
Abstract
Little evidence links emotional labor to either psychological or physical health. This study determined whether the two types of emotional labor (i.e., surface vs. deep acting) were significantly associated with depressive symptoms and work-related musculoskeletal disorders in call center workers. A cross-sectional study was conducted with 274 workers recruited from a call center in Seoul, South Korea. In adjusted regression models, levels of surface, but not deep, acting were significantly and positively associated with depressive symptoms. Higher surface acting levels were significantly and positively associated with low back pain; higher deep acting levels were significantly and inversely associated with low back pain. Study findings could inform occupational health nurses as they delineate differentiated strategies, according to the nature of surface and deep acting, to promote psychological and physical health in call center workers.
The call center market is one of the most rapidly growing industries worldwide. The number of call centers increased by 49% in developed countries, including South Korea, between 2003 and 2008 (Korea Callcenter Information Research Center, 2008). Concomitantly, the number of call center workers has increased by 14% in South Korea (Korean Statistical Information Service, 2014).
According to the classification criteria established by the International Standard Classification of Occupations (International Labour Organization, 2012), call center workers undertake two roles: contact-center information clerk and contact-center salesperson. Call center workers handle customers’ concerns and complaints regarding products and services via voice-to-voice contact using computers and telephones (Korea National Statistical Office, 2007). To manage various aspects of customer relationships, call center workers are required to provide customer service cordially, responsibly, and efficiently using high-quality communication skills (Lin, Chen, & Lu, 2009; Tuten & Neidermeyer, 2004). In this context, call centers are viewed as stressful work environments with high psychological job demands, leading to high turnover and absenteeism (Tuten & Neidermeyer, 2004).
Call center workers demonstrate higher levels of emotional labor than workers in any other occupational group (Kim & Han, 2008). Emotional labor is defined as the management of feelings to create a publicly observable facial and bodily display (Hochschild, 2003). Specifically, emotional labor is a regulation process using feelings and expression of organizational goals; emotional labor is of two types: surface acting and deep acting (Grandey, 2000; Hulsheger & Schewe, 2011). Surface acting is a response-focused form of emotion regulation that inhibits emotional responses once emotion has been generated (Grandey, 2000; Gross, 1998). Deep acting is an antecedent-focused form of emotion regulation that modifies perceptions of a situation to adjust emotion (Grandey, 2000; Gross, 1998).
Emotional labor may be linked to psychological and physical health problems. Depression has been diagnosed and treated frequently in call center workers (Charbotel et al., 2009). A link between emotional labor and depressive symptoms has been identified in other workers (i.e., nurses; Yoon & Kim, 2013). However, no previous studies have examined the association between emotional labor and depressive symptoms in call center workers. Furthermore, few studies have found an independent association between emotional labor and depressive symptoms after controlling for potential confounding factors.
In addition, musculoskeletal disorders, which are associated with job demand, constitute the most prevalent physical health problem observed in call center workers (Halford & Cohen, 2003). High psychological job demand was reported to be the strongest predictor of workers’ musculoskeletal disorders in a 1-year prospective study (Bugajska et al., 2013). In this context, emotional labor, a distinguishing psychological job demand in call centers, could be associated with work-related musculoskeletal disorders (WMSD). However, few studies have examined the association between emotional labor and WMSD. Furthermore, it is unclear whether the two types of emotional labor (i.e., surface and deep acting) exert different effects on WMSD.
The purpose of this study was to determine whether two specific types of emotional labor (i.e., surface and deep acting) were significantly and independently associated with psychological and physical health problems (i.e., depressive symptoms and WMSD) in call center workers.
Method
This study was a cross-sectional, correlational study based on a secondary analysis of data from a parent study that investigated risk factors for WMSD in call center workers between September and October 2014. Participants in the parent study were recruited from a call center that employed 1,133 workers in Seoul, South Korea. The call center was a representative service company offering inbound and outbound services related to telephones, the Internet, and desktop/laptop computers. Of the 925 participants, 274 employees comprised the final sample for the present study, after excluding employees who had worked for the company for less than 1 year (n = 393), female employees who were either pregnant or breastfeeding (n = 4), and employees who had been diagnosed with illnesses unrelated to WMSD (i.e., rheumatoid arthritis, diabetes, gout, or alcoholism; n = 201). The minimum sample size required to achieve statistical power of .80, an anticipated effect size of .15 for predictor variables on outcome variables, a Type I error rate of .05, and 13 predictors was 113 (Cohen, Cohen, West, & Aiken, 2003; Soper, 2015). The study was approved by the institutional review board at Korea University (No. 1040548-KU-IRB-14-134-A-1 [R-P-1]). All participants provided written informed consent.
