
Abstract
The aim of this cross-sectional study was to explore the ergonomic risk factors for low back pain (LBP) and neck pain in an industry in which only light tasks are performed. These common disorders can be significant work-related musculoskeletal disorders. This study included 396 employees who worked in packaging units of pharmaceutical companies. The Nordic Musculoskeletal Questionnaire and the rapid upper limb assessment (RULA) were used to generate data. This study showed an association between LBP, RULA scores, and workers’ education. For neck pain, an association was found with age, gender, and subjective questions about working posture (mostly sitting/standing or alternating between the two). Absence from work more than 3 days, which could have been associated with pain, was significantly associated with both disorders.
Work-related musculoskeletal disorders (WMSDs) are a leading cause of early retirement and absence from work (Choobineh, Tabatabaei, Tozihian, & Ghadami, 2007; Moreira, Sato, Foltran, Silva, & Coury, 2014; Theilmeier, Jordan, Luttmann, & Jager, 2010). The occurrence of WMSDs has risen in the past 20 years (Sartorio et al., 2005), comprising more than half of all reported occupational illnesses (Morse et al., 2005). These disorders are the most frequent occupational injuries and the most common cause of long-term disabilities worldwide (Ekpenyong & Inyang, 2014). The regions most likely affected are the spine, shoulders, elbows, and hands (Sartorio et al., 2005). Some individual characteristics (e.g., gender or age) and also some occupational factors (e.g., type of work, awkward postures, hard or accelerated work, and stereotypical movements) can contribute to the occurrence of these disorders (Choobineh et al., 2007; Lu, Waters, & Werren, 2015; Lynch, Smidt, Merrill, & Sesek, 2014; Sartorio et al., 2005). Awkward postures are defined as repetitive postures or those that are held statically for prolonged periods of time and are capable of causing pain, fatigue, and injury (Das, Ghosh, & Gangopadhyay, 2012).
Low back pain (LBP) is one of the most significant WMSDs because it comprises a large percentage of these disorders (Tamrin, Yokoyama, Aziz, & Maeda, 2014), common among workers with a high economic burden (Ekpenyong & Inyang, 2014; Roffey, Wai, Bishop, Kwon, & Dagenais, 2010; Trask et al., 2010). Low back pain is the most prevalent injury and health complaint among laborers (Burgel, Nelson, & White, 2015), however the literature is somewhat inconsistent about specific risk factors for LBP (Coenen, Kingma, Boot, Bongers, & van Dieen, 2014; van der Molen, Frings-Dresen, & Sluiter, 2010). Several articles have suggested an association between occupation and LBP. Some of these articles highlighted the association between sedentary work and LBP (Kelsey, 1975). Other articles hypothesized that heavy manual labor, heavy lifting, mechanical loads, prolonged work hours, and lifting with awkward postures are significantly associated with LBP and intervertebral disk disease (Ahsan et al., 2013; Ekpenyong & Inyang, 2014; Pope, Goh, & Magnusson, 2002; Theilmeier et al., 2010).
Neck pain is also a common condition and public health epidemic (Koh et al., 2014) with serious consequences for employees and high costs for employers and society (Eijckelhof et al., 2013). Risk factors for neck pain include prolonged desk work, prolonged standing, prolonged sitting, and working at a computer workstation (Shuai, Yue, Li, Liu, & Wang, 2014).
Packaging is a task with many ergonomic risk factors including static load on the back and neck, repetition, awkward postures, and extended reach (Simcox, Flanagan, Camp, Spielholz, & Synder, 2001). Only a few studies have been published about the prevalence of LBP in pharmaceutical and packaging employees. The prevalence of LBP in similar industries has been estimated from 44% to 66% with the highest number in packaging units (Ghasemkhani, Mahmudi, & Jabbari, 2008; Rotgoltz, Derazne, Froom, Grushecky, & Ribak, 1992). In a poultry packaging company, the prevalence of neck pain was 29% (Reis et al., 2012). It was shown that more than half of the neck and lower back complaints in packers were work related (Simcox et al., 2001).
The first aim of this study was to assess the prevalence of LBP and neck pain in the past 12 months in a sample of employees working in packaging units of pharmaceutical companies in Tehran. In addition, the researchers assessed the association between these disorders and several risk factors including ergonomic risk factors and posture.
