
Abstract
A workplace physical activity (PA) study tested a novel use of peers to deliver the intervention. Peer models provided vicarious experience for living physically active lifestyles to a group of inactive women. The purpose of this study was to describe participants’ perceptions of the peer modeling intervention. Nine women from the intervention group (n = 26) participated in a 90-minute focus group. Qualitative description using thematic analysis was used to identify themes from the focus group transcript. Two themes about the intervention were “I am left wanting more” and “focus on food.” Two themes about the peer models were “real people” and “it is doable.” Focus group participants perceived the peer modeling PA intervention favorably; however, they desired more attention to healthy eating and more time with peer models. Replication of the study accounting for themes identified by focus group participants is needed to strengthen the peer modeling intervention.
Work, marriage, and children are common life experiences in adulthood associated with physical inactivity (Bellows-Riecken & Rhodes, 2008; Tudor-Locke, Leonardi, Johnson, & Katzmarzyk, 2011). Working women in the United States are an at-risk group for inactivity, with fewer than 26% meeting guidelines for healthy physical activity (PA; Blackwell & Clarke, 2016), which is 150 minutes of moderate-level aerobic activity and 2 days of strengthening activities per week (PA Guidelines Advisory Committee, 2008). One strategy to improve health behaviors, including PA, is the use of peers. Across health behavior research, peers have been used to provide education, social support, behavior norms, advocacy, and to increase self-efficacy (Simoni, Franks, Lehavot, & Yard, 2011). How peers are defined and used in interventions varies widely and few studies offer a theoretical explanation for the peer effect (Simoni et al., 2011).
Peers as a Strategy to Improve PA Behavior in the Workplace
The workplace has been a useful setting to address PA behavior using a variety of strategies. Significant improvement in PA behavior and/or cardiorespiratory fitness has been found with interventions using electronic calendar (Pressler et al., 2010) or email (Andersen et al., 2013; Plotnikoff, McCargar, Wilson, & Loucaides, 2005) prompts to be active. Web-based PA self-monitoring with activity tracker and tailored advice (Sternfeld et al., 2009) has also been an effective strategy used in the workplace. Interventions providing individual or group PA behavior counseling (Atlantis, Chow, Kirby, & Fiatarone Singh, 2006; Purath, Michaels Miller, McCabe, & Wilbur, 2004; Ribeiro, Martins, & Carvalho, 2014) and/or supervised PA training (Barene, Krustrup, Jackman, Brekke, & Holtermann, 2014; Dalager, Justesen, Murray, Boyle, & Sjøgaard, 2016; Gram, Holtermann, Søgaard, & Sjøgaard, 2012) have also been effective in the workplace. Several workplace PA interventions have been found to use peers to provide informational support and to organize and/or lead PA activities (Campbell et al., 2002; Gazmararian, Elon, Newsome, Schild, & Jacobson, 2013; McEachan et al., 2011). However, the effect of peers as the central intervention strategy remains unclear. In a recent experimental workplace PA study using both quantitative and qualitative methods, peers provided intervention group participants with vicarious experience for living a physically active lifestyle (Rowland et al., 2018). It was hypothesized that active peer role models from the workplace would serve as a target of comparison for living an active lifestyle and facilitate an increase in PA behavior among a group of inactive women. The intervention was based on social cognitive theory (self-efficacy; Bandura, 1998) and social comparison theory (self-improvement based on comparison with others; Festinger, 1954). Prior research has identified a relationship between social comparison thinking and health behavior. In adolescents and young adults exposed to “healthy” role models, greater levels of comparison thinking were related to greater engagement in health behaviors like teenage pregnancy avoidance, healthier food choices, and increased PA (Luszczynska, Gibbons, Piko, & Tekozel, 2004; Tigges, 2001).
Purpose
The purpose of this study was to describe participants’ perceptions of a 12-week, novel, peer modeling intervention to increase PA behavior among a group of inactive working women. Details about the intervention study are reported elsewhere (Rowland et al., 2018). In brief, the intervention was conducted using an experimental, two-group (intervention and attention control), randomized, repeated-measures (baseline and 12-weeks) study design. The primary outcome of the workplace peer modeling PA intervention study was cardiorespiratory fitness and secondary outcomes were PA behavior, lifetime cardiovascular risk, self-efficacy, motivation, and social comparison for PA behavior. Following the 12-week workplace PA intervention, a focus group was held to determine participants’ perceptions of the peer modeling intervention and how it did or did not help with PA behavior change.
