
Abstract
Background:
Depression is the second leading cause of disability worldwide. Health care workers report a higher prevalence of depressive symptoms than the general population. Emotional labor has contributed to poor health and work outcomes. However, the mechanism for the potential association between emotional labor and depressive symptoms has not been well studied. This study examines the relationship between emotional labor and depressive symptoms and whether sleep plays a role in explaining this relationship.
Methods:
In 2018, health care workers (n = 1,060) from five public sector facilities in the northeast United States participated in this cross-sectional survey. The survey included questions on participants’ surface-acting emotional labor (masking one’s feelings at work), depressive symptoms, sleep duration and disturbances, and socio-demographic characteristics. Multivariable linear and Poisson regression modeling were used to examine associations among variables.
Findings:
There was a significant association between emotional labor and depressive symptoms (β = 0.82, p < .001). Sleep disturbances, but not short sleep duration, partially mediated this association. Neither sleep variable moderated this association.
Conclusions/Application to Practice:
Depressive symptoms were prevalent among health care workers and were associated with emotional masking. Sleep disturbances play an important intermediate role in translating emotional labor to depressive symptoms in these workers. Effective workplace programs are needed to reduce health care workers’ emotional labor to improve their mental health. Sleep promotion should also be emphasized to mitigate the negative effect of emotional labor and promote mental wellbeing.
Background
Health care is one of the largest sectors in the United States, employing over 16 million workers, who constitute 11% of the U.S. labor force (Bureau of Labor Statistics, 2018). Numerous physical and psychosocial stressors have been reported in the health care work environment, including shift work and extended hours, chemical and biological hazards, excessive workload, workplace violence, and so on (Centers for Disease Control and Prevention, 2017; Occupational Safety and Health Administration, 2021). All of these contribute to the poor physical and mental health of these workers, such as musculoskeletal disorders, chronic diseases, sleep deficiency, burnout, and depression (Mohanty et al., 2019; Weaver et al., 2018).
Depression is the second leading cause of disability worldwide, contributing to an overall global burden of disease (World Health Organization, 2020). Previous studies have reported a link between depression and poor health behaviors such as smoking, alcohol and substance use, unhealthy diet, and sedentary behaviors (Ruggles et al., 2017; Saneei et al., 2016). Depression is also linked to health outcomes such as musculoskeletal disorders, cardiovascular diseases, diabetes, and all-cause mortality (Bădescu et al., 2016; Del Campo et al., 2017; Machado et al., 2018; Penninx, 2017). In general, nurses and other health care workers report a higher rate of depressive symptoms than the general population, leading to a high incidence of low job satisfaction, burnout, absenteeism, and turnover (Khamisa et al., 2015; Letvak et al., 2012; Weaver et al., 2018).
Work stress, a strong predictor of poor mental health outcomes, has been reported in health care workers including physicians, nurses, and other professionals (Koinis et al., 2015; Lin et al., 2016; Rogers et al., 2014). According to the job demand-control-support model (Karasek & Theorell, 1990), workers who have high job demands (sustained physical and/or psychological effort), low job control (ability to influence decisions), and low social support (assistance from coworkers and/or supervisors) are at a particular high risk for work stress and depressive symptoms (Freimann & Merisalu, 2015; Topp et al., 2015).
Emotional labor, a process of managing feelings and expressions to fulfill the emotional requirements of a job, is a requirement for health care workers during interactions with patients, and sometimes also with coworkers and supervisors (Grandey, 2000; Hochschild, 2012). Generally, emotional labor consists of two primary regulation strategies: Surface acting and deep acting. Surface acting involves masking the actual emotions, for example, using fake smiles to hide one’s true feelings. Deep acting involves putting efforts into actually feeling and expressing the required emotions, for example, modifying feelings to match the situation (Hochschild, 2012). More harmful outcomes to employee health have been reported from surface acting than deep acting (Hülsheger & Schewe, 2011; Qi et al., 2017).
Emotional labor has contributed to poor health outcomes such as musculoskeletal disorders and depression (Kim & Choo, 2017), as well as negative work outcomes such as low job satisfaction and burnout, among employees in carework and other service jobs (Jeung et al., 2018; Psilopanagioti et al., 2012; Roh et al., 2016; Wi & Yi, 2012). Work-family conflict and self-efficacy may mediate between emotional labor and negative consequences such as burnout and poor well-being (Noor & Zainuddin, 2011; Sloan, 2014). In the health care settings, the link between emotional labor and depressive symptoms has been studied among nurses and doctors (Rogers et al., 2014; Yoon & Kim, 2013). Surfacing-acting emotional labor has been reported as a significant contributor to depressive symptoms among health care workers (Suh & Punnett, 2020; Yoon & Kim, 2013).