Method
The study population consisted of employees of packaging units at pharmaceutical companies in Tehran. At the time of this study (2012-2013), 30 pharmaceutical companies in Tehran Province reported a total of 1,046 employees in their packaging units. The researchers used cluster sampling and randomly chose nine of the 30 companies, including all packaging workers in the sample population of 461 workers.
Employees’ tasks, packaging pharmaceuticals, were all considered light (maximum weight = 5 kg). They repeated many work tasks, the tasks were often monotonous, and the level of exertion did not result in workers perspiring. Titles for these jobs included operation supervisor, packaging operator (i.e., fillers and cappers, labelers, carton operators, case sealers), technicians, and quality control staff. Some employees performed their tasks primarily in sitting or standing positions. Other employees did their job while alternating between the two positions. Some employees used computers for variable amounts of time during the workday.
Rapid upper limb assessment (RULA) is an observational technique used to assess posture and can be compared with similar tools such as the Ovako working posture analysis system (OWAS) and rapid entire body assessment (REBA). However, RULA does not underestimate postural loads and is used by the majority of ergonomists for this purpose (Kee & Karwowski, 2007; Pascual & Naqvi, 2008). It is one of the best methods for postural evaluation of high-risk jobs, and its use does not necessitate specific equipment (Golchha, Sharma, Wadhwa, Yadav, & Paul, 2014; Jones & Kumar, 2010). Its scoring system is based on measuring the angular deviation of a particular body part from the neutral position (Garcia & Campos, 2013). This method gives a score from 1 to 9 (9 being the most awkward posture), and then, this score is translated into four categories called action levels. These action levels define the need for ergonomic interventions (McAtamney & Nigel Corlett, 1993). Action Level 1 (RULA scores of 1 and 2) means that if the posture is not held statically for prolonged times, it is acceptable. Action Level 2 (RULA scores of 3 and 4) indicates it is necessary to study the posture in more detail and ergonomic interventions are probable. Action Level 3 (RULA scores of 5 and 6) suggests a more detailed study is warranted and ergonomic interventions should be scheduled in the near future. Action Level 4 (RULA scores of 7 or more) indicates an in-depth study and immediate ergonomic interventions are obligatory. The RULA considers the postures of the arms, forearms, neck, and trunk for scoring and is calculated separately for both sides of the body (Rafie, Zamani Jam, Shahravan, Raoof, & Eskandarizadeh, 2015).
For assessment of the prevalence of LBP and neck pain in the previous 12 months, the Nordic Musculoskeletal Questionnaire was used (Kuorinka et al., 1987). It is one of the most widely used tools for assessment of WMSDs (Ekpenyong & Inyang, 2014; Krishna, Maiti, Ray, & Mandal, 2015). The validity and reliability of its Persian form have been assessed in previous studies (Arsalani, Fallahi-Khoshknab, Ghaffari, Josephson, & Lagerstrom, 2011; Choobineh, Lahmi, Shahnavaz, Jazani, & Hosseini, 2004). This questionnaire focuses on key regions of the body (Choobineh et al., 2007). The first part consists of a general questionnaire and asks about the occurrence of pain in different anatomical regions (e.g., neck, back, shoulder, hand, and wrists), and the second part focuses on each region of the body in more depth (Rafie et al., 2015). The researchers considered only pain in the lower back and neck regions for this article.
The questionnaire consisted of the Nordic Musculoskeletal Questionnaire and also some general questions about sample demographics. Other questions about shift work, exercise frequency, and smoking were also included in the questionnaire (Tables 1 and 2). In this study, work experience was defined as the number of years an employee performed the same task as the current one. Shift work was defined as any working hours out of the normal 8 a.m. to 4 p.m. Shift workers were later subdivided into workers with fixed shifts or rotational shifts. Fixed shifts were considered to have the same work hours throughout the year; rotational shifts alternated among different work hours. Extra work hours were defined as the amount of time that workers stayed at the workplace and worked above the statutory 44 hours per week. In Iran, academic education requires completing 12 years of study so the researchers grouped participants’ education into two categories: those who had completed 12 years or more of school and those who had not finished the first 12 years. Smoking was inclusive of any kind of tobacco use in the past or present. Working posture was also asked subjectively, divided into two groups, one with mostly sitting or standing tasks and the other group with tasks that alternated between sitting and standing. For the alternating group, a minimum of 2 hours of alternating between the usual postures (sitting or standing) was required.
