
Abstract
This article reports on a study examining staff activities being performed when incidents were reported to have occurred. The risk for injury among health care providers who engage in patient handling activities is widely acknowledged. For those working in long-term care, the risk of occupational injury is particularly high. Although injuries and injury prevention have been widely studied, the work has generally focused on incident rates and the impact of specific assistive devices on worker safety. The purpose of this study was to examine reported staff incidents in relation to staff activities. A multicenter cross-sectional exploratory study used retrospective data from reported staff incidents (2010, 2011, and 2012) and prospective data from 360 hours of staff observations in five long-term care facilities during 2013. Descriptive statistics were used to analyze data. A total of 898 staff incidents were reviewed from the facilities. Incidents were most likely to occur in resident rooms. Resident aides were more likely to be engaged in high-risk activities than other care providers. Times when staff incidents were reported to have occurred were not associated with periods of high staff-to-resident contact. Safe handling during low and moderate risk activities should be promoted. Education on what constitutes a reportable incident and strategies to ensure compliance with reporting policies and procedures may be needed to ensure accuracy and completeness of incident data.
Health care institutions are considered high-risk worksites by the Association of Workers’ Compensation Boards of Canada (2014). The risk for injury is particularly high for those working in long-term care (LTC) settings due to the physical demands associated with resident handling, including lifting and transferring residents, and maneuvering equipment in small confined spaces. Monitoring actual or potential employee injuries is essential to understanding how best to mitigate risk and promote safety. Unfortunately, understanding work-related incidents or the circumstances that contribute to these injuries is limited. The purpose of this study was to examine work-related incidents reported by nursing staff in LTC facilities and explore the nature of the work being performed at the time incidents were reported to have occurred.
Background
The risk for injury among nursing staff who engage in patient handing activities is widely acknowledged in the literature (Mayeda-Letourneau, 2014; Theis & Finkelstein, 2014). For those working in LTC, injury rates are reported to be up to 4 times higher than the rates for other sectors (Association of Workers’ Compensation Boards of Canada, 2014; U.S. Bureau of Labor Statistics, 2014). In addition to lifting and handling, health care workers’ injuries have also been linked to several other factors. De Castro et al. (2010) reported that nurses who work more than 40 hours per week have a 45% chance of sustaining a work-related injury compared with a 35% chance for those working less than 40 hours per week. In a meta-analysis of occupational injury and accident data, Folkard and Tucker (2003) identified the risk for injury in the 12th hour of work to be more than double the risk in the first 8 hours. More recently, Harris, Sims, Parr, and Davies (2015) were unable to draw any relationship between 12-hour shifts and injuries among nurses. Evidence shows individuals working rotating day, evening, and night shifts are at increased risk for work-related injury; this risk is highest among women and those recently transitioning to shift work (Wong, Smith, Mustard, & Gignac, 2014). Risk for injury has also been reported with fluctuating physical demands over the course of a 24-hour period, fatigue, inconsistent staffing levels, and the absence of supervisors (McCaughey et al., 2014; P. Tucker & Folkard, 2012)
Injury prevention programs are common in LTC facilities. These programs are often multifaceted consisting of policies and procedures, educational and training curricula, physical conditioning or exercise programs, disability management programs, and specialized lifting and resident handling equipment (Amick et al., 2007; Mayeda-Letourneau, 2014; Thomas & Thomas, 2014; Tullar et al., 2010). Despite these efforts, work-related injuries continue to be of concern (Theis & Finkelstein, 2014). It is argued that safeguarding LTC staff is complicated by a desire to balance quality resident care in a home-like environment with safe handling procedures (Canadian Patient Safety Institute, 2008). The use of mechanical lifts and other assistive equipment does not guarantee worker safety (Koppelaar, Knibbe, Miedema, & Burdorf, 2012; Theis & Finkelstein, 2014). Engst, Chhokar, Miller, Tate, and Yassi (2005) reported a 53% increase in compensation for claims made by health care workers who use ceiling lifts for repositioning.
Although injuries and injury prevention in LTC have been widely studied (D’Arcy, Sasai, & Stearns, 2012; Polinder et al., 2012; Restrepo et al., 2013; Theis & Finkelstein, 2014), this work does not generally differentiate between organizational environments and staff activities when injuries were sustained. Yet the built environment and care activities play a significant role in injury incidence (WorkSafeNB, 2012). This article examines reported staff incidents and concurrent staff activities in five LTC facilities.
Method
A multicenter cross-sectional study was conducted to compare staff incidents in five LTC facilities in Atlantic Canada and identify the activities staff were engaged in when incidents were reported to have occurred. All facilities were government regulated, publicly funded, and not-for-profit. The number of staff and residents in each site varied but all facilities adhered to the same government-mandated resident-to-staff ratio of 20% registered nurses (RNs), 40% licensed practical nurses (LPNs), and 40% resident aides (RAs) to provide 3.1 hours of care per resident per day (Table 1).