The mechanisms for the effect of emotional labor on depression are not well understood. In particular, there has been no study examining the role of health behaviors such as sleep on this association, even though sleep is known to play a critical part in mental wellness. Only one potentially relevant study has been identified, showing that day-specific sleep quality attenuated the influence of emotional dissonance on psychological well-being (Diestel et al., 2015). As we know, health care workers are at risk for short sleep duration and sleep disturbances (Hulsegge et al., 2019). Insufficient sleep may be associated with emotional labor (McGinley & Wei, 2020). In addition, short and poor sleep contribute to depression (Tsuno et al., 2005; Zhai et al., 2015; Zhang et al., 2017a, 2017b). Therefore, it is reasonable to postulate that sleep may play a mediating or moderating role in the association between emotional labor and depressive symptoms among health care workers.
The objectives of this study were (a) to examine the relationship between emotional labor and depressive symptoms among health care workers and (b) to explore the role of sleep duration and disturbances in explaining the relationship between emotional labor and depressive symptoms among these workers.
Methods
Setting and Subjects
As part of a larger research study of health care workers, information was collected on employees’ work and health in five facilities in the northeast United States, including two mental health hospitals and three veterans’ facilities providing a mix of acute and residential care (Punnett et al., 2020). All facilities were managed by the State or Federal government and all workforces were unionized. This study used the baseline cross-sectional survey collected from a sample of 1,060 health care worker between January and June 2018. All full-time, part-time, and per-diem employees over 18 years old and hired directly by these facilities were eligible to participate.
Measurements
Depressive symptoms
Depressive symptoms were assessed with the 10-item version of the Center for Epidemiologic Studies Depression Scale (CES-D) (Andresen et al., 1994; Rodolff, 1977). Each item is rated on a 4-point Likert-type scale (0 = rarely or none of the time, 1 = some or a little of the time, 2 = occasionally or a moderate amount of the time, and 3 = most or all of the time) with a total score ranging from 0 to 30. Higher scores indicate greater severity, and a total score of 10 or more is considered indicative of depression in people aged 18 and older (Andresen et al., 1994). The scale demonstrated good reliability for the study sample (Cronbach’s alpha = .75).
Emotional labor
Emotional labor was assessed with 3 items selected from Brotheridge and Grandey (2002). The three items measured surface-acting emotional labor by asking on an average day at work, how frequently do participants (a) resist expressing their true feelings; (b) pretend to have emotions that they do not usually have; and (c) hide their true feelings about a situation. Each item is rated on a 5-point Likert-type scale (1 = never, 2 = rarely, 3 = sometimes, 4 = often, and 5 = always). The three items were averaged, with higher scores indicating more emotional labor. The scale demonstrated very good reliability for the study sample (Cronbach’s alpha = .85).
Sleep duration
Sleep duration was assessed with one item asking participants’ typical amount of sleep per 24-hr period during the work week (5 hr or less; 6 hr; 7 hr; 8 hr; 9 hr; and 10 hr or more). Sleep duration was dichotomized as >6 hr per day, versus ≤6 hr per day (short sleep duration) for these analyses (Qiu et al., 2012).
Sleep disturbances
The PROMIS Sleep Disturbance Short Form (SD-SF) uses 8 items to assess the severity of sleep disturbances in individuals aged 18 and older (Yu et al., 2012). Each item was rated on a 5-point Likert-type scale; the sum ranges in total raw score from 8 to 40 and a higher score indicates greater severity. We calculated a T-score from the total raw score, with a range from 28.9 to 76.5 based on the instrument scoring manual. The T-score was categorized as mild (55.0–59.9), moderate (60.0 -69.9), or severe (70.0 and over) sleep disturbances (Yu et al., 2012). Sleep disturbances were dichotomized as no (<55) or yes (≥55) for these analyses. The scale demonstrated very good reliability for this study sample (Cronbach’s alpha = .89).
Socio-demographics
The questionnaire collected age, gender, race, height, weight, job title, current job tenure (how long working in the same facility), and responsibility for children and other dependents. Body mass index (BMI) was calculated from self-reported weight and height, expressed as weight/height2 and categorized as normal (<25 kg/m2), overweight (25.0–29.9 kg/m2), or obese (≥30.0 kg/m2) (Centers for Disease Control and Prevention, 2015). Job title was dichotomized as direct care (including doctors, nurses, nursing assistants, mental health workers, social workers, first responders, and rehabilitation staff) or non-direct care jobs (including lab, housekeeping, dietary, facility, orderly, and office/administrative staff).
Working conditions
A wide range of work environment descriptors included usual work shift (days, evenings, nights, and rotating), weekly work hours, and weekly overtime hours; as well as physical demands, psychological demands, decision latitude, social support, work-family conflict, workplace safety, bullying, and assaults at work. These working conditions were selected as covariates for the study analyses because they are common work stressors experience by health care workers (Centers for Disease Control and Prevention, 2017; Occupational Safety and Health Administration, 2021). Furthermore, previous studies have reported their associations with mental health outcomes in health care workers (Freimann & Merisalu, 2015; Koinis et al., 2015; Lin et al., 2016; Mento et al., 2020; Zhang et al., 2016, 2016a, 2017b).
