
Abstract
In the technological era, changes are happening around the globe at a fast rate. In this regard, healthcare organizations are implementing changes to improve their process. Hence, to manage implemented changes, there is a need to assess AI capabilities, cybernetic thinking (CT), organizational ambidexterity (OA), and employee wellbeing (EWB). However, no validated scale exists specifically to measure the aspects mentioned earlier in the context of healthcare organizations (HCO). Accordingly, our study attempted to validate existing scales of AI capabilities, CT, OA, and EWB in the context of HCO. Besides, to attain this purpose, a pilot study was led on a sample of 150 doctors employed in private sector hospitals in Pakistan, and data were analyzed using CB-SEM. This study confirms the validity and reliability of the refined scale in the context of a Pakistani healthcare setting. From the practical context, healthcare organizations can use the validated scale to assess their capacity towards adopting emerging technologies. These scales can be used to formulate strategies for managing technological change from both organizational and employee perspectives in healthcare settings. In addition, this study offers a multidimensional perspective by integrating diffusion of innovation theory (DOIT) with AI capabilities, EWB, CT, and OA to specify how innovation diffuses across complex systems, such as healthcare settings.
Plain language summary
This study attempted to validate the scales of AI capabilities, cybernetic thinking, ambidexterity, and employee well-being to manage technological change. Therefore, a pilot study was run on a sample of 150 doctors working in private-sector hospitals, and collected data was analyzed using CB-SEM. Based on the analysis the validated scales were reported in the context of a developing country like Pakistan to evaluate their capacity towards opting the emerging technologies.
Keywords
Introduction
Nowadays, dynamic changes have been observed in all sectors, including the healthcare setup around the globe, regarding the inclusion of emerging technologies. Among them, artificial intelligence (AI) has taken a prominent place in all areas of businesses and organizations including the service sector. At present, this major shift on the technology side falls under the category of the industrial (fourth) revolution (McKinsey & Company, 2022; Schwab, 2016), machines or algorithms’ second age (Brynjolfsson & McAfee, 2014; Danaher et al., 2017). This major shift is possible through the use of machine learning, natural language processing, image recognition, machine vision, and decision-making systems, leading to the transformation processes (Baabdullah, 2024; Walsh et al., 2019).
Behind this transformation, the most prominent driver is the implementation of AI technology (Bankins & Formosa, 2023; Fassa et al., 2019). On the other hand, this technological shift is transforming individuals’ working patterns and productivity (Bankins et al., 2024). Accordingly, AI refers to the assortment of various technologies that help resolve problems related to processes, working patterns, and customer experience (Wulff & Finnestrand, 2024). Hence, human and machine interaction is changing work dynamics, which in turn improves organizational processes and operational performance (Chen, 2024).
This interaction can be possible when organizations proactively think, act, and communicate using a cybernetic system to meet stakeholders’ needs about technological adoption (Osmanoglu, 2025). The notion of cybernetics was introduced in 1948 by Wiener’s (1948), as a system to control and streamline communication between humans and machines. Thus, communication is a foundational aspect to facilitate this technological change. Accordingly, cybernetics focuses on information processing to streamline structures (Groumpos, 2024). Thus, communication channels can play a critical role in processing and dissemination of information to facilitate behavioral change for technological adoption (Walter, 2024).
In addition, various aspects are required to build a Cybernetics system for the development of effective communication and feedback mechanisms using electronic circuits, brains, and organizational stakeholders to create synergy among all (Baltazar, 2021). In line with this, to facilitate change, cybernetic thinking (CT) includes a link between communication, adaptation, feedback loops, and control systems (Wong, 2023). For instance, during AI implementation, it helps to form a value and knowledge-based relationship between the organization, human, external environment, and society (Lavanderos, 2022). Hence, CT is seen as a new tool for the organization to manage the adaptation with intact control systems (Wong, 2023) and communication to manage human work relationships during AI implementation (Canbul Yaroğlu, 2024).
Accordingly, CT is a critical aspect to manage AI implementation along with protecting employee well-being (EWB), an area of concern for today’s organizations. Different views were presented about AI implementation and EWB within the organization, such as unemployment, pressures, or fear (Frey & Osborne, 2017). All these factors lead to affecting EWB in a negative manner. The prime reason behind this influence is perhaps reliant on AI mischaracterization displayed in science fiction related to emerging technologies and the societal narrative (Cave et al., 2018). Contrary to this, intact management support and communication during AI adoption can transform the process; as a result, EWB can be enhanced (Soomro et al., 2024). Likewise, other studies also report positive outcomes, such as improved work productivity (Al Naqbi et al., 2024), employee well-being (Feijóo et al., 2020; Oosthuizen, 2019), and organizational performance (Olan et al., 2022).
