
Abstract
Around the globe, technological advancements such as artificial intelligence (AI) are reshaping workplaces affecting employee wellbeing (EWB). To understand the AI-EWB link, a conceptual model is developed to explore the link between AI-driven capabilities and employee wellbeing (EWB), with cybernetic thinking (CT) as a mediator. Furthermore, organizational ambidexterity (OA) is introduced as a moderating factor between CT and EWB grounded on integrated dynamic capabilities with resource-based theory in the context of a developing country like Pakistan. Data were collected from 490 doctors working in private sector hospitals across two major cities of Pakistan—Karachi & Islamabad and data analysis was performed using PLS-SEM 4.0. Results indicate that AI-driven capabilities significantly relate to EWB. Furthermore, CT explains the relationship between tangible, human resources, intangible-driven AI capabilities, and EWB. In addition, OA moderates the link between CT and EWB. Hence, mediated moderation is established. To remain resilient, this study offers theoretical as well as practical insights into how healthcare practitioners can harness AI through integrating organizational factors like CT can help reduce stress and improve EWB through adopting a balanced approach to manage innovation. Policy implications along with directions for studies to be conducted by researchers are also provided.
Plain Language Summary
This study investigated the impact of AI capabilities on employee well-being with cybernetic thinking as a mediator between AI-driven capability and employee well-being (EWB). At the same time, organizational ambidexterity (OA) is incorporated as a moderator between cybernetic thinking (CT) and employee well-being. Based on collected data from 490 doctors the results indicate that tangible, human resources, and intangible-driven AI capabilities significantly relate to EWB. Furthermore, CT explains the relationship between tangible, human resources, intangible-driven AI capabilities, and EWB. In addition, OA moderates the link between CT and EWB.
Keywords
Introduction
The socio-economic environment has drastically changed the organizational dynamics after the pandemic in terms of unemployment, economic activities, and technological revolution around the globe, especially in developing countries (International Labour Organization, 2022; Viardot et al., 2023). The execution of artificial intelligence (hereafter, AI) and related technologies brings a drastic change in organizational processes that leads to stress and builds pressure among employees (Wald, 2020). This stress raises concerns for organizations to protect the employee wellbeing (hereafter, EWB) (Kaaria, 2024; Sadeghi, 2024). Stress can be lessened among employees during technological implementation through focusing on upskilling and reskilling to prepare them to manage such change (European Foundation, 2020; L. Li, 2022; Schwab, 2016; Xu et al., 2023).
Technological change like AI adoption can affect EWB positively or negatively (Dutta & Mishra, 2024), depending on how resources and capabilities such as how data, communication, and employees reaction are managed strategically in all sectors, including healthcare settings to sustain competitive advantage (Joshi et al., 2024; Tambe et al., 2019). Following Michael Porter’s view, positioning of organizational resources and capabilities can be a source of competitive advantage (Ghicajanu, 2021; Porter, 1980, 1985).
Past researchers have applied resource-based theory (RBT), explaining the significance of human and complementary resources to leverage the maximum benefits of capabilities apart from the technological resources to gain a competitive advantage (Gupta & George, 2016; Mikalef et al., 2018). Adjacent to this, Teece (2018) presented arguments on dynamic capabilities (hereafter, DC) to reconfigure the existing system using capabilities that can help in grasping the first mover advantage. For adapting complex technological changes, cybernetic thinking (hereafter, CT) can play a critical role in the integration of technologies across organizations using a communication and feedback loop mechanism (Nema & Sharma, 2024; Pao, 2023), which leads to lessening stress and enhancing EWB.
Reconfiguration of an existing system using AI technology is possible through an ambidextrous perspective (Duncan, 1976) by assessing the implementation of technological innovation in the management process. This process can be strengthened through a feedback mechanism from stakeholders, which may affect EWB either positively or negatively. Besides, researchers explained that organizational learning and ambidexterity during technological adoption may affect wellbeing-oriented management practices (Salas-Vallina et al., 2022) and CT to make informed decisions (Armenia et al., 2023), which can lessen the frustration due to timely communication, as a result, EWB can be affected (Muñoz-Pascual & Galende, 2020). However, work regarding the abovementioned aspect is missing in the literature.
Our study is going to fill this gap by investigating the link between AI-driven capabilities, including tangible such as technology, data, and basic resources, human resource AI capabilities such as technical, business as well as management skills, and intangible AI capabilities such as inter-department coordination and EWB (Clark, 2003; Dutta & Mishra, 2024; Wang et al., 2020). As of today, no study examines the mediating role of CT between AI-driven capabilities and EWB, while OA acts as a moderator between CT and EWB (Batra et al., 2022). This study responds to researchers’ call to evaluate how AI-enabled capabilities influence employee and organizational outcomes in the presence of other factors (Castellacci & Viñas-Bardolet, 2019) using the integrated DC and RBT theoretical lens in the context of a developing country like Pakistan. Therefore, the following research questions are projected in this study: 1) How do AI capabilities influence EWB? 2) How does CT mediate the link between AI capabilities and EWB? 3) How does OA moderate the link between CT and EWB? 4) How does the integrated DC with RBT framework fit within the AI context, CT, OA, and EWB?
Theoretical Underpinning
Dynamic Capabilities and Resource-Based Theory
The RBT (Barney, 2001) is a commonly applied theoretical standpoint on organizational resources that are difficult to find and reproduce (Bharadwaj, 2000). Later, the work goes into detail by differentiating between “resource-picking” and “capability-building.” According to the researchers, resources are tradable and nonspecific organizational assets, whereas capabilities are non-tradable specific organizational proficiencies for resource positioning, integration, and utilization (Amit & Schoemaker, 1993). Consequently, resources link to the input and production process, whereas capability links to these resources (Mikalef et al., 2020, 2021); leading to determine the organizational strengths (Makadok, 2001).
