
Abstract
Nurses often face ethically challenging situations that can trigger moral distress and compromise their well-being. Understanding how ethical climate, moral courage, and moral resilience interact is essential for promoting ethical practice and supporting nurses’ psychological and professional integrity. This study examined the relationships among ethical climate, moral distress, moral courage, and moral resilience, and assessed the moderating role of moral resilience. A descriptive-correlational design was employed with a convenience sample of 350 nurses from a university-affiliated Egyptian hospital. Participants completed validated scales assessing ethical climate, moral distress, moral courage, and moral resilience. Data were analyzed using descriptive statistics, Pearson correlation, multiple regression, and moderation analysis. Nurses reported high levels of perceived ethical climate, moral courage, and moral resilience, alongside moderate moral distress. Ethical climate was negatively associated with moral distress (β = −.30, p < .001) and positively associated with both moral courage (β = .36, p < .001) and moral resilience (β = .39, p < .001). Moral resilience moderated the relationships between ethical climate and moral distress (indirect effect = 0.16, p < .001) and moral courage (indirect effect = 0.19, p < .001), buffering distress and amplifying courage. A supportive ethical climate and enhanced moral resilience contribute significantly to reducing moral distress and fostering moral courage among nurses. These findings underscore the importance of resilience-building initiatives, ethical leadership, and targeted policy reforms in healthcare institutions. Nursing education should integrate moral resilience and ethical competence to strengthen professional practice.
Introduction
In today’s increasingly complex healthcare landscape, nurses regularly encounter ethical challenges that test their professional values, moral judgment, and personal beliefs (Abou Hashish, 2017; Abou Hashish et al., 2024; Rajhi et al., 2024). These challenges are intensified in high-stakes, resource-limited environments such as intensive care units, where nurses must make ethically significant decisions under time pressure and institutional constraints (Bruun et al., 2022). Nurses often work in hierarchical systems with limited autonomy, unclear ethical policies, and inconsistent managerial support conditions that compound ethical tensions and complicate care delivery (Abou Hashish, 2017; Abou Hashish et al., 2024).
Despite the global recognition of ethics as a cornerstone of nursing, the ethical challenges faced by nurses in Middle Eastern and North African contexts remain underexplored. Nurses in these regions, including Egypt, frequently operate under cultural, structural, and resource-based constraints that can compromise their ability to act ethically (Abou Hashish, 2017; Abou Hashish et al., 2024). Various factors could influence nurses’ moral judgment and ethical decision-making. These include individual and professional variables, such as ethical climate, moral courage, moral resilience, and moral distress, as well as demographic factors like age, marital status, experience, clinical knowledge, autonomy, and ethical orientation (Abou Hashish, 2017; Haahr et al., 2020). The current study addresses this gap by investigating how ethical climate, moral courage, moral resilience, and moral distress variables interact to shape nurses’ ethical behavior and psychological outcomes in a large Egyptian teaching hospital.
These four variables represent both systemic and individual dimensions of ethical nursing practice. Ethical climate refers to the shared perceptions of organizational values, norms, and support for ethical behavior and is strongly associated with ethical decision-making and moral outcomes (Zhang et al., 2021). A positive ethical climate aligns institutional values with professional nursing standards, reducing role conflict and enabling open ethical discourse (Abou Hashish & Awad, 2019; Kim et al., 2023). In contrast, an unsupportive ethical climate may exacerbate moral distress, which arises when nurses are constrained from acting according to their moral beliefs, leading to psychological conflict, burnout, and withdrawal (Aljabery et al., 2024; Sekerka & Bagozzi, 2007). Left unaddressed, moral distress erodes psychological well-being, leading to burnout, job dissatisfaction, and turnover among nurses (Maunder et al., 2023; Yin et al., 2024).
At the individual level, moral courage enables nurses to advocate for ethical action, even in the face of institutional resistance or personal risk. It is linked to patient advocacy, professional accountability, and a reduction in moral distress (Khatiban et al., 2021; Talebian et al., 2022). Research indicates that moral courage is positively associated with ethical decision-making and inversely related to moral distress, empowering nurses to act in alignment with their ethical beliefs despite adverse circumstances (Khatiban et al., 2021; Luo et al., 2023). Meanwhile, moral resilience, which reflects the ability to maintain or restore integrity in morally adverse situations, has emerged as a protective factor that enables nurses to adapt and recover without compromising ethical standards (Rushton et al., 2022; Yi et al., 2024). By developing moral resilience, nurses can address the psychological toll of moral distress, thereby improving their well-being and commitment to ethical practice. Moreover, fostering moral resilience aligns with broader institutional goals of promoting a supportive ethical climate and empowering nurses to maintain professional and ethical accountability (Abou Hashish, 2017; Abou Hashish et al., 2024; Yi et al., 2024).
