
Abstract
The workplace is cited as a promising setting for physical activity (PA) promotion, but workplace PA interventions tend not to specifically target men. The aim of this article was to review the literature on workplace PA interventions for men and to identify key issues for future intervention development. Articles targeting PA at the workplace were located through a structured database search. Information on intervention strategies and PA outcomes were extracted. Only 13 studies (10.5%) reviewed focused on men, of which 5 showed significant increases in PA. These studies used generic, multicomponent, health promotion strategies with a variety of timeframes, self-report PA measures, and PA outcomes. The systematic review identified that evidence on the effectiveness of workplace PA interventions for men is equivocal and highlighted methodological concerns. Future research should use reliable and valid measures of PA and interventions that focus specifically on men’s needs and PA preferences.
In adults, optimal health benefits are associated with achieving 30 minutes of moderate-intensity physical activity (PA) at least five times a week (Australian Institute of Health and Welfare, 2010; Office of Disease Prevention and Health Promotion, 2008). In developed nations such as Australia, the United Kingdom, and the United States, only 42%, 40%, and 51% of adult men meet these guidelines, respectively (Allender, Peto, Scarborough, Kaur, & Rayner, 2008; Australian Institute of Health and Welfare, 2011; U.S. Department of Health and Human Services, 2010).
High levels of physical inactivity in men, combined with evidence linking inactivity to chronic conditions such as cardiovascular disease (Kohl, 2001), cancer (Parent et al., 2011), obesity (Astrup, 2001), and type 2 diabetes (Hu, Li, Colditz, Willett, & Manson, 2003), highlight the importance of identifying effective interventions through which men can be encouraged to engage in regular PA. A number of reviews have identified the workplace as a valuable setting for health promotion interventions (Dishman, DeJoy, Wilson, & Vandenberg, 2009; Dishman, Oldenburg, O’Neal, & Shephard, 1998; Hooper & Bull, 2009; White, Conrad, & Branney, 2008), and workplace PA promotion has been associated with a reduction in health risks (Engbers, van Poppel, Chinapaw, & van Mechelen, 2005; Harris, 1994; Makrides et al., 2008). The workplace holds significant potential as a context for PA interventions, and this potential may be particularly relevant to men, given that employed men spend an average of 8 hours/day at work (Australian Bureau of Statistics, 2008; Baxter, Gray, & Hayes, 2007).
However, it could be argued that even though there are more men than women at the workplace, workplace PA interventions have tended not to engage men (Adshead & Thorpe, 2008; Plotnikoff et al., 2007; Pritchard, Nowson, & Wark, 1997). Walking, for example, is a popular form of PA intervention in workplaces (Gilson, McKenna, Puig-Ribera, Brown, & Burton, 2008; Gilson et al., 2009), yet qualitative findings suggest that this form of PA fails to appeal to most men (Burton, Walsh, & Brown, 2008). Consequently, uptake by male employees has typically been poor, and study samples tend to be dominated by women (Waters, Galichet, Owen, & Eakin, 2011).
At present, very little is known about either the number or nature of workplace PA intervention studies that have focused on men’s needs or how effective these studies have been at changing PA behavior. The most recent and comprehensive reviews of workplace PA interventions provide no insights into gender differences or preferences (Abraham & Graham-Rowe, 2009; Conn, Hafdahl, Cooper, Brown, & Lusk, 2009; Dugdill, Brettle, Hulme, McCluskey, & Long, 2008). This study reviewed the literature on workplace PA interventions, with a specific focus on men’s issues. The aims of the review were to identify (a) workplace interventions that reported on men’s PA outcomes and (b) strategies that were effective for promoting PA in men.
Method
Literature Search
The databases PubMed, EMBASE, PsycINFO, CINAHL, and CENTRAL (Cochrane Central Register of controlled trials) were searched for relevant studies published up to October 2010. Groups of thesaurus terms and free term words such as worksite, workplace, physical activity, intervention, employee, and worker were used (see the appendix for complete search terms). Additional papers were identified by manually checking the reference list of the included papers—workplace PA review papers and meta-analyses—and by searching the authors’ own literature databases based on the inclusion criteria.