In healthcare, capability building requires exploitation and exploration of resources for effective management of human, technological and patient dealing, operations, collaborations, and decision prospects (Jia et al., 2023). Effective management is possible through the exploitation and exploration of resources (OA) with intact communication and feedback mechanisms to produce rare and inimitable resources (Barney, 1991). Under the canopy of RBT, resources can be used to develop capabilities using OA (exploitation and exploration) through developing a conducive environment (Guerra & Camargo, 2021), with a thinking system (effective communication and control mechanisms) to enhance the absorptive capability can lessen stress and result in affecting EWB (Johannessen, 2019; Nielsen et al., 2017). Yet, the RBT application on EWB has not been taken into consideration (Guest, 2017). Thus, there is a need to expand the theoretical context.
EWB notion should be viewed seen as a strategic issue to attain the competitive advantage rather than a peripheral matter (Chasserio, 2018), as it has become even more crucial concern with rise and inclusion of new technologies in organizational processes (International Labour Office & Labour Administration, 2016; Johnson et al., 2020; Rohwer et al., 2022). DC can allow firms to integrate internal and external competencies to build a system in order to manage technological dynamics to cease first mover advantage (Teece, 2018). However, the DC (Teece, 2018) integration with RBT (Barney, 2001) is often underexplored. To enrich the theoretical robustness of DC into RBT in the context of healthcare setting within the AI capabilities, EWB, CT, and OA link needs to be assessed to broaden the theoretical perspective (Chomutare et al., 2022; Joshi et al., 2024). Hence, this study attempted to fill this gap by evaluating the link between AI-driven capabilities, CT, OA, and EWB from the DC integrated RBT theoretical view.
Hypothesis Development
AI Capabilities and Employee Wellbeing
EWB is an employee’s overall quality of life because of positive work experience and functioning (Grant et al., 2007). In the literature, two perspectives are presented for EWB that is, the hedonic and eudaimonic. These perspectives include pleasure, pain avoidance, meaning, and self-realization to function effectively (Ryan & Deci, 2000). In the organizational context, the hedonic perspective is linked to job satisfaction and commitment, whereas the eudaimonic perspective is associated with engagement and meaning (Grant et al., 2007; Thottathil & Nandakumar, 2025). Furthermore, EWB is viewed from the physical and psychological health, relationships, and work-life balance (Juchnowicz & Kinowska, 2021). Technological change may affect health, relationships, and work-life balance.
Technological change like AI has started to invade organizational operations. Thus, AI has been defined from different perspectives, such as artificial refers to the system developed by humans as natural (Bankins et al., 2024), while intelligence is the capacity to understand, learn, and adapt to change (Legg & Hutter, 2007). Thus, AI denotes the system’s capacity (Kaplan & Haenlein, 2019) that benefits organizations and society (Dwivedi et al., 2021). In the literature, positive and negative results were reported on AI implementation and EWB such as improving wellbeing and organizational processes (Mantello & Ho, 2023; Wood, 2024) and positive link exists between workload, techno stressors, behavioral stress, and work-family conflict (Molino et al., 2020). Contrary to this, AI produces negative impact on job destruction (unemployment), talent experiences, intention to leave, job engagement, satisfaction level (Agar, 2019; Canhoto & Clear, 2020; Charlwood & Guenole, 2022) careers, and EWB (Cramarenco et al., 2023; Oosthuizen, 2019).
To combat technological change like AI while considering its positive and negative impact, it is crucial to view resources as a source of competitive advantage rather than a possession through adopting an DC approach to seize and reconfigure the existing resources by adopting new technologies to safeguard EWB. Thus, the DC and RBT integration highlights a crucial insight in this study: AI implementation should not be merely treated as an upgradation of technology, but viewed as an asset used for capability-building resulting in enhancing EWB. The next section explains the conceptualization of AI-driven capabilities.
Conceptualization of AI-Driven Capabilities
To integrate systems for effective functioning, one in five organizations faces obstacles during AI implementation such as a lack of technological competence, infrastructure, and data requirements (Mikalef et al., 2019; Ransbotham et al., 2017). Furthermore, to overcome these obstacles it is crucial to derail the AI-related initiatives to review existing systems and processes (Davenport & Kalakota, 2019). This review process can help to identify the gap between existing and exploited AI-specific resources within the organization leading to formulate strategy for developing capability to integrate tangible, intangible, and human resources with new technologies. Thus, developing tech integrated complementary resources and capabilities can help in reshaping and reconfiguring the existing processes to gain competitive advantage (Sharma & Vredenburg, 1998; Teece, 2018).
This can be possible through improving interdepartmental coordination and inclusion of cross-functional teams with diverse skill sets (Fountaine et al., 2019), and having sound technical and managerial skills (Chui & Malhotra, 2018; Fountaine et al., 2019; Ransbotham et al., 2018). These all together can help in achieving organizational goals. Hence, in this study, AI-driven capabilities refer to a process for choosing AI-specific organizational resources such as tangible, human resources, and intangible ones respectively, to get maximum benefits following (Mikalef & Gupta, 2021) elaboration. Details about chosen AI-driven capabilities and EWB are specified in the next section.
