
Abstract
Background:
The sedentary aspects of work have been associated with increased health risks. The purpose of this study was to compare the effects of high intensity interval training (HIIT) and increased steps on anthropometric, body mass, and body composition changes over a 12-week period.
Methods:
12 sedentary, obese, body mass index (BMI) = 32.98 ± 3.21 kg/m2, adult (46.10 ± 9.56 years), females volunteered for the study and were randomly assigned into one of the two groups, the HIIT group and the STEP group. During the 12-week study, all participants’ movements were monitored during their workday, via an accelerometer, a Movband™, 5 days/week.
Findings:
The HIIT group (n = 5) engaged in structured exercise (~15.0 ± 3.5 minutes), defined as total body moves which consisted of eight different routines: upper and lower extremity, two cardio segments, two total body, yoga, and abdominal exercises. The STEP group (n = 7) averaged ~7,000 steps/day throughout 12 weeks. Pre- and post-program measurements included: five anthropometric measurements (biceps, waist, abdomen, hips, and thigh), along with body mass and body composition measures: relative (%) body fat via dual x-ray absorptiometry (DEXA) scan, fat mass, fat-free mass, and lean mass.
Conclusions:
Statistical significance was determined among participants for biceps, hips, and thigh measurements along with body mass and body composition changes for improved health.
Application to Practice:
This work is suggestive that a physical activity intervention integrated into the workplace via work processes and/or structured exercise is supportive in reducing anthropometric and body composition measurements, while changing body mass, to increase health and reduce obesity-related chronic disease risks in sedentary women.
Background
Healthy People 2030 targets the occupational health and safety of U.S. workers with an objective to increase the proportion of workplaces that offer a physical activity program as part of an employee health promotion program through prevention and early intervention (Office of Disease Prevention and Health Promotion, U.S. Department of Health and Human Services, n.d.). The sedentary aspects of work have been associated with increased health risks. Sedentary behavior is described as any awake activity in a sitting or a reclining posture equivalent to an energy expenditure <1.5 metabolic equivalents (MET), with resting expenditure, equal to 1 MET (Liguori, 2021). Interventions to reduce sedentary time and increase active time during the workday have been investigated with promising results (Bailey, 2021). Female nurses who represent the largest professional group of healthcare workers, have high levels of sedentary behavior (50%–60% of the day), placing them at risk of obesity-related chronic diseases (Reed & Prince, 2018). A web-based, cross-sectional, self-reported survey among nurses indicated >55% were obese/overweight with ~80% reported as sedentary (≥ 3 hours/week sitting), and not engaged in any type of physical activity (Ross et al., 2019). Workplace physical activity interventions that can address high amounts of sedentary behavior and low levels of physical activity are important in combating obesity and chronic disease risks, yet few interventions have targeted nurses (Reed & Prince, 2018).
The rates of obesity across the world continue to expand at an alarming pace with nearly one third of the world population either overweight or obese (Chooi et al., 2019). Obesity is understood as an energy imbalance, due to an overconsumption of calories and/or a lack of daily physical activity and a serious health threat that predisposes one to increased risks of cardiovascular diseases, metabolic diseases, and other detrimental pathologies (Chooi et al., 2019; Office of Disease Prevention and Health Promotion, U.S. Department of Health and Human Services, n.d., Piercy et al., 2018). Therefore, it is necessary to curb excessive weight gain and associated comorbidities. Despite the continued emphasis on the health benefits of regular physical activity necessary to reduce chronic disease, less than 30% of adults engage in sufficient levels of physical activity (Liguori, 2021; Piercy et al., 2018). Many factors influence physical activity levels and for women with primary barriers; lack of time and social support (Peng et al., 2023).
Traditional aerobic exercise, such as walking or moderate intensity continuous training, has been supported for overweight and obese women. Evidence has included increased aerobic capacity, weight loss, and weight management, along with reductions in obesity-related risk factors (Batrakoulis et al., 2018; Cebrick-Grossman & Payne, 2016; Grossman et al., 2018). Moderate intensity continuous training yielded weight loss and improvements in body composition when volumes were >150 minutes/week, with comparable results for high intensity circuit training, ≤100 minutes/week (Boutcher et al., 2019; Keating et al., 2017). However, greater attrition and lower compliance rates have been associated with high weekly exercise volumes, perhaps, since many women find it difficult during the workday to exercise and to initiate and maintain the level of aerobic activity necessary for weight control and cardiovascular health, with exercise “volume” defined as the product of frequency, intensity, and time of exercise (Liguori, 2021). Carving out for impactful outcomes presents challenges in the workplace, and employers may allow only minimal time during the workday to support such programs (Wasfy & Baggish, 2016).
