
Abstract
This study investigated the potential relationship between shiftwork and work-related physical assault (PA) against nurses who are at high risk of violence globally. Nurses (6,300), randomly selected from the licensing database and working in Minnesota, were surveyed regarding PA experiences. Through a nested case-control study, nurses who reported a PA in the previous 12 months and controls who were randomly selected from their assault-free working months, respectively, identified exposures experienced during the month prior to the assault month (cases) and the random non-PA months (controls). Comparing case and control exposures, shiftwork was examined relevant to PA. Among 310 cases and 946 controls, most worked 8 hours or less (87%, 88%) during day shifts (44%, 70%). Multivariable analyses (odds ratios [ORs] and 95% confidence intervals [CIs]) revealed increased risk of PA for nurses working evening (OR = 1.55, 95% CI = [1.05, 2.27]), night (OR = 3.54, 95% CI = [2.31, 5.44]), and rotating day and evening (OR = 2.88, 95% CI = [1.22, 6.80]) shifts, which provides a basis for intervention opportunities.
Work-related violence, including physical assaults (PAs) and nonphysical violence (NPV; for example, threats, sexual harassment, verbal abuse), has been identified as a major public health problem (Gerberich et al., 2004; Peek-Asa, Schaffer, Kraus, & Howard, 1998; Rosenberg & Fenley, 1991). During 2012, work-related violence in the United States was the second leading cause of occupational fatality (U.S. Department of Labor, Bureau of Labor Statistics [USDOL, BLS], 2012); in 2014, it was the third leading cause (16%) after transportation-related causes (40%) and falls (17%; USDOL, BLS, 2014). Although much is known about work-related homicides, research on nonfatal violent events and relevant risk factors is limited, particularly those events and risk factors related to shiftwork. In a recent publication, based on the National Crime Victimization Survey and the Census of Fatal Occupational Injuries, approximately 572,000 nonfatal violent crimes, rape, robbery, or assault were estimated to have been perpetrated against individuals aged 16 years or older while they were at work or on duty in 2009 (Harrell, 2011). Based on Workers’ Compensation data, it was reported that nighttime work shifts were associated with greater risk of assault for health care workers (Islam, Edla, Mujuru, Doyle, & Ducatman, 2003); however, detailed analysis by type and length of shift was not examined.
Hospital and health care workers are at increased risk for violence, especially nonfatal violence (National Institute for Occupational Safety and Health [NIOSH], 2002; Peek-Asa, Howard, Vargas, & Kraus, 1997; Phillips, 2016). Violence against nurses is a major occupational health problem (Arnetz, Arnetz, & Soderman, 1998; Baxter, Hafher, & Holme, 1992; Carter, 1999; Gerberich et al., 2004; Mahoney, 1991; Phillips, 2016). In 2014, 80% of nurses reported being attacked on the job within the past year; this accounted for 70% of all reported industry nonfatal violence-related injuries with lost workdays (Jacobson, 2014). Exploring and understanding factors that put employees at risk for violence is a critical step toward the development of effective interventions.
The purpose of the study was to identify how shiftwork affects work-related violence using a nested case-control study. Such analysis may provide guidance for interventions to reduce the risk of such violence.
Method
Physical assault was defined as being hit, slapped, kicked, pushed, choked, grabbed, sexually assaulted, or otherwise subjected to physical contact intended to injure or harm. Violence was work-related if it occurred in the work environment or during any activities associated with work, including travel. This definition is consistent with the definition used by NIOSH (1996).
Study Population
The study population included all registered nurses (RNs) and licensed practical nurses (LPNs) working in the state of Minnesota at the time of study data collection. Based on licensing requirements for both RNs and LPNs who practice in the state, an established database provides demographic data and contact information (e.g., home addresses). Nurses who reported working in Minnesota during the 12 months prior to survey completion were included in the sample (Gerberich et al., 2004).
Study Design
The study consisted of two phases. Phase 1 was designed to estimate the frequency and consequences of work-related violence and identify potential risk factors; Phase 2 used a case-control approach (http://www.strobe-statement.org) to investigate the association between exposures and PA outcomes. Phase 2 data provided the basis for the current investigation and analysis.