Continuous Variables and Their Association With LBP in the Previous Year
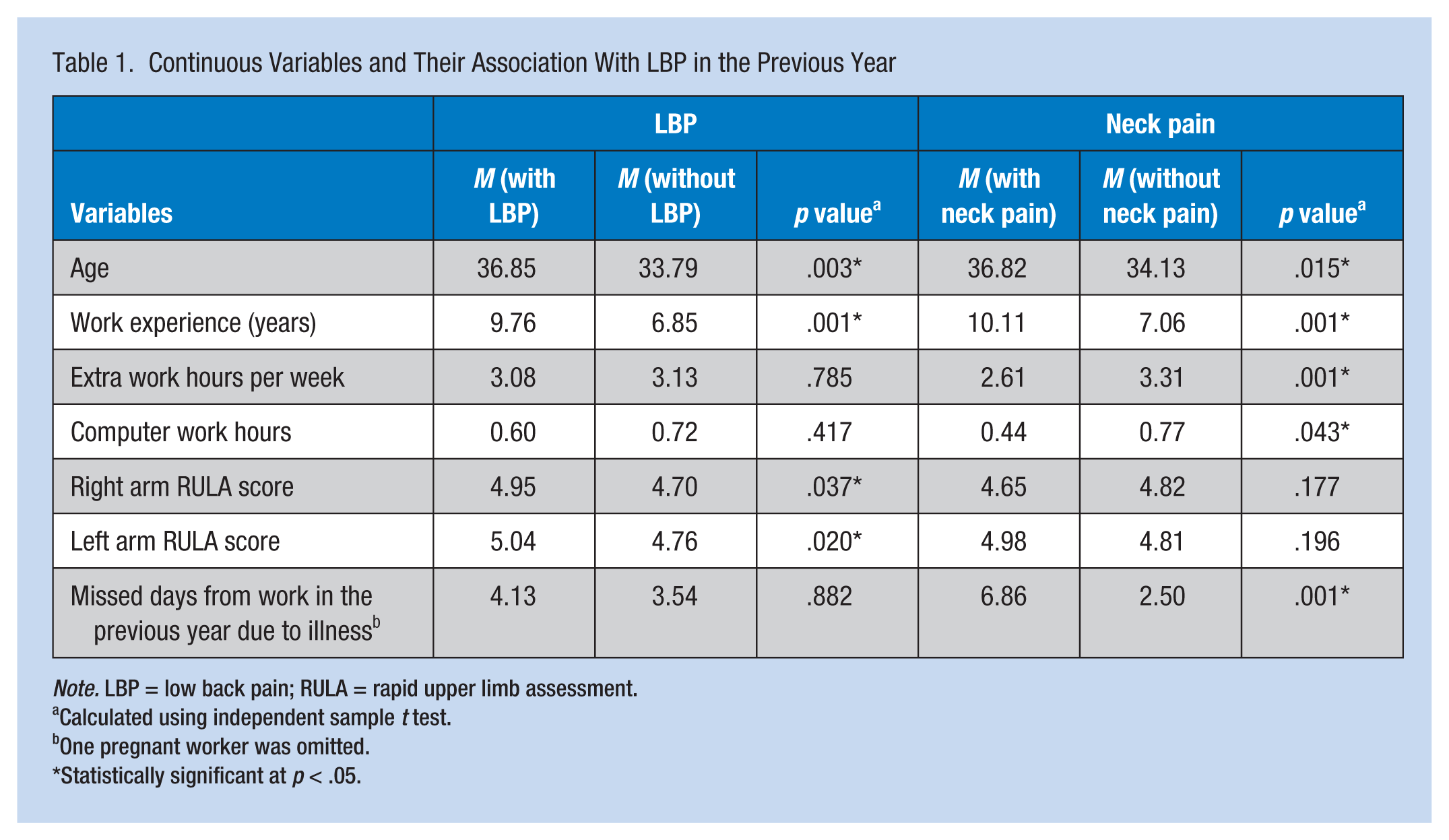
Note. LBP = low back pain; RULA = rapid upper limb assessment.
Calculated using independent sample t test.
One pregnant worker was omitted.
Statistically significant at p < .05.