Study Methods
A qualitative approach was used with a postintervention focus group to obtain participants’ perceptions of the workplace PA intervention, the peer models, and PA behavior change.
Sample and Setting
All 26 participants from the intervention group were invited to a one-time focus group following the intervention study. Nine participants attended the focus group; all nine attendees had completed all aspects of the intervention. The only inclusion criterion for the focus group was assignment to the intervention arm of the workplace peer modeling PA study. No exclusion criteria for participation in the focus group were used. Inclusion criteria used for the intervention study were female employee between 19 and 65 years of age, worked ⩾20 hours/week, and self-reported ⩽60 minutes moderate or ⩽20 minutes vigorous PA per week. Exclusion criteria used for the intervention study were greater than moderate cardiovascular risk (Arena, Pescatello, Riebe, & Thompson, 2014), body mass index (BMI) ⩾ 45 kg/m2, unable to complete cycle fitness testing, pregnancy, night shift worker, active participation in a weight management or exercise program, and treatment with a beta-blocker medication. The study was conducted at a Midwestern health system employing approximately 3,500 people, 80% of whom were female.
Peer Modeling Intervention
To deliver the intervention, physically active women (peer models) were recruited from the workplace study site, a Midwestern health system. Twenty-two women who self-reported engaging in at least 150 minutes of moderate-level PA per week were interviewed about their PA history. Seven women differing in age, occupation, and PA experiences were selected to share their story of living an active life with the intervention group in a lunch and learn format. The active peer models were oriented to the study, completed Collaborative Institutional Training Initiative (CITI) training, and created their own 20-minute PowerPoint presentation describing and depicting their life as a physically active woman. Each presentation followed the same format: personal demographics (family status, job, hobbies), PA level as a young person, turning point for becoming more active (if applicable), barriers, facilitators (goal-setting and self-monitoring) motivation for PA, and technology or tools used for PA. The presentations averaged 12 slides in length and contained approximately 20 images of themselves, their families, PA activities, technology used, and motivating quotes or images. The peer models presented their story and took questions from intervention group participants in a 45-minute lunch and learn format. Each session also included 10 to 15 minutes on the health benefits of PA. The six lunch and learn sessions were held every other week for 12 weeks. Each session featured a different peer model except for the last session, when two peer models presented their PA story. In addition to the peer model sessions, intervention group participants (a) received their fitness test results, (b) received an exercise prescription for 150 minutes of moderate-level PA/week based on a calculated target heart rate and a rating of perceived exertion of 12 to 15, and (c) were asked to submit a weekly PA log.
Data Collection
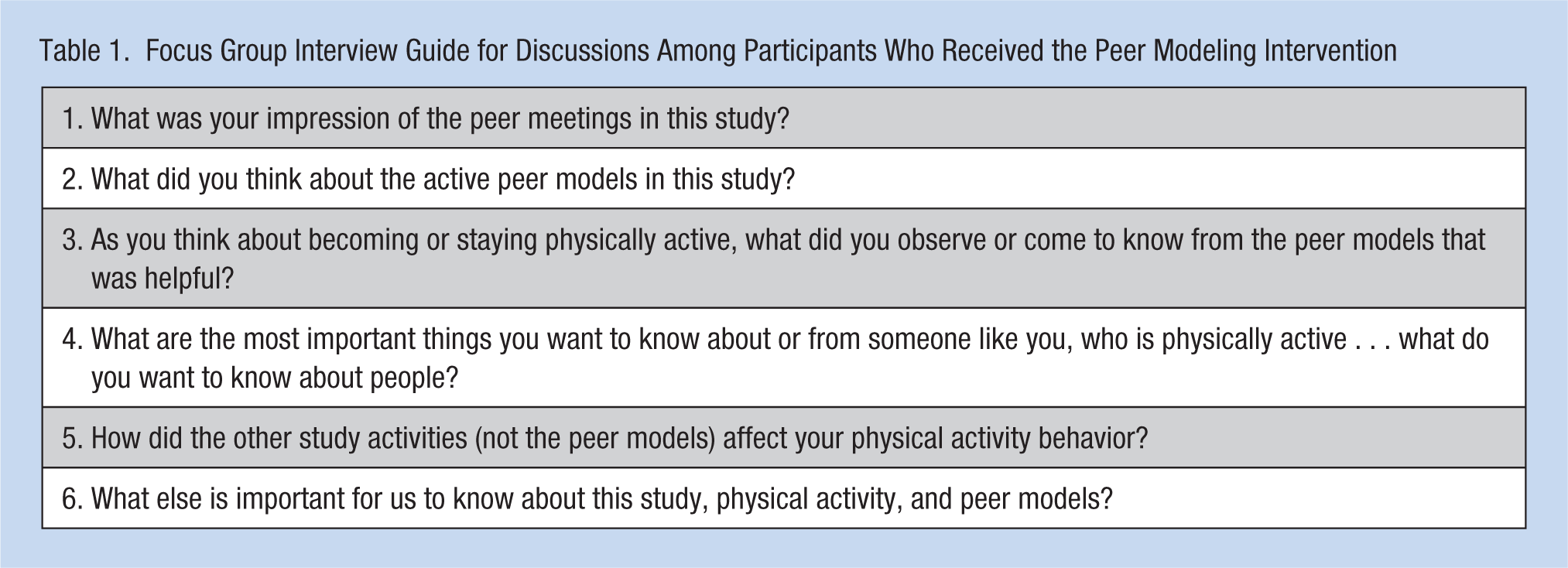