Growing evidence indicates that high-intensity interval training or more commonly known as “HIIT,” might effectively replace traditional moderate intensity continuous training, resulting in similar or even better physiological outcomes with a far less time commitment, for example, 10 minutes, 5 times/week as compared with 30 minutes of traditional activity (walking) 5 times/week (Grossman et al., 2018). A physical activity program of shorter duration is beneficial for individuals with time consuming schedules and HIIT interventions have shown promise to achieve increased health benefits in less time (Metcalfe et al., 2020). A HIIT intervention exercise program for normal body weight, overweight, and obese women resulted in reductions in metabolic profile, anthropometric measurements, subcutaneous and intra-abdominal fat, body composition, and obesity-related diseases (Frimpong et al., 2019). In addition, reductions in body mass and fat mass, relative (%) body fat, waist and hip circumference measurements were observed after 40 weeks of a circuit-type training in overweight, obese females (Batrakoulis et al., 2018). Even more impressive, a workplace HIIT intervention with just two bouts/week of <9 minutes/session, a practical alternative to moderate intensity continuous training for time-constrained populations, demonstrated an increase in maximal aerobic capacity (VO2max) (Metcalfe et al., 2020). The nature of HIIT incorporates resistance training, and if done consistently, recommended twice a week (Liguori, 2021) an increase in lean muscle mass and a reduction in fat mass, may result, which are notable body composition changes necessary for weight control, as lean muscle mass is more metabolically active than fat mass (Bellicha et al., 2021). In addition, excess fat mass increases mortality risk, while increased lean mass and fat-free mass decreases mortality risk. (Liguori, 2021), a crucial point in reducing obesity-related chronic disease risk. HIIT is both time efficient and effective in reducing fat mass by inducing similar metabolic adaptations, as seen with moderate intensity continuous training (Dupuit et al., 2020). Consequently, when time is limited, a shorter duration, physical activity intervention with a resistance training component is ideal for workplace occupational programs, to improve employee health and reduce obesity-related chronic disease risks.
Additional evidence also demonstrates the role of social influences on weight control, particularly the benefits of social support from group-based physical activity programs. The ability to keep participants engaged and connected to one another during an intervention, may prevent attrition, and promote adherence. Thus, physical activity interventions in the workplace may be enhanced by the influence of co-worker social support on behavior change, of which only a few studies have assessed (Fetherman & Cebrick-Grossman, 2024; Payne et al., 2018; van der Put & Ellwardt, 2022). An occupational health promotion program that incorporates social support to enhance adherence and compliance simply makes sense.
Wearable technology, also known as accelerometers, fitness trackers and/or wearables are wrist worn devices used to track body movements and encourage physical activity. According to a survey conducted by the American College of Sports Medicine (ACSM, 2019), of more than 3,000 fitness professionals, wearable technology was identified as the top fitness trend in 2020. Evidence has supported the incorporation of wearable technology within physical activity intervention programs to increase adhere and compliance (Barkley et al., 2019; Grossman et al., 2018; Newton et al., 2023). A recent review highlighted the importance of promoting physical activity via wearable technology in clinical practice for patients, although did not address those delivering the care, the nurses and healthcare workers (Carter & Ford, 2023). The incorporation of activity monitors with behavioral strategies for sedentary workers have indicated promising results, with few such studies specific to nurses (Oreskovic et al., 2023).
Comprehensive workplace occupational programs that are health-focused and employee-centered have the potential to positively impact workers’ health and quality of life and are ideal for impacting health behaviors (Fetherman et al., 2020; Madden et al., 2020; Metcalfe et al., 2020). This study incorporated an occupational physical activity intervention in the workplace to reduce sitting, and change anthropometric, body mass and body composition to reduce obesity-related chronic disease risks and increase overall health. There is limited research specific to workplace physical activity interventions and health risk reductions for obese, sedentary females. This study fills a gap in the literature as it focused on increasing physical activity via wearable technology while reducing sedentary behaviors in the workplace.