Following approval by the University of Minnesota Institutional Review Board (9602S10794), 6,300 nurses from the population (n = 79,128) of currently active RNs (n = 57,388) and LPNs (n = 21,740), licensed in the state of Minnesota as of October 1, 1998, were randomly sampled. The state database included name, license type, address, birthdate, sex, and year of first licensure. Up to four mailings were completed to maximize response rates for both the Phase 1 initial study and the Phase 2 nested case-control study. These mailings included specially designed and pretested survey instruments pertinent to work-related violence and associated exposures, along with a letter inviting participation, informed consent form, and a postage-paid return envelope (“Minnesota Nurses’ Study,” 2016).
The Phase 1 survey was mailed to the entire sample of 6,300 nurses to determine employment status and the incidence and consequences of work-related violence. From this phase, a response rate of 78% (4,918) was realized (80%, RNs; 74%, LPNs). Adjusting for the eligible fraction of the entire sample had little effect on the response rate (Gerberich et al., 2004).
Based on the responses, 475 cases (i.e., those who reported at least one PA event during the previous 12 months) were identified; 1,425 control participants were randomly selected in a 3:1 ratio to cases from among those who reported no PA. Cases were also eligible to be selected as controls during the months prior to their first assault. For the Phase 2 questionnaire, case participants were asked about exposures experienced during the month prior to their assault months; if multiple events were reported, case participants were surveyed about experiences the month before the earliest event. Each selected control nurse was randomly assigned an exposure month during the study period in which nurses indicated if they worked, but before any reported PA occurred to them. This selection process ensured the distribution of months worked among cases and controls was well represented by the distribution of selected exposure months.
Data Analyses
The goal of data analyses in this study was to explore the possible association between shiftwork and PA against nurses in Minnesota, controlling for confounding factors. Shiftwork was classified by shift type (day, evening, night, day and evening, day and night, others) and shift length (≤8, 10, and ≥12 hours), to examine the association between those categories and PA. Based on a priori hypotheses (Gerberich et al., 2005), a