Tangible AI-Driven Capability and EWB
Referring to RBT literature, tangible resources can be bought or sold (Barney, 1991) such as physical assets (e.g., equipment & facilities) as well as financial assets (e.g., debt & equity). In addition to this, resources such as technological infrastructure for the storage and transfer of data, financial flows, and power processing are needed to build AI-driven capabilities (Desouza et al., 2020; Duan et al., 2019; Wirtz et al., 2019). Furthermore, tangible AI resources aid in building organizational capability through developing safe system design along with strong ethical and accountability mechanisms. This leads to create an environment of cooperation across stakeholders to see technologies as an advantage rather than a burden (RamaDevi et al., 2024). Besides, Mikalef and Gupta (2021) categorize tangible AI-driven capabilities (hereafter, TRAIC) as the availability of technology & data and basic resources required to augment organizational creativity. This indicates AI capabilities have become a strategic aspect and cannot be ignored (Fosso Wamba et al., 2024). It is crucial to embed capabilities such as tangible, intangible, and human resources from an integrated DC and RBT lens for the reconfiguration of the organizational processes (Barney, 1991; Teece, 2018). The presence or absence of these resources can affect the EWB because of the stress associated with it (Oviatt, 2021). In this study, TRAIC involves the utilization of basic resources, technology, and data-based infrastructure for hospital management and patient dealing. However, limited empirical studies exist about TRAIC and the EWB relationship (Ahumada-Tello et al., 2023; Oosthuizen, 2019). Thus, to fill this gap, we hypothesize the following:
H1a: TRAIC is related positively to EWB.
Human Resource-Driven AI Capability and EWB
HRAIC refers to an individual’s ability to acquire knowledge and develop skills to perform at par using abilities to manage AI implementation (Fosso Wamba et al., 2024). Furthermore, AI implementation in HRM presents two main issues: (1) digitalization of HRM processes and (2) competence and skill development to remain competitive (Boehmer & Schinnenburg, 2023). Both aspects require due diligence for timely reconfiguration of resources into capabilities while technological adoption (Nankervis et al., 2021). Thus, organizations have begun to invest in upskilling and reskilling to develop technical, business, and management skills to manage AI adoption fits in the category of human resource-driven AI capability (hereafter, HRAIC) (Dwivedi et al., 2021; Spector & Ma, 2019).
Subsequently, HRAIC can aid in improving competitive advantage (Budhwar et al., 2022), employee satisfaction (Barney et al., 2001), and employee mental health and wellbeing (Dutta & Mishra, 2024). DC involves reskilling and reconfiguring talent to cope with technological shift (Teece, 2007) to position employees as “co-creators” of AI capabilities rather than “passive adopters” to gain a competitive advantage, resulting in lessening the stress and enhancing EWB (Cramarenco et al., 2023). Accordingly, HRAIC can potentially contribute to amplifying the EWB (Stone & Gupta, 2024). In this study, HRAIC involves the utilization of technical, business, and management skills among doctors for service delivery and patient management. However, limited empirical studies exist about the HRAIC and EWB relationship. Thus, we hypothesize the following:
H1b: HRAIC is related positively to EWB.
Intangible AI-Driven Capability and EWB
Intangible AI-driven capability (hereafter, ITAIC) refers to inter-department coordination within an organization to initiate technological change (Davenport & Ronanki, 2018; Ransbotham et al., 2018; Sun & Medaglia, 2019), that are hard to imitate by others (Morgan et al., 2006). According to Mikalef and Gupta (2021), ITAIC includes inter-departmental coordination to synchronize tasks by sharing a mutual vision across organizational departments for successful project execution (Kahn, 2001), digital change management (Grover et al., 1995), and risk proclivity to adopt AI effectively (Ransbotham et al., 2018). Contrary to this, ITAIC involves high information asymmetries and is viewed as a non-monetary asset with high-risk profiles (Moro-Visconti, 2024). Likewise, ITAIC can enhance organizational viability and performance using technology, change management strategies, and risk management to gain a competitive advantage (Gazi et al., 2024).
Intangible resources support a healthy transition into AI-integrated systems among employees when organizations invest in reconfiguring the process to build a digital culture and provide training (Bandeira, 2021; Edmondson & Lei, 2014; Zahoor et al., 2024), fostering EWB. Though having a positive side, the technological revolution may negatively affect the EWB if training is not provided to employees aiming towards technological adoption (Gull et al., 2023). Moreover, ITAICs can perhaps affect EWB (Amponsah-Tawiah et al., 2014; Johnson et al., 2020; Vukelić & Čizmić, 2019). In this study, ITAIC involves the utilization of interdepartmental coordination and risk proclivity among doctors for effective coordination. Yet, it is important to evaluate in what way ITAIC is related to EWB (Johnson et al., 2020). To fill this gap, we hypothesize the following:
H1c: ITAIC is related positively to EWB.
Mediating Role of Cybernetic Thinking
CT is the application of system theory, emphasizing three aspects: (1) feedback, (2) regulation, and (3) adaptive control in complex systems (Ashby, 1956; Beer, 1995). Viewing the advent of cybernetics and information theory, it was not a mechanistic attempt to elaborate the purposeful behavior of humans, machines, or animals. It seems to be a process of sending and receiving messages in a feedback mechanism on one side, but on the other side, to comprehend human and machine behavior (Johnston, 2008).
With the advent of AI, there are three approaches to be executed to facilitate and integrate CT (1) aligning the operational aspect of the human brain and intellect with the environment to streamline the thinking process to solve problems, (2) alignment of intellect activity with computer technology, so that AI and algorithms can be used in systems, (3) the cooperation between machine, people, and environment is important (Boyun, 2023). Thus, CT provides a framework to balance the AI-driven capabilities and human-centered outcomes, particularly EWB.
