
Abstract
The objectives of the study were to profile occupational injury patterns across home health and hospice care (HHC), organization characteristics, and home health aides’ (HHAs) individual characteristics, and examine how worker training affects HHAs’ risk of reporting an injury using the model of human factors of health care in the home. The authors measured training knowledge using an 11-item scale and conducted univariate and bivariate analyses to describe injury patterns across individual, occupational, and organizational factors using STATA 12.0. The researchers found that work-related injuries and type of injury were associated with increased likelihood of reporting one or more injuries, full-time employment, high hourly pay, and working in an inpatient or mixed setting. Overall, HHAs perceived that they received “excellent” and “good” training on key topics that promoted safety and job knowledge. Furthermore, the results suggested linkages between worker’s complex personal, occupational, and organizational characteristics.
Occupational Injury Patterns and Perceived Training Quality
In 2011, 4 million home-based direct care workers (DCWs) provided care in the United States, and the number of these workers is anticipated to increase by 93% by 2020 (U.S. Bureau of Labor Statistics, 2012c). Beyond the existing direct relationship between the number of caregivers and patients, the Health Resources and Services Administration (HRSA) identified three main contributors to the increased need for DCWs in long-term care (LTC): (a) increased life expectancy of individuals with one or more chronic conditions, (b) aging population (e.g., baby boomers), and (c) increased access to and availability of community resources (Agency for Healthcare Research and Quality, 2001). Therefore, home-based DCWs will be required to provide home health care services to patients who are older and sicker with multiple chronic conditions, increasing these workers’ risks for hazard exposure and occupational injuries (Bayliss et al., 2014; Brown, 2008; Hootman, Bolen, Helmick, & Langmaid, 2006; R. I. Stone & Barbarotta, 2010).
Safety training and injury prevention programs have not been shown to reduce the above-average injury rate for home-based DCWs (i.e., 424 per 10,000 full-time employees compared with a national average of 117 per 10,000 full-time employees). This finding is of concern because home-based direct care is the second-fastest growing work sector in the United States; yet, information is particularly scarce about worker well-being and safety in this sector (Leff, Hagenbach, & Marn, 2000; U.S. Bureau of Labor Statistics, 2012b, 2012c; U.S. Occupational Safety and Health Administration, 2012).
Work-related injury is defined as any physical injury that required treatment or resulted in days away from work, sustained by an employee, and related to performing work duties and responsibilities (Wing, Langelier, Yamada, Poonthota, & Kumar, 2004). Home-based DCWs reported that work-related injuries accounted for 20% of total reported injuries (U.S. Bureau of Labor Statistics, 2012c). As this subcategory of the workforce continues to grow, it is difficult to ensure workers’ health and safety (Houston, Young, & Fitzgerald, 2013); yet ensuring their occupational well-being is critical to workers’ health, the organization’s success, and patients’ quality of care (P. W. Stone et al., 2007). One key barrier to occupational health and safety is the high turnover rate among DCWs, costing the LTC system US$4.1 billion, approximately US$3,500 per home-based DCW (Seavey, 2004, 2010). In 2003, 40 of the 50 states reported a home-based DCW shortage as a major public health concern (Gropelli & Corle, 2011; P. W. Stone et al., 2007). The persistence of high turnover rates and vacancies among this workforce category is negatively affecting workers’ ability to complete required tasks effectively and safely.
Other factors, any attribute or characteristic of exposure (individual, organizational, or environmental), can increase home-based DCWs’ risk of experiencing work-related injuries (Gropelli & Corle, 2011; Miller, 2013). Worker-specific risk factors for occupational injury include workers’ demographics, including their socioeconomic characteristics and work-related skills and knowledge (Oliver, Cheyne, Tomas, & Cox, 2002). The interrelationship between these factors affects workers’ abilities to provide care to their patients, which is vital because the leading cause of injury among home-based DCWs is manual handling of patients, which commonly leads to musculoskeletal disorders, (e.g., back injuries; Gropelli & Corle, 2011).
The mandatory federal training requirements have not changed for home health aides (HHAs) since they were established over 20 years ago. These requirements do not include formal training; thus, HHAs traditionally have little to no formal training before beginning to care for patients (Cohn, Horgas, & Marsiske, 1990; Sengupta, Ejaz, & Harris-Kojetin, 2012). Many training programs are mandated by states, provide few opportunities for hands-on experience, and do not reflect the complex needs of today’s aging population. Training requirements and contact hours also vary by state and range from 75 to 120 hours, which makes cross-state comparisons challenging (Paraprofessional Healthcare Institute PolicyWorks, 2013). Research has documented that the lack of standardized training negatively affects HHAs’ attitudes toward, perceptions of, and knowledge related to patient care and their ability to provide high-quality care and safety (Gettle, 2009). Research has also shown that workers’ perceptions of on-the-job training, both for knowledge and skill acquisition in key competency areas, are associated with greater job satisfaction and lower risk of occupational injury (Ejaz, Noelker, Menne, & Bagaka’s, 2008).