Inclusion Criteria and Selection Process
Titles, keywords, and abstracts were reviewed, and out of scope papers were removed by JW. The first two authors (JW and NG) independently checked the full text of potentially eligible peer-reviewed English language papers based on the following inclusion criteria. (a) Design: intervention study with randomized controlled trials (RCT); quasi-experimental, controlled trials (CT); or pretest–posttest design (P-P). (b) Population: healthy working men without serious health conditions or physical impairment. Papers were selected if the study included women and findings for men were reported separately. Papers that combined data and did not report on data from only men were rejected. (c) Intervention and outcome: workplace interventions that aimed to increase PA or improve health, with PA as a primary or secondary outcome measure. Any disagreements on study inclusions were resolved through discussions between JW and NG, following independent review.
Data Extraction
Details on study design, workplace description, participant characteristics (proportion of men and age), study objectives, intervention strategies and duration, PA measurement protocols, and changes in PA were extracted. The effectiveness of the strategies for promoting PA in each study group was also assessed relative to PA change.
Results
A flow diagram depicting the search process is shown in Figure 1. After removing duplicates, the electronic database search yielded 602 records. Forty-nine additional papers were identified through other sources, for example, from the reference list of review papers. With three duplicates removed, the titles and abstracts of 648 papers were screened for eligibility and 527 papers were rejected because they were out of scope. The remaining 121 full-text papers were assessed for eligibility; 107 of these were excluded for the reasons shown in Figure 1. Fourteen papers, representing 13 studies, were included in this review.

Flow diagram of papers identified and rejected
Study Design and Participant Characteristics
The selected studies included five RCTs (Kamioka et al., 2009; Nisbeth, Klausen, & Andersen, 2000; Plotnikoff et al., 2007; Pritchard, Nowson, Billington, & Wark, 2002; Pritchard et al., 1997; Rosenfeld, Ruskin, Halfon, & Tenenbaum, 1990), five CTs (Arao et al., 2007; Bauer, Heller, & Challah, 1985; Blair, Piserchia, Wilbur, & Crowder, 1986; Cook, Simmons, Swinburn, & Stewart, 2001; Moy, Sallam, & Wong, 