Outcome Measures
Depressive symptoms were measured using the Korean version of the Center for Epidemiologic Studies Depression (CESD) scale, which was validated by Chon and Rhee (1992). The 20-item scale measured characteristic depressive symptoms and behaviors experienced during the preceding week. Each item is scored on a scale from 0 to 3 according to symptom frequency. Higher scores indicate more severe depressive symptoms. Participants with CESD scores of 16 or higher were considered to have clinical depression (Chon & Rhee, 1992). Cronbach’s α for the scale was .89 in a previous study (Chon & Rhee, 1992); Cronbach’s α for the scale was .78 for the present study.
Work-related musculoskeletal disorders was measured using the Korea Occupational Safety and Health Agency Guide, H-9-2012, based on the guidelines for musculoskeletal disorders created by the National Institute for Occupational Safety and Health (Korea Occupational Safety & Health Agency, 2012). Participants answered questions pertaining to non-specific musculoskeletal disorder symptoms (i.e., pain or discomfort related to their work) experienced in six regions of the body (i.e., neck, shoulders, arms/elbows, hands/fingers/wrists, low back, or legs/feet) during the preceding 12 months. The presence of WMSD was established by using the National Institute for Occupational Safety and Health Criteria (Hales & Sauter, 1992): (a) symptoms of pain, aching, stiffness, burning, tingling, or numbness; (b) symptoms occurred within the past year; (c) no previous accident or trauma to the symptomatic joint area; (d) symptoms occurred while working the current job; and (e) symptoms lasted for more than 1 week or occurred at least once a month.
Exposure Assessment
The Emotional Labor Scale measured participants’ emotional labor levels. The scale was originally developed by Brotheridge and Lee (2003) and translated into Korean by Lee (2006). The scale contains two dimensions (i.e., surface acting and deep acting) and six items, with responses provided using a 5-point Likert-type scale ranging from 1 (never) to 5 (always). The six items of the scale are (a) resist expressing my true feelings, (b) pretend to have emotions that I do not really have, (c) hide my true feelings about a situation, (d) make an effort to actually feel the emotions that I need to display to others, (e) try to actually experience the emotions that I must show, and (f) really try to feel the emotions I have to show as part of my job. Higher scores indicate higher levels of emotional labor. In previous studies, Cronbach’s αs for the dimensions of surface and deep acting were .79 and .83, respectively (Brotheridge & Lee, 2003). In the present study, Cronbach’s α for the dimensions of surface and deep acting were .75 and .90, respectively.
Participants’ characteristics (i.e., sociodemographic, health-related, and work-related characteristics) were collected. Specifically, physical activity that was beneficial to health was defined as engagement in any of the following (Ministry of Health and Welfare & Korea Centers for Disease Control and Prevention, 2013) during the preceding week: (a) vigorous intensity activity on at least 3 days for at least 20 minutes/day, (b) moderate intensity activity on at least 5 days for at least 30 minutes/day, or (c) walking on at least 5 days for at least 30 minutes/day. Work intensity was calculated using “perceived workload” multiplied by “frequency of work.” Perceived workload was assessed via the question, “How do you feel about your workload in your current work environment?” Participants responded using a 5-point scale ranging from 1 (very easy) to 5 (very burdensome). Work frequency was assessed via the question, “How do you feel about work frequency in your current work environment?” Participants responded using a 5-point scale: 1 (1-2 times every 2 months), 2 (2-3 days/week), 3 (4 hours/day), 4 (4-8 hours/day), and 5 (>8 hours/day).