Staffing and Residents in Each Facility
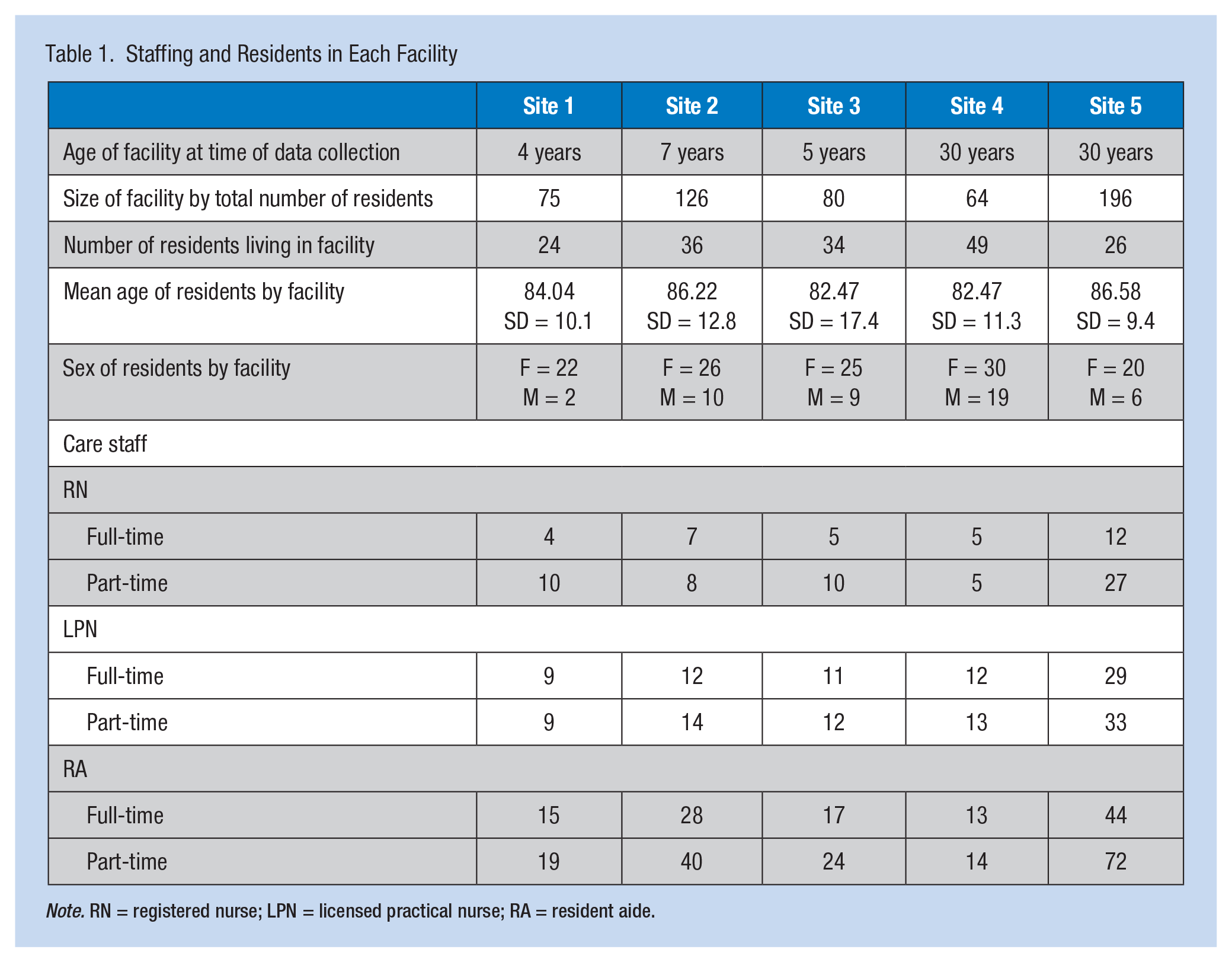
Note. RN = registered nurse; LPN = licensed practical nurse; RA = resident aide.
Data Collection
Data for this study consisted of incident data already collected in each LTC facility and observational data collected specifically for this study. Data on staff incidents were gathered from staff incident forms completed in each facility during 2010, 2011, and 2012 prior to commencing this study. These incident forms were standardized across all study sites, aggregated, and deidentified using employees’ departments rather their specific jobs. For example, incidents reported by RNs, LPNs, and RAs were identified as occurring within the nursing department.