2006), and three P-Ps (Fujii et al., 2009; King, Carl, Birkel, & Haskell, 1988; Wier et al., 2001). The aims and participant characteristics are summarized in Table 1. Eight studies recruited only men (Arao et al., 2007; Bauer et al., 1985; Cook et al., 2001; Kamioka et al., 2009; King et al., 1988; Moy et al., 2006; Nisbeth et al., 2000; Pritchard et al., 1997; Pritchard et al., 2002). The remainder recruited both men and women but reported findings separately for men (Blair et al., 1986; Fujii et al., 2009; Plotnikoff et al., 2007; Rosenfeld et al., 1990; Wier et al., 2001). Across mixed gender studies, the proportion of men ranged from 23% to 69%.
Characteristics of Included Studies
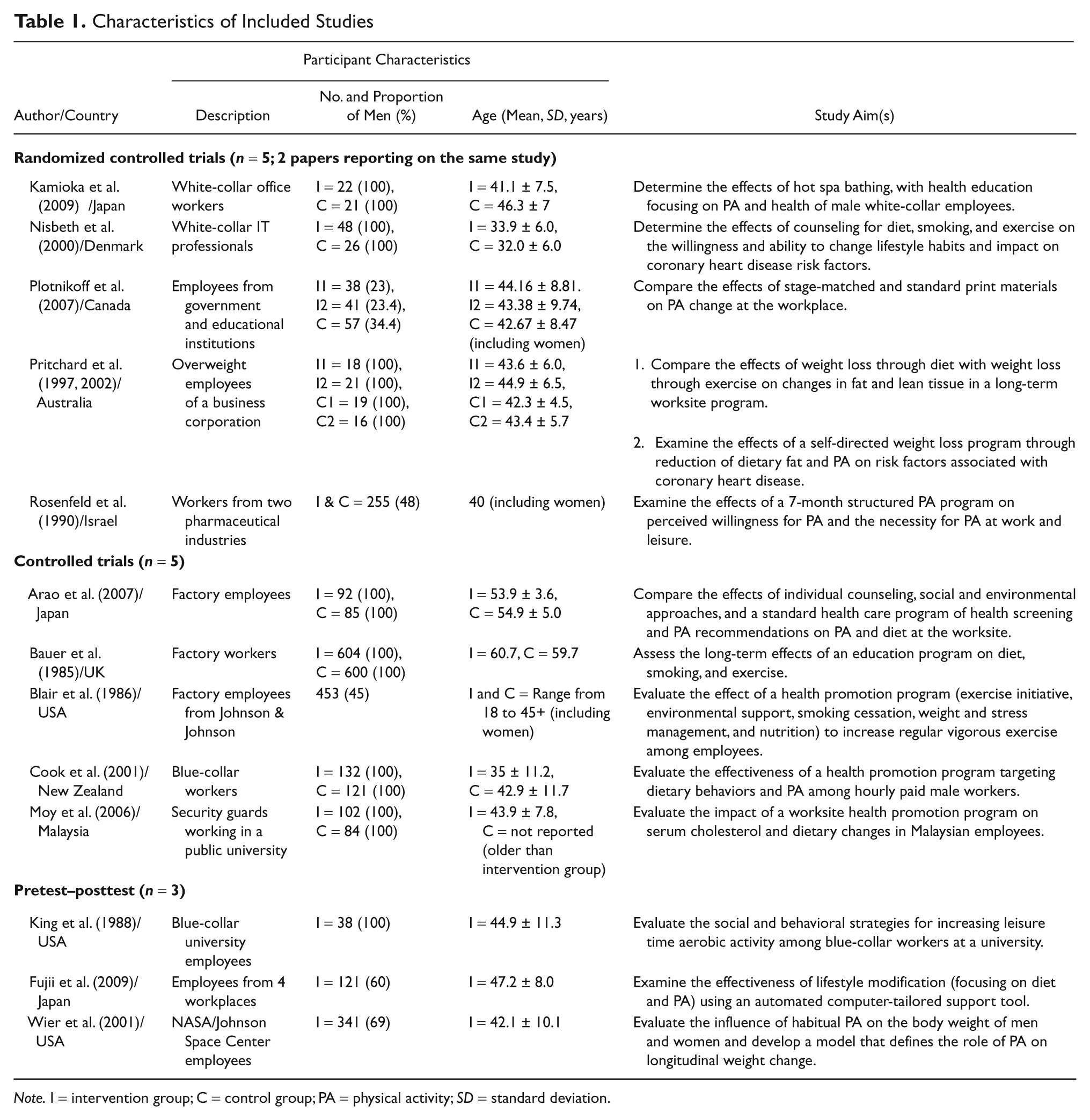
Note. I = intervention group; C = control group; PA = physical activity; SD = standard deviation.
In all the studies, sample size ranged from 38 to 1,204 men (Bauer et al., 1985; King et al., 1988), with an age range of 18 to 60 years (Bauer et al., 1985; Blair et al., 1986). Participants were predominantly middle-aged, blue- and white-collar employees working in a variety of workplaces, including factories (Arao et al., 2007; Blair et al., 1986; Cook et al., 2001; Rosenfeld et al., 1990), offices (Kamioka et al., 2009; Nisbeth et al., 2000), and government and educational institutions (King et al., 1988; Moy et al., 2006; Plotnikoff et al., 2007).
Details of intervention strategies, theoretical frameworks, measurement protocols, and PA outcomes are shown in Table 2. The duration of the interventions ranged from 4 months (Fujii et al., 2009; King et al., 1988) to 6 years (Bauer et al., 1985), and all studies used self-report measures to assess changes in PA. PA was measured at baseline, with follow-up ranging from 4 months (Fujii et al., 2009; King et al., 1988) to 5 years (Bauer et al., 1985).
Intervention Strategies, Measurement Protocols, and PA Outcomes

Note. I = intervention group; C = control group; PA = physical activity; MET = metabolic equivalent of task; TTM = transtheoretical model; TPB = theory of planned behavior; PMT = protection motivation theory; SCT = social cognitive theory; PHM = public health model; JALSPAQ = Japan Arteriosclerosis Longitudinal Study Physical Activity Questionnaire; GLTEQ = Godin Leisure-Time Exercise Questionnaire; KIHDRFS = Kuopio Ischemic Heart Disease Risk Factors Study; WFQ = Worker’s Functioning Questionnaire; NAS = NASA Activity Scale.
Validity of questionnaire used not reported.