Data Analysis
Data were analyzed using IBM SPSS Version 21 (IBM Co., Armonk, New York, USA). The significance level was set at p < .05. Multiple regression analysis was used to examine the association between emotional labor (i.e., surface and deep acting) and depressive symptoms. Logistic regression analysis was used to examine the association between emotional labor and WMSD. The following three regression models were created to test study hypotheses: (a) a crude model without any adjustment for covariates, (b) an adjusted Model 1 for covariates, and (c) an adjusted Model 2 for the covariates plus the variable of either deep acting labor or surface acting labor. Covariates were selected based on previous literature with a cutoff point of p < .20 based on the results of crude associations with the outcome variables. All categorical covariates were coded dichotomously prior to inclusion in the regression models.
Results
Participants’ (n = 274) mean age was 36.5 years. In addition, 74.1%, 48.5%, and 51.3% of participants were women, married, and educated to high school diploma level or less, respectively (Table 1). Their mean body mass index (BMI) was 22.8 kg/m2. Furthermore, 21.9%, 59.1%, and 59.9% of participants were current smokers, consumed alcohol at least once per month, and participated in physical activity for health benefits, respectively. Of total participants, 84.3% had regular employment. Participants’ mean duration of employment was 74.4 months, and their mean daily work time was 8.4 hours. Their mean work intensity score was 15.4 (range = 1-25), their mean surface and deep acting scores were 3.4 and 3.5 (range = 1-5), respectively, and their mean CESD score was 13, which represents a 31% risk of clinical depression.
Participants’ General Characteristics (N = 274)
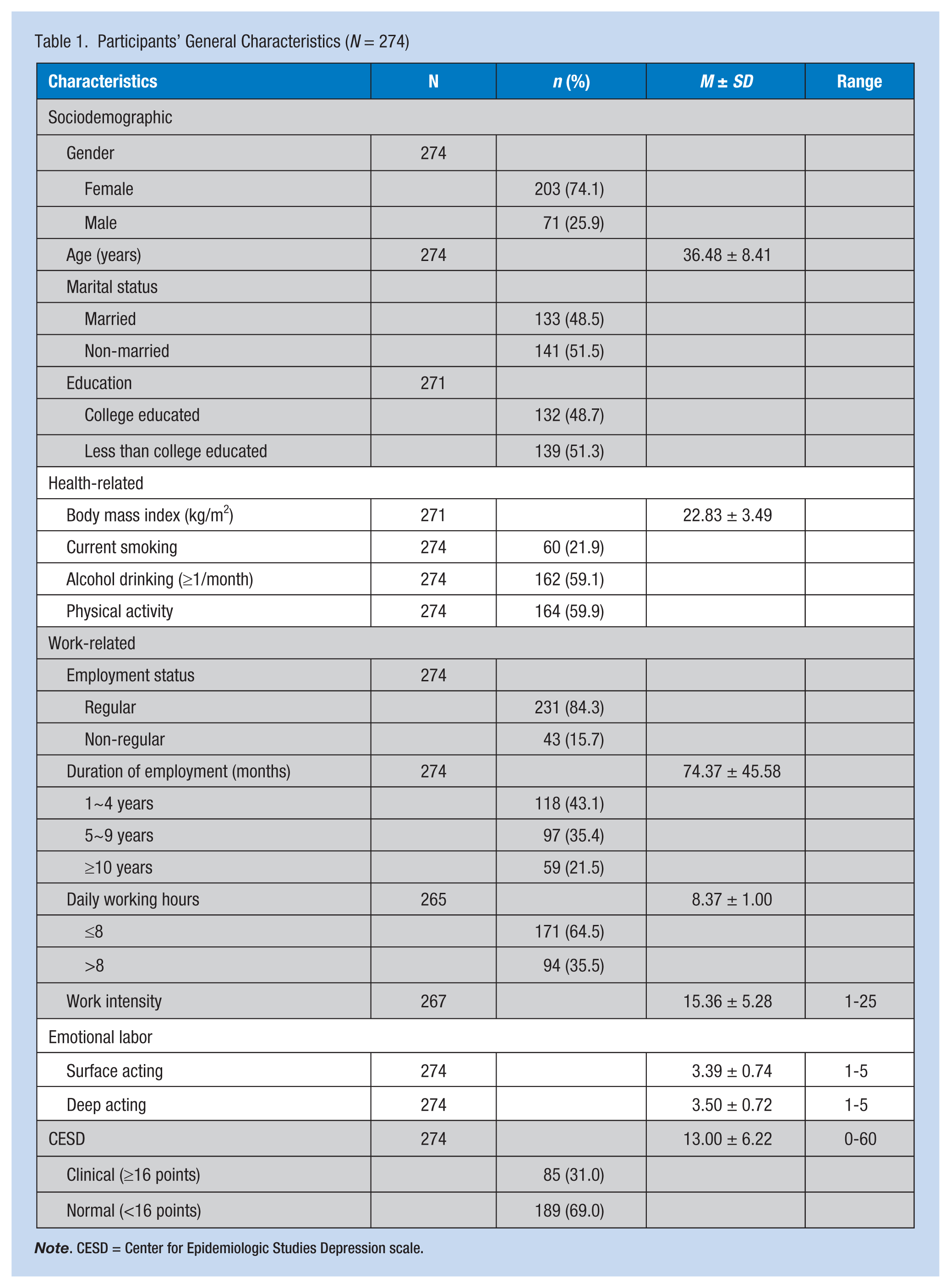
Note. CESD = Center for Epidemiologic Studies Depression scale.