Thus, the objective of this study was to establish a baseline for home-based DCWs by profiling and describing occupational injury patterns by DCWs’ personal characteristics, agency characteristics, and places of care delivery. The primary research questions for this study were:
Conceptual Framework
An approach to accident modeling examined the human aspect of accident causation and was the guiding framework for this study. The model, Human Factors of Home Health Care (Czaja et al., 2006), was selected because of its systems approach; incorporation of human, technology, and environmental factors; and absence of assessment of the actual injury event. The system consists of the individual(s) involved in the delivery of home health care, the manner in which home health care tasks are delivered, the training workers receive, the equipment or technology used by HHAs, and the political, community social, and physical environments in which these interactions take place.
The study of human factors is defined as the application of information “about human strengths and limitations to the design of interactive systems of people, equipment, and their environment to ensure their effectiveness, safety, and ease of use” (Henriksen, Dayton, Keyes, Carayon, & Hughes, 2008, p. 67). The International Ergonomics Association (2010) further defined human factors as the scientific discipline concerned with the understanding of interactions among humans, and other elements of a system, and the profession that applies theory, principles, data, and other methods to design in order to optimize human well-being, and overall system performance. (p. 1)
Method
Study Design and Participants
This study used a secondary cross-sectional design to analyze data from a nationally representative sample of home-based DCWs who participated in the 2007 National Home Health Aides Survey (NHHAS). The samples were selected using a stratified, multistage probability design. The 2007 NHHAS used computer-assisted personal interviewing (CAPI) to randomly identify and interview up to six HHAs at one of 1,036 home health, hospice, and mixed agencies. A total of 4,416 eligible aides were selected, and 3,377 completed the telephone interviews, a response rate of 76.5% (Bercovitz et al., 2011). Of the 3,377 HHAs who participated in the survey, 624 reported suffering an injury during the study period. The research was reviewed and categorized as “exempt” by the Institutional Review Board because of its use of de-identified national secondary data.
Measures
Dependent variables
Three outcome variables were examined. The first item asked all respondents whether they had experienced a back injury, including pulled muscles, other strains, human or animal bites, scratches, bruises, burns, or any other injuries. The second variable was work-related injury, categorized into six types. Injury was defined as any injury reported to the agency, or that required medical attention, or that resulted in missed workdays. Work-related injury was operationalized such that inapplicable/not ascertained was equivalent to not injured (zero incidents of injury) and reporting one or more incidents of injury equated to being injured (McCaughey et al., 2012). The third variable was injury severity measured by home-based DCWs’ self-reported days of work missed because of injuries. The variable was operationalized in accordance with the Bureau of Labor Statistics (BLS) into high and low injury severity using the average number of missed workdays (9 days) as the cutoff point (U.S. Bureau of Labor Statistics, 2012a).
Independent variables
The health care training knowledge measure addressed 11 competencies: patient care skills, talking with patients, talking with families, organizing work tasks, dementia care, working with abusive patients, preventing personal injury, duties that do not directly involve patients, end-of-life issues, abuse and neglect issues, and cultural competency. Respondents answered survey items using a 5-point scale: 0 = indicated lack of training, 1 = poor training, 2 = fair training, 3 = good training, and 4 = excellent training. The mean score was used in the analysis. All 11 items were used to develop the training scale.
The internal reliability estimate for this scale was acceptable with a Cronbach’s α = .8425 (Nunnally, 1975). The researchers used factor analysis to confirm the presence of only one factor (Eigenvalue = 4.07672), strengthening the scale construct. The authors then dichotomized the mean score of all 11 survey items. Poor training consisted of scores ranked in the bottom 25%, and good training consisted of scores ranked in the top 75th percentile.
Control variables
Individual characteristics
The authors used workers’ self-reported socioeconomic and other demographic variables as covariates in profiling occupational injury patterns. These characteristics included race (coded as non-Hispanic, White, Black, Hispanic of any race, and Other), education, age, gender, household income, marital status, number of children in household under the age of 17, place of care delivery (coded as Home Health, Hospice, and Mixed), hourly pay rate (coded as low, average, and high hourly pay rate), job experience, health status, time at current job, number of jobs in the last 5 years, number of current employers, and primary language (measured to reflect the diversity of the home-based direct care workforce and its effect on patient/worker communication). HHAs’ gender and primary language were not controlled for because approximately 95% of the sample were female and spoke English.
Agency characteristics
Last, the authors used agency-specific variables to understand the impact of agency characteristics on occupational injury patterns. In the public version of the 2007 NHHAS, a limited number of agency characteristics included agency location (coded as metropolitan, metropolitan or large rural, and small rural), type of ownership status (for profit and other), and chain affiliation.
Analysis
The researchers conducted all analyses using STATA (Version 12.0, STATA Corporation, College Station, TX, USA) to account for the complex, weighted, and clustered structure of the sample design. They set the level of significance at p < .05 and conducted univariate and bivariate analyses using frequencies, percentages, means, medians, and standard deviations to describe home-based DCWs’ work-related injury patterns across individual and organizational factors. The authors applied parametric and nonparametric tests to identify differences in reporting and severity of occupational injuries by individual, sociodemographic, and organizational characteristics.