CT supports reworking during and after AI adoption change across different tiers through employing a feedback mechanism (Latar, 2018; Nema & Sharma, 2024) to manage AI-driven capabilities such as tangible aspects (Stokes, 2006), human resources (Kummamuru, 2012), and intangible resources (Szasz, 2016) and hence contributes to positively shaping wellbeing (Narayan, 2020; Van der Maden et al., 2023). Nonetheless, the mediating role of CT between AI capabilities and EWB is missing in the literature. Thus, CT reframes not as a tool to control but to help in co-regulating and developing mechanisms to implement AI-driven capabilities, lessening stress and improving EWB rather than compromising. Thus, we hypothesize the following:
H2a: CT mediates the TRAIC and EWB relationship.
H2b: CT mediates the HRAIC and EWB relationship.
H2c: CT mediates the INTAIC and EWB relationship.
Moderating Role of Organizational Ambidexterity
OA is a process to adapt incremental and radical technological change effectively (Chakma et al., 2021; Kassotaki, 2022). To manage such change, organizations focus on the exploitation side to increase their revenues, but are unable to manage environmental and technological change. Nevertheless, balanced exploitation and exploration approaches can support CT systems to make the process transparent and affect the employee’s outcomes (Bedford, 2015; Gschwantner, 2018). CT can also direct people’s behavior through timely communication and affect organizational and individual outcomes such as EWB and performance (Raiden et al., 2020; Salas-Vallina et al., 2022) and firm performance (Fu et al., 2015).
Linking this aspect to the healthcare setting, the execution of AI in hospitals is far behind that of other industries. However, the curricula are being followed with limited digital integration, affecting AI adoption and EWB in Pakistan (Khan et al., 2024), causing frustration. There is a dire need to shift curricula from traditional to ones integrated with digital aspects. Hence, it is necessary to introduce AI-related curricula and professional development programs to improve organizational and human resource readiness to accelerate the successful integration of AI, which positively affects EWB as a result, healthcare service delivery will be enhanced (Habib et al., 2025; Natali et al., 2025). For instance, as per McKinsey’s report, AI can optimize the healthcare setting, including hospitals by effectively utilizing human, tangible, and intangible resources (Zurkiya, 2024), to achieve social and economic goals (Nasir et al., 2023).
Many developed and developing countries have already adopted AI technologies through institutional readiness and healthcare professionals’ training (Zuhair et al., 2024). For instance, different healthcare settings have taken steps to implement AI in numerous processes in developing countries such as Aga khan University hospital and Shaukat khanum Memorial Cancer hospital and Research Centre in Pakistan, Satmed’s Floating hospitals in Bangladesh, Apollo Hospitals in India, and MedSol AI Solutions in South Africa, while in developed countries—NHS and C2-Ai in the United Kingdom, Humber River Health in Canada, and Boston Children’s Hospital in the United States. Contrary to this, if healthcare organizations and institutions do not invest in technological upskilling and institutional reforms, they will be behind regionally and globally (Gill, 2025).
The trajectory in Pakistani healthcare settings mirrors the early signs seen in Nokia’s case, entrenched success leading to complacency and ultimately vulnerability due to lagging behind technological innovation (Nyman, 2024). Contrary to this, it can affect internal stakeholders’ wellbeing on one side, and patients may seek medical services abroad due to institutional failure to adopt technological innovation. Thus, AI adoption is not just a theoretical or operational issue but a strategic necessity to remain competitive and have an impact on different tiers of a country, including economic (GDP), political (formulation of laws to manage technology) & social systems (to build relationships among stakeholders) is more established in developed countries than developing. All together can facilitate the whole process of technological integration (Nema & Sharma, 2024).
Drawing on RBT and DC theoretical lenses, ambidexterity is a valuable, rare, and hard-to-imitate organizational capability like CT and control (Armenia et al., 2023; Bugwandin & Bayat, 2023) to reconfigure the internal competencies in response to technological adoption (Barney, 1991; Teece, 2018). As a result, EWB can be enhanced without chaos (Lund, 2024; Muñoz-Pascual & Galende, 2020). However, limited studies exist in which the OA moderating role has been examined between CT and EWB. Thus, the following statement was hypothesized:
H3: OA moderates the relationship between CT and EWB.
Methodology
Approach and Sample
For the current study, exploratory research was used to examine the link between study variables. This study draws its sample from the population by focusing on doctors practicing in private sector hospitals across two major cities of Pakistan: Karachi and Islamabad. The rationale behind choosing two cities was due to the strategic importance of a well-established, technology-driven healthcare setting with socio-economically diverse patient inflow. Access to such settings in these cities can allow for a better understanding of the study variables. Furthermore, the online method was employed for data collection, which gave participants the choice to contribute and ensured respondents’ voluntary participation using purposive sampling. This sampling technique allows us to gather information from the relevant stakeholders that is, doctors as they are directly involved in AI implementation (Selamat et al., 2021).
To calculate sample size, the “G*power software” was used with f2 = 0.02, a = 0.05, and predictors = 5, and the power was 80% (Aguirre-Urreta & Rönkkö, 2015). So, the sample size required to test this model was 647. To collect the maximum number of responses, around 700 questionnaires were distributed. Only 510 were received in complete form. After an initial evaluation, 20 questionnaires had missing values. So, the final sample size was 490. The response rate is 72.8%. However, after initial scrutiny of the response received, 20 questionnaires were excluded due to missing values, thus, the response rate is 70%. However, the study falls short of 157 participants due to several practical constraints, including participants’ availability and response fatigue. Additionally, a 70% response rate is considered acceptable in survey research (Fowler, 2013) and still provides a substantial base for analysis in PLS-SEM as per the researchers’ recommendation (Gefen et al., 2011).