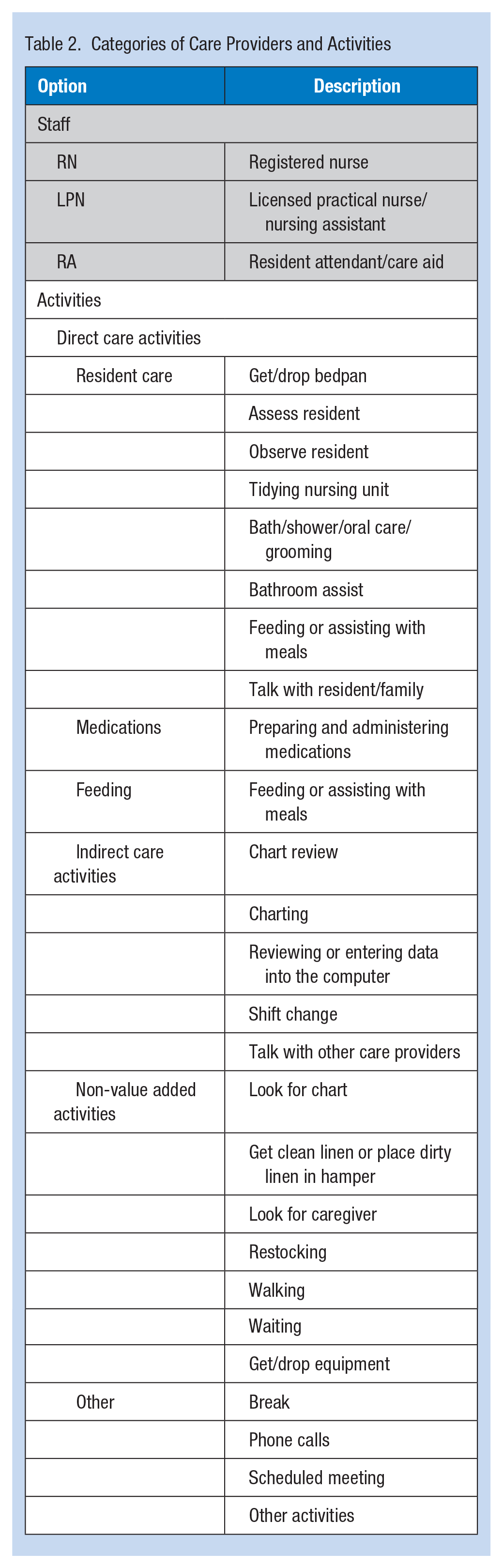
Data on staff activities were collected prospectively during 2013 via structured observations by a trained research assistant using a personal digital assistant (PDA) equipped with touch screen software, Time Study RN. The research assistant was assigned to one unit in each of the study sites and followed an identical path in each facility during 8-hour day and 8-hour evening shifts for a total of 40 shifts or 320 hours of observation. Data were captured according to the three categories of location, individual observed (i.e., job classification of care provider), and activity; a number of subcategories were linked to each category (Table 2). Due to the sensitive nature of activities that took place inside bedrooms and bathrooms, the research assistants was only permitted to observe inside these rooms if the doors were open but were prohibited from entering the areas at any time.
Categories of Care Providers and Activities
Ethical Considerations
A letter explaining the study was sent to all families and staff within each facility prior to beginning the study. Individuals working in, living in, visiting, and volunteering at the study facilities were asked to notify a designated staff member in each facility if they had any objections to the study; no one voiced any objections. No identifiable data on staff incidents or observations were collected. The study was reviewed and approved by the Research and Ethics Review Boards at the University of New Brunswick Saint John and each LTC facility involved in the study.
Data Analysis
Data from staff incident forms and observations were entered directly into Excel 2010. Descriptive statistics were calculated for staff incidents. Due to variation in the number of residents, staff, and incidents within each LTC facility, the proportion of types and time of incidents and activities were calculated for each facility.