Results
The study population was overwhelmingly female (95%) and identified English as their primarily spoken language (94%). More than half of HHAs were White and non-Hispanic with a high school education or less. Only 40% of HHAs had some college or more education. The average income of this study population was less than US$30,000, and the participants on average had more than 6 years of home health experience.
Work-Related Injury
Among HHAs’ demographic characteristics, race (p = .001) and education (p = .034) were significantly associated with work-related injury. Exploring HHAs’ job characteristics, HHAs’ employment status (full-time or part-time), number of jobs they held, hourly pay rate, and place of care delivery were associated with work-related injury. Among HHAs who reported an injury, 65% worked in patient homes, 80% were employed full-time (SE = 4.11, p = .000), 90% held one job (SE = 2.15, p = .000), and 47% had higher hourly pay rates (over the mean wage of US$10.39). Among agency characteristics, more HHAs working for home health agencies reported injuries (57%) than their counterparts working in hospice or mixed agency. In addition, more HHAs at not-for-profit agencies reported injuries than those who worked at for-profit home health agencies.
Injury Severity
The degree of severity, measured by the number of lost workdays and reported work-related injuries, and the association of these injuries with demographic, job, and agency characteristics are shown in Table 1. Examining HHAs’ demographic characteristics, race and education continued to have a significant association with injury severity. Of those HHAs who reported injuries that required 1 or more missed days from work, 64% were White and non-Hispanic, and 57% had a high school degree or less. Of the HHAs who sustained injuries that did not result in missed workdays, 82% were White and non-Hispanic, and 65% had some college or more. Among HHAs’ job characteristics, HHAs’ employment status, number of current employers, hourly pay rate, and place of care delivery were not only associated with work-related injury but were also associated with its severity. Of injured HHAs with no missed workdays, 87% were employed full-time, 90% held one job, 61% had a higher hourly pay rate, and 64% worked in patient homes. Of those HHAs with injuries that resulted in 1 or more missed workdays, 76% held a full-time job, 90% had only one job, 37% had a higher hourly pay rate and another 38% had an average hourly pay rate, and 65% worked in patient homes. Exploring agency characteristics revealed that agency type (p = .001) and ownership status (p = .008) were significantly associated with injury severity.
Injuries and Their Severity Among HHAs in the 2007 NHHAS
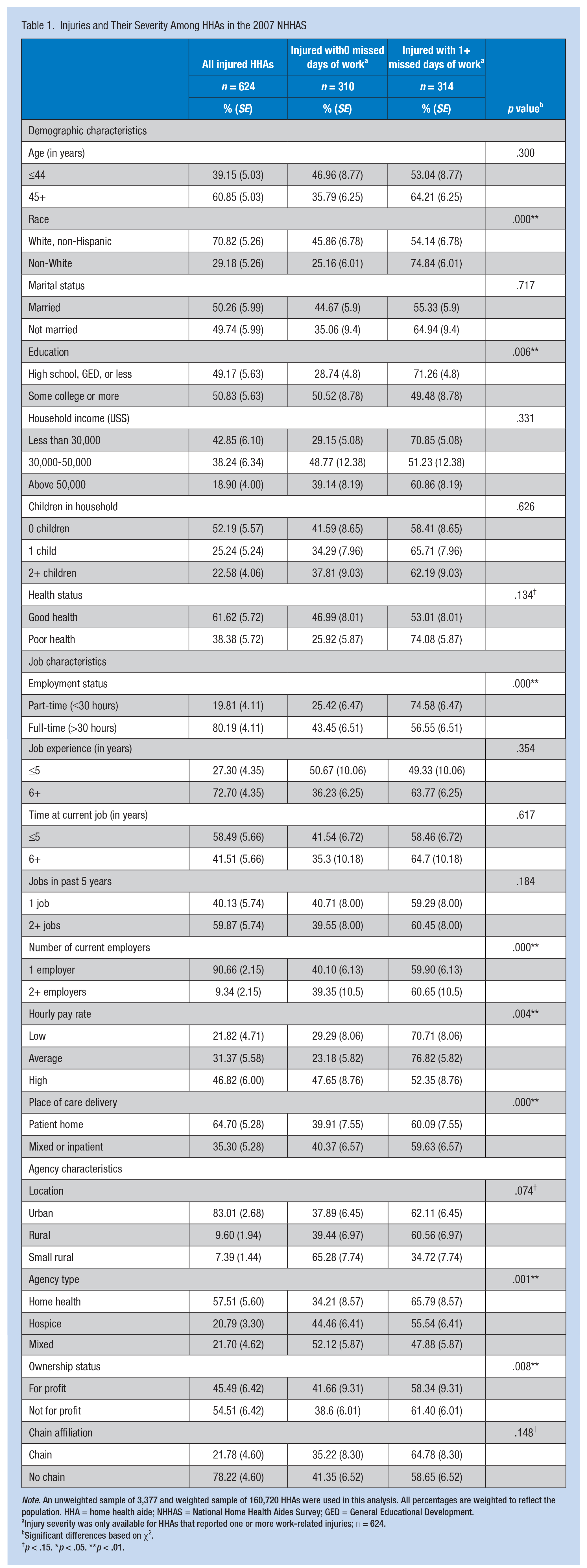
Note. An unweighted sample of 3,377 and weighted sample of 160,720 HHAs were used in this analysis. All percentages are weighted to reflect the population. HHA = home health aide; NHHAS = National Home Health Aides Survey; GED = General Educational Development.