A 90-minute audio-recorded focus group was held in a private conference room at the study workplace site 1 week after the intervention ended. Consistent with Krueger (1997) recommendations, two individuals conducted the focus group. The principal investigator (PI) led the session guided by an a priori interview guide (Table 1). Questions for the interview were established using guidelines on developing questions for focus groups (Krueger, 1997). A PhD student served as assistant moderator by taking notes during the session. To stimulate recall, focus group participants were provided a handout featuring a picture of each of the seven peer models with their name, age, and work position indicated.
Focus Group Interview Guide for Discussions Among Participants Who Received the Peer Modeling Intervention
Procedures
The study was approved by the study site and the university’s institutional review board. Informed consent was obtained prior to enrolling participants into the study. Following postintervention study measures, all intervention group participants were invited to a focus group at the study site to discuss the intervention.
Analysis
The focus group discussion was audio-recorded and transcribed verbatim. The PI reviewed the transcript for accuracy. Analysis of the focus group transcript followed Braun and Clarke’s (2006) method of thematic analysis. Transcripts were read by two investigators multiple times before they conducted a line by line review to code significant statements. Codes were then organized according to themes and were reviewed and discussed by interdisciplinary team members until consensus was reached.
Results
Nine intervention group participants attended the focus group and were mostly Caucasian, married/partnered, and worked full-time; six were employees with sedentary work duties. Those attending were older (M years = 47.4 ± 10.0) than the entire intervention group (M years = 43.5 ± 12.4). The focus group participants were also more engaged with the intervention relative to the overall intervention group participation. For example, the focus group participants submitted more PA logs (focus group M = 10.0 ± 1.7; intervention group M = 8.3 ± 1.5) and attended more sessions (focus group M = 5.0 ± 0.8; intervention group M = 4.2 ± 1.5). Four themes emerged from the qualitative analysis: (a) I am left wanting more, (b) focus on food, (c) real people, and (d) it is doable.
Themes
I am left wanting more
In general, focus group participants indicated they “liked” and were “motivated” by most aspects of the study. Regarding the intervention format, two themes emerged: “I am left wanting more” and “focus on food.” Participants expressed an interest and enjoyment in both the method of intervention delivery (lunch and learn sessions, informational content, peer model presentations, activity logs) and the peer models themselves. However, they desired more meetings, continued accountability with activity logs, additional health information, more time with peer models, and more opportunities to support each other. Remarks that illustrate “I am left wanting more” include “I was sad that it ended at the 12 weeks. . . I just felt like a lot of us were getting comfortable with being active,” “I would have liked to be accountable for longer periods doing the logs and stuff, even if we didn’t have the every other week thing,” and finally “I kinda feel like, where do I go from here?”