Recorded staff activities were grouped into one of three risk-related categories. Activities that involved direct contact with residents or required staff to move equipment or exert themselves were categorized as high-risk-for-injury activities. Activities that placed staff in close proximity to residents without necessarily involving direct contact were classified as moderate-risk-for-injury activities. Activities that did not require staff to have contact with residents or move equipment and supplies or exert themselves were categorized as low-risk injury activities (Table 3). To facilitate analysis and linkages of data, prospective data on staff activities and locations were linked to times of reported staff incidents.
Provider Activities by Level of Risk for Injury
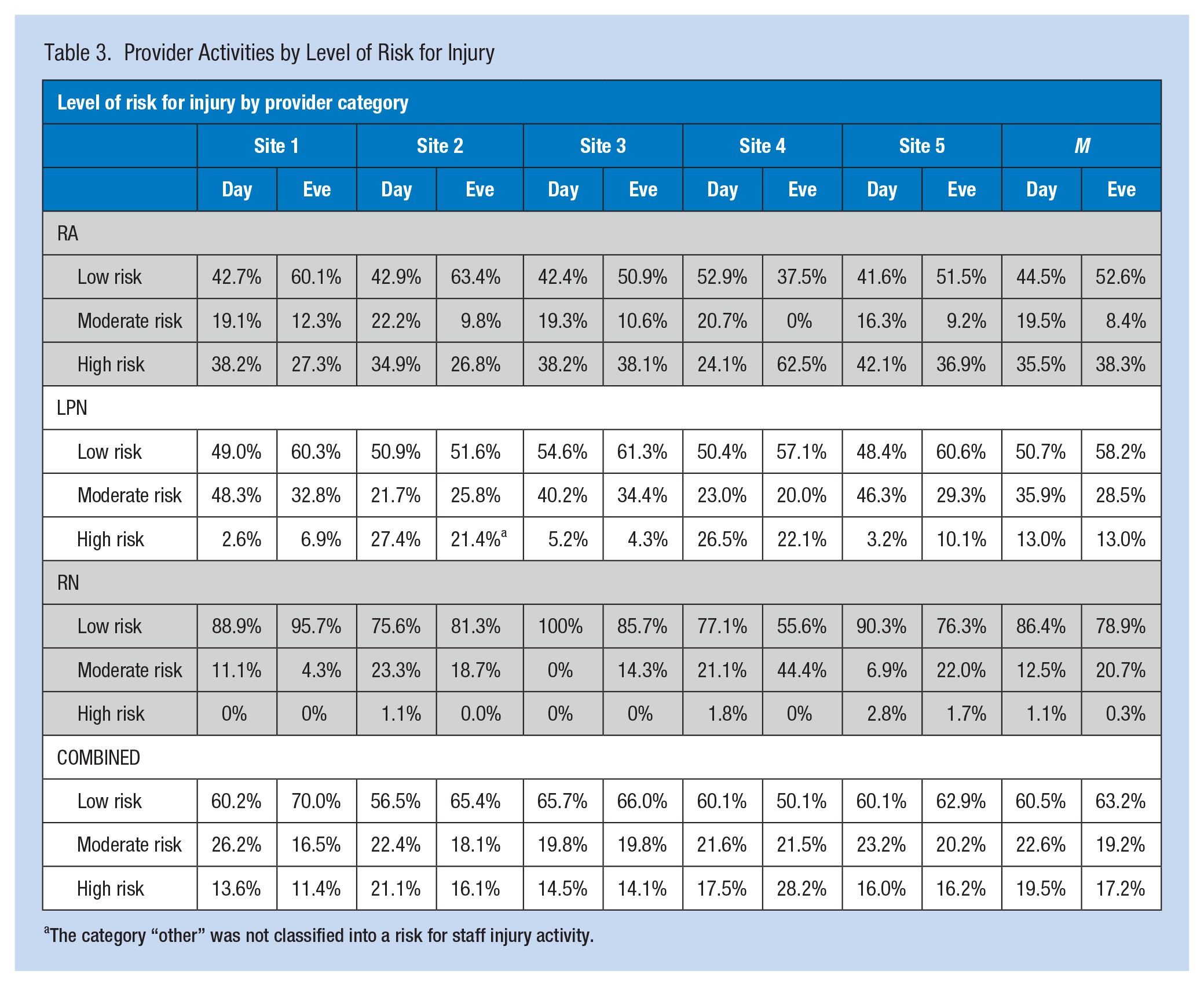
The category “other” was not classified into a risk for staff injury activity.
Results
Staff Incidents
A total of 898 staff incidents were reviewed from the five study facilities. A mean of 64.2 (SD = 49.1) staff incidents were reported annually in each facility (range: 9-142). Almost half (44.9%) of staff incidents involved full-time staff, 35.7% part-time staff, 8.8% casual staff, 7.7% were “unknown,” and 0.9% students; data on employment status were not recorded on 2% of the incident reports. Incidents were most likely to occur during 8-hour shifts (597 or 65.2%) compared with 12-hour shifts (75 or 8.2%), 4-hour shifts (34 or 3.7%), or shifts longer than 12 hours (1 or 0.1%). The length of the shift was recorded as “unknown” on 208 or 22.7% of the reports. The majority of incident reports indicated that staff members were not “working short” at the time of the incident (783 or 85.6%), and only 18 or 1.9% indicated that staff members were “working short” at the time of the incident. The remaining incident reports indicated that it was either unknown if staff were “working short” (82 or 8.9%) or data were not recorded (32 or 3.5%).
The most common time recorded for a staff incident was 9:00 a.m. followed by 10:00 a.m. and 7:00 a.m. (Figure 1). Information about incidents that resulted in lost time from work was absent from an average of 47.4% of the incident reports. According to the data that were available, 13.8% of incidents resulted in lost time from work; it was unknown whether the incident resulted in lost work time for 28.3% of the incident reports.
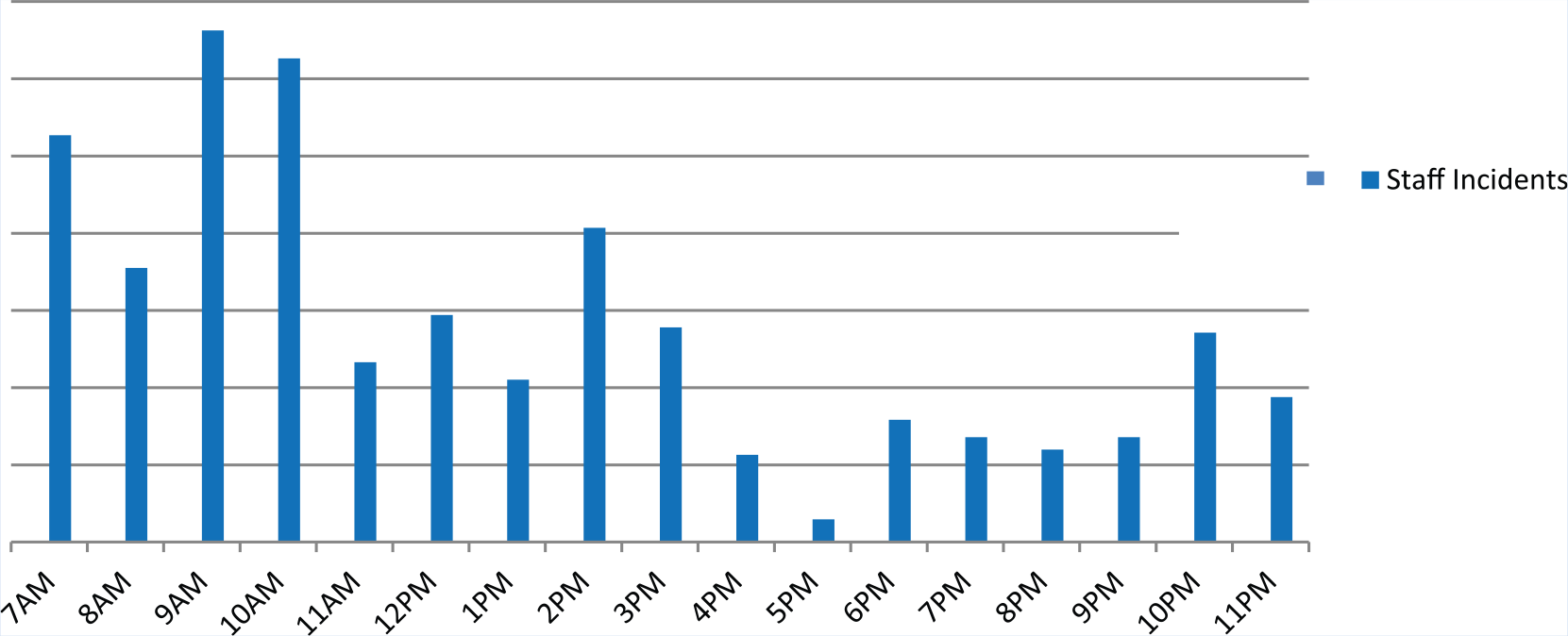
Time of staff incidents.
