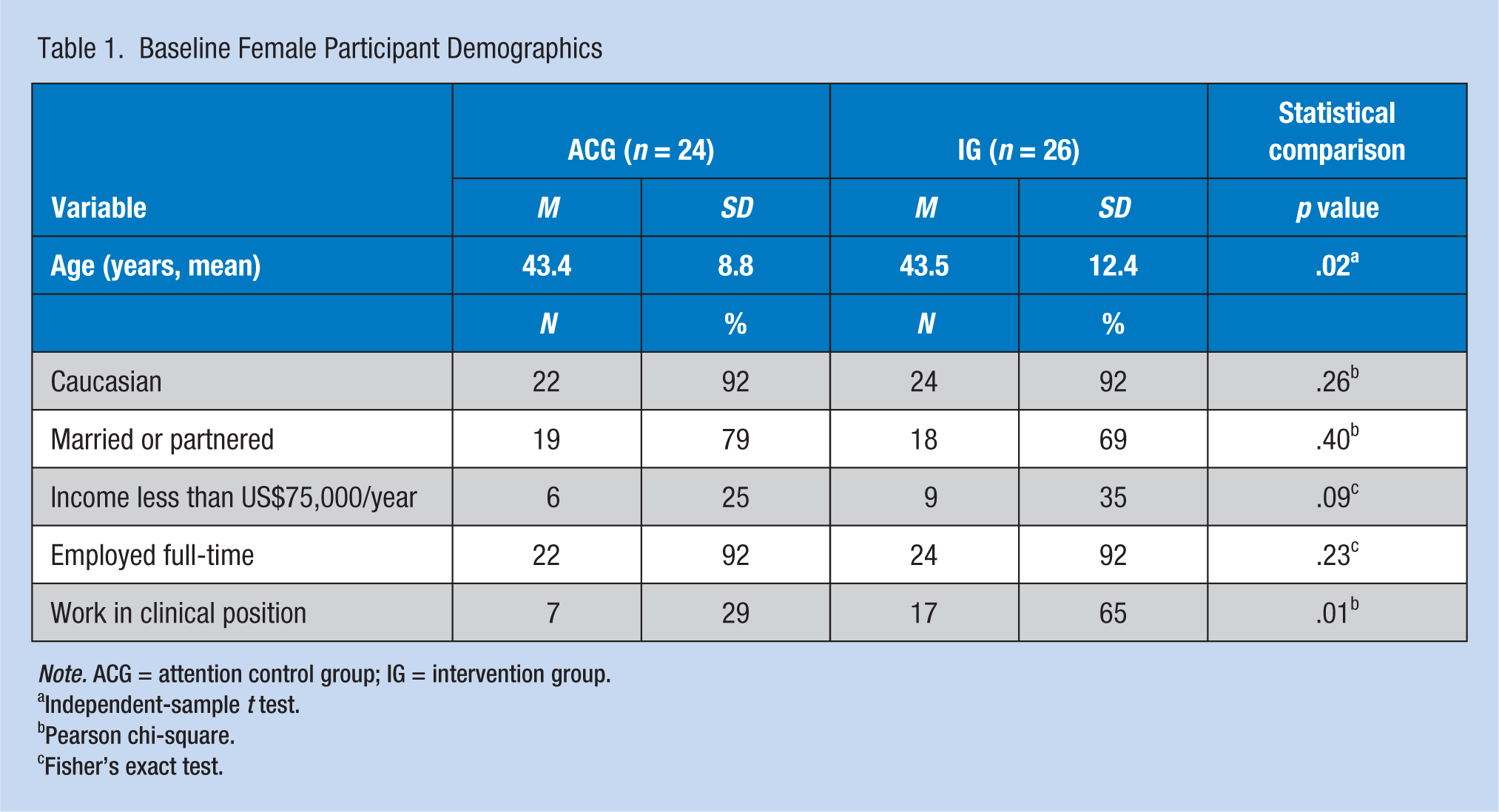
Note. ACG = attention control group; IG = intervention group.
Independent-sample t test.
Pearson chi-square.
Fisher’s exact test.