directed acyclic graph (DAG; Figure 1) was constructed to represent the potential causal relationships between shift type and shift length, PA, and other variables included in the data collection instrument. Using the principles described by Greenland, Pearl, and Robins (1999) and Maldonado and Greenland (2002), and illustrated by Hernan, Hernandez-Diaz, Werler, and Mitchell (2002), the DAG was used to determine which variables should be included as possible confounders when examining the role of shiftwork in episodes of PA. The set of confounders was the minimum required to block all potentially confounding relationships between shiftwork (exposure of interest) and PA (outcome). These confounders included facility in which participants worked most of the time, primary population with which participants worked, primary professional activities, license type, age, gender, and work tenure. A potential source of bias was avoided by excluding those variables in the causal pathway between shiftwork and PA.
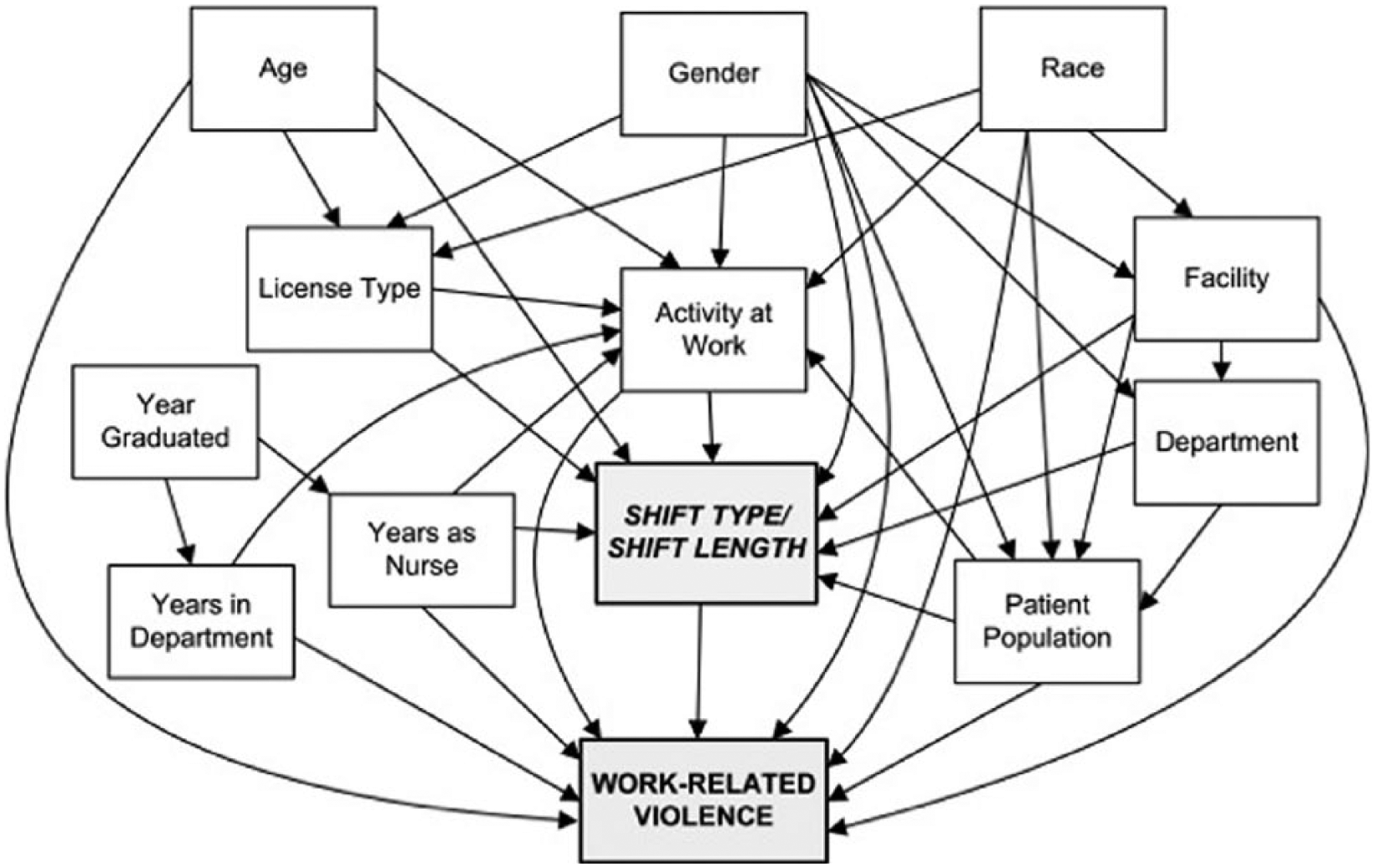
Directed acyclic graph, based on causal model, to select confounders for multiple logistic regression analyses of work-related violence.
Descriptive frequencies were calculated for the main exposures of interest, shift type, and shift length, among cases and controls, as well as for other variables identified as potential confounders in the causal model. Multivariable logistic regression models were used to determine the statistical association between shiftwork and PA; univariate models were included to demonstrate the differences in the effect size (odds ratios [ORs]) when potential confounders were not included. All statistical analyses were performed using SAS 9.3 (SAS, 2011).
Results
From respondents to the Phase 2 case-control questionnaire (324 cases [68%] and 946 controls [66%]), only those cases that involved patient- or client-initiated assaults (310 cases) were included because they comprised the majority of PAs (96%). Table 1 presents the characteristics of the study participants. Among these participants, most were women (96%). On average, participants were 46 years of age (±SD, 10.1); 73% were RNs and 27% were LPNs. Case and control participants were similar in shift length. However, cases were more likely to work evening shifts, night shifts, and day and night rotations. As shown in Table 1, cases—compared with controls—more frequently worked in long-term or assisted care departments—with a geriatric primary patient population—and provided patient care.