The most common location for staff incidents was in residents’ bedrooms (406 or 44.4%), followed by hallways (77 or 8.4%), bathrooms (74 or 8.1%), dining rooms (51 or 5.6%), kitchens (47 or 5.1%), outdoors (31 or 3.4%), laundry rooms (9 or 1%), and lounges (5 or 0.5%). A total of 84 or 9.2% reported “other” as the location of the incident. The location of the incident was “unknown” for 131 or 14.4% of the incidents. Information on the events leading to the incident was not recorded on 11 or 1.2% of the incidents and was unknown for 15.8% of all incidents. The most common event leading to staff incidents in all facilities was “overexertion” (19.0%), followed by “struck by equipment” (18.3%) and unknown (15.8%).
Incidents directly related to residents accounted for 12% of all incidents and included “resident reaction/struck by resident” (M = 11.3%) and “potential resident incidents” (M = 0.7%).
Activities by Risk and Time
Resident assistants spent more time in high-risk-for-injury activities than other care providers; RNs spent the least time in high-risk-for-injury activities. The greatest variation in high-risk-for-injury activities across facilities was for RAs (days 24.1% to 42.1%; evenings 26.8% to 62.5%). Data on reported staff incidents were aggregated and information on incidents among care providers was only available under the broad categories of management, nursing, dietary, housekeeping, maintenance, other, and unknown. When observation data for RAs, LPNs, and RNs across all facilities were combined, little difference was observed for the time staff were involved in high, moderate, or low-risk activities between day and evening shifts (19.5% vs. 17.2%, 22.6% vs. 19.2% and 60.5% vs. 63.2%, respectively; Table 3).
Peak times when staff were providing care to residents did not necessarily correspond to reported incidents (Figure 2). As expected, residents were likely to receive care at 9:00 a.m. when staff incidents were highest; however, residents were equally likely to receive care at 1:00 p.m. which was not a time of high staff incidents. Figure 3 shows staff incidents by location compared with the time staff were observed in the same location. Predictably, an association was found between the number of incidents and the time at which staff were in resident rooms.
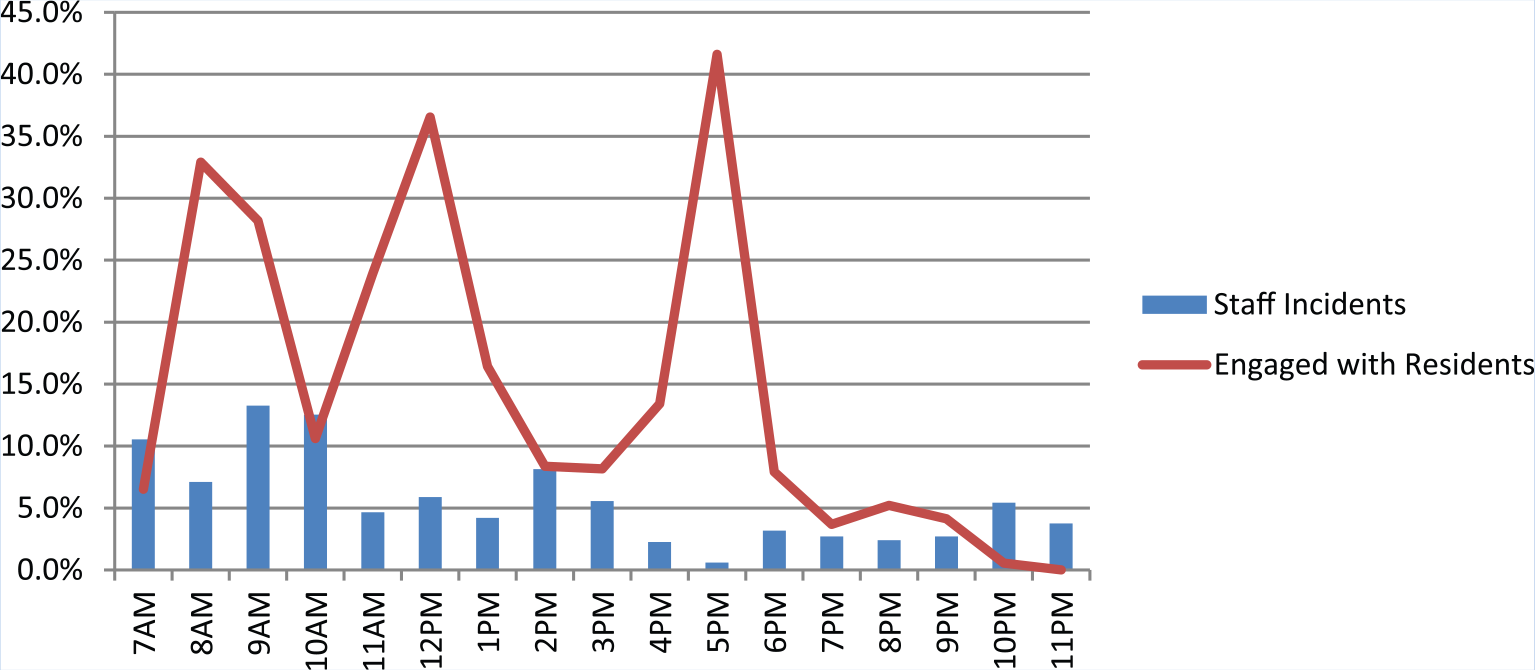
Staff incidents during peak times of resident care.