In order to curtail the non-response bias, a few measures were taken such as follow-up reminders and survey method administration. However, due to a busy schedule and engagements, they remain non-respondents. Furthermore, to check the non-response bias, the mean score was calculated between early and late responders (Groves et al., 2001; Sterne et al., 2002). As per the result, the overall mean is approximately 6.46 closer to the mean score of responders that is, 7. This shows the responders were more dominant than non-responders, indicating no response bias.
Moreover, the representation of respondents in the sample indicates that there were 40.8% (n = 200) females and 59.2% (n = 290) males in our sample. In addition, 22% (n = 108) of respondents fell under the category of <5 years of experience, whereas 21.2% (n = 104) in 5 to 10 years of experience, 29.2% (n = 143) in 10 to 15 years of experience and remaining 27.6% (n = 135) in >15 years of experience. Furthermore, Harman’s single factor was run to assess the variance as data was collected from single source. According to the results, a variance was <50%, confirming that no issue of common method bias was present (Fuller et al., 2016).
Measures
Before collecting data on a larger sample size, a pilot study was conducted on a sample of 150 to see the feasibility of the adapted questionnaire. To measure AI capabilities, the adapted scale contains 40 items, however, 26 items were retained after measurement model assessment with a factor loading >0.70 (Cheung et al., 2023), and the remaining were excluded because of low factor loadings. Moreover, an adapted 9-item scale was used to measure EWB and CT. Lastly, the OA (12 items) scale was adapted, while three items were excluded due to low factor loadings. Therefore, 9 items were included in the study. Details about measures, sources, and sample items are presented in Table 1, and retained items used in this study are mentioned in Appendix 1. The decision to use both 5 and 7-point Likert scales in one study was guided by the nature of the construct being measured. Prior research supports using both scales when the construct sensitivity and respondents’ interpretation vary (Altuna & Müge Arslan, 2016; Russo et al., 2021).
Measures, Sources, Sample Items.

Analysis Tool
Data was analyzed using Smart PLS to assess the link between variables along with mediated moderation effects. Accordingly, PLS-SEM is considered an effective tool in the following scenarios (i) Testing theoretical framework from a prediction stance, (ii) When a structural model has many constructs and model relationships, (iii) Lack of normality, (iv) Effectively measuring the model’s paths along with a small sample size, and (v) Exploring the established theories (Hair et al., 2019). Furthermore, this software is seen as a “silver bullet” in the management sciences field for results (Hair et al., 2011, 2022;C. Li et al., 2020) to test the measurement and structural model.
The following steps were followed for data analysis: Firstly, the data was checked for missing values. Secondly, the descriptive statistics and Harman’s single-factor test were run using Jamovi. Third, following techniques were used in PLS-SEM (1) Assessment of indicator reliability (Cronbach’s Alpha and composite reliability), (2) convergent reliability (average variance extracted), (3) discriminant validity (HTMT ratio), (4) collinearity statistics,(5) outer loadings, (6) assessment of structural model, (7) mediated moderation analysis using bootstrapping with a subsample of 5,000, and (8) predictive relevance (Q2) (Hair et al., 2011; Wehrens & Van Der Linden, 1997).
Results
Measurement Model
Table 2 indicates the factor loadings and VIF values related to each variable. Moreover, the VIF indicates no issue of multicollinearity exists as the values were <5 (Rogerson, 2001). Moreover, the R2 value of EWB increases from .709. This means a 70.9% change in EWB can be explained due to exogenous variables. It is considered as strong according to the researcher’s proposed R2 threshold value for the endogenous variable as specified: .1 (small), .25 (medium), and >.30 (strong) (Falk & Miller, 1992; Wetzels et al., 2009). In addition, the measurement model is shown in Figure 1.
Factor Loadings and VIF.

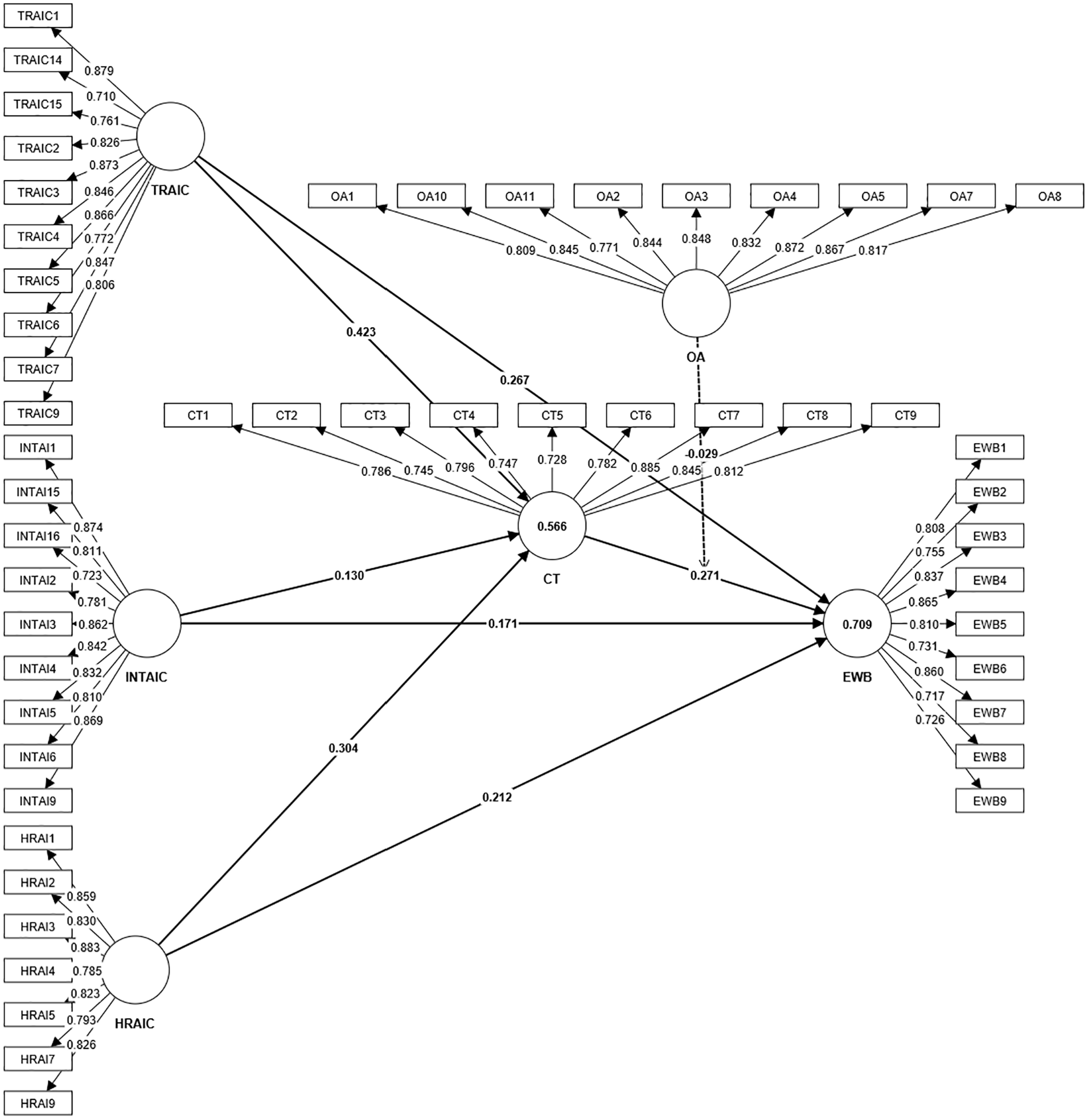