Baseline Mean Values for Fitness and Cardiovascular Risk Indicators by Group
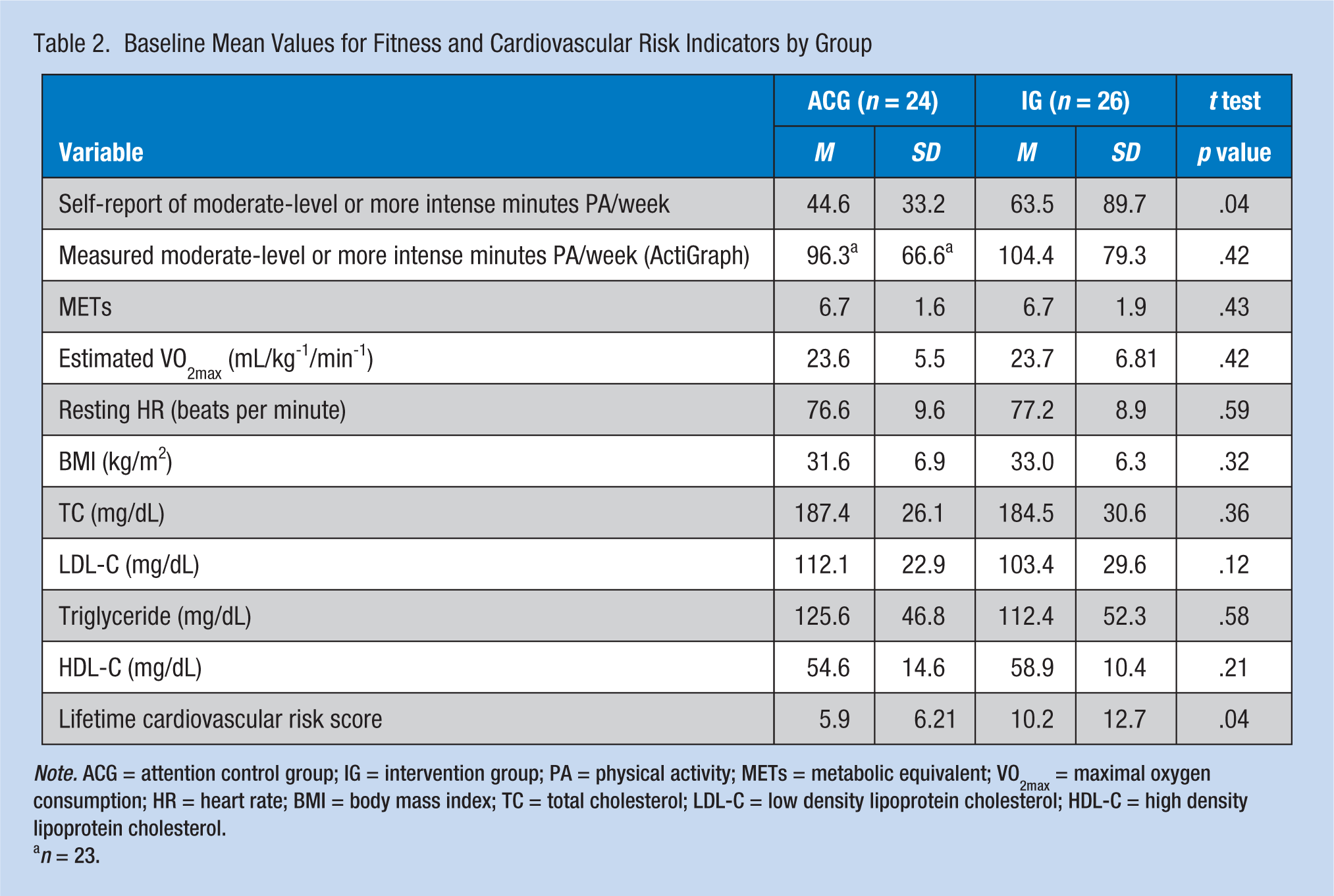
Note. ACG = attention control group; IG = intervention group; PA = physical activity; METs = metabolic equivalent; VO2max = maximal oxygen consumption; HR = heart rate; BMI = body mass index; TC = total cholesterol; LDL-C = low density lipoprotein cholesterol; HDL-C = high density lipoprotein cholesterol.
n = 23.
Feasibility
A 6-week recruitment/enrollment period mid-December through January resulted in recruiting the target sample size (n = 52; Figure 1). Using the organization’s established communication methods (intranet, print newsletter, signage in occupational health office) to recruit potential participants was effective and low cost. Employees with interest in the study (n = 113) emailed the principal investigator (PI) with questions about participating. To facilitate enrollment, four information sessions about the study were held at the workplace. Reasons cited by interested employees for not participating were schedule conflicts, inability to choose group assignment, too active for inclusion criteria, pregnant or planned pregnancy during study, and taking a medication that limited HR (beta-blocker).