Physical demands (5 items), psychological demands (2 items), decision latitude (6 items), and social support (4 items) items were selected from the subscales of the Job Content Questionnaire (JCQ) (Karasek et al., 1998) and assessed with a 4-point Likert-type scale (1 = strongly disagree, 2 = disagree, 3 = agree, and 4 = strongly agree). The JCQ subscales demonstrated good validity and acceptable reliability in large study populations from six countries (Karasek et al., 1998). The Cronbach’s alpha coefficients of these subscales were good at .88 (physical demands), .61 (psychological demands), .71 (decision authority), and .75 (social support) for this study sample, which were similar to their reliabilities reported in a previous study with nursing assistants (Zhang et al., 2016b).
Work-family conflict was assessed from inter-role conflict, measured with 4 items selected from (Frone et al., 1992). The scale demonstrated good reliability for this study sample (Cronbach’s alpha = .77). Participants’ perceived safety on their current job in the facility was measured with 7 items selected from the CPH-NEW All Employee Survey (Center for the Promotion of Health in the New England Workplaces, 2020). The scale demonstrated very good reliability for this study sample (Cronbach’s alpha = .86). Negative behaviors at work were assessed with 6 items from the Negative Acts Questionnaire-Revised which covers being humiliated or ridiculed, ignored or shunned, insulted, shouted at or targeted, intimidated with threatening behaviors, or being the subject of excessive teasing and sarcasm in the past six months (Einarsen et al., 2009). This variable was dichotomized as yes (any) or no (none) for these analyses. Assaults at work were measured with 3 items asking about participants’ experience of physical hurt or assaults including being hit, slapped, punched, kicked, strangled, and so on, in the past 6 months (Amuwo et al., 2011). This variable was also dichotomized as yes (any) or no (none) for these analyses.
Data Collection
The research team distributed and collected the questionnaires at each facility over a 2 to 5-day period to accommodate employees working at different shifts and units. The team members explained the study purpose and procedure, potential benefits and risks, and protection of confidentiality to participants. Although employees were given the option to take home the questionnaires to complete in private, most completed questionnaires during break times and returned them in person. Compensation of $10 was offered for each completed questionnaire with a consent form. The study was approved by the University of Massachusetts Lowell Institutional Review Board (No. 16-131-PUN-XPD).
Data Analysis
All statistical analyses were completed using the SPSS software 26.0. Emotional labor and depressive symptoms were treated as continuous, while sleep duration and disturbances were treated as dichotomous variables. The associations of socio-demographics and working conditions with emotional labor and depressive symptoms were examined using Independent Samples t-Test (for means of two independent groups), ANOVA (means of three or more independent groups), and Spearman correlation coefficients (for variables that are not continuous or not normally distributed) (Field, 2013). Multivariable linear regression modeling was used to calculate coefficients and 95% confidence intervals (CI) for depressive symptoms (continuous). The prevalence of sleep disturbances and short sleep duration were both over 10%. Poisson regression modeling with robust variance estimates was therefore used to calculate prevalence ratios (PR) and 95% CI because it is more conservative and accurate than logistic regression modeling (Barros & Hirakata, 2003). Multicollinearity assumptions were checked using Variance Inflation Factors (VIF) to quantify how much the variance is inflated in the multivariable linear regression models (Field, 2013). Socio-demographics and working conditions were adjusted as covariates in the multivariable regression models using the change-in-estimate criterion (Greenland, 1989), defined as 10% change in the coefficient of emotional labor in the model.
Baron and Kenny’s method (Baron & Kenny, 1986) was used to assess the potential mediating effect of sleep disturbances or duration on the association between emotional labor and depressive symptoms by evaluating four criteria: (a) emotional labor association with depressive symptoms, (b) emotional labor association with sleep disturbances (or duration), (c) sleep disturbances (or duration) association with depressive symptoms; and (d) attenuation of the association between emotional labor and depressive symptoms with inclusion of sleep disturbances (or/and duration).
To assess the potential moderating effect of sleep disturbances or duration, the interaction of sleep disturbances (yes vs. no) or sleep duration (≤6 vs. >6 hr/day) with emotional labor was introduced into the multivariable linear regression models after the main effects and tested for statistical significance.
Results
Descriptive and Correlation Analyses
A total of 1,060 among 2,776 health care workers employed in these five facilities completed the survey (response rate of 38%), with an average age of 47 years (Table 1). More than three-fourths were overweight or obese, and 72% reported working day shifts. Over a half were involved in direct care, including doctors, nurses, nursing assistants, mental health workers, social workers, first responders, and rehabilitation staff. Over one-half reported negative behaviors at work and over one-fourth reported assaults at work in the past 6 months. Nearly one-quarter reported depressive symptoms (CES-D ≥ 10), while short sleep duration (over one-half) and sleep disturbances (nearly one-third) were even more common.