Categorical Variables and Their Association With LBP in the Previous Year
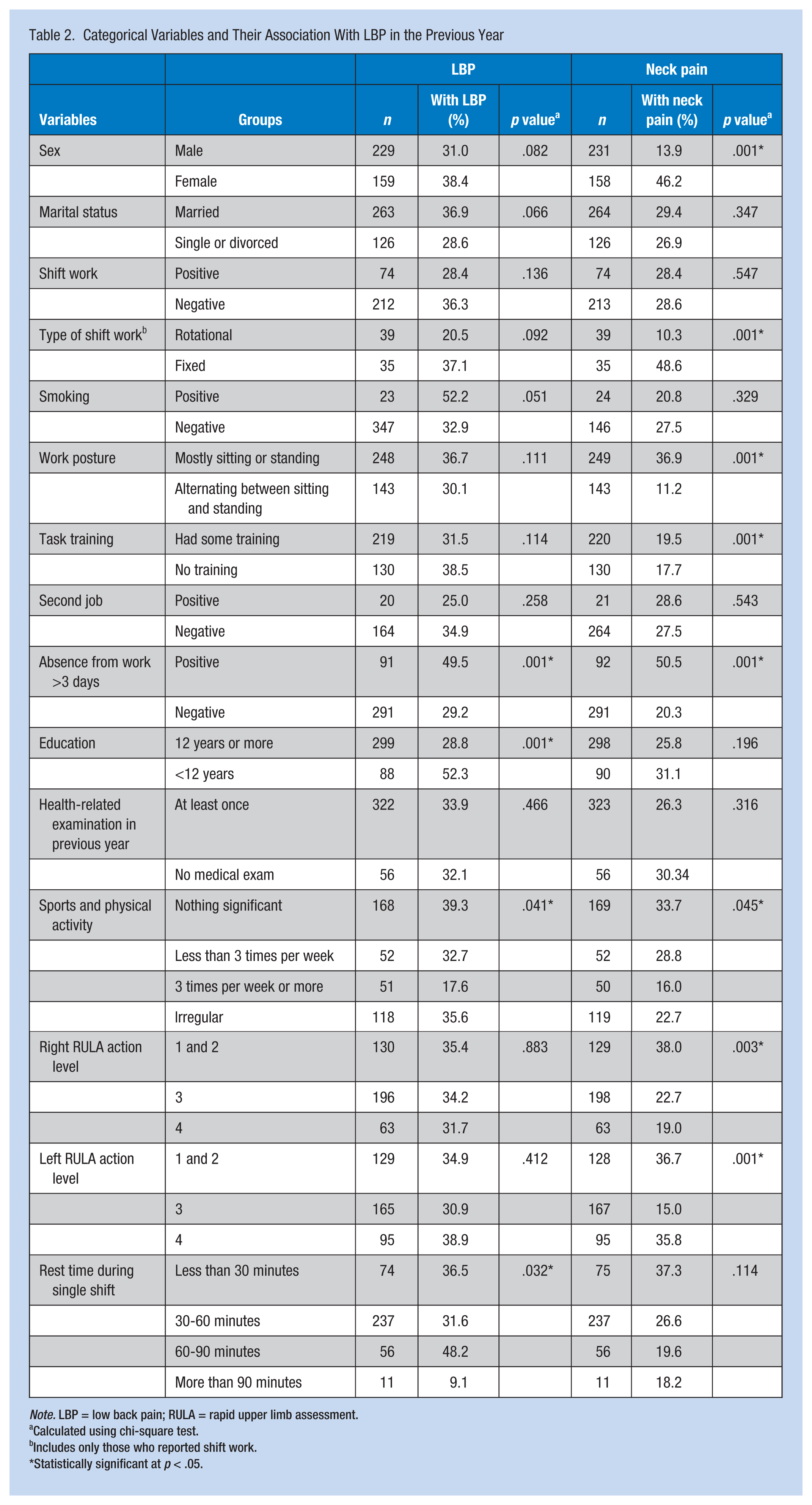
Note. LBP = low back pain; RULA = rapid upper limb assessment.
Calculated using chi-square test.
Includes only those who reported shift work.
Statistically significant at p < .05.
Performing most work tasks for this company required some manual skills, and workers were questioned about whether they had been taught these necessary skills by supervisors or colleagues. The second job was defined as working another job outside of this company. Sickness absence, the total number of days that workers were absent from work due to sickness, was also included. Moreover, a sickness absence of more than 3 days was documented. A question was included concerning physical examinations in the previous 12 months by an occupational physician. Sports activity was divided into three groups: The first group consisted of the participants with no regular exercise; the second group, those with less than three scheduled sports activities; and the third group, the participants with three or more scheduled sports activities during the week. Resting time was defined as the total amount of time spent during the workday not working including lunch breaks.
