
Abstract
Background: Musculoskeletal disorders (MSDs) are the leading cause of pain and disability among nurses and are frequently accompanied by depression. However, the association between the comorbidity of MSDs and depression and working conditions has not been studied, which was the aim of this study. Methods: In 2015, all nurses (n = 1,102) employed at a community hospital in the Northeast United States were invited to participate in this cross-sectional study. A survey was distributed in which participants were asked to report on MSDs, depressive symptoms, as well as subjective working conditions assessed including physical demands, psychological demands, decision authority, social support, and work–family conflict. Findings: 397 nurses responded (36%), and the prevalence of the comorbidity of MSDs and depression was 14.5%. Poisson regression (PR) models suggested that work–family conflict was associated with increased risk of the comorbidity (PR = 2.18; 95% confidence interval [CI] = 1.33–3.58), as was 8-hour night shift (PR = 2.77; 95% CI = [1.22, 6.31]) or 12-hour day shift (PR = 2.20; 95% CI = [1.07, 4.50]). Other working conditions were not directly associated with the comorbidity. Conclusions/Application to Practice: The comorbidity of MSDs and depression is prevalent among hospital nurses, and work–family conflict and working night shift or longer shifts were significantly associated with this. Effective workplace programs are needed to address nurses’ working conditions to reduce their work–family conflict, thereby improving their musculoskeletal and mental health.
Background
Musculoskeletal disorders (MSDs) are the leading cause of pain and disability in the U.S. workforce (U.S. Department of Labor, Bureau of Labor Statistics, 2016). Nursing is among the high-risk occupations for MSDs, which account for nearly half of the total injury and illness cases that occur in this occupational group annually (U.S. Department of Labor, Bureau of Labor Statistics, 2016). The hospital setting ranks as the top most expensive for occupational injuries and illnesses among more than 300 U.S. industries, with nurses contributing to the greatest costs (Dressner, 2017). MSDs among nurses are associated with high direct and indirect costs with respect to workers’ compensation claims, lost workdays, and job turnover (Shraim et al., 2015). The indirect costs associated with MSDs, such as increased nurse turnover and reduced work productivity, can increase the total costs by 2 to 4 times (Hunter et al., 2010). For example, the estimated costs associated with replacing a nurse who leaves the profession, including recruiting, hiring, and productivity loss and training, can range from US$27,000 to US$103,000 per nurse (Li & Jones, 2013). The direct and indirect expenditures resulting from MSDs in the general public were estimated to be 5.7% of the national gross domestic product in the United States (United States Bone and Joint Decade, 2014).
Nurses are susceptible to MSDs because they are exposed to heavy lifting, transferring, and repositioning of patients; frequent bending and twisting of their body; and a rapid work pace with patient handling conferring the highest risk for MSDs (Yassi & Lockhart, 2013). Irregular and long work hours lead to insufficient recovery between shifts, exacerbating MSDs among nurses (Caruso & Waters, 2008). Psychosocial work factors may have small but significant lagged effects on the development of MSDs (Lang et al., 2012). A literature review and meta-analysis found that high psychosocial demands (aspects of the job that require sustained psychological effort or skills), low job control (the ability to influence what happens in the work environment), low social support, and effort-reward imbalance were associated with prevalent and incident MSDs in hospital nurses and nursing assistants (Bernal et al., 2015).
Depression has been identified as the second leading cause of disability in the United States (U.S. Burden of Disease Collaborators, 2013). With work responsibilities around the clock and high occupational stress (Geiger-Brown & Lipscomb, 2010), nurses suffer a higher incidence of depressive symptoms relative to the general U.S. adult population (Letvak et al., 2012), which may lead to a high rate of burnout, absenteeism, and turnover (Gilmartin, 2013; Khamisa et al., 2015). Work stress has been reported as a strong predictor of depression in different occupational groups (Ganster & Rosen, 2013; Wang et al., 2012), including nurses (Khamisa et al., 2013; Lin et al., 2016). Generally, work stress is negatively related to psychological well-being and health among nurses (Khamisa et al., 2015). Specifically, high job demands (aspects of the job that requires sustained physical and/or psychological effort or skills), low job control, and lack of social support were associated with mental health problems among nurses (Friemann & Merisalu, 2015; Roelen et al., 2018).