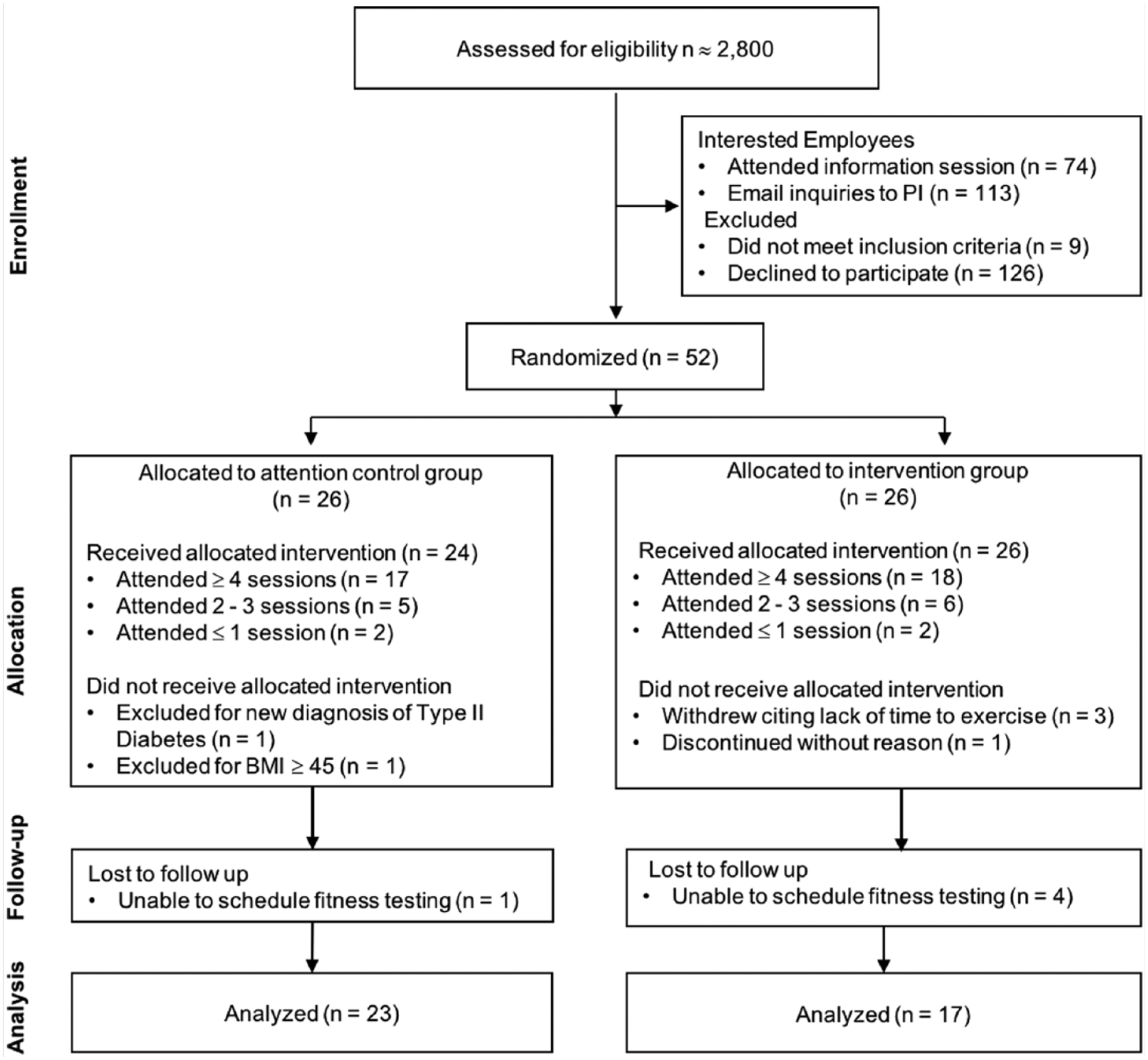
Study flow diagram.