The questionnaires were distributed to packaging employees in each company. After the questionnaires were completed, the working posture of each employee was assessed using the RULA method. The researchers invited trained ergonomists to score the postural assessments. Diagrams were anonymous, and the ergonomists were not informed about the presence or absence of pain in these employees. The scoring process was completed at random times during work hours. The researchers included those employees who had completed parts pertinent to the LBP and neck pain in the previous 12 months for this study (blank answers were excluded). If other questions were unanswered, the questionnaires were not excluded from the analysis and the completed sections were included.
The employees were informed of the purpose of the study and that they could choose not to participate. The process of completing the questionnaires or posture assessment using the RULA method did not influence by any means the salary or employment status of any employees (e.g., results were anonymous). Employees were free to withdraw from the study at any time. This study was approved by the ethics committee of Iran University of Medical Sciences.
The gathered data were analyzed using the Statistical Package for Social Sciences software (SPSS Inc. Released 2007. SPSS for Windows, Version 16.0. Chicago, SPSS Inc). The variables were divided into two categories. Continuous variables are included in Table 1 and categorical variables in Table 2. For the continuous data, t tests were used to define statistically significant differences, and p values of less than .05 were considered statistically significant. For the categorical data, cross-tabulations and the chi-square test were used and the level of significance was the same (p < .05). The rapid upper limb score was considered a continuous variable, but when it was converted to an action level (1-4), it was considered a categorical variable. To evaluate all variables and reduce confounding effects, the variables which were significantly associated with the occurrence of LBP and neck pain were entered into separate binomial logistic regression models.
Results
Of the 461 employees, 396 returned the questionnaire (response rate = 85.9%). The high response rate was the result of a thorough explanation to workers and managers about the benefits of future ergonomic interventions (e.g., improved work efficiency) and classes conducted by the Deputy of Health to promote employee knowledge and understanding of ergonomics.
The average age of study participants was 34.9 ± 9.47 years; 158 women (40.8%) and 229 men (59.2%) were included in the sample. The prevalence of LBP and neck pain during the past 12 months was 34.2% and 27.5%, respectively. Only age, work experience, left arm RULA, and right arm RULA were significantly associated with LBP. Age, work experience, extra work hours, hours of work with a computer, and number of missed days from work in the previous year were associated with neck pain. Because only a few workers were categorized in Action Level 1, the researchers combined the first two action levels into one category.
Cross-tabulations and chi-square tests showed significant associations between absence from work more than 3 days, level of education, and sports activity and LBP. Gender, working posture, task training, absence from work more than 3 days in the previous year, sports activity, and RULA action level were significantly associated with neck pain. Variables significantly associated with LBP and neck pain were entered into separate binomial logistic regression models. Because age and work experience were collinear variables (Pearson correlation = .768, p = .001), only age was entered into the regression model. The same procedure was applied to collinear right arm and left arm RULA scores (Pearson correlation = .815, p = .001); the left arm RULA score was entered into the model. Left arm and right arm RULA action levels were also collinear (Pearson correlation = .894, P value = .001) and the left arm RULA action level was entered. Because the absence from work more than 3 days in the previous year could have been a direct result of the LBP or neck pain, it was not entered into the model. The results of the binomial regression models are presented in Table 3 for LBP and in Table 4 for neck pain. Only the left arm RULA score and education were predictive for LBP, and age, gender, working posture, and task training were significant predictors for neck pain.