Injury severity was only available for HHAs that reported one or more work-related injuries; n = 624.
Significant differences based on χ2.
p < .15. *p < .05. **p < .01.
Injury Patterns Among HHAs
The authors analyzed the distribution of injury types reported by the study sample using unweighted frequencies. The two most frequent types of injuries sustained by the sample that required 1 or more days away from work were back injury (254 injuries) and strain (212 injuries), consistent with studies found in the literature. From the total 624 injuries reported, 129 of HHAs suffered burns and/or wounds, the majority of which (93 incidents) did not require any days away from work. All injury types were significantly associated with injury severity. Approximately 73% of injuries that caused 1 or more days away from work were due to back injuries and strains, but only 26% of injured individuals with 0 missed days of work had back injuries and strains.
Approximately 8% of HHAs who work only in patients’ homes reported back injuries and strains, but less than 2% had other types of injures. This number is slightly greater for those HHAs working in a mixed agency that included one or more inpatient facilities, whereby 14% reported back injuries and 8% experienced other types of injuries. Work-related injuries and types of injuries were significantly associated with place of care delivery. Among HHAs employed in a mixed agency, 20% (SE = 3.01) reported one or more work-related injuries. Of those HHAs who primarily provide care in patient homes, 9% (SE = 1.39) reported one or more injury. Injury severity was not associated with HHAs’ primary place of care delivery.