PA Measures
Four studies used researchers’ own questionnaires to report on PA (Blair et al., 1986; Cook et al., 2001; Fujii et al., 2009; Moy et al., 2006), and two studies used point scales to elicit information on PA frequency and levels (Bauer et al., 1985; Nisbeth et al., 2000); the validity of these measures was not reported. One study measured PA as an index, calculated from the type, duration, and frequency of the PA, as recorded by employees in diaries and activity logs (Pritchard et al., 2002). Another study assessed PA by recording exercise sessions on a group chart posted in a work area (King et al., 1988). Changes in PA were expressed as estimates of total energy expenditure (Arao et al., 2007; Plotnikoff et al., 2007) in MET/min or kcal/week, total minutes spent doing PA (Kamioka et al., 2009; King et al., 1988), an activity index (Pritchard et al., 1997; Pritchard et al., 2002), the proportion of men achieving a predetermined threshold of PA (Blair et al., 1986; Moy et al., 2006; Rosenfeld et al., 1990), or frequency of participation (Fujii et al., 2009).
Intervention Strategies and Effectiveness for Promoting PA
The majority of studies targeted a range of behaviors and associated outcomes through generic strategies that combined PA promotion with smoking cessation and weight and stress management (Arao et al., 2007; Bauer et al., 1985; Blair et al., 1986; Cook et al., 2001; Kamioka et al., 2009; King et al., 1988; Moy et al., 2006). Only four studies (Blair et al., 1986; King et al., 1988; Plotnikoff et al., 2007; Rosenfeld et al., 1990) focused exclusively on PA strategies and behavior measurement. Five studies used theoretical framework to guide their intervention (Arao et al., 2007; Blair et al., 1986; Cook et al., 2001; Fujii et al., 2009; Plotnikoff et al., 2007).
Two studies reported no change in men’s PA (Bauer et al., 1985; Blair et al., 1986). Six studies reported nonsignificant increases using intervention strategies that included encouragement to do free-choice PA (Kamioka et al., 2009; Nisbeth et al., 2000), an education program and a self-supervised fitness program (Wier et al., 2001), PA counseling (King et al., 1988; Moy et al., 2006), and print materials (King et al., 1988; Moy et al., 2006; Plotnikoff et al., 2007). The remaining five studies (two RCTs, two CTs, and one P-P) reported significant increases in PA (Arao et al., 2007; Cook et al., 2001; Fujii et al., 2009; Pritchard et al., 1997; Pritchard et al., 2002; Rosenfeld et al., 1990); three of the studies that showed a PA increase (two CTs and one P-P) used a theoretical framework (Arao et al., 2007; Cook et al., 2001; Fujii et al., 2009).
In the first RCT that reported significant change, Pritchard and colleagues identified that encouraging free-choice activities increased PA by 15.6% compared with a 3.4% increase in men who were given print materials and counseled on diet change (Pritchard et al., 1997; Pritchard et al., 2002). In a third group, who received both strategies, there was a significant PA increase of 7.2%. In the second RCT (Rosenfeld et al., 1990), men who attended instructor-led PA classes significantly increased their PA by 7.3% compared with men in the control group.
Two CTs (Arao et al., 2007; Cook et al., 2001) reported significant increases in exercise energy expenditure and PA time. Arao et al. (2007) used strategies such as PA counseling, family involvement in PA, and environmental change around the workplace (i.e., healthier lunch menus) and reported a significant increase in energy expenditure of 346 kcal/week, while energy expenditure in the control group decreased by 163 kcal/week. Cook et al. (2001) reported significant increases in moderate and vigorous PA (0.9 and 2.8 hr/week) compared with decreases in the control group (−1.7 and −2.6 hr/week). Intervention strategies in this study combined environmental change in the workplace with monthly education workshops on health and PA.
The only P-P study to report a significant PA increase (Fujii et al., 2009) used an interactive web-based program targeting intrapersonal domains such as goal setting, self-monitoring, and feedback. Findings reported an increase of 12.4% in the proportion of men who exercised two or more times per week.
Discussion
The aims of this article were to review the literature on workplace PA interventions that reported on men’s PA outcomes and to identify strategies that were effective for promoting workplace PA in this important target group. The review suggests that few workplace PA interventions have reported data for men. Of the full-text papers assessed, we identified only 13 studies (10.5% of those reviewed) that met inclusion criteria.