Methods
Overview
This intervention research study compared the effects of HIIT and increased steps (walking) on anthropometric, body mass, and body composition changes over a 12-week period in sedentary, obese females. The study was based within a community-based participatory research approach, a partnership between university faculty and a multifaceted, nonprofit, community healthcare and social assistance provider. The workplace administration and wellness committee, of whom one faculty researcher was a member, approved the study design with the physical activity interventions incorporated into the employees’ workday. Approval was obtained from the workplace administration/wellness committee and the university institutional review board (IRB) for human subject research. The project was based on organizational policies and procedures, employee job requirements, work break schedules, and the availability of workplace facilities. The study was publicized at the workplace via print flyers and electronic newsletters, designed to increase physical activity among female employees. Interested individuals were invited to attend orientation sessions with convenient dates and times for employees at the workplace, during which the informed consent form was completed.
Study Population
Participant eligibility was confirmed through self-reported demographic information, followed by the completion of a physical activity readiness questionnaire (PAR-Q) that screened all prospective participants for specific medical concerns related to increased physical activity (Thomas et al., 1992). Additional study criteria study included: an “obese” body mass index (BMI) between 30.0 and 35.9 kg/m2 (Liguori, 2021), a sedentary lifestyle with no structured exercise outside of activities of daily living (with the ability to engage in exercise), nonsmoker, fluency in English, and no self-reported medical concerns. Ineligible criteria included having lost >10% of one’s body weight within the preceding 6 months of the study, enrollment in any structured weight loss programs such as Weight WatchersTM and any form of gastric or bariatric surgery.
Forty women were screened, 13 met the study criteria, one withdrew due to hospitalization for a kidney stone. The PAR-Q identified four participants as hypertensive, and a physician medical release was required prior to participation, per industry standards (Liguori, 2021). A convenience sample of twelve, voluntary, sedentary, obese (BMI = 32.98 ± 3.21 kg/m2), adult (46.10 ± 9.56 years) female employees (nurses, nursing assistants, and administrative office workers), completed the study, a purposeful sample size for this community-based participatory/translational research study. To ensure confidentiality, each subject was assigned a number for identification, and was randomly assigned into the HIIT group or the STEP group.
Study Design
A pretest, posttest, randomized experimental design compared female employees of a HIIT group (n = 5) against those who increased their daily steps, through walking, the STEP group (n = 7). Both interventions took place during the workday over a 12-week period, consistent with exercise program guidelines to allow for intervention impact (Liguori, 2021). Participants’ total body movements and steps were tracked via wearable technology, a valid, low-cost, wrist worn activity monitor/accelerometer, a Movband™ (DHS Group, Houston, TX; Newton et al., 2023), provided to each participant at the outset of the study. Participants were instructed on the use of the wearable technology, by the second author, which included the frequency, intensity, type, time, and progression of exercise. The participants were directed to wear the device only while at work, to track and self-monitor total body movements and steps, as the purpose of this study was to increase physical activity and reduce sedentary behaviors in the workplace. Activities of daily living were to remain unchanged, and any additional physical activity outside of the workplace was discouraged, so not to confound the study results. Participants’ compliance and retention were monitored through the Movband™, which the research team had access to view and download all activity. At the outset of each week (Sunday evening), a reminder smartphone text message was sent to each participant from a faculty partner (student research assistant), regarding upcoming weekly physical activity goals. Upon conclusion of the study, participants were given the accelerometer to keep as their own.
Procedures
The HIIT group participants (n = 5), were encouraged to exercise with at least one other co-worker, at the workplace, which was dependent upon employee break and lunch times. Each exercise session was 15 minutes in length which included, a 5-minute warm-up, followed by 10 minutes of exercise, guided by the DVD exercise program, the “10-minute Trainer”™ (Beachbody, 2013). This commercially based DVD exercise program was selected for several reasons; convenience at the workplace, reasonably priced (<$100), with exercises rooted in empirical evidence (Liguori, 2021). In addition, this DVD program was used in similar studies with promising results (Cebrick-Grossman & Payne, 2016; Fetherman & Cebrick-Grossman, 2024; Grossman et al., 2018). The exercise videos included eight different routines: upper and lower extremity, two cardio segments, two total body, yoga, and abdominal exercises (Beachbody, 2013). Throughout the study period, HIIT intervention group participants were instructed to complete five of the eight different exercises/week, in no specific order, with the eight sessions completed within eight workdays, after which the rotation of the exercises was repeated. Baseline moves for the HIIT group were tracked, the week prior to the study. The progression of the HIIT intervention began with 3 days of exercise for Weeks 1 to 3, 4 days for Weeks 4 to 6, and 5 days for Weeks 7 to 12.