HHAs’ Assessments of Training and Knowledge
HHAs’ ratings of the 11 training topics (e.g., performing resident/patient care skills, organizing work tasks, providing dementia care, and preventing injury) were also examined (Table 2). Approximately 50% of HHAs reported that training across all topics had provided them with excellent skills and knowledge to care for their patients, and another 35% reported their training was good. Between 14% and 16% of HHAs stated they had not received training in one or more of the topic areas or that they received poor training.
Injured HHAs’ Assessment of Individual Training Topics
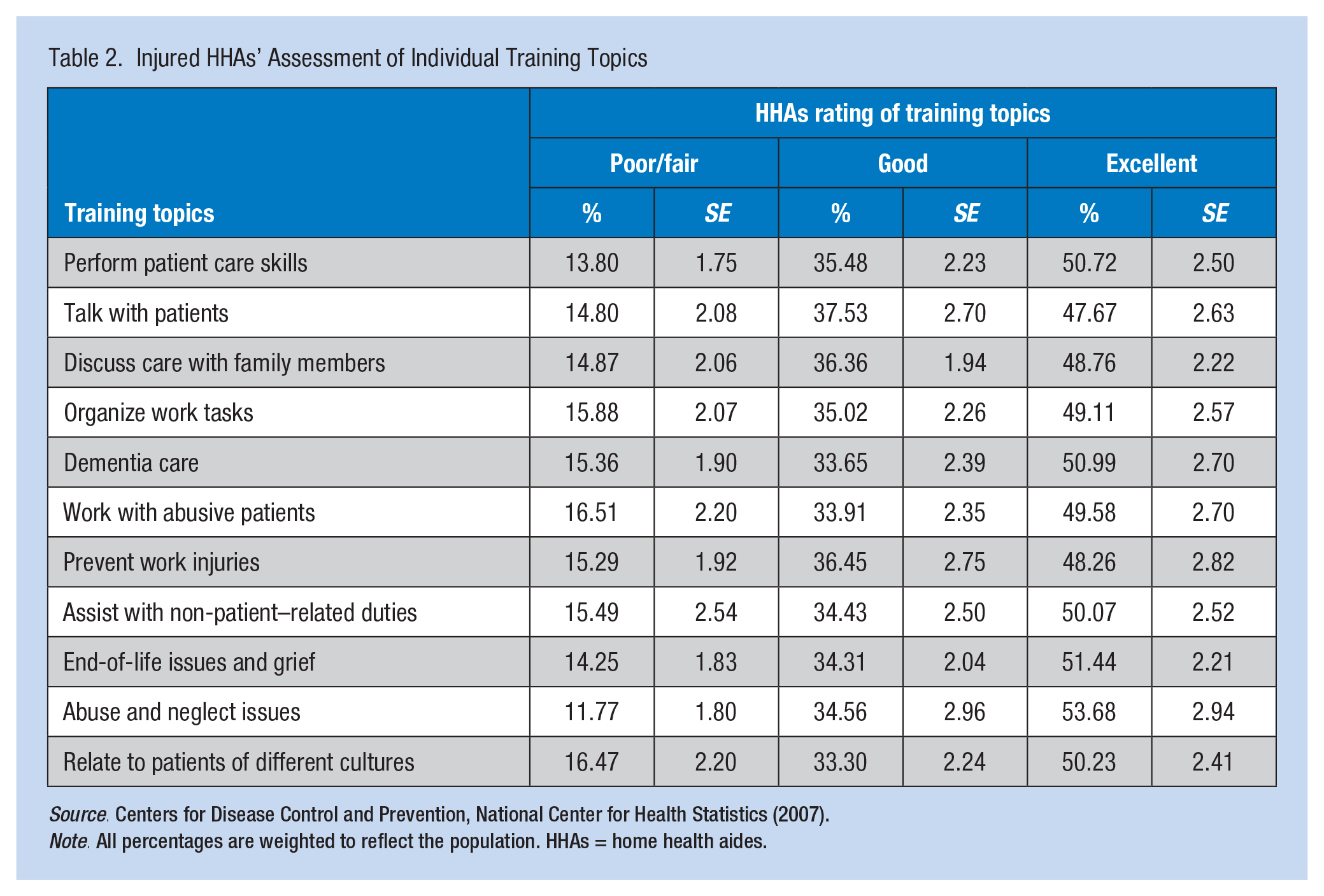
Note. All percentages are weighted to reflect the population. HHAs = home health aides.
A weighted cross-tabulation was calculated between HHAs’ overall assessment of training knowledge (good training, poor training) and work injury patterns as measured by work-related injury, injury severity, and type of injury; findings are presented in Table 3. Chi-square results indicated that overall assessment of training knowledge did not vary significantly by injury pattern. Thus, perceived training knowledge was not associated with HHAs’ risk of injury, injury type, or injury severity.
HHAs Perceived Training Knowledge and Work Injury Patterns
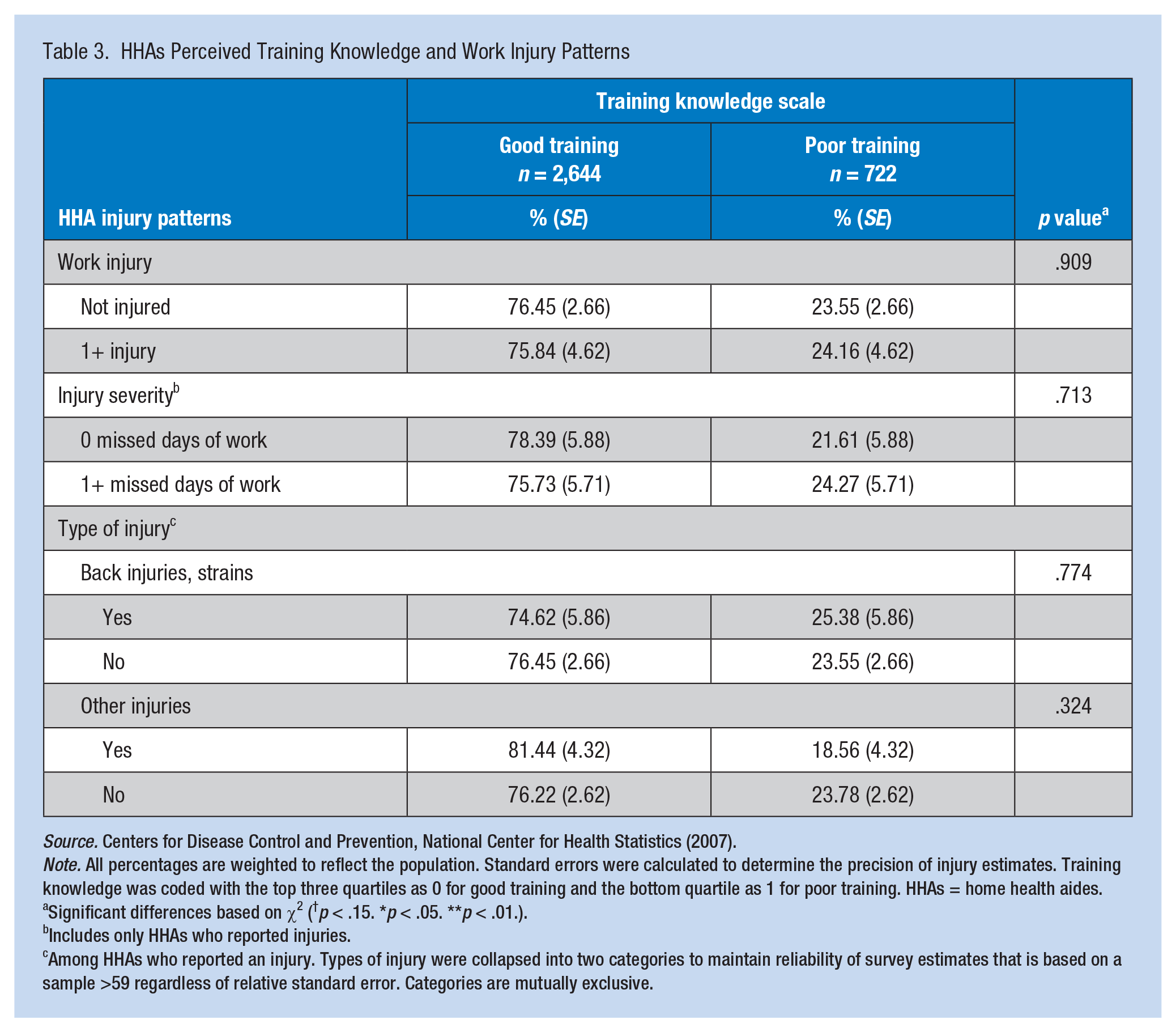
Note. All percentages are weighted to reflect the population. Standard errors were calculated to determine the precision of injury estimates. Training knowledge was coded with the top three quartiles as 0 for good training and the bottom quartile as 1 for poor training. HHAs = home health aides.