Of the limited number of papers that presented findings for men, around 40% (or 5 from 13) reported significant increases in PA. Four of these studies were RCTs or CTs, and while sometimes difficult to apply in real-world settings, more studies, which adopt these types of higher quality study designs, are needed. Three of the five studies used a theoretical framework, suggesting that the adoption of models and theories may benefit intervention planning and design. This said, the intervention strategies used in the five studies varied widely and tended to be part of multicomponent approaches targeting a range of health behaviors. Given the limitations of the current evidence base and the different types of strategies used, at this present time, it is difficult to identify which components, or combinations of components, are most effective at promoting men’s workplace PA. Furthermore, these studies used a variety of timeframes, self-report PA measures, and PA outcomes (e.g., absolute changes in PA time, bouts, or percentage change).
The findings highlight an important gap in the extant literature and a dearth of evidence on workplace intervention strategies for men. Strategies and approaches that lack PA specificity and invalid or unreliable PA measures further limit insights into intervention effectiveness.
Future studies need to address these concerns to better inform the use of PA strategies for men in the workplace. To develop the quantity and quality of evidence on strategies for increasing PA among working men, researchers should consider three guidelines. First, in line with other workplace reviews (Conn et al., 2009; Dugdill et al., 2008), men’s PA interventions should use valid and reliable self-report or objective measures of PA (pedometers or accelerometers). This will allow for detailed and accurate comparisons of strategy efficacy across different interventions. Second, interventions that target PA either specifically, or as part of a theory-driven multicomponent health initiative, are more likely to be effective at changing PA behavior (Abraham & Graham-Rowe, 2009). Finally, most workplace PA intervention studies tend to include men and women, with more women than men volunteering to participate in trials (Waters et al., 2011). Interventions are needed that specifically target men through consultation at the preintervention and planning phase. This approach will not only facilitate men’s involvement, but it will also enable strategies to be built that reflect men’s real-world PA needs and preferences.
Consideration of these guidelines should be set against the caveat of the relatively small number of studies identified for inclusion. This was a limitation of the review and reflects the paucity of evidence found for men’s workplace PA interventions. Also, although the search undertaken was comprehensive, it is possible that the literature search did not identify all published studies in the area, because of, for example, language issues or publication bias.