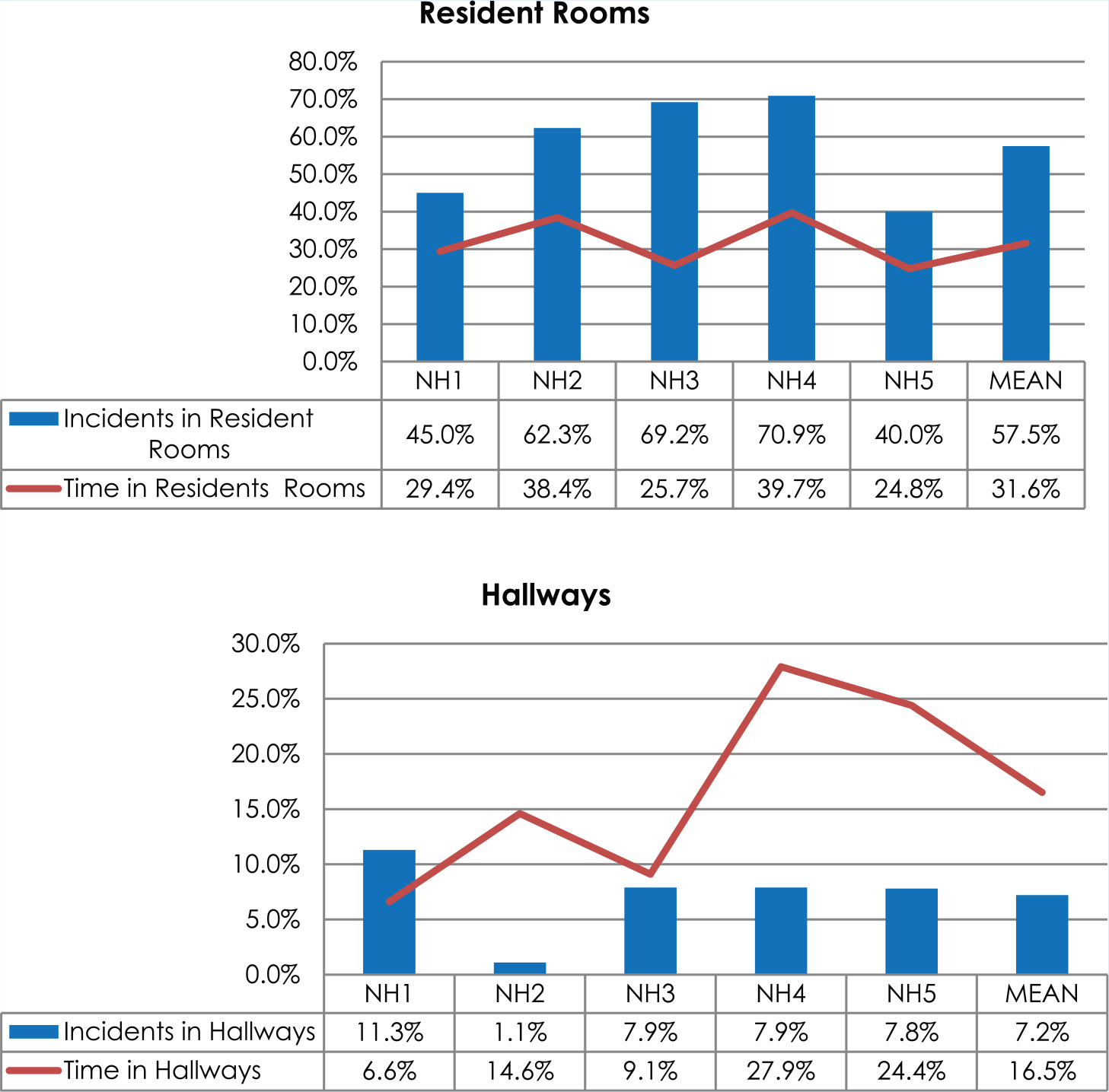
Staff incidents by location compared with staff time in area.