Presence of WMSD
Of all participants, 45.6% reported WMSD in any part of the body (Figure 1). The largest group of participants reported WMSD in their shoulders (35.8%), followed by WMSD in hands/wrists/fingers (22.6%), low back (21.9%), and neck (20.1%).
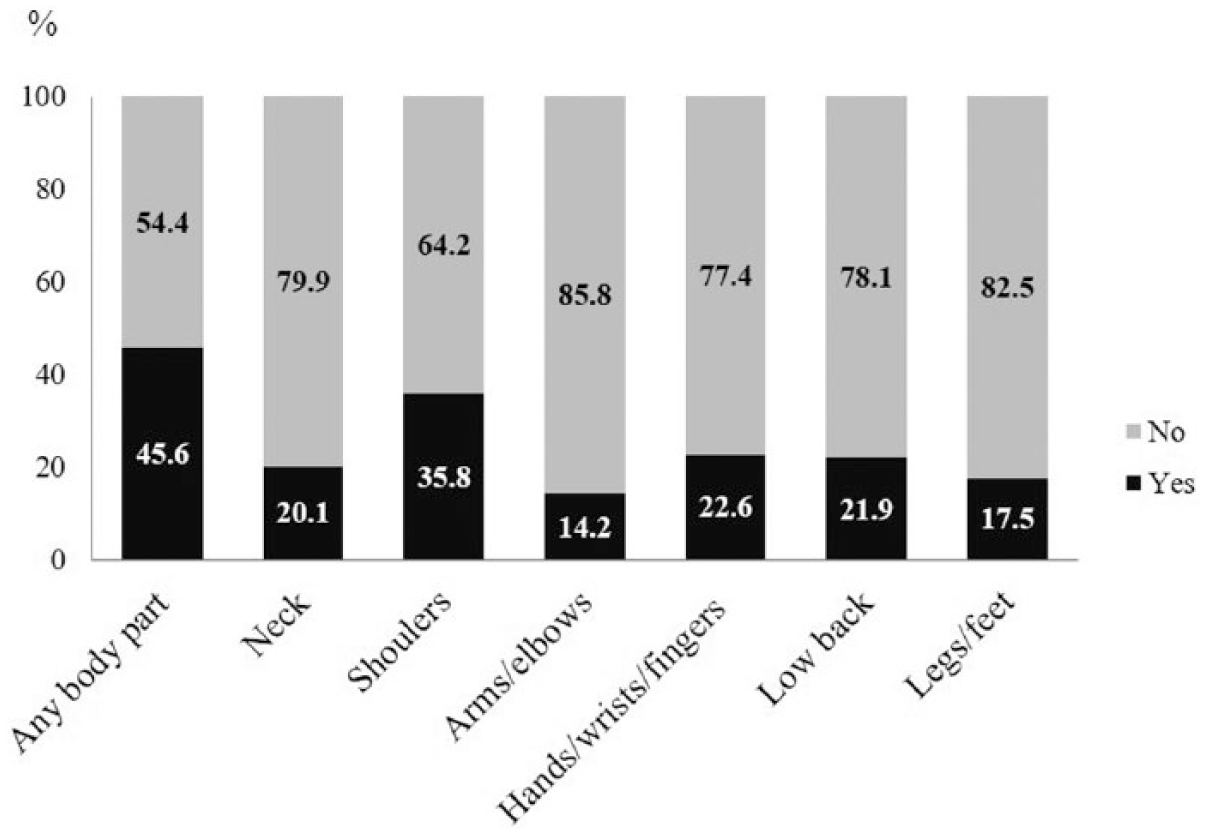
Prevalence of WMSD in call center workers (N = 274) according to National Institute for Occupational Safety and Health Criteria.