Participation
Following informed consent, 52 women were randomized to either the ACG (n = 26) or the IG (n = 26). All participants completed baseline measures; postintervention measures were completed by 92% (n = 23) of the ACG and 65% (n = 17) of the IG (Figure 1). Both groups had similar attendance rates for the six lunch and learn sessions (ACG M = 4.2 ± 1.7; IG M = 4.2 ± 1.5). An additional indicator of participation in the IG was the submission of 12 weekly PA logs (M = 8.3 ± 1.5). Of those in the IG who completed posttesting measures (n = 17), 65% (n = 11) had high participation (≥4 sessions and ≥90 minutes PA/week) and 35% (n = 6) had moderate participation (≥2 sessions and/or 30 to 90 minutes PA/week). Low participation (≤1 session and/or ≤30 minutes PA/week) was characteristic of most of the IG participants who did not complete postintervention fitness testing.
Retention
Postintervention scheduling and measurement completion, particularly the cycle fitness test, were more challenging in the IG than the ACG. Only 65% (n = 17) of IG completed the postintervention cycle fitness test compared with 92% (n = 22) of the ACG. Lunch and learn session attendance averaged 66% for both groups.
Outcomes
Primary outcomes
No significant differences between the groups were found by time interactions for estimated VO2max, METs, or resting HR. Although nonsignificant, the IG had greater improvement in VO2max (IG = 6.7%; ACG = 4.2%), METs (IG = 5.5%; ACG = 4.4%), and resting HR (IG = −5.3%; ACG = −1.0%) compared with the ACG (Table 3).
Mean Values for Cardiorespiratory Fitness and Cardiovascular Risk Indicators by Group
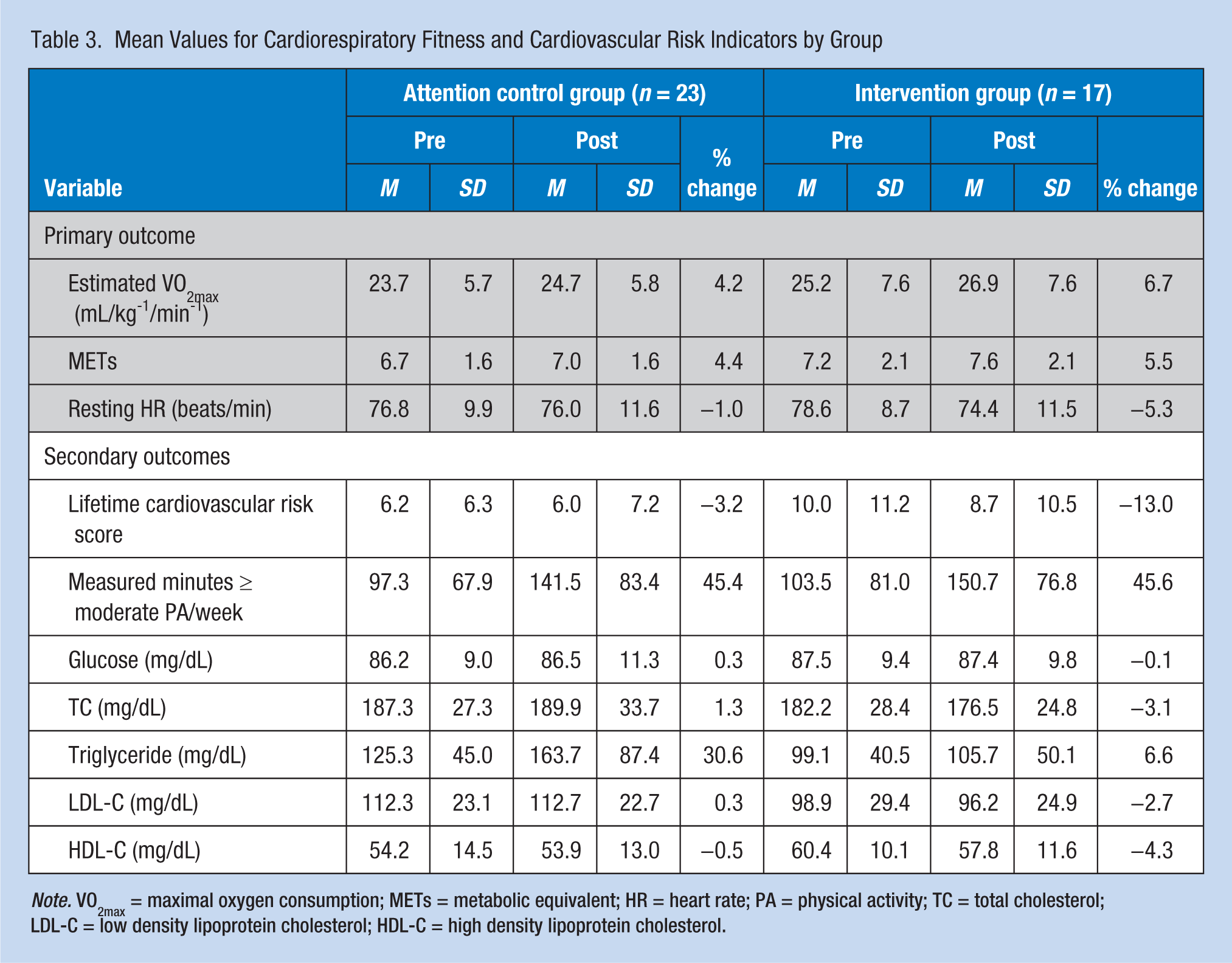
Note. VO2max = maximal oxygen consumption; METs = metabolic equivalent; HR = heart rate; PA = physical activity; TC = total cholesterol; LDL-C = low density lipoprotein cholesterol; HDL-C = high density lipoprotein cholesterol.