Consequently, wellbeing is linked to how happy and satisfied an individual feels about their job (Anitha & Shanthi, 2020). For instance, in what way is EWB protected during AI adoption? However, when effective measures are taken, such as reskilling and upskilling to deal with technological innovations within the organization (Bodea et al., 2024) creates a synergy among teams to perform well, leading to improved EWB (Babu et al., 2024). Undoubtedly, the future of all organizations will be tech-driven, and EWB remains the most important aspect to be protected in the advent of AI technologies on the other side.
EWB can be protected by adopting effective exploration and exploitation strategies when implementing AI (Stovall, 2023). During AI implementation and adoption of innovative technologies, the notion of organizational ambidexterity (OA) can play a role (Chakma et al., 2024). In OA, the emphasis on the exploitation aspect warrants the current organizational viability and exploration to ensure the forthcoming organizational viability (Levinthal & March, 1993; Yunita et al., 2023). Accordingly, OA is a potential force that ensures the service and cost excellence and organizational efficacy. This efficacy is attained by implementing AI and robot technologies that can support various tasks (Wirtz, 2020). Without OA, an organization cannot stand out in the market and fall behind in taking advantage of AI adoption (Sliż & Jackowska, 2025).
Even though researchers have developed scales on AI, CT, OA, and EWB to accurately capture phenomena in other contexts. However, no validated scale has been established till today to measure the abovementioned aspects from the diffusion of innovation theory (DOIT) perspective in the Pakistani healthcare setting. Investigators propose that there is a need to assess AI implementation in different sectors and contexts with different factors (Böhmer & Schinnenburg, 2023). To cover the existing gap, our study attempted to substantiate the existing scale in Pakistani private sector hospitals by conducting a pilot study. It is seen as a valuable addition to the literature that will help researchers and managers to use it in the future for further deliberations.
Theoretical Underpinning and Overview of Scales
Diffusion of Innovation Theory
Diffusion of innovation theory (DOIT) has been a widely used theoretical perspective in organizational settings (Rogers, 1981). It refers to sharing new concepts, ideas, philosophies, and practices from an innovation standpoint for the adoption and integration of technologies across organizations (Patnaik & Bakkar, 2024). The adoption process of innovation usually completes in five stages from emergence to implementation including (1) knowledge stage (exposure to innovation); (2) persuasion stage (favorable and unfavorable attitude); (3) decision stage (accept or reject adopted technology); (4) implementation stage (usage of innovation); and (5) confirmation stage (innovation is reinforced; Xia et al., 2022).
The abovementioned stages for technological adoption can be completed (Martins et al., 2016) via using different communication channels (Rogers et al., 2014), along with leadership, as well as considering internal and external organizational factors (De Mattos & Laurindo, 2017). Referring to internal organizational factors, technological adoption can be challenging for managers due to employees’ reluctance and unwillingness to accept changes introduced across different levels (Yousif et al., 2024). This challenge can be overcome by using communication channels to portray the advantages of technological innovation to lessen employees’ reluctance (Patnaik & Bakkar, 2024). Here, CT can play a critical role. It refers to developing system thinking and communication channels to gather feedback from stakeholders and adopt technological innovations (Osejo-Bucheli, 2025; Pfiffner, 2022). Hence, the use of AI across various organizational functions can lead to building confidence and resilience among employees to manage such change (Espejo, 2017; Espejo & Reyes, 2011). Therefore, developing and implementing AI capabilities can transform organizational functions; as a result, it offers a relative advantage in process automation (Brynjolfsson & McAfee, 2017). Adjacent to this, AI adoption can improve or lessen EWB. However, it depends on communication, and the way the problem is solved through AI. Consequently, it lessens the frustration level and EWB can be preserved and improved (Sadeghi, 2024). Moreover, innovation is a significant factor in determining individual determination for technological adoption and fostering better outcomes such as performance and wellbeing (Labay & Kinnear, 1981).
In line with the above argument, exploration is one of the key dimensions of OA that involves the early adoption of technological innovation, and exploitation leads to improving existing processes. These dimensions enhance employee confidence as well as build trust to grasp the technological change as an opportunity, as a result fostering wellbeing. DIOT is applied in several organizational contexts (Xu et al., 2024) related to the technological adoption in the accounting profession (Assidi et al., 2025), and cloud computing adoption in supply chain management (Amini & Jahanbakhsh Javid, 2023). However, the application of DIOT in the context of AI capability, EWB, OA, and CT remains inconclusive in the extant literature related to healthcare settings.