Demographic and Occupational Characteristics of Cases and Controls in a Population-Based Study of Licensed Nurses
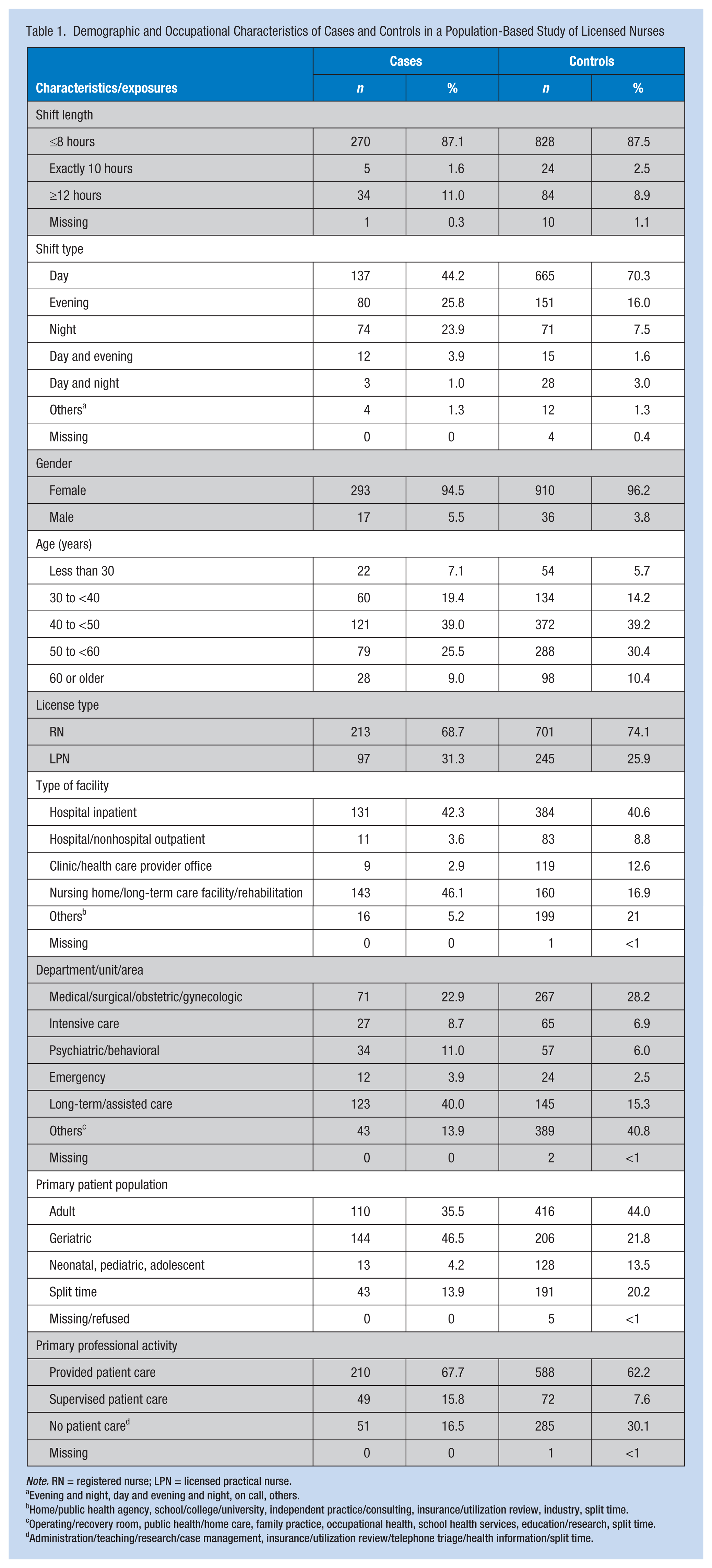
Note. RN = registered nurse; LPN = licensed practical nurse.
Evening and night, day and evening and night, on call, others.
Home/public health agency, school/college/university, independent practice/consulting, insurance/utilization review, industry, split time.
Operating/recovery room, public health/home care, family practice, occupational health, school health services, education/research, split time.
Administration/teaching/research/case management, insurance/utilization review/telephone triage/health information/split time.
Although not shown, through a subanalyses of cases and controls combined, differences in frequencies of environmental factors and patient characteristics were found among shift types; for example, nurses working evening or night shifts (39%, 77%, respectively), compared with day shifts (16%), were more likely to report dim or soft versus bright lighting. Nurses working evening or night shifts more frequently reported higher percentages (44%, 41%, respectively) of impaired patients (e.g., under the influence of disease, prescribed medication, alcohol, or other drugs), compared with day shift nurses (26%).
Table 2 provides risk estimates at both levels of unadjusted and adjusted multivariable analyses. Even though the effect sizes were smaller in the adjusted compared with the unadjusted models, the effect of shift type remained statistically significant after adjusting for potential confounders. Nurses at greatest risk of assault were those working in the following shifts: evening (OR = 1.55, 95% confidence interval [CI] = [1.05, 2.27]), night (OR = 3.54, 95% CI = [2.31, 5.44]), and rotating day and evening (OR = 2.88, 95% CI = [1.22, 6.80]). Length of shift was not significant in this analysis.