Participants in the focus group also wanted more support for measuring heart rate beyond the manual method they were taught when they received their exercise prescription. Most focus group participants did not have an activity tracker and some had difficulty taking their own pulse. Some experimented with other methods of tracking heart rate (pulse ox, phone app) and others bought themselves an activity tracker. One participant remarked,
At first I didn’t have a monitor at all, I just used the flash on the back of my phone, like we heard in the class, that helped. Then I got that app, and that helped. But then I was like, this is kind of annoying, cause I’d have to turn my phone on, get the app up, and if my phone died [giggling], it was disaster. Then I ended up getting a Fitbit®, and now I’m obsessed with it.
The theme “I am left wanting more” was evident in the focus group discussions about support for making PA behavior change. Peer models were identified as a potential source of “wellness coaching,” a “mentor,” someone with whom to meet, exercise, and walk at lunch. Two fellow participants exercised together and met with a peer model on their own, outside of the intervention, to learn about strength exercises. Several suggested assigning participants to a “buddy” to be more accountable and supported for PA.
Focus on food
The second major theme from the focus group session was “focus on food.” In this PA study, participants were neither encouraged or discouraged from making dietary improvements. Nutritional content during the intervention was limited to brief comments made by some of the peer models as context for their healthy lifestyles. Although diet was not a focus of the intervention study, within the focus group, discussion repeatedly turned to food and the challenges of maintaining a healthy diet. Participants “compared notes,” and exchanged information, opinions, and experiences on eating and preparing healthy food as individuals and families. Much discussion centered on being “scared” and “intimidated” by healthy food they did not know how to prepare such as couscous, quinoa, and vegetables. While participants in the intervention group were not directed to change eating behavior, many focus group participants reported doing so by monitoring or limiting calories and/or carbohydrates, substituting fruit for chips, cooking more at home, and subscribing to a mail-order fresh food service.
Participants often paired the topics of diet and exercise when commenting on the challenges of healthy behaviors: “it’s still the struggle of just getting it all together, that I can get in that groove and feel like I’m making progress on the exercise and the eating part of it.” Much discussion focused on the need for more nutritional information during the study. For example,
I was hoping for more on food choices, like fast, healthy choice meals. I mean there were some people who talked about food and how they coped with, like, their husband and them not eating similar meals. It would have been nice to know some, like quick recipes.
Another remarked,
It would be nice if that [the intervention] actually had the wellness coach or group like this, where you had the physical, but then you also had the diet and nutrition part of it with it, because then, you get the best of both worlds.
Real people
In general, focus group participants “really, really liked” the peer models and the “good stories” that they shared. They “liked that they weren’t professionals” and were “just average people.” Participants remarked “it was a great combination of people at different life stages, dealing with different things,” “it was really good mix, their age, what they do for work, something about their personal life, and then their journey,” and “they all had a different story, something to connect with.” However, not every peer model appealed to every focus group participant. Some found one peer model to be “energizing” and “motivating,” while others found the same peer model “intimidating in her energy level and the fitness level that she’s at.”
Many comments focused on the realness of the peer model through seeing them and the images they used to tell their stories. One participant said,
I think the PowerPoint, everything was really good, being able to see it. You know their busy lifestyles, what works out for them, I believe [peer model] showed us the video of her dancing with her daughter, and I thought that was really nice.
Another participant stated,
I really liked the speakers. You know I was able to get a lot out of just seeing their life, their own success story, and just knowing that are just busy, busy people and even busier than me and they are able to do it. And then, I should be able to do it.
One participant remarked on seeing a peer model’s before and after pictures using resistance bands, “the pictures were like wow, you know, just using resistance bands. And she had those [resistance bands] to pass around which I thought was really nice also.” Another participant commented,
They were real people, and it’s not like they were walking around with this obsessive kind of approach to it you know. It was just, regular, average daily changes in things. They weren’t going to the gym five days a week for two hours per day, or so fit now that they looked like that’s all they did.
The focus group participants found the peer models to be “real” through hearing about their struggles and turning points in their lives. For example, one participant remarked, “I appreciated how honest they were, like struggling with depression, and then you know someone else talked about their families and then their other issues, their husband, and their kids, and so I thought that was real helpful.” Another participant remarked, “their struggles and hang-ups are the same as what my struggle is—kids, work, time, energy, whichever.” The experiences of peer models were perceived as real as one participant said,
That’s the thing of what was nice about them being, you know, the people that are here [at the workplace] and the fact that they’re not someone who has been on the Biggest Loser or one of those things where, you know, it wasn’t reality and it wasn’t that they had, you know, three months solitary, where that is all they did.