Significant differences based on χ2 (†p < .15. *p < .05. **p < .01.).
Includes only HHAs who reported injuries.
Among HHAs who reported an injury. Types of injury were collapsed into two categories to maintain reliability of survey estimates that is based on a sample >59 regardless of relative standard error. Categories are mutually exclusive.
Multivariate Analysis: Effects of Training Knowledge and Other Risk Factors
Generalized logistic regression was used to distinguish the effects of training knowledge and the likelihood of HHAs reporting one or more work-related injuries holding other characteristics constant. The binary logistic regression analysis modeled the effect of perceived poor training on the risk for injury. The multinomial logistic regression analysis modeled the effect of poor training knowledge on injury severity. Table 4 displays the results of binary and multinomial regression modeling. Poor training knowledge, with other characteristics held constant, had no effect on the likelihood of HHAs reporting work-related injuries or injury severity.
Effects of Poor Training on Work-Related Injuries and Their Severity, Holding HHA and Agency Characteristics Constant
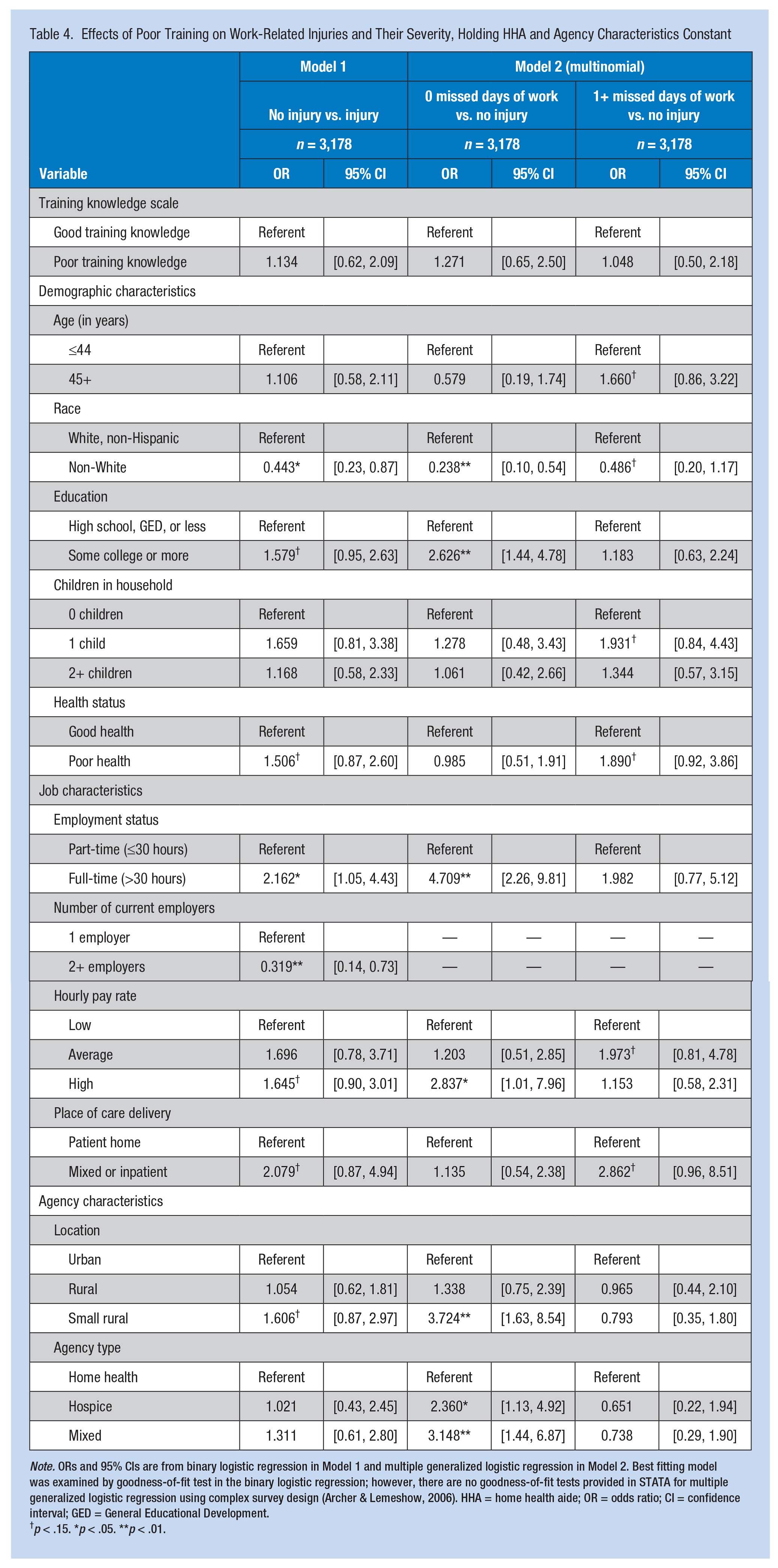
Note. ORs and 95% CIs are from binary logistic regression in Model 1 and multiple generalized logistic regression in Model 2. Best fitting model was examined by goodness-of-fit test in the binary logistic regression; however, there are no goodness-of-fit tests provided in STATA for multiple generalized logistic regression using complex survey design (Archer & Lemeshow, 2006). HHA = home health aide; OR = odds ratio; CI = confidence interval; GED = General Educational Development.
p < .15. *p < .05. **p < .01.
Race, employment status, and number of current employers were linked to the risk of work-related injury. Non-White HHAs were 40% less likely to report work-related injuries compared with White HHAs (odds ratio [OR] = 0.44, 95% confidence interval [CI] = [0.58, 2.11]). Full-time HHAs were more likely to report work-related injury than part-time HHAs (OR = 2.16, 95% CI = [1.05, 4.43]). HHAs with more than one employer were less likely to report work-related injuries than HHAs with a single employer (OR = 0.32, 95% CI = [0.14, 0.73]).
The factors associated with less injury severity (i.e., injury that resulted in 0 missed days of work) were race, education, employment status, hourly pay rate, agency geographic location, and agency type. Non-White HHAs were less likely to report work-related injuries with 0 missed days of work than White HHAs (OR = 0.238, 95% CI = [0.10, 0.54]); however, race had no effect on reporting high injury severity (1+ missed days of work). Full-time employees, HHAs with higher hourly pay rate, home health agencies in small rural areas, and hospice and mixed agencies were associated with work-related injuries with lower injury severity but had no effect on higher injury severity.