STEP group participants (n = 7), incorporated steps (walking) into their day, via work processes and/or during break or lunch times. Baseline steps for the STEP group were determined the week prior to the intervention start, as participants were instructed to track their daily steps, without any increase. Participants were then guided to independently increase their steps as part of their typical workday to 2,500 steps above baseline for Weeks 1 to 3; to 5,000 steps, 4 days/week for Weeks 4 to 6; and between 7,500 and 10,000 steps, 5 days/week for Weeks 7 to 12. The progression of both HIIT and STEP interventions were based upon American College of Sports Medicine guidelines (Ligouri, 2021).
Data Collection
Basic demographic information, participant criteria determination, PAR-Q questionnaire, and informed consents were obtained immediately after the completion of the orientation sessions by the primary and secondary authors, in a private, onsite workplace location. Anthropometric, body mass, and body composition measurements were completed in a university body composition laboratory by the first author and principal investigator, an exercise physiologist and registered dietitian/nutritionist. Anthropometric measurements included body weight (mass) and height (for BMI calculation) and five circumference measures (in inches): waist, abdomen, hips, biceps, and thigh, with the latter two measured on the right side of the body to maintain universal consistency (Ligouri, 2021). These measurements occurred at baseline (Week 0), mid-program (Week 6) to support study compliance, and at the end-program assessment (Week 12). The total inches lost per participant was determined from the reduction or differences in the girth measurement from the baseline measures (Week 0) to the end-program (Week 12) measures. Body composition measurements were performed by the principal investigator, certified, and trained in DEXA scan procedures (General Electric, Madison, Wisconsin), and included relative (%) body fat, fat mass, fat-free mass, and lean mass. Seated blood pressure measurements were assessed at baseline (Week 0) by the principal investigator with a standard sphygmomanometer and stethoscope to confirm a normotensive state for overall participant health, not a study criterion. Four participants identified as hypertensive from the PAR-Q, all of whom had been prescribed anti-hypertensive medication, prior to the start of the study. The principal investigator verbally provided participants with an explanation of their anthropometric, body mass, and body composition measures at baseline (Week 0) and mid-program (Week 6), and upon completion of the end-program assessment (Week 12), all participants received a written comprehensive report of their program results.
Data Analysis
Descriptive and inferential statistical analyses of the data were examined using SPSS Statistics (Version 24). Dependent sample t-tests determined pretest and posttest statistical significance of anthropometric outcome measures for the full sample (N = 12), along with the intervention groups HIIT (n = 5) and STEP (n = 7) (Table 1). Dependent sample t-tests determined pretest and posttest statistical significance of body composition outcome measures among the HIIT group (n = 5), with no statistical differences among the STEP group (n = 7) (Table 2). Independent sample t-tests and multivariate analysis of variance (ANOVA) probed for differences between groups, with no statistical differences. Regression analyses examined Movband™ data, using Pearson’s correlation coefficient (r = 1.0), i.e., total body moves and steps tracked from both groups, were correlated to miles, for ease of understanding (Table 3).