Work–family conflict is a type of interrole conflict experienced when role pressures from the work and family domains are incompatible with one another (Greenhaus & Beutell, 1985). Previous studies have reported a significant association between work–family conflict and depressive symptoms among nurses (Hao et al., 2015; Sugawara et al., 2017) and other health care professionals such as nursing assistants (Zhang et al., 2017) and physicians (Hao et al., 2016). Studies have also reported possible effects of work–family conflict on musculoskeletal pain in nurses (Baur et al., 2018; Nützi et al., 2015) and other patient care workers (Kim et al., 2013).
Comorbidity describes the simultaneous presence of two or more disorders or illnesses in one person. MSDs are frequently accompanied by comorbid symptoms such as depression (Baek et al., 2015). Previous studies have reported that employees with depression were more likely to develop MSDs (Del Campo et al., 2017); and similarly, depression was found to be more prevalent in employees with MSDs relative to employees without MSDs (Baek et al., 2015). The comorbidity of MSDs and depression (Amin et al., 2018; Del Campo et al., 2017), if existing in nurses, may cause negative safety and health outcomes for both nurses themselves and their patients, given nurses’ responsibility in providing most of the front-line care to patients.
Although the effect of work stress on physical outcomes such as MSDs or mental outcomes such as depression has been studied in nurses, little research has described the prevalence of the comorbidity of MSDs and depression in hospital nurses, nor has any research examined the association of this particular comorbidity (MSDs and depression) with physical and psychosocial working conditions. Therefore, the objectives of this study were to describe the prevalence of the comorbidity of MSDs and depression in hospital nurses, and to examine the association of this comorbidity with a range of physical and psychosocial working conditions among hospital nurses.
Methods
Study Participants
We employed a cross-sectional study in which data were collected from a sample of registered nurses (RNs) and licensed practical nurses (LPNs) at an independent, not-for-profit community hospital in the Northeast United States in March 2015. A nonprobability convenience sampling method was used to recruit study participants. All RNs and LPNs over 18 years of age and working full-time, part-time, or per-diem in the hospital were eligible to participate (n = 1,102). This work is part of a larger study in which details have been published elsewhere (Zhang et al., 2018).
Recruitment and Data Collection
Study recruitment flyers were posted in each hospital unit 2 weeks before the onsite survey collection. Paper surveys were distributed and collected by the research team over 5 days at the Annual Nurse Skill Days in March 2015, which all nurses at the hospital were required to attend. The study purpose, procedures, and potential benefits and risks were explained to the participants in person and they were requested to complete the survey onsite. Participants were assured that their employer would not receive any identifying information from the surveys, and that participation in the study would not affect their work status. Participants received a compensation of US$5 cash for completing the survey. The study was approved by the Institutional Review Boards at the hospital and at the University of Massachusetts Lowell (No. 2015-001).
Study Measures
MSDs were assessed for six body regions: low back, shoulder, neck, wrist/forearm, knee, and ankle/feet (Zhang et al., 2016). Participants were asked to rate the severity of pain in the past week for each of the six body regions. A 5-point Likert-type scale was used to categorize the answers (1 = none; 2 = mild; 3 = moderate; 4 = severe; and 5 = extreme). MSDs was defined as “yes” for participants who reported moderate, severe, or extreme pain (≥3 on a 1–5 scale) in any region (Zhang et al., 2016).
Depression was assessed with the Center for Epidemiologic Studies Depression Scale (CES-D; Radloff, 1977), the 10-item version (Andresen et al., 1994). This scale is used to identify current depressive symptomatology in individuals aged 18 years and older during the past week. Each item is rated on a 4-point Likert-type scale (0 = rarely or none of the time; 1 = some or a little of the time; 2 = occasionally or a moderate amount of the time; and 3 = most or all of the time) with a range in total score from 0 to 30, with higher scores indicating greater severity of depressive symptomatology. A total score of 10 or more is indicative of depression (Andresen et al., 1994). The scale demonstrated acceptable reliability for this study sample (Cronbach’s α = 0.77).