One of the peer models was noted to be nervous giving her presentation, and a focus group participant commented, “that [her nervousness] just makes it more real, I mean they are us.”
It is doable
Participants in the focus group accepted the peer models as models for living an active lifestyle. One participant said, “it can be done, . . . a lot of times what keeps you from working out is you think, I just can’t work it in, I can’t put the time in. . .and they [peer models] modeled that you can.” Not all strategies used by the peer models appealed to every participant. However, even if focus group participants were not “into running” or “Zumba,” they were accepting that some of the strategies used by the peer models to be active were “doable.” One participant remarked,
I think one of the greater things that I feel I walked away with was that it doesn’t have to be, you know, 30 minutes at a gym, doing this or that. It can be, you know, many different things, it’s just that movement out of the chair, off the couch. You know, I think that’s what I got out of it, that it doesn’t have to be you know, an hour of Zumba five days a week.
Some focus group participants described the changes they made based on strategies used by the peer models such as pacing while waiting for the elevator, standing or walking while watching the news, and taking the stairs. One participant described,
You learn a little bit of something from everyone and it pushes you and [peer model] really got me going just because of her energy. And it’s like, ok, yeah, if I’m making popcorn I can do the exercise while I’m waiting for it. Simple things like that you don’t think about or like when you are watching a show you can do sit-ups. I mean you can do that.
Other support for the theme “it is doable” was found in the focus group participants’ desire to have more details about peer models’ strategies. A “tips and hints” handout was requested with information about the exact web address and/or name of the application the peer models were using with PA. Discussion time and peer model “shadowing” were also suggested to get more detailed information about healthy PA strategies the peer models were using.
Discussion
This peer modeling intervention introduced vicarious experience, a less understood strategy for increasing PA behavior. It is uncommon in health behavior research or clinical practice to facilitate behavior change by directing attention to someone else who is successful with a health behavior. To learn vicariously is to make comparisons between yourself and someone else. Negative effects may result from deliberate comparative thinking; it may create anxiety, jealousy, and lower self-esteem. Therefore, it was important to find out what the intervention group participants thought of this strategy as few studies have reported participants’ perceptions of peers used in PA interventions (Simoni et al., 2011).
In general, perceptions of the peer modeling intervention and the peer models themselves suggest the intervention format was useful to the focus group participants. While not all focus group participants found all peer models appealing, the focus group participants were able to articulate what they did or did not like about the peer models. The theme “I am left wanting more” indicates an opportunity to expand the intervention by increasing time and interaction with the peer models as suggested by participants. Focus group participants wanted more time with peer models for “chit-chat,” “shadowing grocery shopping and working out,” “support,” and endorsements of foods, products, or activities the peer models used to be active. Several suggested weekly peer model meetings and/or extending the study longer to get more from the intervention. These comments affirm that the intervention provided a positive vicarious experience for living an active lifestyle.
An interesting finding relating to the intervention format is the theme “focus on food.” During intervention sessions and across focus group interview questions, participants migrated toward the topic of healthy eating with peer models and/or with each other. Several explanations may exist for this. Perhaps food is simply more interesting to talk about then PA. Alternatively, addressing diet and PA behavior together is a natural tendency because they are often paired in recommendations to be healthy. Also, several were motivated to participate in a PA study for weight-loss. It may also be that peer models were regarded as experts in health behavior; seeking endorsements of products or methods of food preparation were ways in which participants were learning vicariously through the peer models. For participants, incorporating more information and support to improve their diet would have expanded the intervention to deliver “the best of both worlds.”
In addition to the comments about the intervention format, the themes identified in this study align with the theoretical variables in the intervention study. The two themes “real people” and “it is doable” address the concern for this intervention study regarding comparison thinking, and whether intervention group participants would identify with or compare themselves with the peer models. Vicarious experience and social comparison theory explain that similarity identification (recognition of shared attributes) is needed for the information gained from a model to be relevant enough to support behavior change (Bandura, 1998; Festinger, 1954). In this study, peer models and their PA experiences (running 5 km and half-marathons, kick boxing, and Zumba classes) could have been regarded by participants as too dissimilar, even off-putting. Comments by focus group participants suggest that even though they may have not had interest in PA activities like running half-marathons, they gained valuable information and “motivation” from the peer models. Motivation from seeing others exercise was also found in a recent qualitative study using focus group exploration of why and how peers trained as workplace “health champions” influenced PA behavior among fellow employees (Edmunds & Clow, 2016).