Binary Logistic Regression Model for Low Back Pain
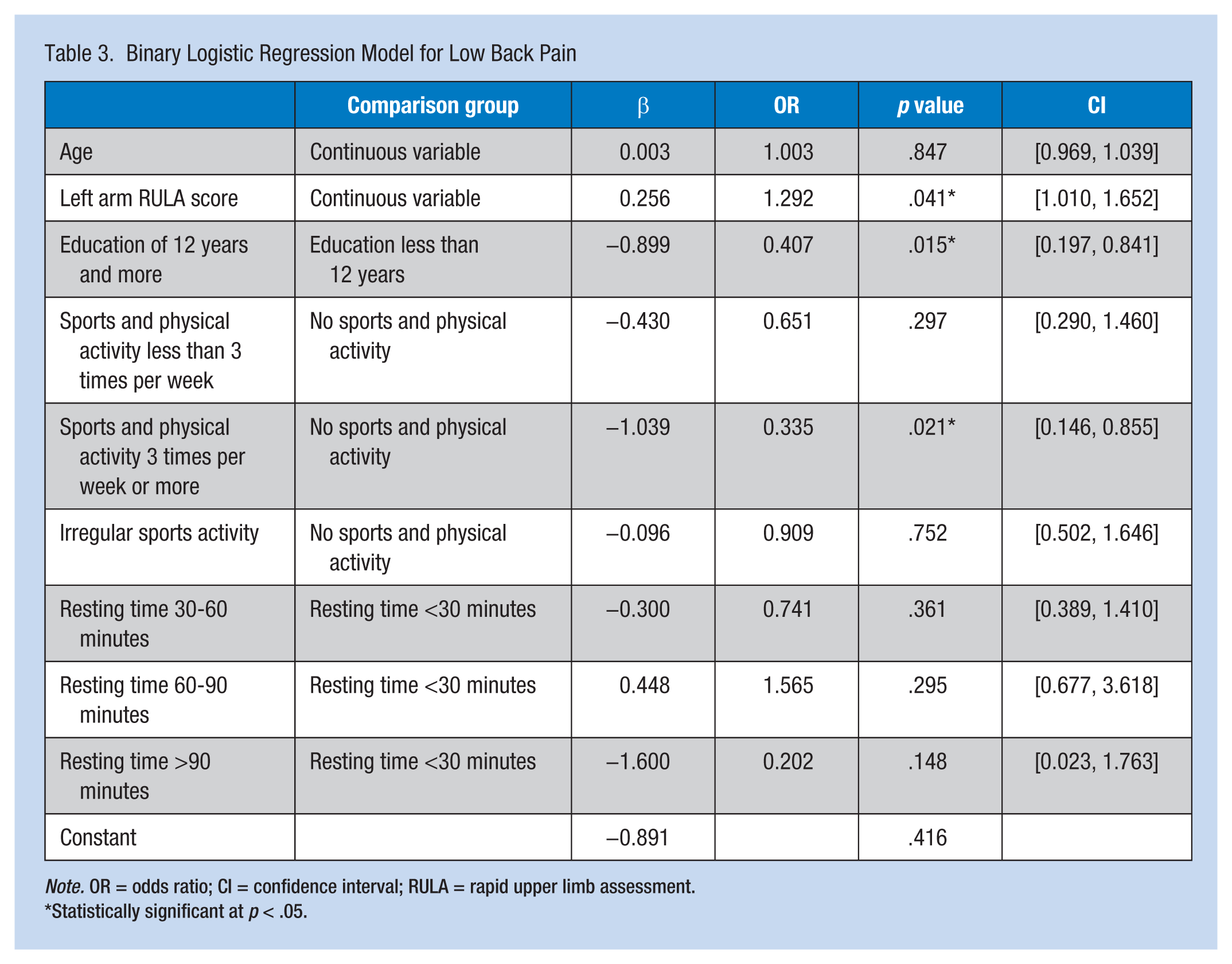
Note. OR = odds ratio; CI = confidence interval; RULA = rapid upper limb assessment.
Statistically significant at p < .05.