Participants were defined as having comorbidity of musculoskeletal disorders and depression if they had both MSDs (score ≥ 3) and depression (CES-D ≥ 10).
Working conditions was measured using the Job Content Questionnaire (JCQ; Karasek et al., 1998). The physical demands (five items), psychological demands (four items), job control (three items), and social support (four items) items were selected from the subscales. The JCQ subscales have demonstrated good validity and acceptable reliability in large study populations from six countries (Karasek et al., 1998). Work–family conflict was assessed with the interrole conflict scale from the original instrument, measured with three items from Kopelman et al. (1983). The three items asked whether, “After work I come home too tired to do some of the things I’d like to do,” “On the job, I have so much work to do that it takes away from my personal interests,” and “My family and/or friends dislike how often I am preoccupied with my work while I am at home.” All three items were assessed using a 4-point Likert-type scale (1 = strongly disagree; 2 = disagree; 3 = agree; and 4 = strongly agree). The three items were averaged to give a mean score, with a higher score indicating more work–family conflict.
Nurses mainly worked permanent shifts at the study hospital. Participants’ were asked to provide their primary work schedule with the choices including an 8-hour day (7 a.m.–3 p.m.), 8-hour evening (3 p.m.–11 p.m.), 8-hour night (11 p.m.–7 a.m.), 12-hour day (7 a.m.–7 p.m.), 12-hour evening (including schedules of 9 a.m.–9 p.m., 11 a.m.–11 p.m., and 12 p.m.–12 a.m.), and 12-hour night shifts (including schedules of 7 p.m.–7 a.m. and 3 p.m.–3 a.m.).
The survey collected information on nurses’ sociodemographics, including age, gender, race, height, and weight, and frequency of exercise. Body mass index (BMI) was calculated from self-reported weight and height, expressed as weight/height2 and was categorized as normal (<25.0 kg/m2), overweight (25–29.9 kg/m2), or obese (≥30 kg/m2). Frequency of exercise was measured with one single item “How many times a week on average do you exercise to work up a sweat (at least 20 minutes per session, for example, fast walking, jogging, bicycling, swimming, rowing, etc.)?” on a 5-point Likert-type scale (0 = None; 1 = less than once/week; 2 = 1–2 times/week; 3 = 3 times/week; and 4 = more than 3 times/week). Regular exercise was defined as “exercised three or more times per week.”
Data Analysis
All analyses were conducted using SPSS software version 24.0. The associations of the comorbidity of MSDs and depression (yes or no) with sociodemographics and working conditions were examined using t-tests (comparing means) and chi-square tests (comparing categorical variables) (Field, 2013). Correlations among working conditions were examined using Spearman correlations (Rho), given that some of the variables were not continuous or not normally distributed (Field, 2013).
Given the prevalence of the comorbidity in the study participants was 14.5%, PR modeling with robust variance estimate was used for these analyses (Barros & Hirakata, 2013), because it is more conservative and accurate than logistic regression modeling, and it was therefore used to calculate prevalence ratios among groups, and to investigate potential confounding (Barros & Hirakata, 2003). Multivariate modeling was employed to identify working conditions associated with the comorbidity while adjusting for age, gender, race, BMI, and regular exercise. Furthermore, the effect modification of age (≤40 vs. >40) on the association between working conditions and the comorbidity was examined in the PR modeling. Two-tail significance level was reported at p < .05.
Results
A total of 397 RNs and LPNs completed the survey in March 2015 (response rate: 36%). The participants were primarily (95.2%) middle-aged women (Table 1). More than half (55.6%) of the participants were overweight or obese, and over half (56.9%) reported not exercising regularly. Over one third (35.9%) of these participants worked 8-hour days, 13.7% worked 8-hour evenings, 6.9% worked 8-hour nights, 20.1% worked 12-hour days, 3.6% worked 12-hour evenings, and 19.8% worked 12-hour nights.