In this study, within the theme of “I’m left wanting more,” focus group participants described the peer models and their experiences as “motivating” and feeling “really motivated to do more” even though they were not asked specifically about motivation. Focus group participants also described situations where they lacked confidence (self-efficacy) for PA or healthy eating. Participants reported being “scared” or “intimidated” by activities such as using weight equipment and distance running and “healthy” food they have never tried or prepared before like quinoa. By desiring more time with peer models to “chit-chat” and shadow during exercise and grocery shopping, focus group participants may have been using vicarious experience to alleviate apprehension to engage in certain activities or try healthy foods with which they lacked experience.
Statements of social comparison were also made: “I liked the fact that [peer model] and I did the same job” and “I just saw some similarities in my story as far as clothes not fitting, and using it is as a motivator.” Many of these statements about similarity supported the theme of “it is doable.” Two other studies using focus group qualitative methods to evaluate a PA intervention also identified themes related to finding similarity with others (Learmonth, Marshall-McKenna, Paul, Mattison, & Miller, 2013; Luoma et al., 2014). Learmonth et al. (2013) used group exercise with multiple sclerosis patients and Luoma et al. (2014) used group exercise with breast cancer survivors. In both studies, focus group participants commented on the importance of shared experiences or “being in the same boat” as others who are working to increase PA. It may be that PA interventions with a social component to the intervention have more success if similarities like age, job, family status, diagnosis, life experiences, and experiences with PA are known by participants.
There are limitations to the findings of this focus group inquiry. First, the focus group participants were a subsample of the intervention participants who responded to an invitation to discuss the intervention in a focus group format. Therefore, not all intervention participant views were reflected in this thematic analysis. The focus group participants were slightly older and more engaged (more PA logs submitted; more sessions attended) with the intervention than those intervention participants who did not participate in the focus group. As the intervention group participants with low-level participation in the intervention did not attend the focus group, their perceptions of the peer modeling intervention may differ and were not represented. Another limitation was having the PI lead the focus group. Knowing the PI, who is an advanced practice nurse working at the study site, and that the study was a dissertation project may have influenced participants to be either overly complimentary or less critical than if an unknown person led the focus group.
Despite the limitations of this qualitative inquiry, the themes identified begin to reveal what participants perceive during a novel peer modeling intervention to improve PA behavior. Activating comparison thought processes by using peer models appeared to have a positive and motivating effect on focus group participants. In fact, the bulk of feedback from participants suggests the opposite; they found the peer models to be “real people” who demonstrated PA “is doable,” and participants were “left wanting more.” In future research using peer models in PA interventions, including nutritional content may be useful; this was a prominent theme in this study. Finally, when using peer models in PA interventions, researchers may want to include “comparison content,” that is, information about the peer model that allows participants to find points of similarity and sources of motivation.
Footnotes
Conflict of Interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Author Biographies
Sheri A. Rowland is an assistant professor at the University of Nebraska Medical Center College of Nursing. Sheri is an early career nurse researcher with interest in the social influences on physical activity behavior in women.
Marlene Z. Cohen is a professor at the University of Nebraska Medical Center College of Nursing. Marlene has been an NIH funded researcher investigating the patient experience for health promotion and disease prevention. Marlene is currently a nurse researcher at the VA Nebraska-Western Iowa Healthcare System.
Carol H. Pullen is a professor in the College of Nursing at the University of Nebraska Medical Center. Carol has been awarded three RO1 NIH grants for her research on promoting healthy eating and physical activity behaviors in midlife and older rural women.
Paula S. Schulz is an associate professor at the University of Nebraska Medical Center College of Nursing. Paula is an NIH funded nurse researcher with experience and interest in cardiovascular risk reduction in cardiac patients and their spouses.
Kris E. Berg is Professor Emeritus and former Director of the Clinical Exercise Physiology Lab at the University of Nebraska Omaha. Kris has several decades of experience in design of exercise programs and fitness assessment, particularly among persons with chronic health conditions.
Bernice C. Yates is a Professor Emeritus at the University of Nebraska Medical Center College of Nursing. Bernice has been funded by the NIH to study couple-focused interventions to assist cardiac patients and spouses with the adoption and maintenance of health behaviors.