Associations Between General Characteristics and WMSD
Female workers were more likely to experience WMSD in any part of the body (odds ratio [OR] = 2.29, 95% confidence interval [CI] [1.29, 4.07]), the shoulders (OR = 3.61, 95% CI [1.83, 7.14]), or the hands/wrists/fingers (OR = 2.43, 95% CI [1.13, 5.24]; Table 2). Unmarried workers were more likely to report WMSD in the low back (OR = 1.86, 95% CI [1.03, 3.36]). Stronger work intensity was significantly associated with WMSD in any part of the body (OR = 1.07, 95% CI [1.02, 1.12]), the shoulders (OR = 1.06, 95% CI [1.01, 1.12]), the arms/elbows (OR = 1.08, 95% CI [1.01, 1.16]), the low back (OR = 1.08, 95% CI [1.02, 1.14]), and the legs/feet (OR = 1.07, 95% CI [1.01, 1.14]).
Associations Between General Characteristics and WMSD in Call Center Workers (N = 274)
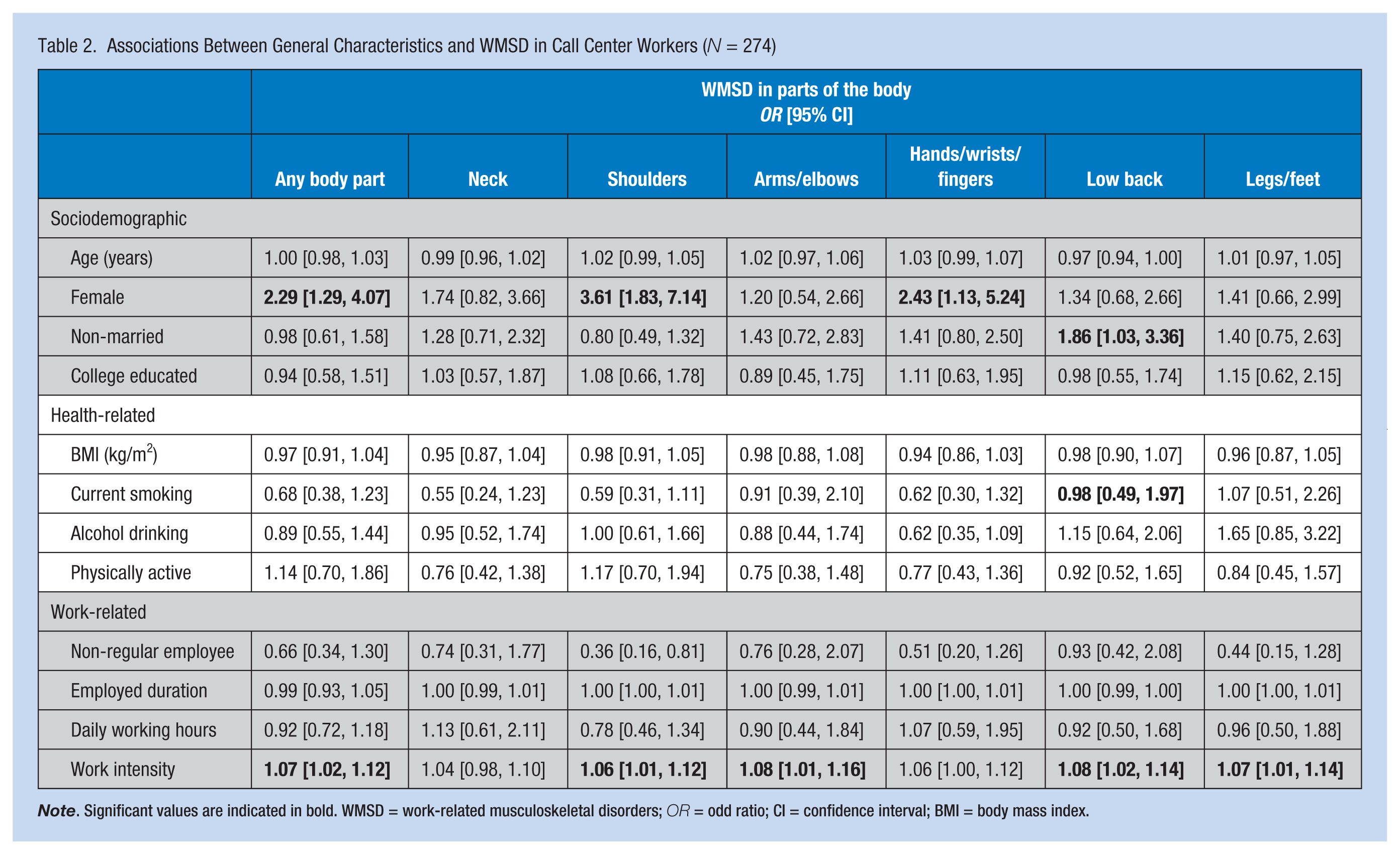
Note. Significant values are indicated in bold. WMSD = work-related musculoskeletal disorders; OR = odd ratio; CI = confidence interval; BMI = body mass index.
Associations Between Emotional Labor and Depressive Symptoms
In the crude model, higher surface acting was significantly associated with higher CESD scores (β = .35, p < .001; Table 3); this association remained significant in the adjusted Models 1 and 2 (β = .32, p < .001 in adjusted Model 1; β = .32, p < .001 in adjusted Model 2). However, deep acting was not significantly associated with CESD scores in any of the regression models.
Associations Between Emotional Labor and Depressive Symptoms and WMSD in Call Center Workers (N = 274)