Sociodemographics, Working Conditions, Musculoskeletal Disorders, and Depression Among Nurses (n = 397)
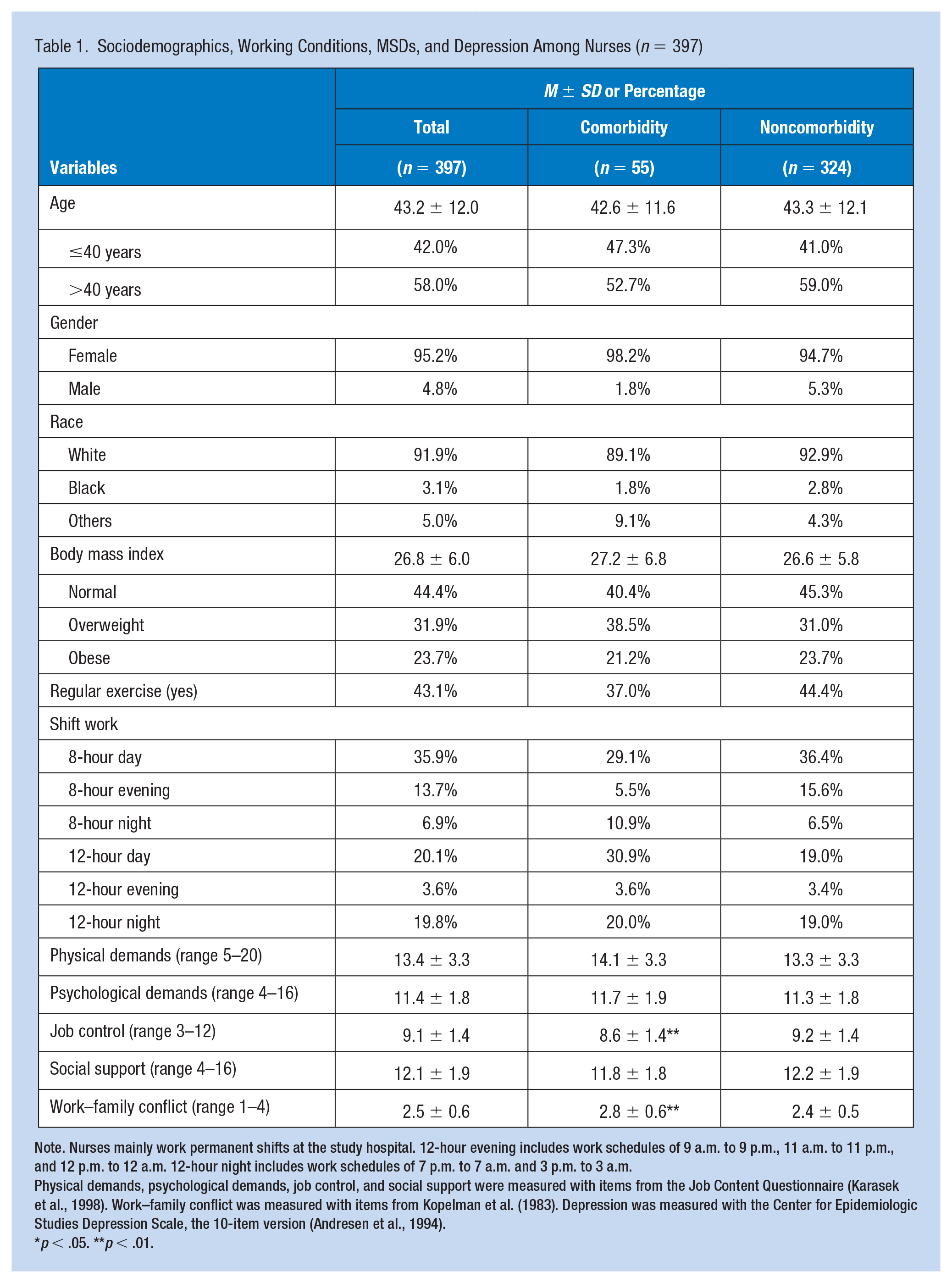
Note. Nurses mainly work permanent shifts at the study hospital. 12-hour evening includes work schedules of 9 a.m. to 9 p.m., 11 a.m. to 11 p.m., and 12 p.m. to 12 a.m. 12-hour night includes work schedules of 7 p.m. to 7 a.m. and 3 p.m. to 3 a.m.