Socio-Demographics, Working Conditions, Emotional Labor, Sleep, and Depressive Symptoms Among Health Care Workers (N = 1,060)
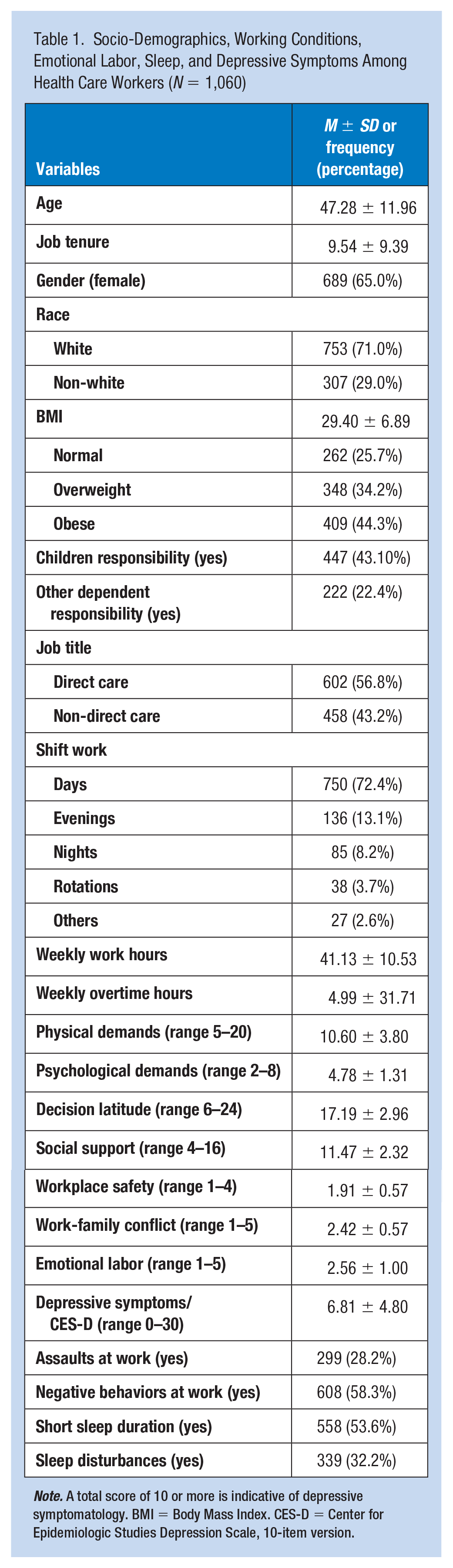
Note. A total score of 10 or more is indicative of depressive symptomatology. BMI = Body Mass Index. CES-D = Center for Epidemiologic Studies Depression Scale, 10-item version.
Depression scores were higher if employees reporting higher emotional labor (p < .01), as well as higher physical demands (p < .01), psychological demands (p < .01), social support (p < .01), work-family conflict (p < .01), negative behaviors at work (p < .01), assaults (p < .01), and more weekly overtime hours (p < .05); but lower decision latitude (p < .01) and workplace safety (p < .01). Younger and white workers had higher depression scores than older (p < .01) and non-white (p < .01) ones.
Employees reported higher emotional labor when they also experienced higher psychological demands (p < .01), work-family conflict (p < .01), negative behaviors at work (p < .01), assaults (p < .01), and more weekly work hours (p < .05), but lower decision latitude (p < .01), social support (p < .01), and workplace safety (p < .01).
Direct care employees reported more physical demands (p < .001), decision latitude (p < .05), workplace safety (p < .001), and work-family conflict (p < .01), more weekly overtime hours (p < .05), working more evening and night shifts (p < .001), and more prevalence of negative behaviors (p < .01), assaults (p < .001), and short sleep duration (p < .05). Older employees reported lower prevalence of short sleep duration (p < .01), while female employees reported higher prevalence of sleep disturbances (p < .05). Non-white employees reported less emotional labor (p < .01), but higher prevalence of short sleep duration (p < .01) (Table 2).
Associations of Selected Demographic Characteristics With Emotional Labor and Sleep.