While these constructs have been individually studied, few have been examined in an integrated framework that explains how they function together in ethical nursing environments (Rushton et al., 2022; Talebian et al., 2022). To address this gap, the current study draws on two complementary theoretical perspectives. First, Virtue Ethics provides an ethical foundation grounded in moral character and practical wisdom, highlighting virtues such as integrity, compassion, and courage as essential to ethical nursing practice (Lachman, 2016; Scott, 2024). Second, Conservation of Resources (COR) Theory explains how nurses strive to acquire, protect, and replenish personal and professional resources—such as moral resilience to manage stress and adversity (Hobfoll, 1989; Kim et al., 2023).
By integrating these ethical and psychological frameworks, the study positions moral resilience as both a personal virtue and a psychological resource that might moderate the effect of ethical climate on moral distress and moral courage. This dual approach offers a more comprehensive understanding of how organizational and individual factors interact to support nurses’ ethical decision-making and emotional well-being.
Given the significant impact of these variables on nursing practice, this study examines the relationships among ethical climate, moral distress, moral courage, and moral resilience within the nursing context. Understanding these dynamics can help healthcare institutions implement strategies to foster a supportive ethical climate, build moral courage, and strengthen moral resilience, ultimately enhancing patient care and promoting the well-being of the nursing workforce.
Theoretical Background and Conceptual Framework
This study is guided by a conceptual framework that integrates both ethical and psychological theories to explain how nurses navigate moral challenges in clinical settings. Specifically, the framework draws upon virtue ethics to provide a moral foundation grounded in character and ethical practice and the conservation of resources (COR) theory to explain the psychological mechanisms through which nurses manage moral adversity. Together, these theories support the study’s investigation into how ethical climate, moral distress, moral courage, and moral resilience interact to influence nurses’ ethical functioning and well-being.
Virtue Ethics as a Moral Foundation for Nursing
Virtue ethics, rooted in the work of Aristotle, emphasizes the role of moral character and the cultivation of virtues as the basis of ethical action. Unlike deontological ethics, which is rule-based, or utilitarianism, which is outcome-focused, virtue ethics centers on the moral agent and asks not “What should I do?” but “What kind of person should I be?” (Lachman, 2016; Scott, 2024). This theory holds that virtues—such as courage, compassion, integrity, and honesty—are cultivated through repeated ethical practice, reflection, and moral commitment (Crossan et al., 2013).
This perspective is highly relevant to nursing, a profession grounded in care, empathy, and relational ethics. Nurses make moral decisions daily, often in ambiguous or high-pressure environments, and must rely not only on protocols but also on deeply held values and ethical judgment (Abou Hashish, 2017). In this context, moral courage can be viewed as the habitual capacity to act ethically despite institutional constraints, while moral resilience reflects the strength to preserve or restore integrity in morally adverse situations (Rushton et al., 2022; Sekerka & Bagozzi, 2007).
A supportive ethical climate, from a virtue ethics standpoint, serves as a fertile environment that enables the enactment of moral virtues. For instance, a caring ethical climate encourages compassion and collaboration, while an independent climate supports autonomy and moral agency (Abou Hashish et al., 2024; Victor & Cullen, 1988). Conversely, climates that emphasize hierarchy or instrumental goals may hinder virtue development, thereby increasing the likelihood of moral distress (Abou Hashish, 2017; Abou Hashish et al., 2024).
Conservation of Resources Theory: A Psychological Perspective
To complement this moral foundation, the study incorporates the COR Theory developed by Hobfoll (1989), which posits that individuals strive to acquire, retain, and protect valuable resources—material, social, and psychological. Stress occurs when these resources are threatened, lost, or insufficient to meet situational demands. Conversely, individuals with strong internal resources such as confidence, self-efficacy, or resilience are better equipped to handle adversity.
In the nursing context, moral resilience functions as a psychological resource that helps nurses recover from or adapt to morally distressing situations. Nurses who experience a supportive ethical climate are likely to gain external resources such as professional support, ethical guidance, and peer collaboration. Those with higher moral resilience are better able to maintain psychological equilibrium and act with integrity, even in ethically complex or unsupportive environments (Kim et al., 2023; Yi et al., 2024).
Importantly, COR theory also helps explain why some nurses experience moral distress in the same environment where others thrive. It highlights the role of individual differences in resource capacity, such as resilience, in moderating the impact of environmental stressors including ethical climate. Thus, moral resilience is conceptualized in this study not only as a virtue but also as a key moderating variable that shapes how ethical climate influences moral distress and moral courage (Maunder et al., 2023). By integrating Virtue Ethics and COR Theory, this study provides a comprehensive understanding of both the moral and psychological processes underpinning nurses’ responses to ethical challenges. Virtue ethics grounds the inquiry in the importance of cultivating moral traits essential to ethical practice, while COR theory explains how these traits function as internal resources that protect against stress and promote ethical engagement (Crossan et al., 2013; Hobfoll, 1989).