Secondary outcomes
No significant group by time interactions were found for secondary outcome measures of cardiovascular risk (i.e., glucose, lipids, ActiGraph measured PA, and lifetime 30-year risk). Over time, both groups significantly increased PA, F(df = 1) = 11.49, p = .002, and decreased cardiovascular risk, F(df = 1) = 6.550, p = .014. Although not significant, improvements favored the IG in lifetime cardiovascular risk (IG = −13.0%; ACG = −3.2%), total cholesterol (IG = −3.1%; ACG = 1.3%), triglycerides (IG = 6.6%; ACG = 30.6%), and LDL (IG = −2.7%; ACG = 0.3%; Table 3). The IG had a greater reduction in HDL than the ACG (IG = −4.3%; ACG = −0.5%).
Discussion
This is the first study found to use a randomized, two-group intervention design to affect PA behavior using vicarious experience (attention to someone successfully performing a given behavior) with peer models in the workplace. Vicarious experience of physically active working women to favorably affect the PA behavior of inactive working women shows promise as an intervention for PA behavior change.
A main finding of this study was that the PA intervention was feasible. Active peer models were recruited and trained; participants were recruited and enrolled; and the intervention was delivered at the workplace. More noncompleters in the IG compared with the ACG could be explained by lack of participant readiness to change PA behavior. It is possible that although increasing PA behavior was appealing, actual behavior change may require more than participants were prepared to do. Several participants in the IG group cited lack of time for PA as the reason for not completing the study. In addition, it was more difficult to schedule those workers in the IG group with low-level study participation (session attendance and PA log submission), despite encouragement to complete postintervention testing regardless of PA level during the study. This situation was not the case for the ACG and IG participants who had regular session attendance and PA log submission. Early noncompleters and low-level participators in the IG may have been in precontemplation or contemplation stages of behavior change (Prochaska & Velicer, 1997).
Another main finding is that although not statistically significant, primary and secondary outcomes improved more in the IG than the ACG. The IG had greater improvements in measures of fitness (estimated VO2max, METs, resting HR) and cardiovascular risk (total cholesterol, triglyceride, LDL, calculated risk score) compared with ACG. This finding is notable given 35% of the IG could be characterized as low-level participators (≤1 session and/or ≤30 minutes self-report PA/week).
According to ActiGraph measured PA pre- and postintervention, both groups increased their PA behavior. The women, knowing they were in a PA behavior study, may have been motivated to increase PA during ActiGraph measurement. If the ACG had increased time and/or intensity of PA throughout the study, postintervention fitness measures should have been comparable with the IG. Although not significant, the IG had greater improvement in VO2max, METs, and resting HR compared with the ACG, suggesting the IG engaged in more and/or more intense PA throughout the study.
Implications for Practice
Future PA behavior interventions may address the loss of participants by use of readiness to change screening and/or inclusion criteria to include only those who are in preparation and action stages of change (Prochaska & Velicer, 1997). Continued enrollment to replace dropout participants once the intervention had begun was not feasible. Interventions delivered in the workplace have appeal, offering employees a convenient, low cost means to support health behavior change. Excluding participants in the precontemplation stage of change would facilitate efficient use of resources and promote a stronger group dynamic. Social norms, social patterns of behavior, social support, and modeling all have influence on PA behavior (McNeill, Kreuter, & Subramanian, 2006). Nonattendees may have weakened intervention effects through missed opportunities for participants to connect with others making the same changes in PA behavior or partner to engage in PA together.