Discussion
The 898 staff incidents reviewed for this study include approximately 64 staff incidents annually at each study facility. It is possible that this number represents only a portion of the incidents that actually occurred in each facility. A Canadian study found that up to 50% of employees do not report work-related incidents to their employers (S. Tucker, Diekrager, Turner, & Kelloway, 2014). Other studies found less than 10% of work-related incidents were reported (Pransky, Snyder, Dembe, & Himmelstein, 1999; Qin, Kurowski, Gore, & Punnett, 2014). Some of the reasons for not reporting work-related incidents include the incident not being perceived to warrant a report, lack of time to complete necessary paperwork, fear of reprisal from supervisors or co-workers, and lack of understanding about incidents that are reportable (S. Tucker et al., 2014). Although data collected in this study may underrepresent the extent that incidents actually occurred in study facilities, safety is still a serious issue. The incidents reported by study facility personnel underscore the importance of identifying risks confronted by staff working in LTC so health and safety interventions can be appropriately implemented.
The quantity of incident reports that had incomplete or missing information is concerning. For example, it was not clear why employment status (full-time, part-time or casual) was unknown for nearly 10% of staff incidents or why the length of injured employees’ shifts was unknown for more than 22% of incidents. Likewise, differences noted in the types of incidents reported suggest some facilities were more likely to document incidents that do not result in physical injury while others were not. For instance, some facilities did not report any resident or family complaints, verbal assaults, or medication errors, but others did. Although it is possible that some of the information required on the incident forms may not have been known at the time the report was submitted (e.g., whether or not the incident resulted in injury or lost time from work), many unreported pieces of information would have been known. These inconsistencies and incomplete reports create challenges in comparing and drawing conclusions about risks across facilities. Without accurate reporting, administrators may never be fully aware of the risks that exist in LTC and therefore lack the necessary knowledge required to make informed decisions about where to direct preventive health and safety measures. Inaccurate or incomplete data also complicate the identification of safety priorities within the sector and recognition of unique features, programs, or policies within each facility that could mitigate risk and promote safety.
Efforts to improve incident reporting should focus both on incident monitoring and methods used to report incidents. It cannot be assumed that LTC staff are knowledgeable about what constitutes a reportable incident. According to the Canadian Patient Safety Institute (2012), health care providers do not always understand what constitutes a reportable incident and this may have contributed to the inconsistent and incomplete incident reports used in this study. The National Steering Committee on safety listed the identification and reporting of incidents as a priority in Canadian health care institutions (Flemons & McRae, 2012). Although the standardized incident report used in this study did allow staff to report incidents that did not involve injury or harm (near miss incidents), some facilities only completed incident reports when an obvious injury or adverse outcome was reported. Limiting reporting to incidents that only result in injury fails to capitalize on opportunities to learn of vulnerabilities or risk factors in the workplace. The U.S. Department of Health and Human Services (Levinson, 2012) recommends that health care institutions develop a list of potentially reportable incidents to demonstrate the full range of circumstances and events that constitutes an incident and share this list with their staff. Although not intended to represent an exhaustive list of reportable incidents, this list may establish the characteristics of a reportable incident.
A unique feature of this research was the observational component which allowed the researchers to identify the activities staff was doing at the times incidents were reported to have taken place. More specifically, the researchers examined incidents in relation to staffs’ direct contact with residents. Interestingly, staff incidents did not necessarily take place at times of high resident–staff contact. Data actually showed an inverse relationship between resident contact with staff and staff incidents; times of high resident–staff contact were associated with lower staff incidents, and times of low staff–resident contact were associated with higher staff incidents. This finding was consistent across all facilities. It is possible that staff were more conscious of safety during periods of high resident activity and thus less likely to sustain an injury or place themselves at risk. The fact that all study facilities had transfer equipment either mounted in ceilings or readily available for staff may explain the low incident rate during periods of high resident contact. However, the higher incident rate during periods of low resident contact deserves attention. Shannon and Lowe (2002) argued transfer equipment has decreased the need for staff to physically lift and transfer residents; however, equipment availability has also lowered staff skill in handling residents. It has also been reported that some resident handling activities do not necessarily lend themselves to the use of mechanical lifts, yet they pose a high risk of injury. These activities include repositioning or adjusting residents in bed, assisting residents while walking, and assisting residents to rise from a sitting position (Hodder, MacKinnon, Ralhan, & Keir, 2010; Skotte, Essendrop, Hansen, & Schibye, 2002). This finding many explain the higher than expected rate of incidents occurring in hallways, where staff were less likely to be observed in direct care activities.
Pompeii and colleagues (2009) reported 32% of work-related injuries among hospital workers were related to repositioning patients in bed, pulling patients up in bed, and catching patients who fall, all of which are common handling activities in LTC facilities and none of which may trigger staff to use mechanical lifts. Although the use of lateral transfer devices (i.e., slider sheets and gait belts) are often available in LTC facilities, Kurowski et al. (2012) reported a 12% compliance rate with the use of transferring equipment during repositioning. Findings from this study point to the need to explore staff safety practices during periods of low resident contact and suggest a need for more intensive training and policies regarding the use of lateral transfer devices and “lighter” resident handling techniques.
Given the majority of high-risk-for-injury activities that take place in resident rooms, it is not surprising that the percentage of incidents compared with time in resident rooms is high. Although the percentage of staff incidents in hallways is lower than the percentage of staff incidents in residents’ rooms, it is nonetheless concerning given the nature of activities that take place in hallways (e.g., resident sitting, staff walking, waiting, and communicating).