Conceptual Framework
This study is guided by the conceptualization of four variables—ethical climate, moral distress, moral courage, and moral resilience under a framework that underscores their interaction in shaping nurses’ ethical decision-making and their ability to provide quality patient care (Kim et al., 2023; Rushton et al., 2022). Understanding the relationship among these variables is essential for informing organizational strategies that foster ethical climates, build resilience, and support nurses in delivering morally grounded patient care.
Ethical Climate
Ethical climate refers to the shared perceptions within an organization about what constitutes ethically appropriate behavior and how ethical issues are managed (Victor & Cullen, 1988). It shapes decision-making and influences how ethical challenges are addressed. Victor and Cullen (1988) identified five types of ethical climate: instrumental, caring, independence, professional (law and code), and rules. An instrumental climate prioritizes organizational interests or personal benefits, often disregarding the needs of others. A caring climate fosters organizational practices that emphasize compassion and empathy, encouraging ethical behavior (Victor & Cullen, 1988). An independence climate empowers employees to rely on personal moral convictions and judgment, reducing conflicts between institutional expectations and individual values (Chae et al., 2016). A professional climate supports decision-making grounded in external frameworks such as laws or professional codes of conduct. Finally, a rules-oriented climate ensures decisions are guided by internal policies or codes of conduct, providing clear ethical guidelines and promoting consistency and accountability (Lachman, 2016; Talebian et al., 2022).
Collectively, these types offer a comprehensive view of the ethical climate’s role in supporting nurses’ moral resilience and professional satisfaction. A strong ethical climate is linked to reduced moral distress and improved well-being (Abou Hashish, 2017; Abou Hashish et al., 2024). By fostering a supportive ethical climate, healthcare organizations can empower nurses to navigate ethical challenges more effectively, contributing to both professional satisfaction and high-quality patient care.
Moral Distress
Moral distress is defined as the psychological discomfort or anguish that arises when an individual knows the ethically appropriate action to take but is unable to act upon it due to various external constraints (Morley et al., 2019). In nursing, moral distress frequently occurs when institutional barriers—such as rigid hierarchies, policy restrictions, or lack of organizational support-prevent nurses from acting in alignment with their professional and personal ethical standards. This dissonance leads to emotional strain, frustration, and a diminished sense of professional integrity (Morley et al., 2019; Talebian et al., 2022).
Chae et al. (2016) identified five dimensions for measuring moral distress. Futile care refers to situations where nurses are required to provide care they perceive as unnecessary or ineffective, resulting in frustration and a sense of ethical compromise (Rushton et al., 2022; Talebian et al., 2022). Distress in nursing practices arises when nurses cannot practice according to ethical standards due to organizational limitations, workload, or resource constraints (Scott, 2024). Institutional and contextual factors encompass broader organizational and systemic issues, such as policies or structural limitations, that prevent ethical practice (Rabhi et al., 2023). Distress in physician practices relates to conflicts in interactions with physicians, particularly when nurses feel their ethical perspectives are disregarded or overridden (Rushton et al., 2022; Talebian et al., 2022). Limitations on ethical advocacy represent restrictions on nurses’ ability to raise or advocate for ethical concerns, leading to moral distress when they cannot act in the best interest of patient welfare (Khatiban et al., 2021).
The discomfort experienced in these aspects can lead to emotional exhaustion, diminished moral integrity, and eventual disengagement from the profession (Aljabery et al., 2024; Sekerka & Bagozzi, 2007). Together, these dimensions underscore how various aspects of healthcare practice contribute to moral distress, highlighting the importance of a supportive ethical climate in mitigating these impacts (Abou Hashish, 2017; Victor & Cullen, 1988). Unlike general occupational stress, moral distress is morally grounded and stems from the tension between what one knows is right and what one is able to do within institutional limits. In contrast to the strain of moral distress, moral courage represents the capacity to act ethically despite the presence of risk or adversity (Nsiah et al., 2019; Seidlein & Kuhn, 2023).
Moral Courage
Moral courage represents the ability to uphold ethical principles and take action in defense of moral values, even when doing so involves personal or professional risk (Lachman, 2016; Sekerka & Bagozzi, 2007). It reflects a deliberate choice to uphold ethical principles in real-time ethical conflicts and enables nurses to speak up, advocate for patient rights, and challenge unethical practices despite fear, opposition, or potential consequences. As a multidimensional trait, moral courage comprises three dimensions of advocacy, integrity, and accountability. Sekerka and Bagozzi (2007) identified five core dimensions of moral courage that provide a comprehensive framework for understanding ethically driven behavior in professional settings. These dimensions include moral agency, which reflects an individual’s willingness and preparedness to engage in moral behavior; multiple values, which assesses the capacity to integrate both personal and professional values in ethical decision-making; endurance of threats, which evaluates the ability to recognize and uphold moral principles despite external risks or pressures; going beyond compliance, which captures the tendency to act ethically even when not mandated by rules or regulations; and moral goal setting, which reflects the individual’s aspiration to pursue actions that embody and advance moral ideals. These dimensions collectively illustrate how moral courage operates as a multidimensional construct essential to ethical nursing practice (Sekerka & Bagozzi, 2007).