AI Capabilities
For organizations, AI is a foundational base for success in digital servitization and innovation. Innovation can be adopted by investing in infrastructure, technologies, and data. Thus, the artificial component is linked to the manufactured side, and intelligence refers to acquiring information from the available data and life experiences to learn and build the capability to perform (Chowdhury et al., 2023). However, this is not enough; Chowdhury et al. (2023) and Sjödin et al. (2021) elaborated that AI technology adoption requires new skills and capabilities that help in improving operational processes.
Hence, AI capabilities involve developing a system to utilize organizational resources to improve operational efficiency and make informed decisions. Moreover, it varies from industry to industry and sector to sector. According to Sjödin et al. (2021), context-specific AI capabilities relevant to the organization or culture need to be assessed. Moreover, researchers call for seeing the role of AI capabilities in different industries and sectors to broaden the scope of AI-related studies (Böhmer & Schinnenburg, 2023). To understand AI capability, it is necessary to validate the existing scale in private-sector hospitals of Pakistan, especially among the key players, that is, doctors. To attain this purpose, the AI scale was taken from the authors (see Mikalef et al., 2022; Mikalef & Gupta, 2021). Table 1 displays elaboration presented by investigators related to the existing AI scale in the extant literature.
AI Capabilities.

Employee Wellbeing
EWB refers to individual psychological, physical, and emotional health to ensure comfort and happiness. In today’s technological era, organizations have adopted different approaches to improve EWB, such as flexible methods, a clock schedule for work, and thinking out of the box, to facilitate the smooth functioning (Buick et al., 2024; Myrvang, 2020; Panda & Rath, 2018). These approaches grasped the employees’ attention due to the flexibility offered by the organization, performing assigned roles, especially in stressful working environments such as hospitals (Mahendra & Kurniawati, 2024).
Likewise, employees working in the education and hospital sectors suffer from burnout, stress, and emotional exhaustion (Angioha et al., 2020; Marquez, 2024; Sohani et al., 2024). In unification with this misery, sustaining wellbeing is a perceived challenge during AI adoption for service organizations (Deswal & Arora, 2025). However, understanding the EWB is still inconclusive and needs further deliberation to manage technological change (Pradhan & Hati, 2022) in healthcare settings. Achieving resilience among employees requires strong organizational support and practices to accept changes, enhancing EWB (Johnson et al., 2020). Table 2 indicates elaboration related to the EWB scale and related dimensions in the existing literature.
Employee Wellbeing.

EWB is a key issue for doctors in particular, when a service organization adopts technological innovation. It is important to have a contextual scale to evaluate EWB in today’s digital era (Feijóo et al., 2020; Oosthuizen, 2019). Therefore, this study attempts to fill this gap by validating the scale taken from Juchnowicz and Kinowska (2021) to assess EWB among doctors working in Pakistani private sector hospitals from the perspectives of relationships, work-life balance, and physical and psychological health.
Cybernetic Thinking
Cybernetics involves steering, navigating, or governing the process by internalizing the feedback loop. This can help to decide actions based on the input and output received (Maden et al., 2022), leading to understanding and thinking about problems in a cybernetic manner to manage algorithms and data during the advent of AI (Krippendorff, 2021). CT eliminates the risks and socio-technical issues during AI execution in organizational systems by streamlining the input and output (Maden et al., 2022).
In a complex system, cybernetics is defined as a science that assesses the organizational abstract principles from the information imported and employed in the system with intact controlling actions to achieve goals despite various turbulences (Álvarez-Fontalvo et al., 2024). Cybernetics is a tool for assessing and controlling individual behavior to attain the designated goals (Peña-Ayala & Cárdenas-Robledo, 2019). Moreover, cybernetics involves purposes, values, sensorial mechanisms, and feedback to manage systems labor for goal achievement. Thus, it refers to goal-directed and self-regulating systems (DeYoung, 2015; Wiener, 1948).
Referring to the above-mentioned arguments, regulation and control are the central aspects of cybernetics. Accordingly, Girolami et al. (2015) explained cybernetics as a meta-theory for complex model systems. However, DeYoung (2015) outlined it as an integrated theory. In addition, cybernetics has a transdisciplinary paradigm, designing a variety of systems including physical, ecological, biological, technological, and social models, or an integration of all to create synergy in working (Peña-Ayala & Cárdenas-Robledo, 2019). Contrary to this, cybernetics is an interdisciplinary platform that uses communication and decision-making tools to acquire, manage, and share new ways of doing things (Choudhury, 2024; Montagnini, 2017; Montagnini et al., 2016).