Anthropometric Measures, Change in Key Outcomes
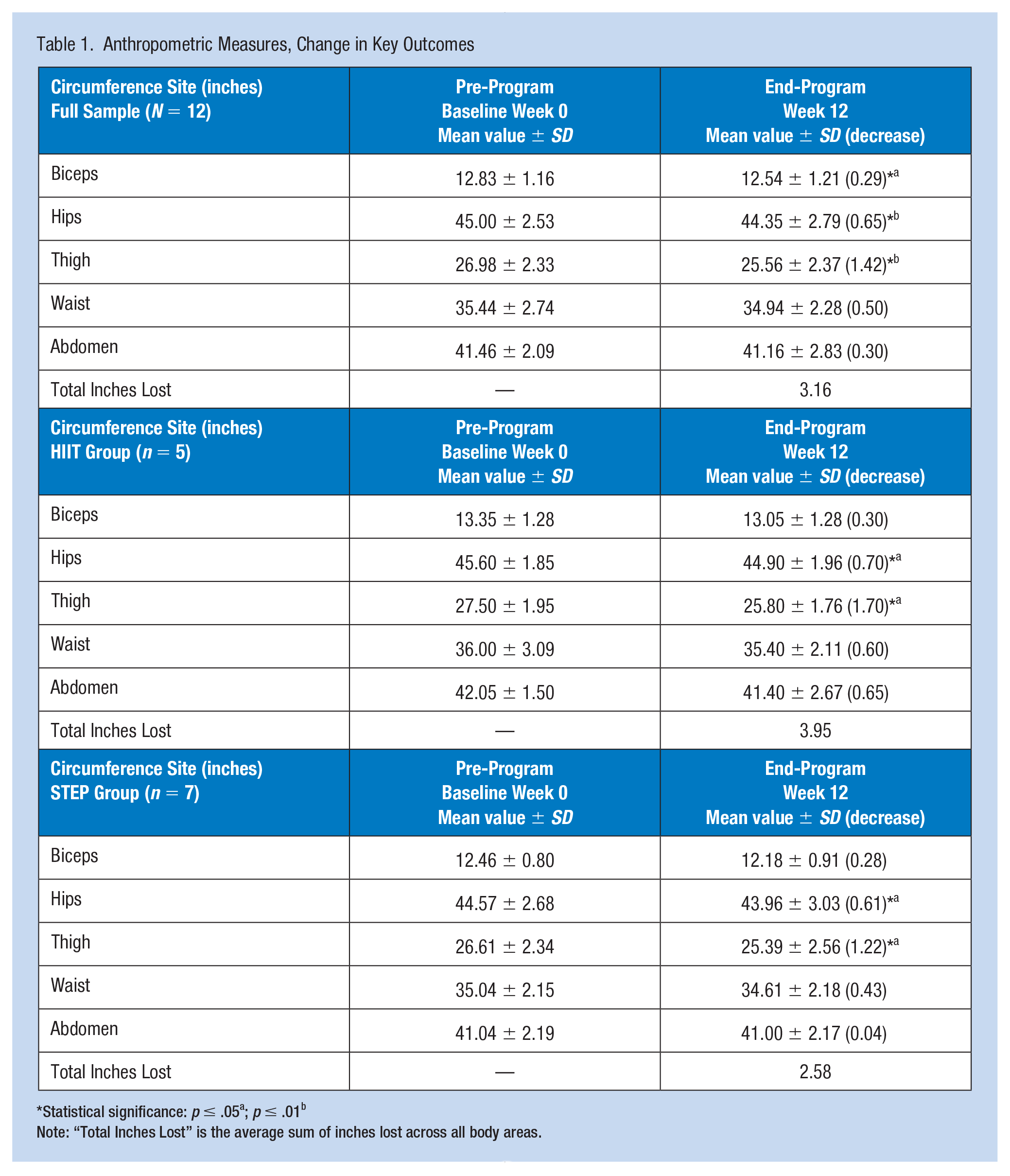
Statistical significance: p ≤ .05a; p ≤ .01b
Note: “Total Inches Lost” is the average sum of inches lost across all body areas.
Body Composition Measures, Change in Key Outcomes by Intervention
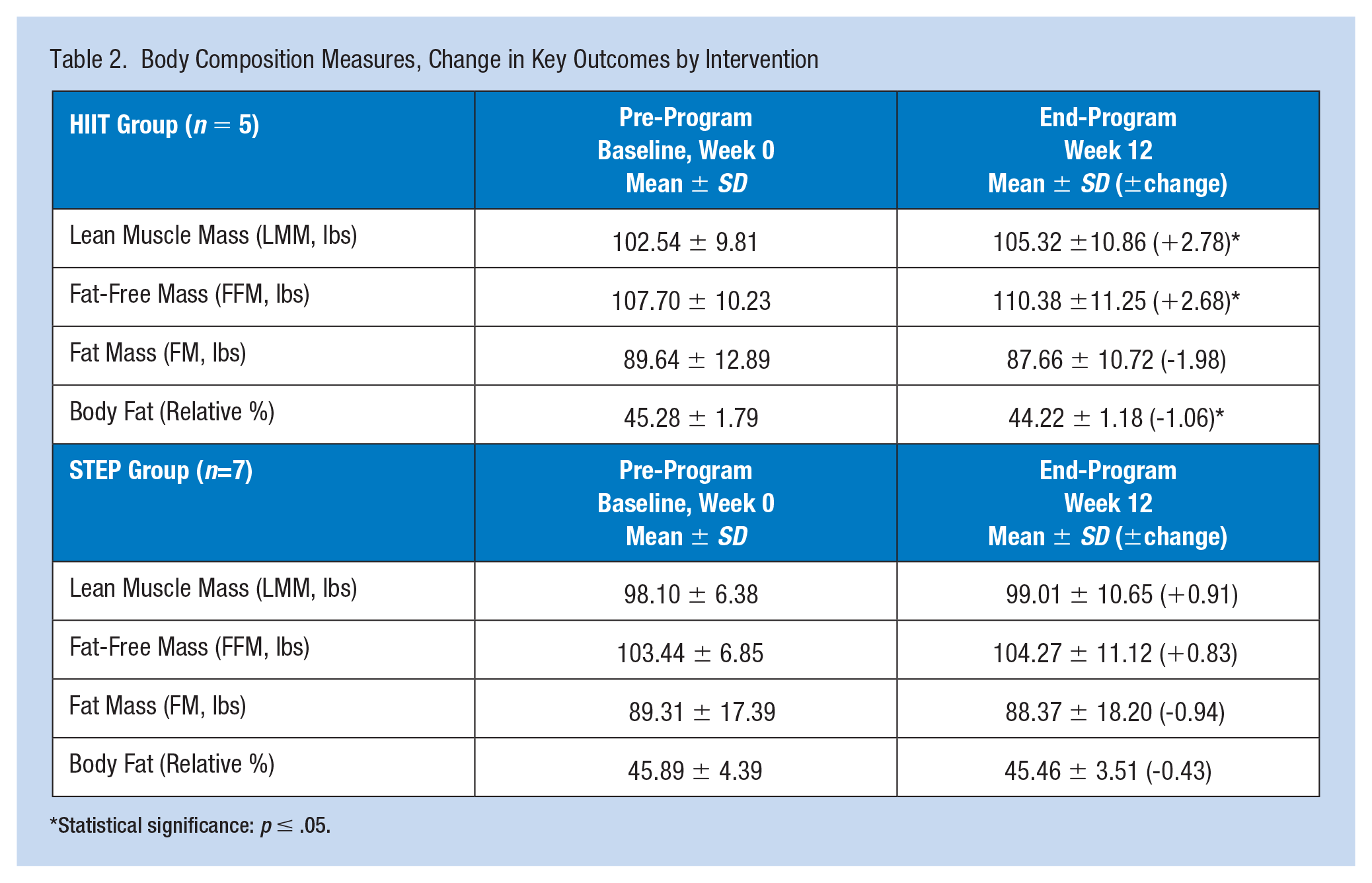
Statistical significance: p ≤ .05.
Pre- and Post-Program Intervention Changes
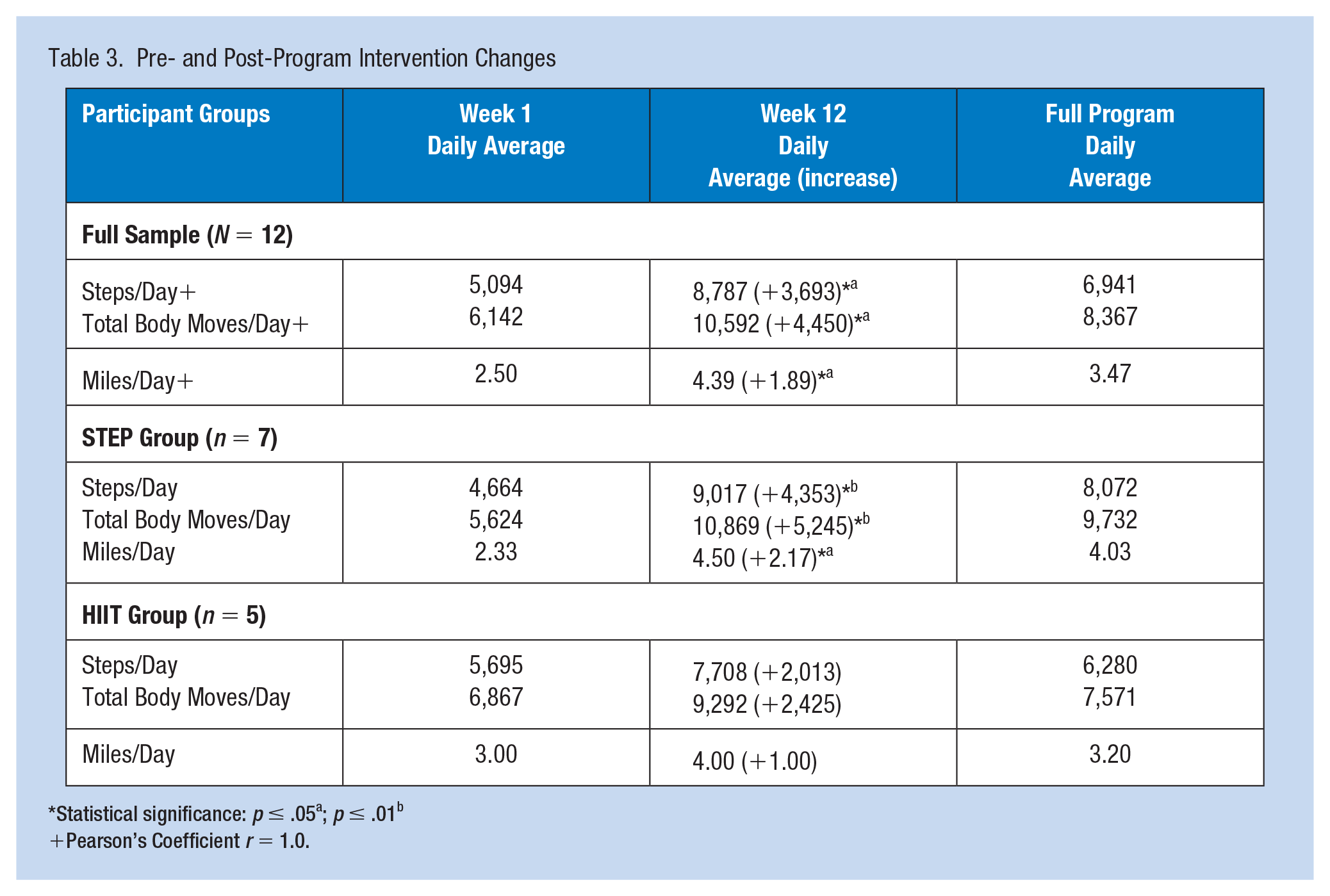
Statistical significance: p ≤ .05a; p ≤ .01b
Pearson’s Coefficient r = 1.0.
Results
Dependent sample t-tests determined statistical significance for pretest and posttest anthropometric outcome measures among participants with reductions in biceps (p ≤ .05), hips and thigh measurements (p ≤ .01), for the full sample (N = 12), along with reductions in hips and thigh measurements (p ≤ .05), within both groups STEP (n = 7) and HIIT (n = 5) (Table 1). Additional dependent sample t-tests for pretest and posttest body composition outcome measures, determined statistical significance among the HIIT group (n = 5), with increased fat-free mass, and lean mass (p ≤ .05), and reduced relative (%) body fat (Table 2). Independent sample t-tests and multivariate ANOVA probed for differences between groups (STEP and HIIT) with no significant differences determined, likely due to small sample sizes.
The Movband™ accelerometer data for each participant was downloaded and examined via regression analyses. Pearson’s correlation coefficient (r = 1.0) correlated total body moves and steps to miles, a recognizable value, for both groups (STEP and HIIT). Statistical significance (p ≤ .05) was determined for pretest and posttest, dependent sample t-tests with increases in steps/day, total body moves/day, and miles/day for the full sample (N = 12) (Table 3). Statistical significance was determined for the STEP group (n = 7), with increases in posttest: steps/day, total body moves/day (p ≤ .01), and miles/day (p ≤ .05), with no significant difference among the HIIT group (n = 5) (Table 3).