Discussion
With the paucity of literature on work-related injuries and training knowledge among HHAs, the findings of this study cannot be compared with other studies. The study had several key findings. First, in this study, HHAs reported that they received “excellent” and “good” training on key topic areas that promoted safety and job knowledge. However, the appropriateness of this training was not addressed in this study.
Second, the researchers found that working part-time, being non-White, and having multiple employers decreased the risk of reporting one or more injuries. However, the relationship between work-related injury, race, employment status, and number of current employers might be the result of reporting patterns and issues. Contributing to this finding, national data are often collected on the number of full-time equivalent (FTE) workers employed in Medicare-certified home health and hospice care (HHC) agencies. However, HHAs are often hired on a contingent or part-time basis or are privately employed, suggesting that national data may have underestimated the total number of both HHAs and injuries (Institute for the Future of Aging Services, 2007; Montgomery, Lyn Holley, Deichert, & Kosloski, 2005; U.S. Occupational Safety & Health Administration and National Association for Home Care, 1992).
Third, no differences were found between HHAs reporting high injury severity and HHAs’ sociodemographic, job, and agency characteristics. On the contrary, when examining low injury severity, the study found relationships with high hourly pay rate, full-time employment, hospice or mixed agency employment, and geographic locations in small rural areas.
The reporting discrepancy is critical to a better understanding of injury patterns. Data from the BLS provide a percent distribution for nonfatal occupational injuries and illnesses including days away from work by race: 39.4% of incidents for Whites and 21.6% for non-Whites (U.S. Bureau of Labor Statistics, 2012a). A survey conducted by the American Nurses Association found that the DCWs’ reasons for not reporting incidents included (a) fear of termination or possible disciplinary action, (b) fear of harassment by others, (c) possible reason for denying promotion or career advancement opportunities, and (d) sullying reputation among colleagues, patients, or supervisors (de Castro, 2003).