Moreover, cybernetic system thinking is a human-focused approach based on the integration of system theory, cybernetics, management science, and operations to deal with innovation to succeed from the designer’s perspective by executing technologies to meet people’s needs as well as business requirements (Forlano, 2025; Greene, 2019; Krippendorff, 2007). Understanding the CT principles, the first aspect is feedback controls behavior, and it is demarcated as a negative feedback loop to lessen deviations from the expected outcomes (Fischer & Riedl, 2015), and works on the self-regulating system to better comprehend and manage human behavior. Therefore, Key aspects of cybernetics include feedback loops, control systems, adaptation, and communication (Wong, 2023), to acquire new knowledge (Armenia et al., 2023), leading to influence wellbeing and firm performance (Raiden et al., 2020; Salas-Vallina et al., 2022). Figure 1 indicates the organizational CT, such as communication, conduction, coordination, cohesion, co-autonomy, and centralization (Lavanderos, 2022). However, limited CT scales exist. This study attempts to validate the CT scale of Greene (2019) in the context of Pakistani private sector hospitals among doctors.

Structure of cybernetics.
Organizational Ambidexterity
OA is a process of adapting a technology effectively by considering knowledge as a key resource for implementing incremental and radical change (Chakma et al., 2021). Accordingly, two factors are involved in OA such as exploitation and exploration. The exploitation side focuses on amplifying the revenues. Contrary to this, this side cannot accept environmental and technological changes. However, the exploration side of OA can accept these changes to bring innovation (Gschwantner, 2018). Therefore, exploration and exploitation can support the adoption and acceptance of technological innovation in an organization by streamlining both sides, including revenue generation and embracing technology, leading to improved market presence (Koryak et al., 2018).
Accordingly, ambidexterity refers to the ability to meet external environmental demands by accepting, adopting, and executing technological changes (Hwang et al., 2023; O’Reilly & Tushman, 2011; Restuputri et al., 2024). This means OA can support the change process and can have an impact on AI adoption and EWB. In addition, evidence found that OA creates a trust culture by ensuring consistency among key stakeholders (Sorsanen, 2009), through the timely sharing of information with team members (Çelik & Uzunçarşılı, 2023). As a result, wellbeing is affected (Salas-Vallina et al., 2022) and performance (Dranev et al., 2020).
The OA notion has gained popularity among investigators and practitioners. It can influence organizational management, learning, and technological innovation (Kassotaki, 2022). Apart from its significance for today’s organizations, limited studies exist about the applicability of OA in the healthcare setting. This study attempts to validate the OA scale taken by the authors Lubatkin et al. (2006) and Ojiako et al. (2023). Table 3 shows the elaborations related to the OA scale in existing literature.
Organizational Ambidexterity.

Method
Participants and Scale Validation Overview
A pilot study was conducted on a small sample to validate the scales before the data collection on a larger sample size. To achieve this purpose, data were collected from doctors working in private sector hospitals in Pakistan using convenience sampling with a sample size of 150 to validate the scales. Hence, several measures were incorporated to limit the potential risks of harm to the respondents: first, minimization of risk through ensuring voluntary participation. Furthermore, no physical and psychological risks were involved, as respondents were not exposed to any intervention. Moreover, this study offers potential benefits to society by providing a validated scale that can help improve the adoption of emerging technologies and the decision-making process in the healthcare setting. Henceforth, the following aspects were incorporated into the consent process, providing a detailed explanation of the study’s purpose to the respondents, ensuring the voluntary participation of all respondents, and data collected would be kept confidential.
To complete the data collection process, 200 questionnaires were disseminated. Only 150 were received in a duly filled manner for further analysis. Among the respondents, there were n = 86 male doctors with a percentage of 57.3, and n = 64 were female doctors with 42.7% in the sample. In addition, 8.7% (n = 13) of doctors with 1 to 2 years of experience represent the sample, 24.7% (n = 37) with 2 to 3 years of experience, 38.7% (n = 58) with 3 to 4 years of experience, and the remaining 28% (n = 42) with >4 years of experience. In addition, as far as education level is considered, 63.3% (n = 95) represent the sample with bachelor’s, 27.3% (n = 41) with master’s, and 9.3% (n = 14) with PhD degrees. Moreover, referring to job title, 12.7% (n = 19) represented the sample as house officers, while the remaining 78% (n = 117) represented as medical officers, and 9.3% (n = 14) as postgraduate residents. Table 4 shows the scale validation overview. Moreover, respondents were presented with 70 items measuring AI capabilities, OA, CT, and EWB.
Scales Validation Overview.

Measures
To measure AI capability, EWB, CT, and OA scales were taken from different sources for validation in a Pakistani healthcare setting, particularly private hospitals. Details about each scale in mentioned in Table 5.
Scales Overview.