Physical demands, psychological demands, job control, and social support were measured with items from the Job Content Questionnaire (Karasek et al., 1998). Work–family conflict was measured with items from Kopelman et al. (1983). Depression was measured with the Center for Epidemiologic Studies Depression Scale, the 10-item version (Andresen et al., 1994).
p < .05. **p < .01.
Nearly half (47.4%) of the participants reported MSDs (moderate, severe, or extreme pain in one or more body regions). Musculoskeletal pain (mild, moderate, severe, or extreme pain) was reported in the following body regions: low back (63.0%), shoulder (42.4%), neck (50.6%), wrist/forearm (24.2%), knee (35.0%), and ankle/feet (39.3%). Nearly one quarter (24.4%) reported depression (CES-D ≥ 10), with 14.5% prevalence with the comorbidity of MSDs and depression.
Significant associations were found between the comorbidity with job control (8.6 ± 1.4 vs. 9.2 ± 1.4, t = −2.82, p < .01) and work–family conflict (2.8 ± 0.6 vs. 2.4 ± 0.5, t = 4.47, p < .01). Although nurses with the comorbidity worked more on 8-hour nights (10.9% vs. 6.5%) or 12-hour days (30.9% vs. 19.0%) compared with nurses without the comorbidity, the association between shift work and the comorbidity was not significant (chi-square = 8.62, p = .13) at the bivariate level.
Significant correlations were found between work–family conflict with physical demands (Rho = 0.25, p < .01), psychological demands (ρ = .31, p < .01), and job control (ρ = −.15, p < .01) (data not shown). Younger age was significantly associated with more work–family conflict (t = 2.47, p < .05) and higher depression score (t = 3.13, p < .01), but was not associated with MSDs (chi-square = .57, p > .05) or the comorbidity (chi-square = .76, p > .05) (data not shown).
For the multivariate analysis, work–family conflict was significantly associated with the comorbidity (PR = 2.18; 95% confidence interval [CI] = 1.33–3.58) after adjusting for covariates (Table 2). With every one-unit increase in work–family conflict, the prevalence of the comorbidity increased by 118%. Compared with 8-hour days, nurses working 8-hour nights (PR = 2.77; 95% CI = [1.22, 6.31]) or 12-hour days (PR = 2.20; 95% CI = [1.07, 4.50]) reported higher prevalence of the comorbidity. Age, gender, race, BMI, regular exercise, and physical demands, psychological demands, job control, and social support were not significantly associated with the comorbidity.