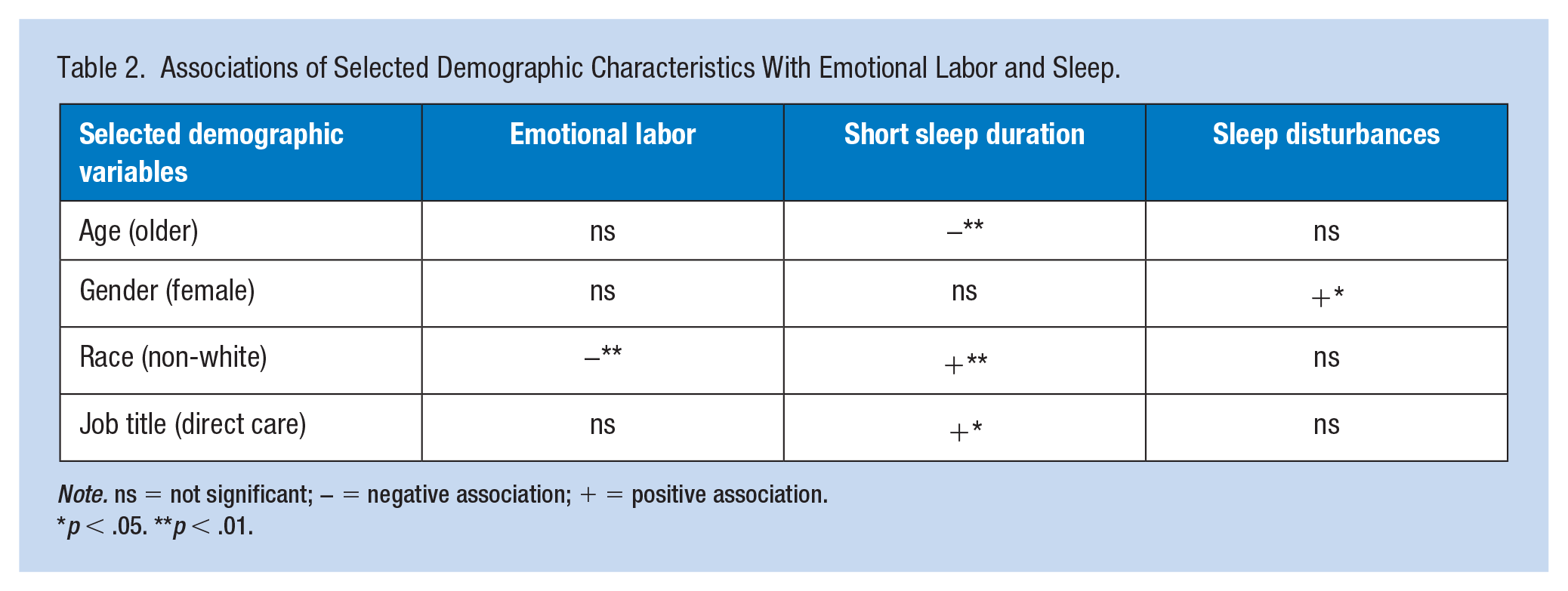
Note. ns = not significant; − = negative association; + = positive association.
p < .05. **p < .01.
Multivariate Analyses
Multivariable linear regression model of emotional labor and depressive symptoms was adjusted for social support, work family conflict, and negative behaviors at work (Table 3). Variance Inflation Factor (VIF) ranges from 1.11 to 1.38, indicating non-multicollinerity. There was a significant association between emotional labor and depressive symptoms. With every unit increase of the emotional labor score, the depressive symptoms score increased by 0.88 units (Table 3, Model 1).
Multivariate Linear and Poisson Regression Models for Emotional Labor, Sleep, and Depressive Symptoms among Health Care Workers.
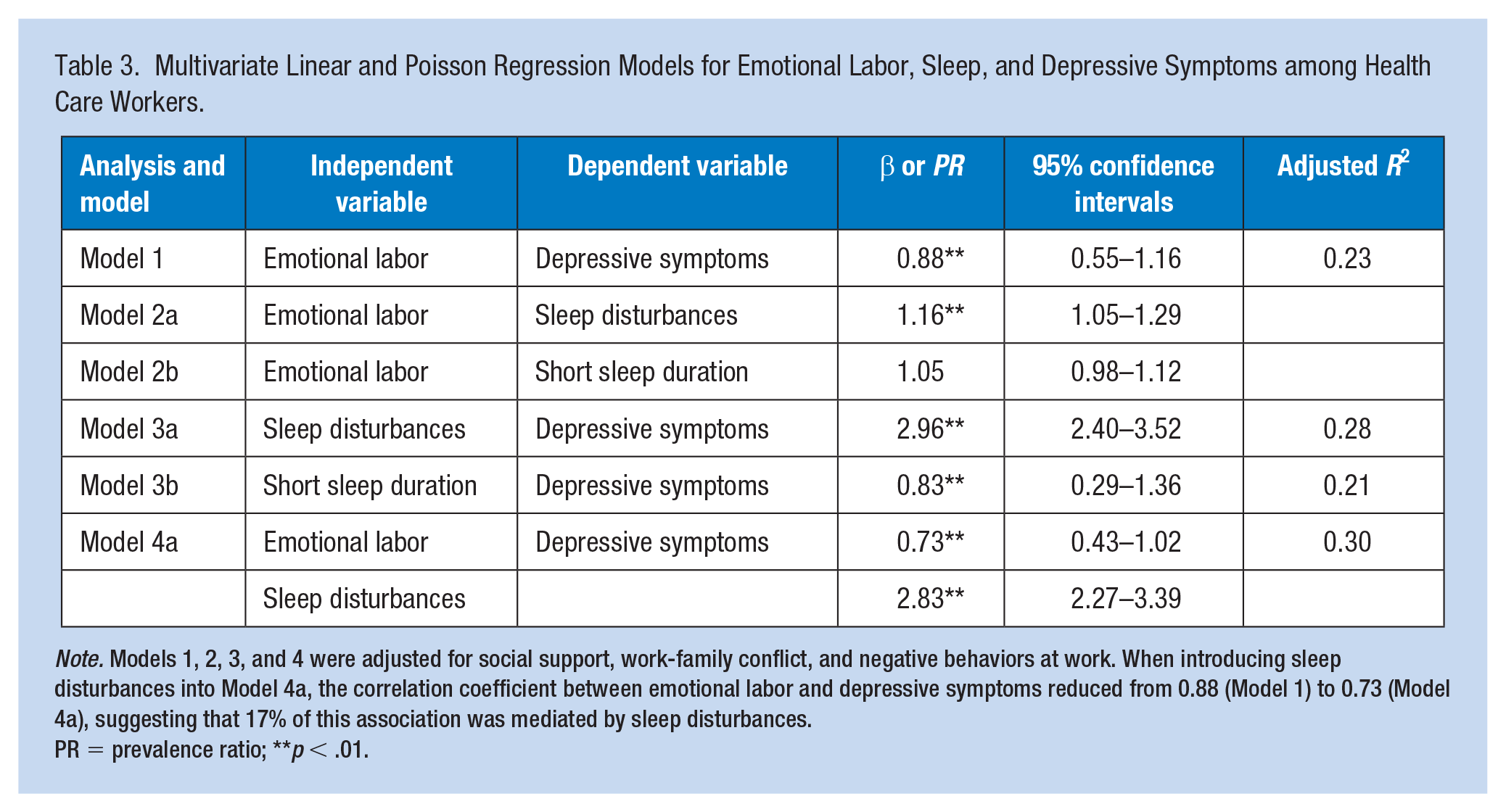
Note. Models 1, 2, 3, and 4 were adjusted for social support, work-family conflict, and negative behaviors at work. When introducing sleep disturbances into Model 4a, the correlation coefficient between emotional labor and depressive symptoms reduced from 0.88 (Model 1) to 0.73 (Model 4a), suggesting that 17% of this association was mediated by sleep disturbances.
PR = prevalence ratio; **p < .01.