Univariate and Multivariable Analyses of the Relation Between Shift and Physical Assault Against Licensed Nurses
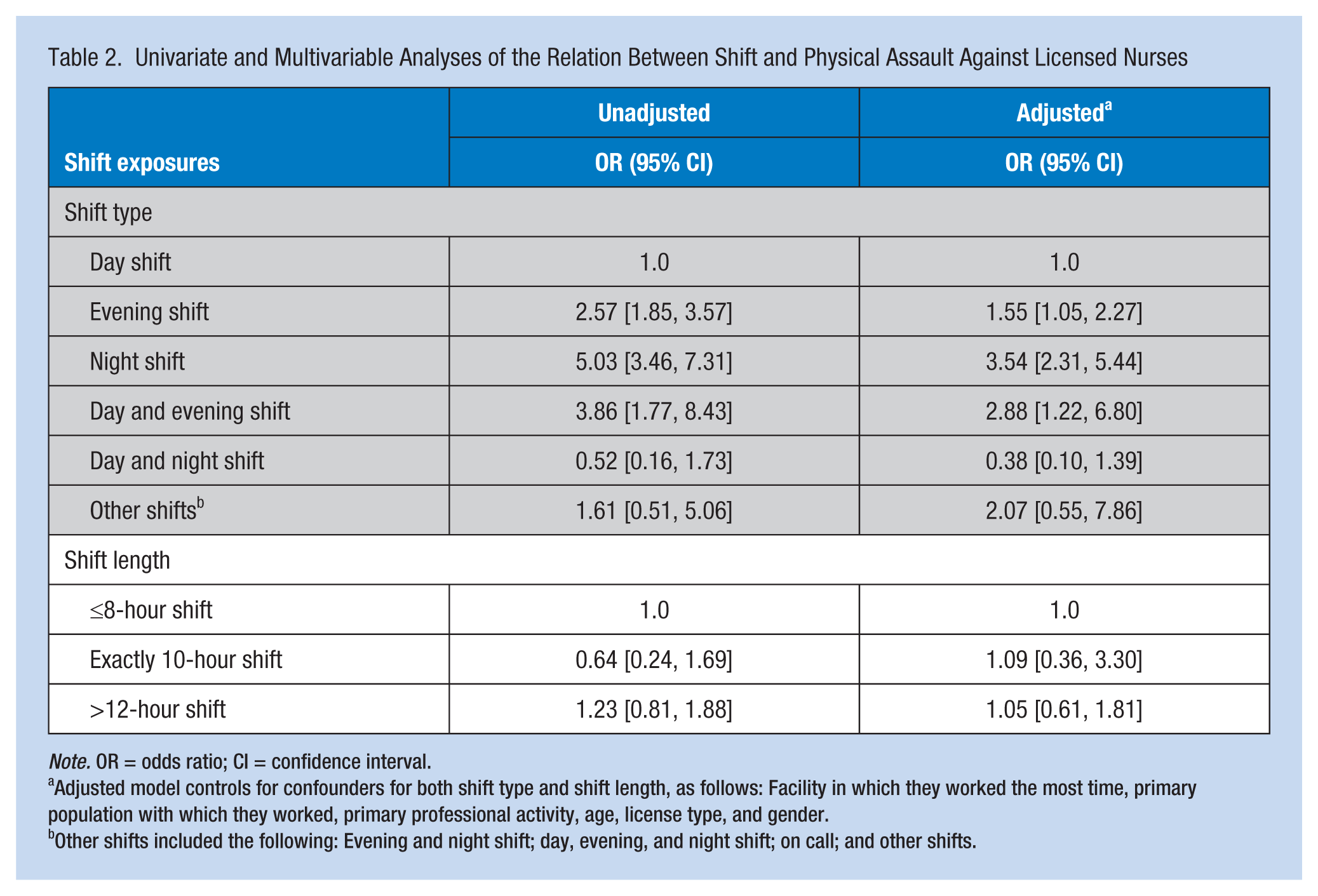
Note. OR = odds ratio; CI = confidence interval.
Adjusted model controls for confounders for both shift type and shift length, as follows: Facility in which they worked the most time, primary population with which they worked, primary professional activity, age, license type, and gender.
Other shifts included the following: Evening and night shift; day, evening, and night shift; on call; and other shifts.