The peer modeling intervention has promise as an effective and feasible method of PA behavior change among inactive working women by using resources already commonplace in organizations: fitness center, occupational health office and staff, and employees who were already successful engaging in a healthy level of PA. Total Worker Health® research supports integrating occupational and wellness activities to increase intervention efficacy and/or boost fiscal efficiency (Barbeau et al., 2012). Employees intersect with occupational health services for both scheduled and episodic services. Therefore, occupational health nurses may be a key point of connection linking physically inactive workers to individuals and places within the organization that facilitate healthy PA behavior. These social connections are known to support healthy PA through increased PA time, knowledge, adherence to PA goals, and reduced body fat (The Community Guide, 2014).
A common focus of workplace wellness programs is weight loss. However, just as weight, BMI, and blood pressure can be measured and counseled in the occupational health setting, so too can self-reported PA behavior, resting HR, and even fitness. Adults with low to moderate cardiovascular risk are appropriate for submaximal fitness testing such as walk/run, cycle, or step tests. Because “fitness” is more influential on morbidity and mortality than “fatness,” methods of assessing and boosting fitness are needed (Barry et al., 2014; McAuley et al., 2014). Occupational health nurses should address the fitness deficit among working adults by screening for personal and occupational risks of physical inactivity. Both employers and employees benefit from a physically fit workforce through reduced health care costs and absenteeism, and increased productivity (Centers for Disease Control and Prevention, 2017).
Limitations to the study include a small sample size, predominately Caucasian participants, and a single workplace which limit generalizability to other populations and other work environments. Another limitation relates to assessment of PA behavior using “spot checking” with an activity monitor. In this study, PA behavior in both groups was assessed using an ActiGraph worn daily for 1 week at baseline and postintervention. The Hawthorne effect may actually explain the increase in PA behavior in both groups (McCambridge, Witton, & Elbourne, 2014). Knowing PA is being monitored may prompt employees to be more active. Objectively measuring physiologic indicators of PA behavior (resting HR, VO2max, blood pressure, cholesterol, glucose) may provide a more accurate indication of behavior change and associated health benefits. A strength of this study was the randomized design intervention, testing for the first time a strategy using peer models to provide vicarious experience to increase PA behavior in the workplace. The findings support the need for a fully powered study.
Applying Research to Practice
Peer models may be an effective means of increasing PA among inactive employees. Although not significant in this small sample, compared with those workers who received general health information, the workers exposed vicariously to active peers had greater improvement in fitness and cardiovascular risk.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Research reported in this publication was supported by the University of Nebraska Medical Center Nellie House Craven Scholarship and the National Institute of Nursing Research of the National Institutes of Health under Award Number F31NR016174. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health.
Author Biographies
Sheri A. Rowland is an Assistant Professor at the University of Nebraska Medical Center College of Nursing. Sheri is an early career nurse researcher with interest in the social influences on physical activity behavior in women.
Kris E. Berg is a Professor Emeritus and former Director of the Clinical Exercise Physiology Lab at the University of Nebraska Omaha. Kris has several decades of experience in design of exercise programs and fitness assessment, particularly among persons with chronic health conditions.
Kevin A. Kupzyk is a biostatistician in the College of Nursing at the University of Nebraska Medical. Kevin has research interest in multivariate statistics, assessment, longitudinal methods, structural equation modeling, latent growth curve modeling, power analysis, and multi-level modeling.
Carol H. Pullen is a professor in the College of Nursing at the University of Nebraska Medical Center. Carol has been awarded three RO1 NIH grants for her research on promoting healthy eating and physical activity behaviors in midlife and older rural women.
Marlene Z. Cohen is a professor at the University of Nebraska Medical Center College of Nursing. Marlene has been a NIH funded researcher investigating the patient experience for health promotion and disease prevention. Marlene is currently a nurse researcher at the VA Nebraska-Western Iowa Healthcare System.
Paula S. Schulz is an associate professor at the University of Nebraska Medical Center College of Nursing. Paula is an NIH funded nurse researcher with experience and interest in cardiovascular risk reduction in cardiac patients and their spouses.
Bernice C. Yates is a Professor Emeritus at the University of Nebraska Medical Center College of Nursing. Bernice has been funded by the NIH to study couple-focused interventions to assist cardiac patients and spouses with the adoption and maintenance of health behaviors.