Multivariate Robust Poisson Regression Models for the Association Between Working Conditions and the Comorbidity of Musculoskeletal Disorders and Depression Among Nurses (n = 397)
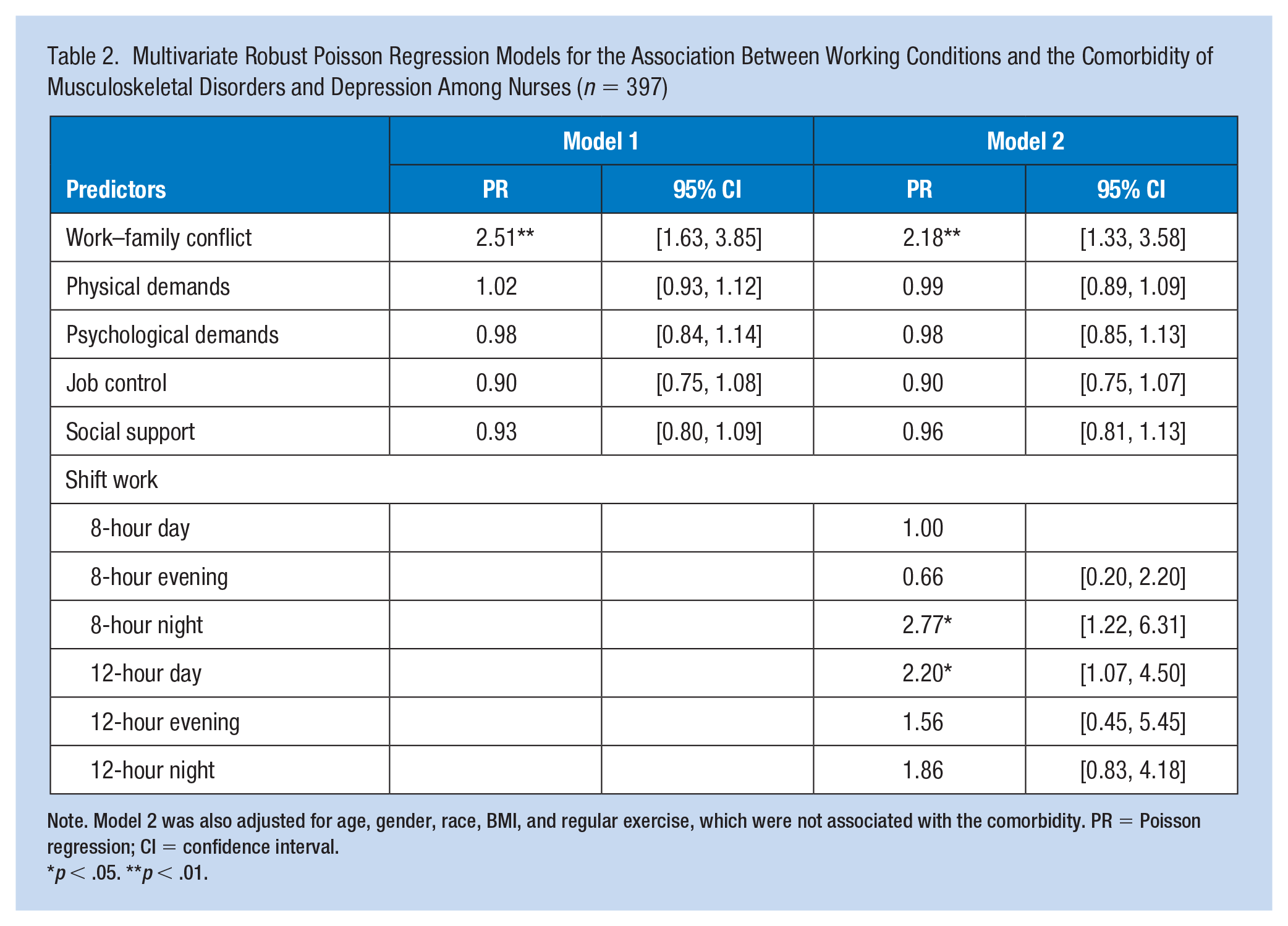
Note. Model 2 was also adjusted for age, gender, race, BMI, and regular exercise, which were not associated with the comorbidity. PR = Poisson regression; CI = confidence interval.
p < .05. **p < .01.
The effect modification of age on the association between work–family conflict and the comorbidity by age (≤40 years vs. >40 years) was not statistically significant (PR = 1.10; 95% CI = [0.41, 2.93]) (data not shown), suggesting age was not an effect modifier of this association.
Discussion
In this study, nearly half of the nurses reported MSDs in at least one of the six body regions. Consistent with previous studies, we found that the reported prevalence of musculoskeletal pain in nurses was greatest in the lower back, followed by the neck and shoulders (Davis & Kotowski, 2015). One quarter of these nurses reported depressive symptoms in the past week, which is a higher prevalence than that reported from the general population in the United States (National Institute of Mental Health, 2019), and a higher prevalence than that reported from a random sample of hospital nurses (Letvak et al., 2012). The prevalence of the comorbidity of MSDs and depression was 14.5% in the study sample. A previous study with over 6,500 Danish female health care workers reported an 18% comorbidity including one or more musculoskeletal pain locations and medium or higher levels of depressive symptoms (Melkevik et al., 2018). The comorbid pain and depression have been widely reported in the patient population (Goesling et al., 2013). This comorbidity should be of particular concern to hospital administrators and other employers, because either symptom or their comorbidity could have critical implications for the safety and health of nurses themselves and their patients, considering nurses’ role in direct contact with patients and providing most of the front-line services in hospitals. Nurses’ ability to physically and mentally function at a high level is essential to ensure a high quality of care and patient safety.