Discussion
The purpose of this effort was to study the effect of shift on PAs among nurses through a comprehensive case-control analysis not previously conducted, either on this major database (Gerberich et al., 2005; Gerberich et al., 2004) or in previous studies that examined potential risk factors for occupational violence. Through logistic regression analysis, increased risks of work-related violence were identified among nurses who worked evening, night, and rotating day and evening shifts. Although substantial variations were found in other studies of workplace violence impacting nurses because these studies used various methods, including diverse populations, and varying study periods and definitions, similarities in study results were also identified. The European Nurses’ Early Exit (NEXT) cross-sectional and longitudinal study (Estryn-Behar et al., 2008) identified increased risk of PA during night versus day shifts (OR = 2.17, 95% CI = [1.76, 2.67]). Through a cross-sectional study conducted by Abbas, Fiala, Rahman, and Fahim (2010), increased risk (OR = 1.6, p = .002) was reported for nurses working night versus day shifts. From a 2005 three-month cross-sectional national telephone survey of Canadian nurses (Shields & Wilkins, 2009), respective risks (ORs, 95% CIs) for working evening, night, and mixed versus day shifts were as follows: OR = 1.4, 95% CI = [1.2, 1.8]; OR = 1.3, 95% CI = [1.1, 1.6]; and OR = 1.5, 95% CI = [1.3, 1.8]. More recently, a cross-sectional study of violence against nurses in Chinese hospitals (Jiao et al., 2015) identified a risk of 3.7 times greater for those who worked rotating versus fixed day shifts. These increased risks of assault might be explained, in part, by low staffing and diminished lighting; the risk of assault among nurses working in environments that were not fully illuminated was higher than for brighter settings (Gerberich et al., 2005), similar to findings identified in an intervention study on a different population by Loomis, Marshall, Wolf, Runyan, and Butts (2002). In addition, the finding of higher percentages of impaired patients (Gerberich et al., 2004) cared for on these shifts is suggestive. The relationship between impairment and assault was recently reported by Hahn et al. (2010).
Limitations
Potential limitations of the present study include the data collection method for both the exposures and outcome, which was based on self-report. However, this bias was minimized by limiting the recall of violent events during Phase 1 data collection to the previous 12 months (Gerberich et al., 2004) and the recall of exposures in the case-control study to a 1-month period within the preceding year (Gerberich et al., 2005) comparable with approaches used in previous studies (Gabel & Gerberich, 2002; Gerberich et al., 2002; Lee, Gerberich, Waller, Anderson, & McGovern, 1999). In addition, the nurses were contacted, as necessary, to clarify ambiguous or missing information for the purpose of further minimizing bias (Gerberich et al., 2005; Gerberich et al., 2004). Also, validation substudies of environmental exposures and health care treatment were conducted (Gerberich et al., 2002).
Implications for Practice
Although this study focused on a specific population of nurses, violence and shiftwork are global problems in health care (Abbas et al., 2010; Estryn-Behar et al., 2008; Jiao et al., 2015; Shields & Wilkins, 2009). In the United States, in 2013, 23,000 significant injuries were reported due to occupational assault, with 70% of these assaults occurring in health care and social service settings (Occupational Safety and Health Administration [OSHA], 2015). The American Nurses Association (ANA; 2016) notes that no federal standard requires workplace violence protections; however, some states have enacted legislative solutions including mandatory comprehensive prevention programs for health care employers and substantial penalties for those individuals convicted of assaulting a nurse or other health care personnel (ANA, 2016).
The 2014 projections of deficits in health care workers in the U.S. and global health care industries were 2.2 and 7.2 million workers, respectively; by 2035, these deficits are projected at 3.9 and 12.9 million workers, respectively (Campbell et al., 2013). Given these projected shortages in the U.S. and global health workforces, it is imperative that health care workers’ safety be a priority throughout the health care industry.