Measurement model.
Results are mentioned in Table 3 related to construct validity as well as reliability. As per the result, there is no issue of reliability as the alpha value is more than .70. This value falls within the recommended value (Hair et al., 2019). In addition, the CR value is greater than the AVE value. This designates that there is no issue of construct validity in our study. Thus, we can pursue further analysis to assess the structural model.
Construct Validity and Reliability.

Note. CA = Cronbach alpha; CR = composite reliability; AVE = average variance extracted.
Table 4 indicates the HTMT values for the assessment of discriminant validity. As per the results, no issues of discriminant validity were found as values were below 0.85 (Henseler et al., 2015, 2016).
Discriminant Validity.

Structural Model
As per the analysis of data, TRAIC, HRAI, and INTAI have a positive as well as significant link with EWB as beta values are .240 (p = .000), .230 (p = .000), and .133 (p = .000), respectively. Moreover, CT and OA also have a significant and positive link with EWB. However, OA has a negative but significant moderating role between CT and EWB as the p-value is <.05. Furthermore, an index value of OA for mediated moderation shows meaningful results (−0.015, −0.003, and −0.012). Hence, mediated moderation is supported as indicated in Table 5. Figure 2 indicates the path analysis and Figures 3 to 5 show the graphical presentation of the mediated moderation analysis.
Hypothesis Testing.

Note. U_LCI = upper limit confidence interval; LL_CI = lower limit confidence interval.

Path analysis.

Mediation moderation graphical illustration for TRAIC, CT, EWB × OA.

Mediation moderation graphical illustration for HRAIC, CT, EWB × OA.

Mediation moderation graphical illustration for INTAIC, CT, EWB × OA.
To check the predictive relevance of the finding. The Blindfolding method was used to check robustness through the Q2 value. As per the results shown in Table 6 specifies that the model has predictive relevance as the Q2 value is >0 (Hair et al., 2022).
Predictive Relevance.

Discussion and Conclusion
This study attempted to determine the link between AI-driven capabilities (TRAIC, HRAI, and INTAI) and EWB alongside CT as a mediator between TRAIC, HRAI, and INTAI and EWB, while OA as a moderator between the CT and EWB relationship among doctors working in two big cities of Pakistan: Karachi and Islamabad, using the integrated RBT and DC theoretical lens. This study found that TRAIC, HRAI, and INTAI have a significant relationship with EWB. As per the results, the TRAIC exerts a stronger impact on EWB than INTAI in private sector hospitals in Pakistan. Availability of tangible resources includes physical assets, finances, technology as well as data, and basic resources, along with technical and managerial skills, coordination, and adaptability, can help to manage change and risk proclivity for new technological ventures like AI in a private sector hospital that leads to reduce stress and enhance EWB as a result.
The reason behind the prominence of TRAIC may be directly related to reducing workload, while INTAI may take longer to impact and may not be directly felt in the workflow. Results are aligned to the studies and arguments presented in the literature by different researchers (Ahumada-Tello et al., 2023; Amponsah-Tawiah et al., 2014; Johnston, 2008; Oosthuizen, 2019; Stone & Gupta, 2024; Vukelić & Čizmić, 2019). Moreover, technological change might negatively affect the EWB (Gull et al., 2023), which is not aligned with our study results. Our study further broadens the scope of Mikalef and Gupta (2021) study in the service sector, particularly private sector hospitals.
Furthermore, CT mediates the relationship between TRAIC, INTAI, HRAI, and EWB. Using the integrated RBT and DC stance, CT enables private sector hospitals to convert AI capabilities into an adaptive system that fosters a supportive environment, leading to enhanced EWB. This means CT facilitates the effective use of AI-driven capabilities using a feedback loop to make effective decisions about diagnosis and patient care and amplifying EWB (Latar, 2018). Results are compatible with prior studies (Campbell & Ramamoorti, 2023; Gruszczak & Kaempf, 2023; Narayan, 2020; van der Maden et al., 2023).