Binary Logistic Regression Model for Neck Pain
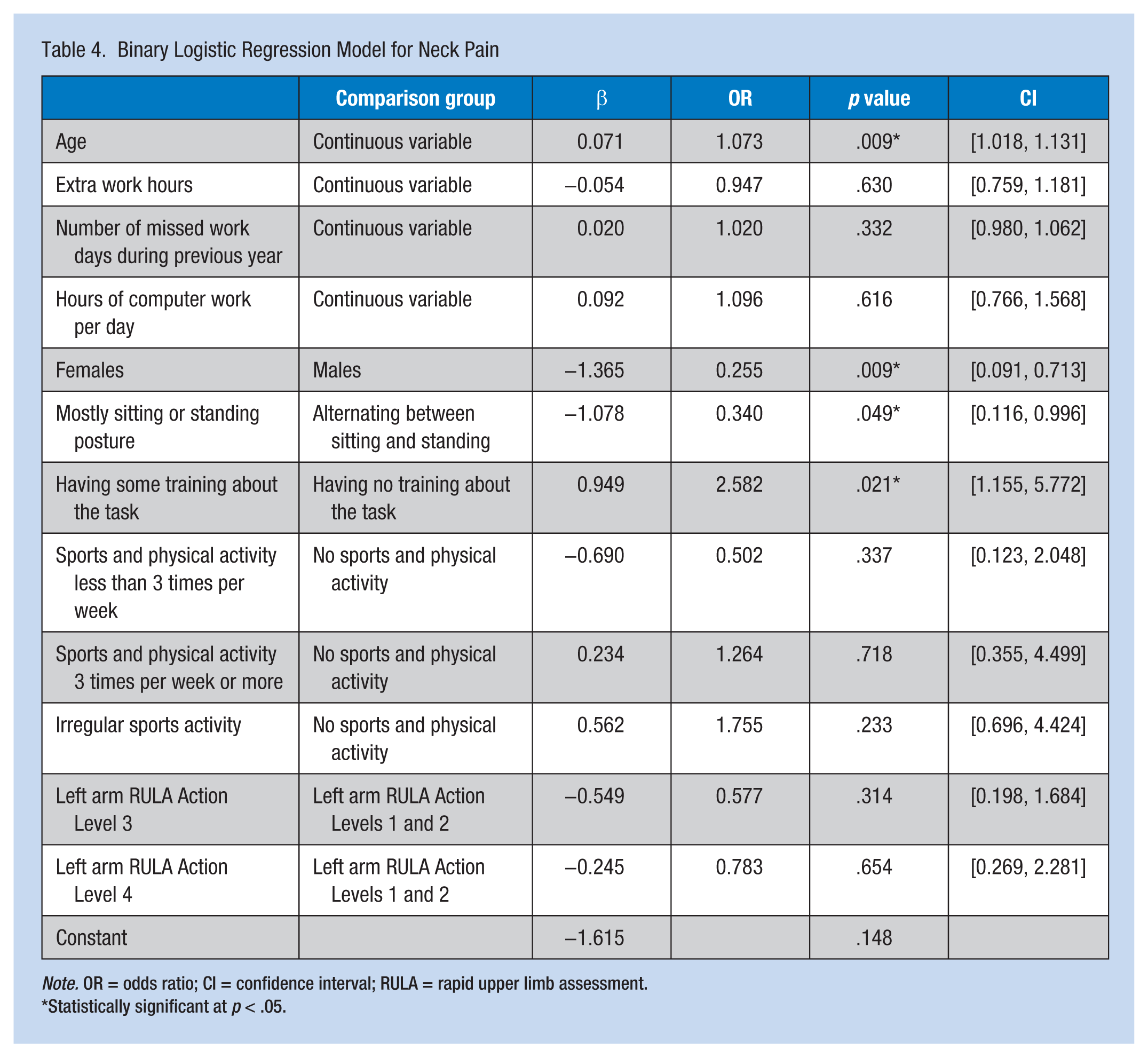
Note. OR = odds ratio; CI = confidence interval; RULA = rapid upper limb assessment.
Statistically significant at p < .05.
Discussion
After adjusting for confounding effects, the researchers found that RULA score and education were significantly predictive of LBP in pharmaceutical packaging employees. For neck pain, predictive variables were worker age, work experience, gender, subjective working posture, and task training.
In other studies conducted primarily in developing countries, education, age, work experience, and awkward postures were associated with LBP; the prevalence of LBP in these studies was approximately 40% (Arsalani et al., 2011; Ekpenyong & Inyang, 2014; Li et al., 2012; Sadeghian, Kasaeian, Noroozi, Vatani, & Taiebi, 2014). In studies on neck pain conducted primarily with dentists and teachers, gender, age, work experience, and static posture (e.g., sitting or standing) were significant predictors (Bernard & Putz-Anderson, 1997; Chiu & Lam, 2007; Rafie et al., 2015; Tirgar, Javanshir, Talebian, Amini, & Parhiz, 2015; Yue, Liu, & Li, 2012). The results of this study confirm previous studies of light work and demonstrate similar results in pharmaceutical packaging units.
Even though results of the t-test analysis suggested that age was significantly associated with LBP and neck pain (employees with LBP were about 3 years older than those without LBP), age was not significantly predictive in the regression model. In contrast, the mean difference in age of 2.5 years between those with and without neck pain was significant, and age was retained as a significant predictor in the regression equation. A similar outcome was observed for work experience which the t-test analysis suggested was longer for employees with LBP or neck pain than those employees who did not report either. In the regression analysis, age (which, due to collinearity, was used as a proxy for experience) was a significant predictor of neck pain but not LBP. Education was significantly lower for employees with LBP and was a significant predictor in the regression model. The researchers concluded that less education is a risk factor for LBP.