Data Analysis Procedure
Firstly, the descriptive analysis was performed to see the sample representation. Moreover, “KMO” as well as “Bartlett’s test of sphericity (BToS)” to assess sampling adequacy, and “Harman’s single (exploratory) factor test (HSFT)” to assess common method bias were performed by utilizing Jamovi software on each aspect of AI capabilities, CT, OA, and EWB. Additionally, CFA was run to see the underlying structural outline using PLS (CB-SEM). The reason for using CB SEM was to assess the measurement model in terms of fitness indices. PLS and CB-SEM are complementary, nonparametric, and variance-based approaches used in studies (Sarstedt et al., 2023). However, CB-SEM explains the covariance among the related indicators and constructs that were taken as common factors (Rigdon et al., 2017). In addition, CB-SEM has higher accuracy compared to PLS-SEM, and CB-SEM helps to better recover the parameters than PLS-SEM.
The reason for choosing CB-SEM over PLS-SEM was to test the theory and assess model fit rather than prediction, and when the data met sampling adequacy (Hair et al., 2018). Therefore, this study was focused on validating the scales based on DIOT. Henceforth, CB-SEM was an appropriate choice. Contrary to this, PLS-SEM is considered suitable for prediction rather than model fit assessment (Hair et al., 2013; Sarstedt et al., 2014). Thus, goodness of fit indices, item loadings, validity, and reliability were examined using CB-SEM. Details of each executed technique are shown in the subsequent section.
Assessment before Factor Analysis
An assessment of sampling and correlation matrix adequacy is a crucial test to be performed before factor analysis. For sampling adequacy, the KMO test was employed; as per the result, the value was .719, which is >.60, meeting the threshold criteria as proposed by Murugesan et al. (2023). Therefore, the data was considered satisfactory for factor analysis. Moreover, BToS was employed to assess the adequacy of a correlation matrix. As per the result, a significant link exists among the variables as the p-value is <.001 with a χ2 = 26,283. This indicates variables are not orthogonal, and the sig value indicates the data set is appropriate for further analysis (Bilgiç & Aytaç, 2024).
Harman’s Single Factor Test