Conclusion
To our knowledge, this is the first systematic review to examine workplace PA interventions in men. The study findings suggest that the evidence base is limited by a small number of studies and key methodological concerns. To better inform practice efforts, future research needs to use objective measures of PA and develop bottom-up, primary workplace PA interventions that focus on men’s PA needs and preferences.
Footnotes
Appendix
Search Terms Used for Databases a
| Database | PubMed (MeSH and Free Terms) | Embase (Emtree and Free Terms) | PsycINFO and CINAHL (Search Terms) | CENTRAL (MeSH and Free Terms) |
|---|---|---|---|---|
| Setting | workplaces, employment, work place, work-place, place of work, job, job site, job-site, jobsite, office, office-based | workplace, employment, work place, jobsite, job-site, job site, office, office based | workplace, work place, jobsite, job-site, job site, office, office based, employment | workplace, work place, work-place, job, office, office based, place of work |
| Population | worker, employee, white collar, white-collar, blue collar, blue-collar | worker, employee, blue collar, white collar | worker, employee, white collar, blue collar, white-collar, blue-collar | worker, employee, white collar, white-collar, blue collar, blue-collar |
| Design | intervention studies, randomized controlled trial, control groups intervention, randomised controlled trial, control group, randomized controlled trial [publication type], controlled trial, review [publication type] | intervention study, randomized controlled trial, control group, randomised controlled trial, randomized clinical trial, randomized clinical trial | intervention, intervention studies, randomized controlled trial, randomised controlled trial, controlled trial, control group, review | intervention studies, randomized controlled trial, randomised controlled trial, control group, controlled trial |
| Outcome | physical activity, motor activity, exercise, physical fitness, physical activities, sport, sports, sporting, fitness, exercise, walking | physical activity, walking, exercise, sport | physical activity, exercise, physical activities, sport, fitness, walking | motor activity, exercise, physical activity, physical activities, sport, fitness, walking |
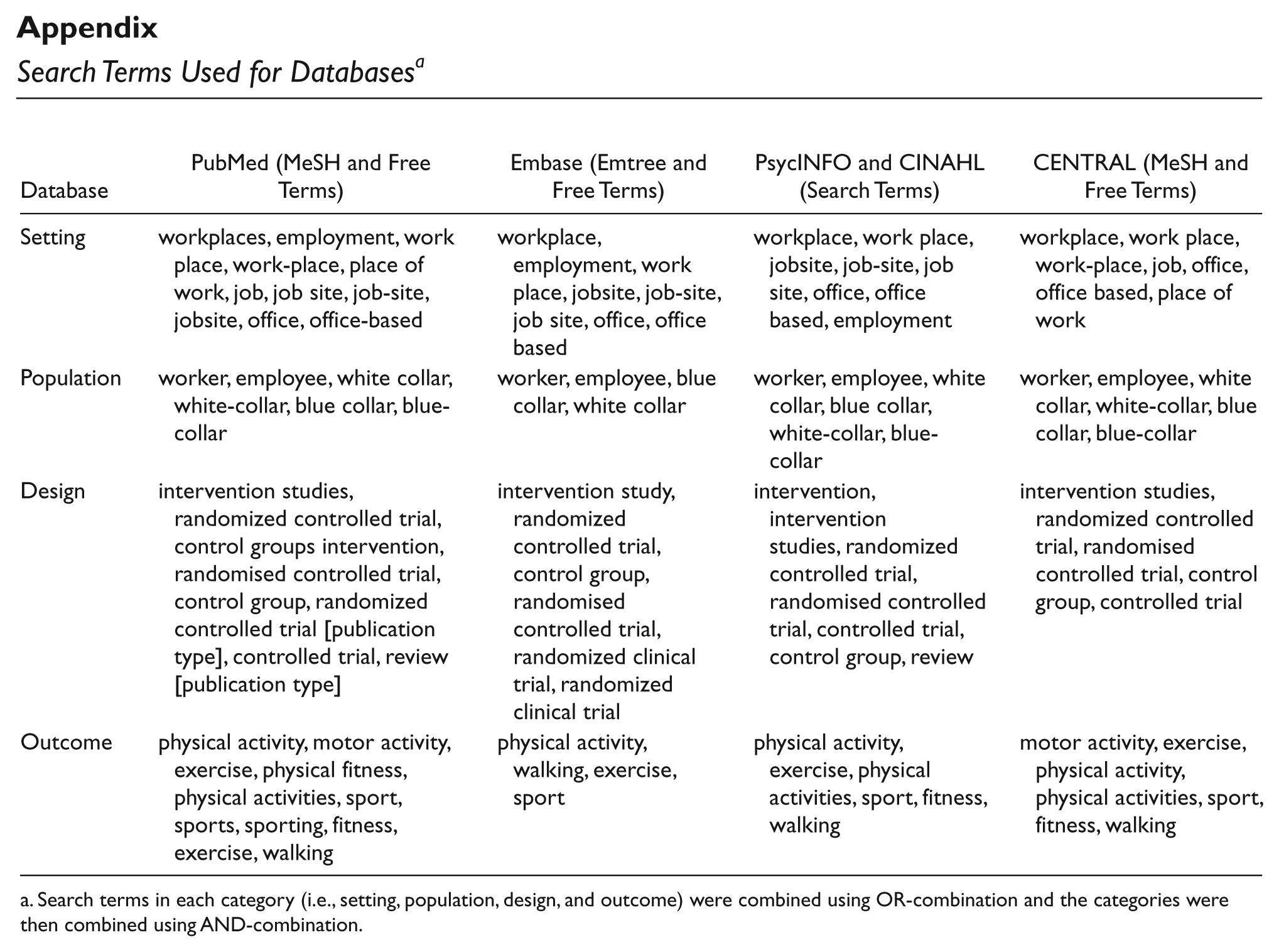
Search terms in each category (i.e., setting, population, design, and outcome) were combined using OR-combination and the categories were then combined using AND-combination.
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Jason Y. L. Wong is supported by the Australian Postgraduate Award Scholarship (The University of Queensland). Jannique G. Z. van Uffelen was supported by National Health and Medical Research Council Program Grant (#569940) at the School of Human Movement Studies, The University of Queensland.