Posture can be assessed both subjectively and objectively. The RULA method has been used as an objective method for assessing postural or ergonomic upper extremity risk factors. Previous articles have supported the benefits of using RULA to assess LBP (Massaccesi et al., 2003). The RULA score in this study was about 0.25 points higher in the LBP group, and the score was a significant predictor in the regression model. Because RULA is easy to perform, the researchers recommend RULA to predict LBP in workers assigned high-risk tasks.
Rapid upper limb assessment was not associated with neck pain but when categorized into action levels, RULA was significant. However, RULA action levels were not predictive in the regression model. Subjective responses about work posture (i.e., static posture vs. alternating between sitting and standing) were significantly associated with neck pain which highlights the role of posture as a risk factor for this disorder. Female gender was associated with neck pain, a finding consistent with the literature. Those workers who received training for tasks associated with neck pain actually reported more pain than those employees who received no training. The reason for this finding is unknown. Absence from work more than 3 days due to any cause was significantly associated with pain in both anatomical regions. Because this study was cross-sectional, it is not clear whether the absence preceded the pain or the absence was due to the pain.
The most significant limitation of this study was its cross-sectional design which cannot establish causation; a longitudinal design is recommended for future research. This study was conducted in the packaging units of pharmaceutical companies where workers were engaged in light tasks. These data are not expected to apply to workers in other industries working under different conditions. The researchers recommend additional studies in other industrial settings to define specific risk factors for those workers. Moreover, this sample population may not be representative of workers in other countries. However, the study may represent working conditions in developing countries. The lack of random sampling also reduced the external validity of study results. Because workers were asked to recall information from the past 12 months, recall bias may also be an issue. Asking about experiences in the past month may reduce this bias. A questionnaire was used to define risk factors (except RULA) for LBP and neck pain (i.e., workers were not examined), so most of the data were subjective. Even though the workers were ensured confidentiality, some may not have provided accurate data, and thus, disease rates may have been underestimated.
This study had several strengths. The researchers chose to study a group of light manual workers to assess risk factors other than heavy lifting, a variable that is often considered in industrial settings. This study population had not previously been assessed for ergonomic risk factors. Nine different companies were included in the study so that the sample was more representative of industries in Tehran Province. All risk factors were also compared with the occurrence of shoulder and wrist pain as well as LBP and neck pain; the study was designed to identify specific risk factors for specific body region pain. Rapid upper limb assessment, an objective measure, was used to predict musculoskeletal pain of the upper limbs. The researchers concluded that RULA, education, and absence from work more than 3 days predict the occurrence of LBP. For neck pain, age, gender, absence from work more than 3 days, and subjective working posture are the best predictors.
Implications for Practice
This article can familiarize occupational health nurses with WMSDs, particularly LBP and neck pain, and their significance for workers and management. In addition, the article acquaints nurses with ergonomic assessment tools such as RULA and the concept of action levels and appropriate ergonomic interventions at each level. Finally, this study highlights tasks performed by pharmaceutical packaging employees and workers’ risk factors for LBP and neck pain. These variables may offer managers, and occupational health and safety professionals, guidance for better resource allocation and disease surveillance.
Applying Research to Practice
This study demonstrated that RULA, an objective assessment of posture and guide for prioritizing high-risk tasks, and education can predict LBP in pharmaceutical packaging employees. Age, gender, and work posture can predict neck pain for the same workers. Absence from work more than 3 days in the previous year was associated with both types of pain. The results of this research are applicable to light-task manual workers. Prioritizing high-risk employees can guide screening and surveillance resource allocation decisions.
Footnotes
Conflict of Interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Author Biographies
Yasser Labbafinejad graduated from Tehran University of Medical Sciences and completed his occupational medicine specialty in 2006. He is now associate professor in occupational medicine at the Department of Medical Faculty of Iran University of Medical Sciences.
Zahra Imanizade graduated from Iran University of Medical Sciences and completed his occupational medicine specialty training in 2016.
Hossein Danesh graduated from Iran University of Medical Sciences and completed his occupational medicine specialty training in 2016.