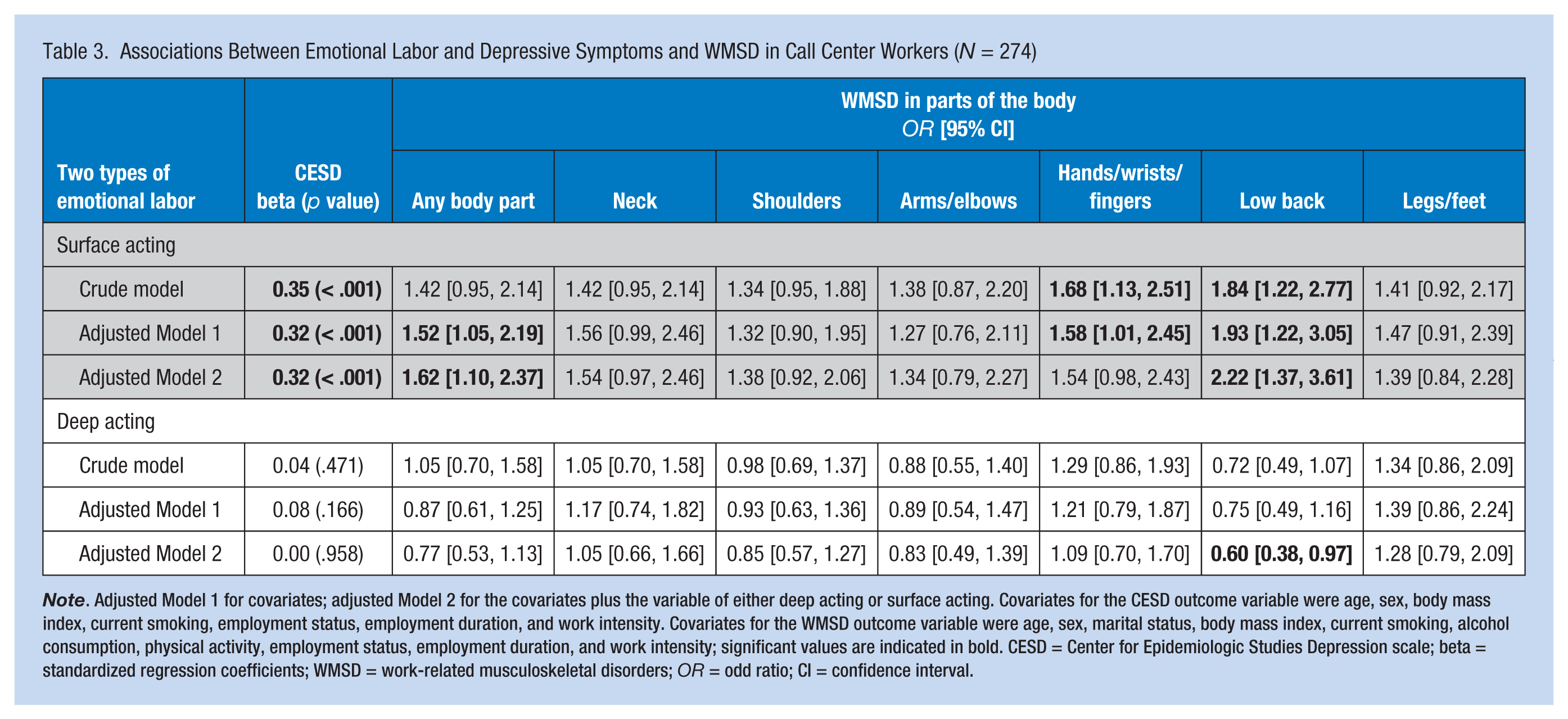
Note. Adjusted Model 1 for covariates; adjusted Model 2 for the covariates plus the variable of either deep acting or surface acting. Covariates for the CESD outcome variable were age, sex, body mass index, current smoking, employment status, employment duration, and work intensity. Covariates for the WMSD outcome variable were age, sex, marital status, body mass index, current smoking, alcohol consumption, physical activity, employment status, employment duration, and work intensity; significant values are indicated in bold. CESD = Center for Epidemiologic Studies Depression scale; beta = standardized regression coefficients; WMSD = work-related musculoskeletal disorders; OR = odd ratio; CI = confidence interval.
Associations Between Emotional Labor and WMSD
In the crude models, higher levels of surface acting were significantly and positively associated with WMSD in the hands/wrists/fingers (OR = 1.68, 95% CI [1.13, 2.51]) and low back (OR = 1.84, 95% CI [1.22, 2.77]; Table 3). In the adjusted Model 1, higher levels of surface acting remained significantly associated with WMSD in the hands/wrists/fingers (OR = 1.58, 95% CI [1.01, 2.45]) and low back (OR = 1.93, 95% CI [1.22, 3.05]). In the adjusted Model 2 (further adjusted for deep acting), higher levels of surface acting remained significantly associated with WMSD in the low back (OR = 2.22, 95% CI [1.37, 3.61]) but were not significantly associated with WMSD in the hands/wrists/fingers.
In the crude models, higher levels of deep acting were not significantly associated with WMSD in any part of the body; these non-significant associations remained in adjusted Model 1 (Table 3). However, in adjusted Model 2 (further adjusted for surface acting), higher levels of deep acting were significantly and inversely associated with WMSD in the low back (OR = 0.60, 95% CI [0.38, 0.97]).
Discussion
In this study, emotional labor was linked to depressive symptoms and WMSD in call center workers. Higher levels of surface, but not deep, acting were significantly associated with higher levels of depressive symptoms. Furthermore, higher levels of surface acting were significantly and positively associated with WMSD in the low back; higher levels of deep acting were significantly and inversely associated with WMSD in the low back.
In the present study, levels of surface, but not deep, acting were significantly and positively associated with depressive symptoms. The finding was consistent with findings of previous studies (Lee, 2006; Schmidt & Diestel, 2014; Yoon & Kim, 2013). Schmidt and Diestel (2014) also reported that surface, but not deep, acting was positively correlated with depressive symptoms in nurses. However, the researchers did not control for covariates that could have confounded the relationship between emotional labor and depressive symptoms (e.g., work intensity). Therefore, the present study demonstrated an independent association between emotional labor and depressive symptoms, a well-known psychological health problem.