As expected, work–family conflict was significantly associated with the comorbidity of MSDs and depression among nurses. Nurses, as formal caregivers at work and informal caregivers at home, are often engaged in multiple work and family responsibilities and therefore have a high risk for work–family conflict and negative outcomes (Cortese et al., 2010). Previous studies have reported the high prevalence of both family interference with work and work interference with family among nurses (Alazzam et al., 2017). Work–family conflict was previously reported to be associated with poor physical health such as musculoskeletal pain (Kim et al., 2013) and poor mental health such as depressive symptoms (Hao et al., 2015) in nurses. One study reported that work-to-family conflict was a strong predictor of MSDs, and this association was mediated by work stress (Hämmig et al., 2011). Nützi et al. (2015) reported that work–family conflict significantly predicted lumbar and cervical pain, which are the most prevalent musculoskeletal complaints among operating room nurses. Two meta-analyses have reported significant correlations between work–family conflict and mental health outcomes including depression (Amstad et al., 2011).
As expected, compared with 8-hour day shift, nurses working 8-hour night shift and 12-hour day shift reported a higher prevalence of the MSDs-depression comorbidity. Shift work, especially night shift and long work hours, have been associated with increased risk for a wide range of chronic diseases (Caruso, 2014). A systematic review has identified eight studies which linked long work hours to adverse musculoskeletal disorders (Caruso & Waters, 2008). Another systematic review and meta-analysis reported that night shift work was significantly associated with an increased risk of depression (Lee et al., 2017).
In contrast to our expectation, this study did not find an association of the MSDs-depression comorbidity with any of the other working conditions we tested (physical demands, psychological demands, job control, and social support). However, work–family conflict, specifically the work interference with family life assessed in this study, may be greatly affected by these working conditions. For example, work–family conflict was significantly associated with physical demands, psychological demands, and job control in this study sample. Yildirim and Aycan (2008) found that heavy workload and demanding work schedules were important predictors of work-to-family conflict, which was associated with lower job and life satisfaction among nurses. This finding indicates that while some working conditions may not directly affect the comorbidity, they may indirectly contribute to the comorbidity through work–family conflict. Previous studies have recommended that increasing employee control over work assignments (job control) and supportive behaviors from supervisors (social support) may buffer the negative influence of work–family conflict on employees’ health and well-being (Kelly et al., 2011; Kossek et al., 2011).
In this study, age was not observed as an effect modifier in the association between work–family conflict and the comorbidity, suggesting that the association between work–family conflict and the comorbidity was not different in either age group (≤40 years vs. >40 years). As expected in this study, nurses of 40 years or younger reported more work–family conflict than nurses over 40 years, likely due to child care responsibilities. In addition, nurses 40 years or younger reported higher depression than nurses over 40 years, likely due to better coping abilities and strategies with irregular work schedules and work stress among older and experienced nurses (Chiang & Chang, 2012), or older nurses who became depressed may have terminated their jobs and are not reflected in our sample. However, there was no difference reported in the prevalence of MSDs or the comorbidity between the two age groups. Previous studies have reported potential higher prevalence of MSDs in older nurses (Trinkoff et al., 2003), for example, Trinkoff et al. reported a significant positive association between age (>40 years) and shoulder complaints in nurses.
The strengths of this study are the consideration of a variety of physical and psychosocial working conditions, the adjustment for multiple confounders, and the testing of age as an effect modifier in the data analyses. This study has several limitations. First, although the study avoids some possible confounders at the organizational level because all nurses were employed by a single not-for-profit community hospital, the generalizability of the findings is limited as a result. Second, the response rate of 36% is comparatively low, which may have led to a selection bias of the nursing population. A follow-up study using a more nationally representative, random sample would improve the generalizability of the study findings. Finally, definitive conclusions about causal relationships cannot be drawn with a cross-sectional design. Future analyses of longitudinal data would be desirable to verify the study findings.
Implications for Occupational Health Nursing Practice
This quantitative cross-sectional study found that the comorbidity of MSDs and depression is prevalent among hospital nurses, and work–family conflict and night or longer shift were significantly associated with the comorbidity. The results from the study suggest that, in addition to efforts that directly address prevention of MSDs and depression, future workplace education and training programs that reduce work–family conflict or help nurses cope better with night or longer shifts may also be able to reduce the MSDs-depression comorbidity indirectly, thereby promoting the physical and mental health of nurses.