Discussion
This study demonstrated a practical approach to incorporate an occupational, physical activity intervention, health promotion program, into the workday for sedentary workers. Increased physical activity tracked over a 12-week period in obese, sedentary females, resulted in significant reductions in anthropometric outcome measures: biceps (p ≤ .05), hips, and thigh (p < .01), measurements, for the full sample (N = 12), along with significant reductions in hips and thigh (p ≤ .05) measurements within both groups, STEP (n = 7) and HIIT (n = 5) (Table 1). In addition, body composition outcome measures displayed significant increases in fat-free mass and lean mass along with significant reductions in relative (%) body fat, in the HIIT group (n = 5) (Table 2). The body composition data for the STEP group (n = 7), although not statistically different, had had pre–post changes supportive of improved health (Table 2). These results are quite promising, considering the small group sample sizes. Such a change in body composition, that is, a reduction in relative (%) body fat along with an increase in fat-free mass and lean mass, is key to weight control. Fat-free mass consists of all body components except fat. Lean mass has a small amount of essential fat from the bone marrow and internal organs and is more metabolically active than fat mass (Bellicha et al., 2021). For example, lean mass such as skeletal muscle mass burns ~13 kcals/kg per day for muscle and ~5 kcals/kg per day for fat with ~80% of the difference in energy expenditure explained by body composition, and the remainder, due to genetics, age, and gender (DeNino, 2022). A workplace health promotion intervention program that increases energy expenditure through increased physical activity, along with an incorporated resistance training component, should be encouraged to change body composition, i.e., a reduction in relative (%) body fat and fat mass, while increasing fat-free mass, and lean mass, in favor of improved health and reduced obesity-related chronic disease risks.
The wearable technology (Movband™) created a level of accountability (both self and co-worker social support) necessary for subject compliance and retention, observed with significant increases (p ≤ .05) in steps/day, total body moves/day, and miles/day for the full sample (N = 12), and significant increases within the STEP group (n = 7), for steps/day, total body moves/day (p ≤ .01), and for miles/day (p ≤ .05) (Table 3). Increased physical activity through increased walking (tracked steps or miles) into the workday is a practical intervention to reduce sedentary behaviors for most everyone in comparison to a HIIT intervention which required dedicated time carved out of the workday, in addition to the use of a DVD. It would benefit employers to encourage increased physical activity via increased steps, total body moves, and miles each day to reduce sedentary behaviors. This study fills a gap in the literature as the healthcare industry has a greater prevalence of obesity, with limited such studies, specific to wearable technology and physical activity interventions for improved health (Carter & Ford, 2023; Ito-Masui et al., 2021). Such a health promotion program is valuable to both the employee and the employer, not only with improved health behaviors among workers but also with increased employee morale and work performance (Grimani et al., 2019).
The primary limitation of this work was the small group sample size (N = 12) that restricted statistical significance between groups, STEP (n = 7) and HIIT (n = 5). Future work with larger group sizes and longer interventions could investigate, the intersect between HIIT, increased steps, caloric intake, energy expenditure, while tracking steps and total body movements during both the workday and outside of work to positively impact health. Overall, this work provides promise for the implementation of a workplace intervention to improve health and reduce obesity-related chronic disease risk by incorporating physical activity into the workday in obese, sedentary, female workers.
Applications to Professional Practice
This community-based participatory research partnership between the workplace and academia is a unique approach to develop, implement, and evaluate health promotion programs. This study provides a framework for reducing sedentary behavior and increasing physical activity to impact change in anthropometric, body mass, and body composition measures. Increased physical activity, via increased steps integrated into the work routine with a simple message of “move more, sit less,” is a practical way to impact health. In addition, as evidenced in this work, the incorporation of a resistance training component as part of the physical activity intervention could have a greater impact on health via body mass changes, reductions in fat mass and increases in fat-free mass and lean mass, normalizing body weight. Finally, the integration of wearable technology provides a level of accountability (self and co-worker) that can enhance retention and compliance to change behavior and further enhance increased physical activity and support health promotion practices in the workplace.
Footnotes
Conflict of Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Author Contributions
Dr. J.A.C.-G. along with Dr. D.L.F. conceptualized and designed the study and together worked with the community-based partner. Dr. J.A.C.-G. completed all the statistical analyses and data interpretation and wrote the intellectual content. Dr. D.L.F. completed the document review and editing.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Human Subjects Review
The University of Scranton [985650-1]—Full Committee Review
CITI Certification
Completion Date 13-Apr-2021
Expiration Date 12-Apr-2024
Record ID 30596333
Author Biographies
Dr. Joan A. Cebrick-Grossman is an Associate Professor and Registered Dietitian/Nutritionist in the Department of Health and Human Performance at The University of Scranton, Scranton, PA.
Dr. Debra L. Fetherman is an Associate Professor and Health Promotion Program Director in the Department of Health and Human Performance at The University of Scranton, Scranton, PA.