An ideal comprehensive approach to the mitigation of work-related violence and injury, including attention to shiftwork, is through application of the Total Worker Health™ approach (NIOSH, 2016). This approach includes policies, programs, and practices that integrate protection from work-related hazards with promotion of injury and illness prevention efforts to advance worker well-being (NIOSH, 2016). Elaboration on this approach is displayed in Figure 2. Given the findings from this study, the need for baseline and ongoing record-keeping that enables analysis of trends and rates of violent events, both physical and nonphysical (verbal abuse, threats, harassment, and bullying), as well as injuries in general, is essential. In particular, frequent institutional assessment and evaluation of factors, that may mitigate risk, including attention to relevant safety and health training, the shifts worked, availability of coworkers and emergency assistance, and environmental conditions, including appropriate lighting, protective barriers, alarm systems, and personal cell phones, among others (Gerberich et al., 2005; OSHA, 2015), is fundamental to protecting workers. Integral to the success of this approach are management commitment, leadership including employee involvement, and the provision of relevant resources by management to ensure mitigation of injury and violent events; these events may vary by individual institution and work location (Figure 2). This model and information is further reinforced by Wyatt, Anderson-Drevs, and Van Male (2016) who emphasized that “leaders have a duty to their employees to institute programs and ensure adherence to policies requiring all reported events be taken seriously, assessed appropriately, and managed individually and ethically” (p. 1037).
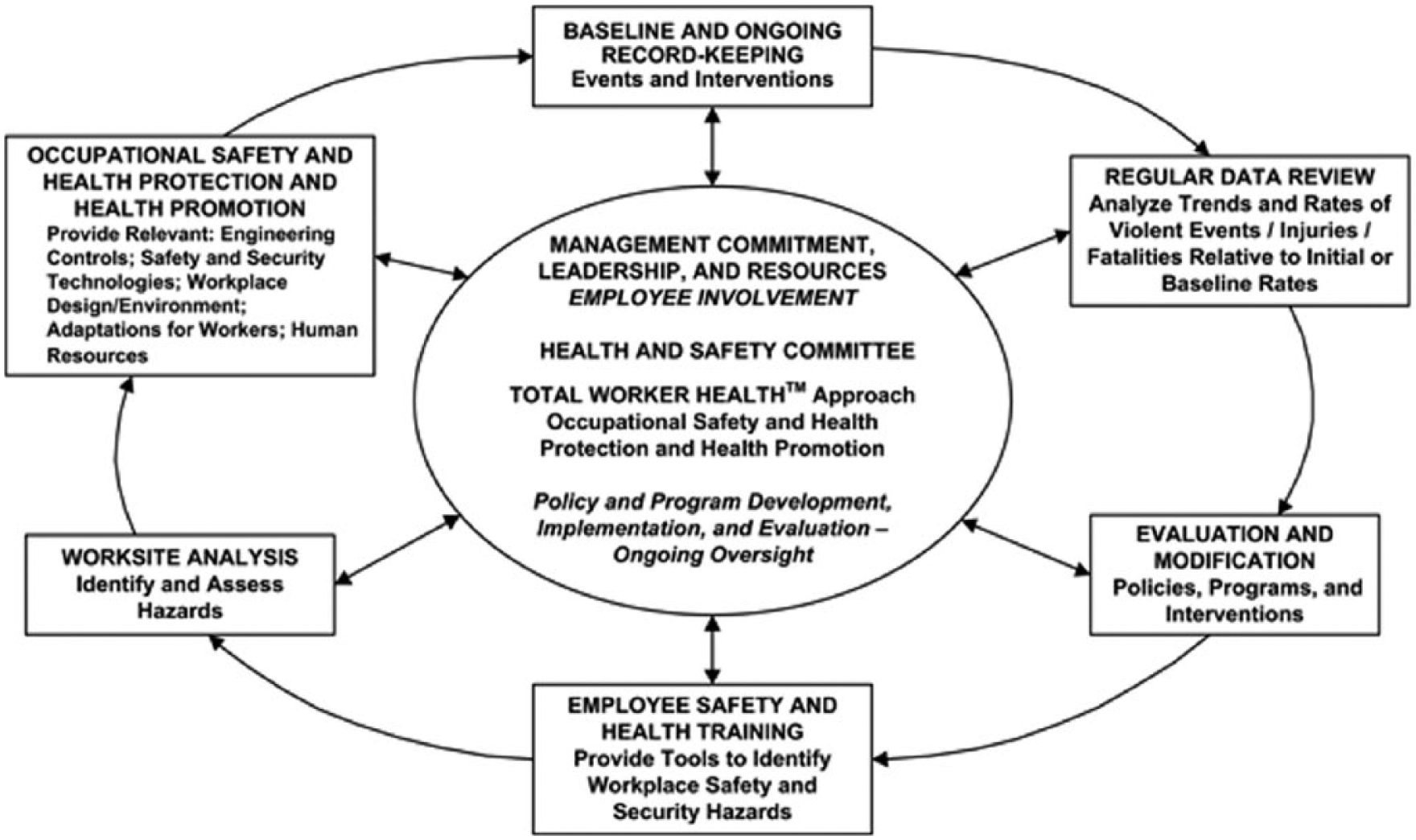
Prevention through a Total Worker Health™ approach.