Variation in the number of staff incidents across facilities is noteworthy. It is possible that lower incident rates in some facilities may be attributed to organizational cultures that recognize the importance of well-designed work processes to support staff who care for physically and emotionally demanding residents (Tullar et al., 2010). However, it is also plausible that RN presence may have influenced incident events. One of the facilities with a lower staff incident rate had the highest RN-to-resident ratio; RNs in the facility with the second lowest incident rates were observed providing more direct resident care than in any of the other facilities. The value of RNs in improving resident outcomes has long been established (Bedin, Droz-Mendelzweig, & Chappuis, 2013; Corazzini et al., 2010; McConnell, Lekan, & Corazzini, 2010). However, what this study suggests is that having RNs closer to the bedside may have positively impacted staff safety. In their supervisory capacity, RNs may be ensuring organizational safety standards are followed. Registered nurses may also be exercising their clinical judgment and critical thinking skills to adjust established plans of care in response to fluctuating resident needs.
Due to the type of data available for analysis, the researchers were only able to determine that staff within the “nursing department” experienced more incidents than staff in all other departments combined. The researchers were unable to differentiate incidents sustained by RNs, LPNs, or RAs, or between staff working with residents with cognitive impairment (dementia) or psychiatric conditions (psychogeriatric) and those who were not. Nonetheless, findings from this study are consistent with the literature which reports musculoskeletal injuries are common among health care workers, especially those who have high levels of patient or resident contact including moving or transferring patients or residents.
The high rates of incidents related to being “struck by equipment” should be further explored given evidence to suggest it is an industry-wide problem (U.S. Bureau of Labor Statistics, 2014) and not just an issue in the study facilities. A search of the literature suggests “struck by equipment”-related incidents have not received the attention needed; not a single research report or anecdotal paper dedicated to equipment-related incidents or injuries in LTC could be located. Research dedicated to being “struck by equipment” is needed to understand how these incidents occur and how they can be mitigated.
The fact that all facilities reported no-lift policies and readily available mechanical lifts for staff use must be considered when interpreting the findings. Available lifts does not guarantee their use, nor does the provision of education and training ensure their proper use (Anyan, Faraklas, Morris, & Cochran, 2013; Kurowski, Boyer, Fulmer, Gore, & Punnett, 2012; Schoenfisch, Lipscomb, Pompeii, Myers, & Dement, 2013). A study by Theis and Finkelstein (2014) demonstrated the need for retraining staff in the safe handling of residents 18 months after the initial training. Kurowski et al. (2012) reported a 12% staff compliance rate in the use of assistive equipment to reposition residents after only 2 years post-training and 6% after 3 years post-training. An estimated cost benefit of US$3.71 for every dollar invested in retraining has been reported. Training and retraining standards should be established for LTC facilities.
Although direct care providers (RNs, LPNs, and RAs) were the primary focus of this study, data showed that staff working in other departments were also at risk for work-related incidents. For most of the study facilities, work-related incidents for nonnursing staff accounted for more than 30% of reported incidents. Staff working in dietary, maintenance, and management are not typically highlighted in discussions pertaining to staff safety as these groups are relatively small in comparison with nursing departments. Yet the burden of incidents for these groups is troublesome given the smaller number of individuals working in these areas. Strategies to improve safety in the workplace need to attend to all potential risk activities and not just those related to resident care.
Limitations
Findings must be considered within the limitations of this study, including the study design and methods of data collection. The use of two different data sets collected at different points in time was not ideal. However, it should be noted that the work of care providers has long been criticized as being ritualistic and routine, which implies that different time periods for data collection may have had minimal effect on study findings. It is also possible that care providers altered their usual routines because they were aware they were being observed. Incident data were limited to information recorded on standardized reporting forms which the researchers found contained both inconsistent and incomplete data. The use of aggregate data for staff incidents prevented a comprehensive analysis of individual categories of care providers.
Conclusion
Although work-related incidents are common in LTC facilities, results of this study show they are not always related to high-risk-for-injury resident care activities. Findings underscore the need to promote safe handling during low and moderate risk-for-injury activities, including those activities that take place outside of resident rooms. Because incident reports are often used to track organizational practices and inform the allocation of safety resources, it is imperative that efforts be made to ensure the accuracy and completeness of safety data. Organizations should consider establishing quality initiatives targeted specifically to incident reporting. Education on the definition of reportable incidents and strategies to ensure compliance with reporting policies and procedures may be needed to ensure accuracy and completeness of incident data.
Applying Research to Practice
Further research is required to understand staff incidents that take place in hallways and involve staff being struck by equipment.
Attention to safe patient handling, especially during low to moderate injury risk activities is required.
Training on how to complete incident reports and what constitutes an incident should take place in all health care organizations.
Footnotes
Conflict of Interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Funding for this study was received from WorkSafeNB.
Author Biographies
Rose McCloskey is a Nursing Professor at the University of New Brunswick, Saint John, New Brunswick, Canada. Her scholarly interests lie in gerontological nursing practice.
Cindy Donovan is the Chief Executive Office of Loch Lomond Villa Inc., Saint John, New Brunswick, Canada. She also serves as a surveyor for Accreditation Canada.
Alicia Donovan is an undergraduate student enrolled in the Bachelor of Science Degree Program, University of New Brunswick, Fredericton, Canada.