The results also showed that higher levels of surface acting were significantly associated with WMSD in the low back. In contrast, higher levels of deep acting were significantly associated with absence of WMSD in the low back. Yoo, Choi, Song, and Lee (2011) reported that civil-affairs officials with high levels of emotional labor were 2.57 times more likely to report WMSD than those with low levels of emotional labor. However, they did not differentiate between surface and deep acting and their associations with WMSD. To the best of the authors’ knowledge, this study was the first to report differentiated associations of surface and deep acting with WMSD.
The association between surface acting and low back pain could be explained by emotional suppression and neglect. Unlike deep acting, surface acting is a response-focused form of emotion regulation (Grandey, 2000; Gross, 1998). Call center workers manipulate their emotions, via suppression or pretense, according to customer need. Previous studies showed that individuals who suppressed their emotions exhibited greater sympathetic activation (Gross, 1998; Rohrmann, Bechtoldt, Hopp, Hodapp, & Zapf, 2011), which could be associated with chronic musculoskeletal pain (Hallman, Lindberg, Arnetz, & Lyskov, 2011). In addition, Mehling and Krause (2005) reported that public transit operators who lacked emotional awareness (i.e., neglecting feelings) were 2.23 times more likely to report low back pain than those operators who did not lack emotional awareness. Therefore, the association between surface acting and low back pain observed in call center workers could be explained by sympathetic activation induced by suppression of emotion during the process of surface acting.
Study findings showed that deep acting was significantly and inversely associated with WMSD in the low back, after further adjustment for a more sophisticated component of surface acting. Although the mechanism via which deep acting exerts a protective effect against WMSD is unclear, the link has practical implications, as it suggests that occupational health nurses must address this issue in the workplace. In other words, occupational health nurses should teach workers effective coping strategies to enhance deep acting in emotional labor.
The present study has limitations. First, because of the cross-sectional design, the researchers were unable to infer a causal association between emotional labor and WMSD (or depressive symptoms). Prospective cohort studies should be conducted in the future. Second, data for the assessment of WMSD were collected via questionnaire and could therefore have been subject to recall bias. Furthermore, the generalizability of the results to other ethnicities or employees from other types of workplaces is limited.
Implications for Practice
The results of the present study showed that emotional labor was linked to adverse psychological and physical health outcomes (i.e., depressive symptoms and WMSD related to low back pain) in call center workers. Most importantly, the two types of emotional labor exerted different effects. Surface acting exerted harmful effects with respect to depressive symptoms and WMSD, and deep acting exerted a protective effect against WMSD. In this context, surface acting should be discouraged in call center workers to reduce the occurrence of depressive symptoms and WMSD, and deep acting should be encouraged to reduce the occurrence of WMSD. These findings could be used by occupational health nurses to delineate differentiated strategies according to the nature of surface and deep acting to promote psychological and physical health in call center workers. Moreover, occupational health nurses should identify individual and organizational factors that influence surface and deep acting with call center workers and employers, and then develop a comprehensive intervention involving changes at individual and organizational levels to modify and eliminate these factors for call center workers.
In this study, emotional labor was linked to adverse psychological and physical health outcomes (i.e., depressive symptoms and work-related musculoskeletal disorders [low back pain]) in call center workers. Most importantly, the two types of emotional labor exerted different effects; surface acting exerted harmful effects with respect to depressive symptoms and WMSD, and deep acting exerted a protective effect against WMSD. In this context, surface acting should be discouraged in call center workers to reduce depressive symptoms and WMSD, and deep acting should be encouraged to reduce WMSD. Study findings could assist occupational health nurses to delineate differentiated strategies according to the nature of surface and deep acting to promote the psychological and physical health of call center workers. Moreover, occupational health nurses should identify individual and organizational factors that influence surface and deep acting among call center workers, and then develop a comprehensive intervention to change individual workers and the organization to modify or eliminate surface acting among workers in call centers.
Footnotes
Conflict of Interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Author Biographies
Hye-Jin Kim is a graduate student in the PhD program at Korea University College of Nursing. She has a certificate of advanced occupational health nursing and approximately 10 years professional experience as an occupational health nurse.
Jina Choo is an associate professor of community health nursing at the College of Nursing, Korea University. She has been an executive member of the Korean Academic Society of Occupational Health Nursing since 2011.