To evaluate common method bias (CMB), HSFT was run (Harman, 1976). As per the analysis shown in Table 6, there is no issue of multicollinearity in the data set, as the percentage of variance is 28.5% which is less than 50 as per the threshold recommended for CMB (Fuller et al., 2016). Therefore, data can be run for further analysis.
Harman’s Single Factor Test.

Results
Factor Loadings, Alpha Values, and Model Fit
Table 7 shows the factor loadings along with alpha values and items used (Bibi et al., 2025). All items were retained with factor loading values >.70 as per the recommendation of Cheung et al. (2023), while factor loading values <.70 were removed. Moreover, the model fit value of RMSEA falls under the threshold, that is, .05, showing that the model is reasonably fit as values fall between .05 and .08. On the other hand, CFI value is .94 again, which specifies an acceptable fit as values fall between .90 and .95. Likewise, TLI value is .91, which is again an acceptable fit as the value falls between .90 and .95 as per the recommendation of Hu and Bentler (1999). The measurement model (CFA) graphical illustration is shown in Figure 2.
Model Fit Indices, Outer Loading, and Cronbach’s Alpha.

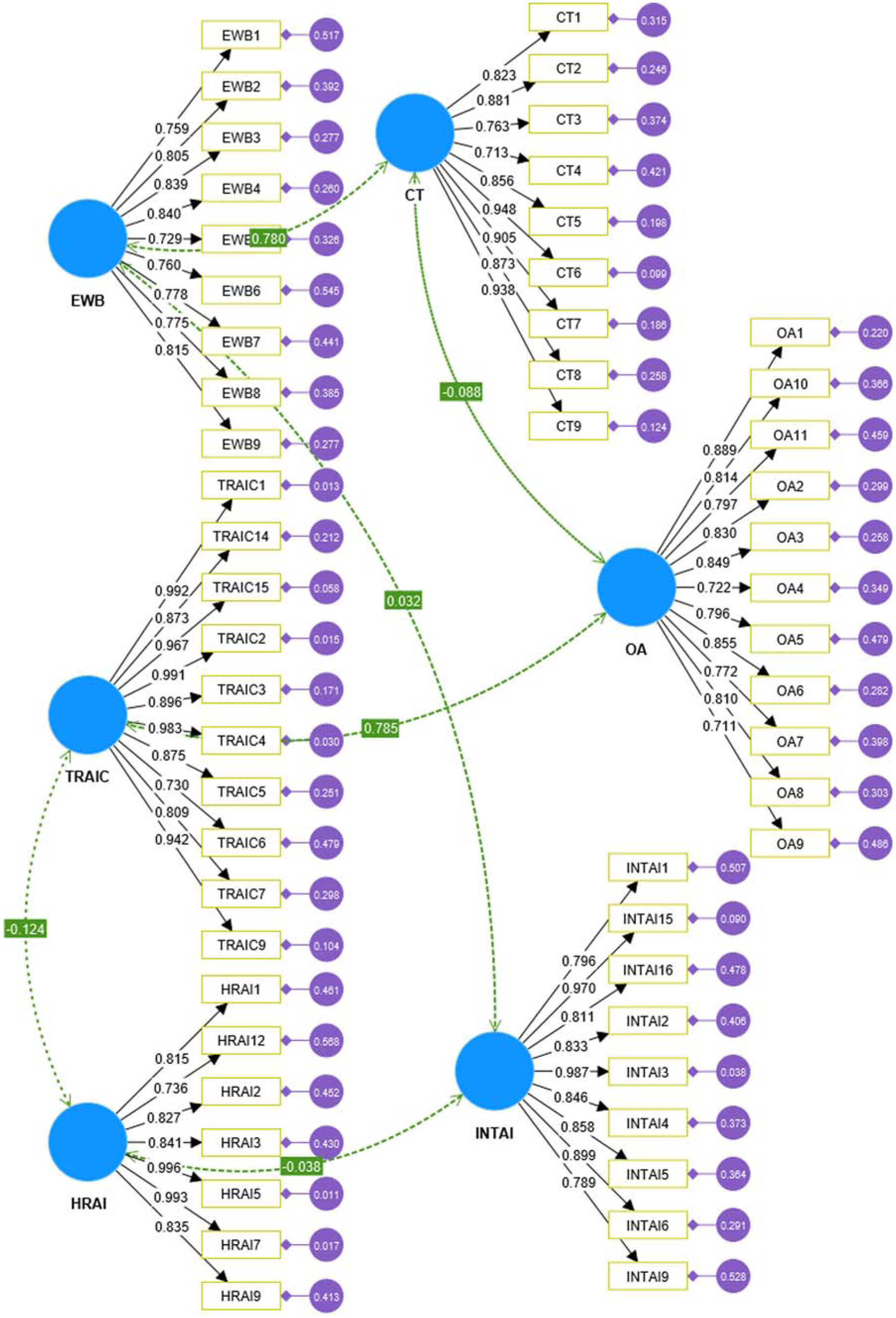
Confirmatory factor analysis.
In addition, Table 8 shows the estimation parameters of latent variables to assess the indicator’s variance and covariance. Latent variables are seen as the indicator’s parameters. All latent variables have been significant parameters for the indicator, with a p-value (<.001) for each variable.
Estimated Parameters of Latent Variables.

As per Table 9, CR values fit with the suggested threshold of >.70. Moreover, AVE values >.50 also show that it meets the suggested value (Dos Santos & Cirillo, 2023; Niclasen et al., 2013). Thus, there is no issue of validity as well as reliability in the data analyzed.
Scales Validity and Reliability.

Note. AVE = average variance extracted; CA = Cronbach alpha; CR = composite reliability.
As per Table 10, all construct values fall under .85 as suggested by Cheung et al. (2023) and Henseler et al. (2015). Therefore, the discriminant validity is achieved for all constructs.
Discriminant Validity.

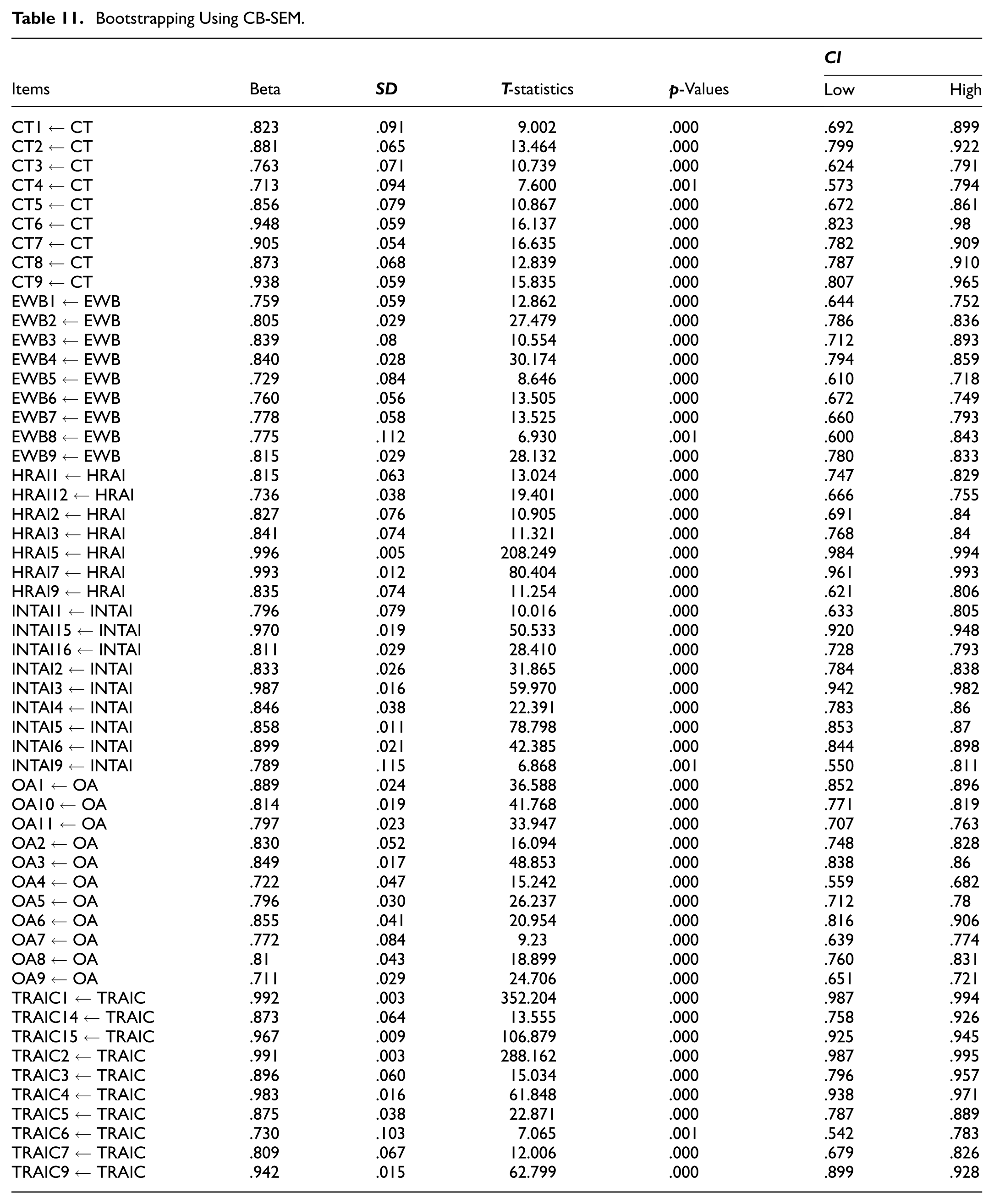