In the multivariable Poisson and linear regression models, there were significant associations between emotional labor and sleep disturbances (Table 3, Model 2a), and between sleep disturbances and depressive symptoms (Model 3a), after adjustment for covariates (Table 3). After introducing sleep disturbances into the model (Model 4a), emotional labor remained a significant association with depressive symptoms. Sleep disturbances were associated with depressive symptoms and partially attenuated this association by 17.0%. The mediating role of sleep disturbances between emotional labor and depressive symptoms is shown in Figure 1.
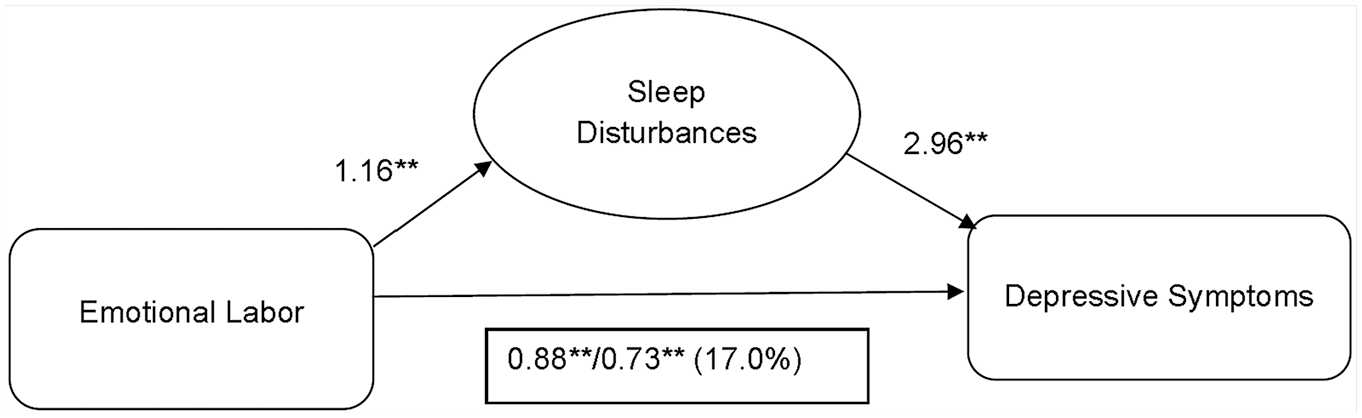
Sleep disturbances mediate the association between emotional labor and depressive symptoms.
Although the association between short sleep duration and depressive symptoms was significant (Table 3, Model 3b), the association between emotional labor and short sleep duration was not significant (Model 2b), after adjustment for covariates. Therefore, short sleep duration was not considered as a mediator or moderator in the association between emotional labor and depressive symptoms.
In the multivariable linear regression model with emotional labor and sleep disturbances as main effects, the interaction between emotional labor and sleep disturbances was not statistically significant (β = 0.21, 95% CI: -0.33, 0.74, p = .46), indicating that sleep disturbances did not modify this association.