Nurses and other health care workers can also benefit from a free comprehensive online course relevant to workplace violence prevention (NIOSH, 2016). This course provides various scenarios to better understand key elements of prevention programs, application of specific strategies, and development of skills for preventing and responding to workplace violence.
Conclusion
In summary, licensed nursing professionals’ risks of working various shifts were estimated. As a result, increased risks associated with work-related assaults were identified through the application of a case-control study. These results strongly suggested that working evening, night, and rotating day and evening shifts leads to higher risks of PAs. Based on prior analyses from this major case-control study, reasons behind this finding could include inadequate lighting (Gerberich et al., 2005) and potential limitations in staffing (Shields & Wilkins, 2009). In addition, patient impairment likely contributed as well (Gerberich et al., 2004).
All these factors lend support to the conclusion that types of shifts worked may play a significant role in work-related PA against nurses. These findings serve as the basis for further investigation and the development of effective methods for reducing a substantial risk of PA in health care settings. Such methods include a high level of commitment by management in concert with participation by workers in a comprehensive program to ensure mitigation of violence against health care workers (OSHA, 2015). It is incumbent upon administrators to ensure the safety of all workers in the workplace.
Applying Research to Practice
Violence against nurses, and health care workers overall, is a serious national and global problem. Although many factors contribute, working specific shifts—particularly evening, night, and rotating day and evening shifts, compared with working only day shifts—places nurses at very high risk of PA; risks for those shifts, respectively, were 1.6, 3.5, and 2.9 times greater. The need for comprehensive policies against workplace violence, together with rigorous record-keeping enabling analysis of trends and rates of violent events, both physical and nonphysical, and unintentional injuries, is crucial. Particularly, frequent assessment and evaluation of factors that may mitigate risks, including shifts worked, relevant training, availability of coworkers and emergency assistance, and environmental conditions (e.g., lighting, protective barriers, alarm systems, personal cell phones), is fundamental to protection and retention of workers. To ensure success of this approach, management commitment, leadership including employee involvement, and provision of relevant resources are essential.
Footnotes
Authors’ Note
The contents of this effort are solely the responsibility of the authors and do not necessarily represent the official views of the Centers for Disease Control and Prevention or other associated entities.
Conflict of Interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported, in part, by the National Institute for Occupational Safety and Health, Centers for Disease Control and Prevention, Department of Health and Human Services (RO1-OH007816, T42-OH008434); the Midwest Center for Occupational Health and Safety Education and Research Center, Center for Violence Prevention and Control and Regional Injury Prevention Research Center, University of Minnesota.
Author Biographies
Steve Sun worked previously as a software engineer at ![]() and is currently employed at MA Labs in San Jose, California. He has dual Master of Science (MS) degrees in computer science and environmental health from the University of Minnesota. He has a major interest in improving workplace safety by applying his programming and data analytical expertise.
and is currently employed at MA Labs in San Jose, California. He has dual Master of Science (MS) degrees in computer science and environmental health from the University of Minnesota. He has a major interest in improving workplace safety by applying his programming and data analytical expertise.
Susan Goodwin Gerberich is the Leon S. Robertson Professor in Injury Prevention and Mayo Professor in Public Health. She is also the principal investigator (PI) and director, Midwest Center for Occupational Health and Safety Education and Research Center; codirector, Regional Injury Prevention Research Center, Center for Violence Prevention and Control, and Occupational Injury Prevention Research Training Program, Division of Environmental Health Sciences, School of Public Health, University of Minnesota. She has served as the PI for numerous population-based studies, including the study addressed in this article. She has also published extensively in peer-reviewed publications.
Andrew D. Ryan is a senior research fellow in the Division of Environmental Health Sciences, School of Public Health, University of Minnesota. He co-advises graduate students, conducts complex analyses, and manages numerous population-based studies, and has significant peer-reviewed publications to his credit.