In addition to structuring work schedules to allow sufficient recovery between shifts, workplaces may provide education to nurses on coping strategies with night or longer shifts and behavior or lifestyle changes to adapt to shift work. It has been reported that the health effect of irregular shift is less severe when it is selected by nurses (Buessing, 1996); therefore, providing nurses with the authority to choose their work shifts may reduce the negative health and safety consequences resulting from it.
Workplace programs should involve both the organization and nurses themselves in the prevention and intervention of work–family conflict. Previous studies have suggested that enhancing career development opportunities, encouraging nurses to participate in policy decisions, and supporting nurses’ communication about risks at work and active participation in safety and health activities may reduce their demands at work and in turn reduce work–family conflict (Camerino et al., 2010; Leineweber et al., 2014). Nursing management should be actively involved in the process of reducing nurses’ work–family conflict through supporting staff in achieving collective goals, modeling effective work–family management strategies, and providing useful information and advice (Gillet et al., 2013). In addition, developing hospital policies and practices to facilitate the successful combination of work with family life for nurses would promote better work–family balance, and promote a better and more collaborative atmosphere between coworkers, which may itself have positive effects on the safety, health, and productivity of the workforce (Leineweber et al., 2014).
As we found that work–family conflict was associated with physical demands, psychological demands and job control, our study suggests that to reduce nurses’ work–family conflict, organizations could involve nurses in making decisions about work activities; reduce nurses’ workload through increasing staffing; genuinely listen to nurses’ expectations and opinions when difficulties arise from their work or family life; and provide an Employee Assistance Program (EAP) to nurses for psychological counseling. A specific focus on mitigating work–family conflict should be considered in future efforts to promote musculoskeletal and mental health in nursing employees.
Applying Research to Occupational Health Practice
This study provides innovative information about the prevalence of musculoskeletal disorders (MSDs)-depression comorbidity and its association with working conditions among hospital nurses. Both physical and mental health of nurses are critical because nurses’ ability to physically and mentally function at a high level is essential to ensure a high quality of care and patient safety. The results from this study suggest that, in addition to efforts that directly address prevention of MSDs and depression, future workplace education and training programs that reduce work–family conflict or help nurses cope better with night or longer shifts may also be able to reduce the MSDs-depression comorbidity indirectly, thereby promoting the physical and mental health of nurses. To reduce nurses’ work–family conflict, workplaces may involve nurses in making decisions about work activities; reduce nurses’ workload through increased staffing; genuinely listen to nurses’ expectations and opinions when difficulties arise from their work or family life; and provide an Employee Assistance Program (EAP) to nurses for psychological counseling.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Y.Z. and J.F.D. were supported by a grant from the National Institutes of Health (R01 AG044416). The funder played no role in the study design, data collection, data analysis, manuscript preparation, or decision to publish the report.
IRB Protocol Number
This study was approved by the Institutional Review Boards at Lowell General Hospital and the University of Massachusetts Lowell (No. 2015-001).
Author Biographies
Yuan Zhang, PhD, RN, is an associate professor of Nursing at the University of Massachusetts Lowell. Her research focuses on the broader effect of work environment on sleep quality, physical and mental health of health care workers; and workplace participatory interventions to improve employee health and safety.
Mazen ElGhaziri, PhD, MPH, RN, is an assistant professor of Nursing at the University of Massachusetts Lowell. His research focuses on workplace violence prevention and its impact on physical and mental health of the health care and correctional workforce, with a bio-behavioral approach to preventive interventions.
Sarah Nasuti is a student nurse at the University of Massachusetts Lowell. She has worked as a research assistant on this study and is interested in research related to nurses’ shift work, working conditions, and safety and health outcomes.
Jeanne F. Duffy, MBA, PhD, is an associate professor of Medicine at Harvard Medical School and a Neuroscientist at Brigham and Women’s Hospital. Her research focuses on understanding individual differences in sleep timing, duration, quality, and response to sleep loss, and exploring ways to improve sleep so as to reduce the risk of accidents, errors, and adverse health outcomes.