On the adjacent side, OA moderates the relationship between CT and EWB. As per the results of this study, OA presence weakens the link between CT and EWB. This shows that CT has been shown to enhance EWB in the presence of AI-driven capabilities in private sector hospitals. However, OA may weaken this link by overburdening employees and fragmenting strategic focus. Thus, when OA is high in private hospitals may demand both exploration through continuous learning and exploitation by following strict process optimization (Sorsanen, 2009), leading to increased workload and causing the weaker positive impact of CT on EWB. However, studies specify that OA facilitates adapting incremental and radical technological change (Chakma et al., 2021; Kassotaki, 2022) with timely communication and decisions, which in turn shape wellbeing (Raiden et al., 2020; Salas-Vallina et al., 2022).
In addition, integrated RBT and DC (Barney, 2001; Teece, 2018) specify that the OA can suppress the effective utilization of CT to reconfigure the process, leading to undermining EWB in a stressful and technology-driven environment like private sector hospitals (Jia et al., 2023). In addition, combining DC with RBT offers a more comprehensive view, allowing healthcare settings to build and sustain a competitive edge not just based on improving the existing systems to continuously innovate and adopt new technologies (Agwunobi & Osborne, 2016; Chomutare et al., 2022; Joshi et al., 2024).
It is concluded that AI-driven capabilities, including TRAIC, HRAI, and INTAI, significantly relate to EWB. Furthermore, CT mediates the relationship between TRAIC, HRAI, INTAI, and EWB. When hospitals think and make decisions by keeping the people-centric approach when implementing technological changes, it can leads to reducing stress and amplifying the EWB. In addition, OA moderates the link between CT and EWB. Thus, hospitals need to incorporate the AI-driven capabilities to take full advantage of technological changes to improve the existing processes and management practices, and as a result, wellbeing and service delivery will be enhanced.
Theoretical and Practical Implications
This study contributes to the extant literature by integrating RBT and DC with emerging perspectives on AI capabilities, EWB, CT, and OA. Besides, the study results are linked to “Goal 3—good health and well-being” and “Goal 9— industry, innovation, and infrastructure” (UN, 2024). Hence, several contributions emerge from this study. Firstly, in this study, The integration of RBT and DC (Barney, 1991; Teece, 2007) reveals that AI capabilities, when embedded within the dynamic processes, enhance private sector hospitals’ competitiveness and affect EWB and a driver of human-centric strategic value when configured to adapt, renew, and reconfigure to foster machine and human interaction positively to meet the patients’ needs, quicker diagnosis and reduced administrative load effectively in private sector hospitals.
Secondly, CT as a mediating mechanism between AI capabilities and EWB offers a novel contribution. Drawing on the RBT and DC integrated perspective shows that the benefits of AI capabilities on EWB are not direct but channeled through an organizational capacity for feedback processing and control mechanisms. This positions CT as a cognitive enabling process that links technology adoption to produce positive outcomes such as enhanced EWB in private sector hospitals.
Third, the moderating role of OA between CT and EWB challenges the prevailing assumptions in the RBT and DC literature. Ambidexterity is traditionally linked to performance benefits. However, this study suggests that a negative moderation effect shows that a high level of exploration and exploitation balance may inadvertently lessen the positive impact of CT on EWB. This paradox reveals tension inherent in the simultaneous pursuit of innovation and efficiency and adds nuance to understanding organizational design. Due to organizational norms in private sector hospitals that often focus on stability or control over flexibility, excessive pressure to innovate while maintaining existing operations could overwhelm employees, leading to stress and burnout. Our study adds a new perspective to RBT’s stance. Recent AI developments are seen as a competitive driver in the healthcare setup (Kasula, 2024).
This study provides practical implications for practitioners working in healthcare settings in Pakistan as they embark on the digital transformation journey. Healthcare organizations may assess their strengths and weaknesses regarding AI technologies by identifying the resources required for infrastructure development. The digital transformation journey should be viewed as an enabler among developed and developing countries rather than solely focusing on automation through AI, CT, and EWB, leading to produce economic impact such as enhanced GDP and productivity, social impact such as service delivery and system thinking to design policies, political aspects such as crisis management and real time policy adaptation. While AI and CT can lessen the cognitive load, automation of repetitive tasks and promote a smarter work environment. Healthcare practitioners should implement AI technologies by developing capabilities to foster learning and a feedback mechanism to create a healthy work environment.
On the other side, CT is not yet a norm; to support EWB, training programs should be introduced to help doctors embrace a feedback mechanism that can help to navigate through digital technological adoption, reduce uncertainty, and improve EWB. Moreover, healthcare managers need to broaden their competencies from a basic understanding to an advanced level related to software, programming & algorithms, and analytical techniques, from patient to hospital and employee management. Besides, technical and statistical skills need to be developed among managers and employees to manage the dataset.
Healthcare organizations must be cautious about pushing for ambidexterity that can affect EWB negatively. Therefore, healthcare practitioners need to develop a tailored approach focusing on innovation at a manageable pace and ensuring that doctors are not overwhelmed by competing demands. Leadership should focus on creating an inclusive environment where doctors feel supported in their digital transformation journey.
Limitations and Directions for Future Researchers
The limitation of our study includes the following: the first dataset of this study was comprised of doctors only. So, future studies may examine the proposed model among other healthcare professionals and sectors. In addition, this study focused on two major cities of Pakistan, which limits its validity. Future researchers may examine this framework across various cities and other regions to improve the generalizability of the study. Furthermore, the relationship between AI-driven capabilities and EWB was examined. Future studies may evaluate the relationship between AI-driven capabilities and other wellbeing dimensions including community and environmental wellbeing. The findings of this study, especially regarding the negative moderation effect of organizational ambidexterity. Future researchers could delve deeper by using sector-specific dynamics such as environmental dynamism and organizational agility to examine the effects.