In this sample, 11.7% of HHAs reported a work-related injury, significantly less than the 56% of certified nursing aides in the 2004 National Nursing Assistant Survey (NNAS) and other estimates of injuries among DCWs (Khatutsky, Wiener, Anderson, & Porell, 2012; Kopiec, 2000; Squillace et al., 2009; Tak, Sweeney, Alterman, Baron, & Calvert, 2010). Several hypotheses could explain this discrepancy. HHAs often work alone, typically unsupervised, and thus have more opportunity to hide injuries and not report them. This is not as likely for certified nursing assistants (CNAs) who work with other individuals and are directly supervised by a registered nurse (RN), licensed practical nurse (LPN), or licensed vocational nurse (LVN). This explanation is evident in Table 4: HHAs working in mixed or inpatient facilities had the highest rate of reported injury (OR = 2.079, 95% CI = [0.84, 4.94]). The findings of this study shed light on the importance of the work environment, and its effects on worker safety and well-being. Furthermore, the results presented here are supported by other studies suggesting a link between workers’ complex personal, job, and agency characteristics.
Implications for Practice
The most readily incentivized approach to increasing worker safety, and decreasing the number of work-related injuries, is training and prevention interventions. Employers’ main goal is to prevent work-related injuries by eliminating DCWs’ unsafe behaviors (Brannon, Zinn, Mor, & Davis, 2002; Service Employees International Union, 1995). As home health care services became reimbursable under Medicaid and Medicare, certification training for home-based workers has been implemented to meet the Centers for Medicare and Medicaid Services (CMS) standards (Fishman, 2004). Training has improved employee statistics and provided more employee control over their work. In addition, it is apparent that workers are willing to invest in their futures (Wassell, 2009). Furthermore, it was observed that trained HHAs were less likely to suffer occupational injuries (McCaughey et al., 2012).
The findings of this study have several implications related to the content and intensity of HHA training. When examining training content and employee knowledge, the association between training and injury disappears. This finding highlights the need to establish an appropriate teaching–learning pedagogy and specific training on injury prevention. The current mandatory state requirements for HHAs might be insufficient in effectively teaching workers how to maintain their safety in patients’ homes (Paraprofessional Healthcare Institute PolicyWorks, 2013). Future research is needed to explore training curricula, workers’ experiences with and perceptions about occupational injuries, and the effect of various adult learning strategies on the incidence of workplace injuries.
Limitations
This study had several limitations. First, the study used a cross-sectional design and was derived from a secondary analysis, inhibiting the ability to determine causal inference. Second, the survey heavily relied on self-reported data by asking respondents to recall information. Last, the researchers’ inability to examine and evaluate reported injuries may have affected the study’s findings. In risk factor assessment, examining how injuries occurred is instrumental in developing appropriate prevention programs. The study found no relationship between reported work-related injuries and perceived training knowledge. However, the most incentivized approach to promoting worker safety and reducing occupational injury is training: Training has been used for many years to address unsafe behavior (Brannon, Barry, Kemper, Schreiner, & Vasey, 2007; Service Employees International Union, 1995). However, this finding may be explained by the method in which the training was implemented. Most HHA training occurs in a classroom with minimal hands-on experience, which has been shown to be critical in improving care delivery (Paraprofessional Healthcare Institute PolicyWorks, 2013; Sengupta et al., 2012; Yeatts, Cready, Swan, & Shen, 2010).
Future research is needed to examine the effects of HHA work-related injuries and workplace outcomes because little relevant research was found in the literature. Future studies should explore the effect of worker satisfaction and turnover on work-related injuries among this subgroup of workers. Finally, future studies should expand the understanding of training knowledge by exploring the types of and strategies for worker training to appropriately identify optimal training methods to significantly reduce occupational injury.
Applying Research to Practice
This study has implications for a subcategory of the workforce that will be in demand over the next several decades but for whom little occupational research has been published. This issue is a major public health concern because this workforce will be in high demand as the U.S. population grows older and sicker. Therefore, home health aides (HHAs), who are required to lift patients independently, must be trained to effectively protect themselves, care for their patients, and benefit the long-term care system.
Footnotes
Authors’ Note
The article has not been previously published and is not under consideration in the same or substantially similar form in any other journal. All those listed as authors are qualified for authorship and all who are qualified to be authors are listed as authors on the byline. Each author has participated and contributed sufficiently to take public responsibility for appropriate portions of the content.
Conflict of Interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Author Biographies
Hanadi Hamadi is currently a junior faculty at the Department of Health Administration at the University of North Florida. His research interest is in workforce development and safety.
Janice C. Probst is a professor in the Department of Health Services Policy and Management at the University of South Carolina. Her research interest includes rural health care delivery, health disparities, and potentially preventable hospitalization.
M. Mahmud Khan is currently professor and chair, Department of Health Services Policy and Management, University of South Carolina. His research projects include costing, economic evaluation, health economics and policy, healthcare financing, and impact evaluation of results based financing.
Jessica Bellinger is a research assistant professor in the Department of Health Services Policy and Management, University of South Carolina. Her research explores health services delivery in primary care settings, adolescent vaccine policy, and cancer prevention and control with an emphasis on rural, minority, and underserved populations.
Candace Porter is currently a research assistant in the Aging Department, University of South Carolina. Her research explores health services and statistical analysis.