Furthermore, bootstrapping was run in CB-SEM to assess the significance of the validated scale. All the specified loadings are significant as shown in Table 11.
Bootstrapping Using CB-SEM.
Discussion and Conclusion
This study attempted to validate the developed scale on AI capabilities, OA, CT, and EWB for doctors working in Pakistani private sector hospitals. Our study provides an empirically validated scale that researchers and practitioners can use to assess the link between AI capabilities, OA, CT, and EWB from the theoretical lens of DOIT. Results indicate a good fit, along with the reliability and validity of the scales. So, AI capabilities are viewed as intangible resources, tangible resources, and human resources. The questionnaires were taken from Mikalef et al. (2022), Mikalef and Gupta (2021) to apply and validate in the Pakistani context. Moreover, to measure EWB, the scale was taken from Juchnowicz and Kinowska (2021) to evaluate relationships, work-life balance, and physical and psychological health. Furthermore, CT was assessed using the scale adapted from Greene (2019) to evaluate the communication and feedback loop. Lastly, the scale was adapted from Lubatkin et al. (2006), Ojiako et al. (2023) to measure OA. However, a few items were excluded due to the low factor values according to the results of our study.
Organizations need to assess their capabilities in an era of technological changes related to AI capability, EWB, CT, and OA. Therefore, it is important to have a scale to determine the aspects in different sectors and contexts with different factors (Böhmer & Schinnenburg, 2023). Our study filled this gap by validating the scale in healthcare settings. Accordingly, this integrated approach to validate the scale for the healthcare setting in this study can be used by practitioners to assess their capabilities to adopt the technology promptly. This study provides a framework for understanding an employee-centric approach to how innovation, like AI, can affect organizational systems. In addition, DOIT’s integrated framework with AI capabilities, CT, OA, and EWB demonstrates that effective execution requires an ecosystem within a complex organizational setup like healthcare. This integrated framework will help lower the adoption barrier and create a comprehensive foundation for the sustained adoption of innovation in healthcare organizations.