Moreover, future researchers may examine the AI and well-being relationship with other moderating and mediating variables in other service sectors like education, banks, and public administration. Moreover, Harman’s single-factor test was used to assess common method bias. Future researchers may use more robust techniques like marker variables or common latent factor methods for assessment. Lastly, future researchers may examine the framework using mixed methods to further broaden the scope of AI and EWB research.
Footnotes
Appendix 1
Scales

| Variables items |
|---|
| Cybernetic thinking |
| CT1 [My technical decisions influence the system in hospitals]. |
| CT2 [I like to help my colleagues, even if it is not linked to my work directly]. |
| CT3 [I feel comfortable working in a hospital with a flexible/changing system]. |
| CT4 [I can make technical decisions in a hospital with partial information]. |
| CT5 [I always make a backup plan when things don’t go as planned]. |
| CT6 [I like taking on leadership roles during stressful situations]. |
| CT7 [I can create a common vocabulary to facilitate communication with colleagues from other disciplines]. |
| CT8 [I feel happy while giving tasks to others]. |
| CT9 [I can resolve minor issues at work in person rather than over email]. |
| Employee wellbeing |
| EWB1 [A friendly environment exists in my hospital]. |
| EWB2 [Relationship with my supervisor is good]. |
| EWB3 [My supervisor respects me rather than treats me like a subordinate]. |
| EWB5 [My health is appropriate for the work I perform]. |
| EWB6 [I always feel optimistic about the future with hope]. |
| EWB7 [My hospital environment gives me satisfaction]. |
| EWB8 [I do my best every day at a hospital]. |
| EWB9 [In my hospital good work and personal life balance exist]. |
| Organizational ambidexterity |
| OA1 [Hospital management always looks for novel technological designs]. |
| OA2 [Hospital management built on its ability to sightsee new technologies]. |
| OA3 [Hospital management focuses on creating innovative products and services to manage patients]. |
| OA4 [To satisfy patients’ needs, hospital management always finds new ways to manage creatively]. |
| OA5 [Hospital management looks for new ventures in the market]. |
| OA6 [Hospital management actively targets new patient groups for their health management]. |
| OA7 [Hospital management shows commitment to improving quality]. |
| OA8 [Hospital management displays a commitment to lower cost]. |
| OA9 [Hospital management focuses on improving its products and services continuously]. |
| OA10 [Hospital management focuses on increasing automation in hospital operations and processes]. |
| OA11 [Hospital management constantly surveys existing patients to assess their satisfaction]. |
| Intangible resources AI capabilities |
| INTAI1 [Hospital management allows for collaboration among different departments in a hospital]. |
| INTAI2 [Departments effectively work on collective goals]. |
| INTAI3 [Leaders’ emphasis on teamwork]. |
| INTAI4 [All hospital departments work on the same vision]. |
| INTAI5 [Employees and hospital management have a greater level of mutual understanding]. |
| INTAI6 [All information is shared with each stakeholder within the hospital]. |
| INTAI9 [Hospital management considers the dimensions and aspects of the reengineering efforts]. |
| INTAI15 [In our hospital management takes courageous steps to accomplish objectives]. |
| INTAI16 [Hospital management typically adopts a courageous stance by exploiting possible opportunities]. |
| Tangible resources AI capabilities |
| TRAIC1 [I can access large and unstructured data for investigation]. |
| TRAIC2 [I can integrate data from multiple internal sources into data in a central database for easy access]. |
| TRAIC3 [I can integrate data from external to internal sources to facilitate high-value assessment in our hospital]. |
| TRAIC4 [I can share data across hospital departments]. |
| TRAIC5 [I can prepare and evaluate AI data efficiently for errors]. |
| TRAIC6 [I can obtain data to produce meaningful insights]. |
| TRAIC7 [Hospital management has adopted cloud-based services for processing AI data and machine learning to streamline procedures]. |
| TRAIC9 [Hospital management has invested in networking infrastructure to support the application’s efficiency]. |
| TRAIC14 [The hospital has enough team members to get the work done using AI-based tools and projects]. |
| TRAIC15 [The hospital has given team members enough time to complete AI-based projects]. |
| Human resources AI capabilities |
| HRAI1 [In hospital we have an internal and external talent pool with the technical skills to support AI]. |
| HRAI2 [I can use AI technologies such as machine learning, natural language processing, and deep learning effectively]. |
| HRAI3 [I possess the right skills to complete jobs]. |
| HRAI5 [We are provided with the required training to deal with AI applications]. |
| HRAI7 [I have appropriate experience to justify job requirements]. |
| HRAI9 [Hospital managers can work with stakeholders and data scientists to grasp opportunities that AI might bring]. |
| HRAI12 [Hospital management demonstrates ownership and commitment to AI initiatives]. |
Acknowledgements
This work was supported by a postdoctoral fellowship from the Universiti Malaysia Kelantan, Kelantan, Malaysia.
Ethical Considerations
Not applicable as we declare that we have no human data or tissues. Principles of informed consent, confidentiality, and academic integrity were strictly adhered to. The Faculty of Management Sciences, Bahria University, Pakistan, granted ethical clearance: Letter number BUKC/DMS/2024 (112).
Author Contributions
Munaza Bibi: original draft, investigation, formal analysis, conceptualization, validation, methodology. Tse Guan Tan: review & editing, original draft, supervision. Heng Yao: analysis, review & editing.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data will be available on request.