Discussion
In this study of 1,060 mixed-occupation health care workers, nearly a quarter reported depressive symptoms over the past week. This prevalence is higher than in the U.S. general population (Centers for Disease Control and Prevention, 2013) and also higher than that in one random sample of hospital nurses (Letvak et al., 2012). Over one-half of the study participants reported short sleep duration (≤6 hr per day) and nearly a third had sleep disturbances. These prevalence values were similar to those in a sample of hospital nurses (Zhang et al., 2018).
Surface-acting emotional labor was positively associated with depressive symptoms; this relationship has also been found previously (Rogers et al., 2014; Yoon & Kim, 2013). Suh and Punnett reported that surface-acting emotional labor strongly predicted depressive symptoms 2 years later among health care workers at nursing homes (Suh & Punnett, 2020). Rogers and colleagues found positive associations among surface-acting emotional labor, work-related burnout, and depressive symptoms among Australian doctors, in contrast to a negative association between deep-acting emotional labor and burnout. The authors also suggested work-related burnout as a mediator between surface-acting emotional labor and depressive symptoms (Rogers et al., 2014). Two studies have reported negative associations between surface-acting emotional labor and job satisfaction, one of physicians in Greece (Psilopanagioti et al., 2012) and another of social workers in health care settings in the United States (Roh et al., 2016).
As expected, we found that sleep disturbances were associated with both emotional labor and depressive symptoms. However, short sleep duration was associated with depressive symptoms but not emotional labor. Sleep duration is largely dependent on time availability, which is affected by the limited amount of resources to allocate to activities associated with life domains such as work, family, and sleep. Therefore, it is understandable that emotional labor has more effect on sleep quality than quantity, but both sleep domains have significant effect on mental health and wellbeing. A meta-analysis of seven prospective studies suggested that both short and long sleep duration was significantly associated with increased risk of depression in adults, with the pooled relative risk for depression as 1.31 for short sleep duration compared to normal sleep duration (Zhai et al., 2015). Sleep disturbances have been previously associated with poor mental health among health care workers (Zhang et al., 2017a, 2017b). The association between emotional labor and sleep has not been well studied, with only a few studies published from a sample of dental hygienists (Park et al., 2017; S.-U. Yoon & Nam, 2011).
This study adds new evidence to the literature by reporting that sleep disturbances partially attenuated the strength of the association between surface-acting emotional labor and depressive symptoms in health care workers. Sleep has been reported as a significant mediator between work-family conflict and poor mental health (Park et al., 2017; Yoon & Nam, 2011). Our study is innovative in examining and verifying this mechanism between emotional labor and depressive symptoms in a large sample of mixed-occupation health care workers. Confirming our expectation, sleep disturbances play a partial mediating role in this association. If this finding reflects a causal mechanism, then it may be that masking one’s actual emotions during work interactions may cause sleep disturbances, which in turn lead to depressive symptoms among health care workers.
Emotional labor, especially the surface-acting form (masking of actual emotions), can be greatly impacted by working conditions or perhaps exacerbated by them. For example, due to health care workers’ high exposure to occupational violence, it has been recommended to adjust the effect of verbal and physical assaults when examining the negative effect of emotional labor on employee health (Jeung et al., 2018; Phillips, 2016). In our bivariate analyses, emotional labor was positively associated with psychological demands, work-family conflict, negative behaviors at work, assaults, and weekly work hours, while negatively associated with decision latitude, workplace safety, and social support. Shani and colleagues (2014) reported four contextual themes that may affect emotional labor in hospitality industries, including the manager-employee relationship, the job’s physical demands, the quality of emotional labor training, and the frequency, duration and repetition of guest-employee encounters. Another study reported that customer contact, role ambiguity, job autonomy, and social support potentially moderated the association between emotional labor and burnout in service workers (S. Kim & Wang, 2018).
Strengths and Limitations
This study has several strengths, including the large sample of workers, the inclusion of a wide range of health care jobs, the adjustment for multiple sociodemographic and work covariates in the data analyses, and the consideration of possible mediating and moderating effects of sleep. This study also has several limitations. Definitive conclusions about causal relationships cannot be drawn in a cross-sectional design. Future longitudinal studies are needed to verify the study findings. The study setting (public sector facilities with union representation) might limit the generalizability of the study findings. A prospective study using a more nationally representative random sample of health care workers would be a valuable follow-up.
Implications for Occupational Health Nursing Practice
This quantitative cross-sectional study found that surface-acting emotional labor was significantly associated with depressive symptoms among health care workers. This association was partially mediated by sleep disturbances. These findings have particular implications for occupational health nurses who are responsible for reducing work-related safety and health hazards and promoting healthy behaviors of employees. Health care work involves high physical and psychosocial stress, leading to low employee job satisfaction, burnout, intention to turnover, and poor health outcomes (Iliceto et al., 2013; Khamisa et al., 2015; Mosadeghrad, 2013; Zhang et al., 2014). These workers’ sleep and mental health deserves particular attention since poor sleep and mental health likely affect the quality of care delivery and patient safety.