It is concluded that healthcare organizations can use the validated scale to assess their capacity, processes, efficiency, communication, and control mechanisms towards adopting innovation such as AI from the view of organizational tangible, intangible, human resources, CT, EWB, and OA. Moreover, using DOIT as a theoretical lens to formulate a strategy regarding the development of organizational capabilities to meet the organizational demand for adoption of technologies, leading to improved existing processes, and EWB using effective communication channels.
Theoretical and Practical Implications
Our study has made the following contributions. Initially, our study seals the gap by validating the scale related to AI capabilities in private sector hospitals in Pakistan as per the call of Böhmer and Schinnenburg (2023). Furthermore, this study contributes to the theoretical development of DIOT (Rogers, 1983, 1987) by applying it to the AI implementation in healthcare settings, particularly private sector hospitals in Pakistan. In addition, this study offers a multidimensional perspective by integrating DOIT with AI capabilities, EWB, CT, and OA to specify how innovation diffuses across complex systems like healthcare settings. In addition, the scales provide empirically grounded tools for assessing how the organizational and individual factors can influence the adoption, adaptation, and internalization of AI innovation across various elements of DOIT, which are not represented in prior studies. This study enriches the extent of DOIT not only from the theoretical context but also provides a robust measurement tool to be used by researchers and practitioners. This study also shows that innovation diffusion is embedded in human systems and organizational factors, contributing to the validation of measurement tools that can be used for meaningful analysis across various settings and cultures.
This study extends the DOIT (Rogers, 1983, 1987) perspective on AI capabilities, OA, CT, and EWB. To provide a holistic framework, five elements of DOIT are used to develop a guide for integrated AI using a people-centric approach in which AI capabilities affect EWB in the presence of CT and OA, as mentioned in Table 12.
DOIT Application to AI Capabilities, EWB, CT, and OA.

From the practical context, healthcare practitioners can use the AI capability scale to assess their capacity for adopting technologies from the perspective of tangible, intangible, and human resources. This will help identify gaps from the capability perspective on technological readiness to automate the process using AI to align the operational priorities, such as diagnostic and patient management, using AI capabilities. Furthermore, the EWB validated scale can be used by practitioners to track the work-life balance, relationships, and physical and psychological well-being among the doctors working in private sector hospitals during AI implementation, thereby enabling the timely use of interventions for better EWB. Therefore, the EWB scale can help managers manage job burnout, stress, and emotional exhaustion in the hospital context (Angioha et al., 2020; Bakker et al., 2005).
Subsequently, the OA scale can assess the balance between exploration (innovations like AI) and exploitation (existing processes). This may help in strategic alignment and allocation of resources to create a balance between exploitation and exploration levels. Moreover, the CT scale can be used to develop a feedback system that allows healthcare practitioners and managers to monitor the technological adoption and adjust the system and strategies based on doctors’ input.
Limitations and Directions for Future Studies
The following are the limitations of this study. Primarily, the sample size was limited to 150 doctors working in private sector hospitals in Karachi, Pakistan; however, it is relatively small and context-specific, which may limit the generalizability of the study and may not be representative of the public sector hospitals. Thus, the cultural norms, availability of resources, and sector-specific dynamics may differ in the public sector and other regions, affecting the generalizability of the provided insights. Therefore, future researchers may validate this scale on a larger sample size in public sector hospitals and conduct comparative research to expand the horizon and generalizability of the study, along with focusing on other geographical territories.
Moreover, future researchers may collect cross-level data from managers and nurses on AI capability, EWB, OA, and CT, as it remains unexplored in this study. In addition, the data was taken at one point in time. So, future researchers may examine this scale using longitudinal studies to capture the temporal specifications that surface between AI capability, CT, OA, and EWB. In addition, only CFA was run to validate the scale; future studies may use the validated scale to test the study variables’ relationship by keeping AI capability and EWB as predictors and outcome variables, and CT and OA as mediators or moderators between AI-EWB link using PLS-SEM for analysis on a larger sample size. Accordingly, these validated scales allow researchers to examine the mediating and moderating roles in innovation diffusion, like AI, to refine and expand the DOIT explanatory power.
Footnotes
Acknowledgements
This work was supported by a postdoctoral fellowship from the Universiti Malaysia Kelantan, Kelantan, Malaysia.
Ethical Considerations
The Faculty of Management Sciences, Bahria University, Pakistan, granted ethical clearance: Letter No. BUKC/DMS/2024 (111).
Consent to Participate
Not applicable as we declare that no data related to human medical intervention, and tissues were involved in this study. Principles of informed consent, data confidentiality, and voluntary participation were strictly followed.
Author Contributions
Munaza Bibi: Original draft, investigation, formal analysis, conceptualization, validation, methodology. Tse Guan Tan: Review & editing, original draft, supervision. Heng Yao: Analysis, review & editing.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data will be available on request.