Workplace programs are needed to prevent or reduce emotional masking in order to address the prevalence of depressive symptoms among healthcare workers. Previous studies (Kim & Wang, 2018; Shani et al., 2014) as well as this one suggest that improving the work environment to reduce surface-acting emotional labor may have great potential for employee well-being. Team climate may act as a moderator between emotional labor and burnout, subsequently influencing employee turnover intention (Cheng et al., 2013). Flores and colleagues stated that the higher the organizational support received by nurses, the less they manifest surface acting (Flores, 2018). Another study reported that social support may offset the harmful effect of emotional masking on organizational commitment (Mikeska et al., 2015). Therefore, workplace programs improving social support from coworkers, supervisors, and the organization could potentially reduce the negative effect of emotional labor.
Other organizational strategies to reduce surface-acting emotional labor may include but are not limited to: Provide more opportunities to make job decisions; improve workplace safety through reducing negative behaviors and assaults at work, schedule appropriate length of work hours on a weekly basis, and genuinely listen to workers’ difficulties when conflict arises from their work or family life. In addition, providing sufficient resources at the workplace with regards to facilitating work-family balance, promoting more collaborative team environment, and providing free and supportive psychological counseling may reduce emotional masking and in turn, may improve worker mental health and wellbeing. Workplaces may also provide programs that can help employees understand their reactions to emotional labor and develop policies and procedures to reduce its negative impact.
Sleep is an important self-care domain and sufficient sleep is needed for optimum human function. In order to attenuate the negative influence of emotional labor on worker mental health, sleep promotion is important. Workplace education or interventions are encouraged to address healthy sleep practices including sleep hygiene education. Additionally, non-pharmacological strategies, such as meditation, mindfulness, yoga and other complementary medicines are recommended as effective treatments of sleep problems and practical strategies of sleep promotion. These may be implemented through workplace training or continuing education.
Applying Research to Occupational Health Practice
This study provides innovative information about sleep disturbances as a partial mediator in the association between surface-acting emotional labor and depressive symptoms among health care workers. Both sleep and mental health of health care workers are of significance since their ability to mentally function at a high level during the work process is essential to ensure patient safety and quality of care. Findings from this study provide useful information to occupational health nurses to identify organizational risk factors associated with emotional labor and to understand poor health behaviors and outcomes resulting from emotional labor. Workplace programs are needed to improve health care workers’ work environment and help them understand their reactions to emotional labor, thereby develop policies and procedures to reduce the negative impact of emotional labor. In addition, sleep promotion needs to receive considerable attention for health care workers to mitigate the negative effect of emotional labor on their mental health and wellbeing.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The Center for the Promotion of Health in the New England Workplace is supported by Grant Number 2 U19 OH008857 from the National Institute for Occupational Safety and Health (CDC). This work is solely the responsibility of the authors and does not necessarily represent the official views of NIOSH. We are grateful to the CPH-NEW Research Team members who collected the questionnaire data and the workers who shared their experiences with us.
IRB Protocol Number
This study was approved by the Institutional Review Board at University of Massachusetts Lowell (No. 16-131-PUN-XPD).
Author Biographies
Yuan Zhang, PhD, RN, is an Associate Professor of Nursing at the University of Massachusetts Lowell. Her research focuses on the broader effect of work environment on sleep quality, physical and mental health of health care workers; and workplace participatory interventions to improve employee health and safety.
Mazen ElGhaziri, PhD, MPH, RN, is an Assistant Professor and Associated Chair of Nursing at the University of Massachusetts Lowell. His research focuses on workplace violence prevention and its impact on physical and mental health of the health care and correctional workforce, with a bio-behavioral approach to preventive interventions.
Sundus Siddique, MBBS, MPH, is a doctoral candidate in Epidemiology at the University of Massachusetts Lowell. She has worked as a general physician and surgeon. Her primary research focuses on occupational medicine, specifically burnout in health care professionals.
Rebecca Gore, PhD, is a Senior Biostatistician in the Department of Biomedical Engineering at the University of Massachusetts Lowell. She has experience in regression modeling of various types including robust regression, regression smoothing and mixed and multilevel models. Other areas of interest are causal inference and Bayesian modeling.
Alicia Kurowski, ScD, is a Research Professor in the Department of Biomedical Engineering at the University of Massachusetts Lowell. Her research interests are in health care ergonomics, safe patient handling, and participatory ergonomics methods for employee engagement.
Suzanne Nobrega, MS, is Outreach Project Director and a doctoral student in Education Research and Evaluation at the University of Massachusetts Lowell. Her research interests are in job stress and chronic disease, Total Worker Health, and participatory interventions.
Laura Punnett, ScD, is Professor of Biomedical Engineering at the University of Massachusetts Lowell. Her research interests include the interacting effects of physical and psychosocial job features on workers’ health and safety; the contribution of working conditions to gender and socioeconomic health disparities, and the effectiveness of workplace programs to improve safety, ergonomics, and health.