Nurses with high moral courage are more likely to act in alignment with their ethical beliefs, thereby enhancing the ethical climate of healthcare settings (Luo et al., 2023). Research demonstrated that nurses who exhibit moral courage are more likely to advocate for patient rights, challenge unethical practices, and uphold professional integrity, particularly in environments where ethical norms are inconsistent or contested (Khoshmehr et al., 2020). Previous research has shown that caring and autonomy-supportive climates are associated with greater ethical awareness, professional satisfaction, and moral engagement among nurses, whereas climates dominated by hierarchy or instrumentalism may restrict moral agency and elevate emotional strain (Almutairi, 2015; Kim et al., 2023).
Moral Resilience
Complementing moral courage is the construct of moral resilience, which is defined as the continued commitment to moral behavior in the face of, perhaps, failures in past attempts to act according to a person’s moral values or in situations where past attempts have not resulted in successful moral outcomes (Morley et al., 2019). It also refers to the ability to maintain or restore ethical integrity when confronted with moral adversity, value conflicts, or ethically compromising situations (Lachman, 2016; Rushton et al., 2022). It is more reflective in nature, enabling individuals to recover, learn, and grow from ethical setbacks or morally injurious experiences, thereby preparing them to engage ethically in future challenges.
Moral resilience allows individuals to recover from moral challenges without losing their commitment to ethical values. Several interrelated dimensions shape and express moral resilience, including the response to moral adversity, personal integrity, relational integrity, and moral efficacy. While personal integrity and moral efficacy are commonly described as core components of moral resilience (Heinze et al., 2021; Rushton et al., 2022), they may also act as enabling capacities that support its development. In this way, resilience is both a reflection of and dependent upon the presence of these foundational moral strengths (Lachman, 2016; Yi et al., 2024).
Moral adversity refers to ethically challenging situations in which individuals face value conflicts, ambiguous ethical responsibilities, or morally compromising conditions that threaten their ability to act in alignment with their core moral beliefs (Talebian et al., 2022). Unlike moral distress, which involves emotional conflict when action is constrained, moral adversity encompasses the broader context of exposure to difficult ethical environments—such as inadequate resources, conflicting duties, or systemic injustices—regardless of whether distress is felt or action is blocked. It is considered the precursor condition from which responses like distress, courage, or resilience may emerge depending on individual and situational factors (Lachman, 2016; Rushton et al., 2022).
Response to moral adversity reflects the ability to cope with and respond constructively to ethical challenges without compromising personal values. Personal Integrity encompasses a nurse’s commitment to personal ethical standards, forming the foundation of resilience in morally complex scenarios. Relational Integrity, involves maintaining ethical relationships and respecting the dignity and perspectives of colleagues, even when faced with disagreements. Moral Efficacy refers to the nurse’s confidence in their ability to navigate ethical challenges effectively, enhancing resilience and reducing the impact of moral distress. Research indicated that fostering moral resilience enables nurses to mitigate the effects of moral distress and reduce the risk of burnout and turnover (Lachman, 2016; Rushton et al., 2022). Furthermore, cultivating moral resilience enables nurses to adapt to ethical challenges, enhancing their psychological well-being and commitment to ethical practice (Abou Hashish, 2017; Yi et al., 2024).
Moral sensitivity is widely recognized as a foundational antecedent to both moral courage and moral distress. It refers to the nurse’s ability to recognize moral issues, interpret ethical situations, and perceive how actions affect others (Luo et al., 2023; Lützén et al., 1995). Without this awareness, individuals may not experience distress in morally problematic situations or may not engage in morally courageous behavior. Thus, the activation of moral distress or courage is contingent on one’s capacity to identify ethical tensions. Integrating this perspective enriches the conceptual understanding of nurses’ ethical behavior by recognizing moral sensitivity as the lens through which ethical challenges are perceived and processed (Campbell et al., 2018; Talebian et al., 2022).
Likewise, moral integrity and moral efficacy are best understood as antecedents of moral resilience rather than its outcomes. Moral integrity—defined as consistency between moral values and ethical action—provides a foundational ethical compass, while moral efficacy reflects an individual’s belief in their capacity to act in morally appropriate ways despite challenges. Drawing from Virtue Ethics and COR theory, these traits serve as essential internal resources that enhance the development of moral resilience. Thus, moral resilience emerges as a dynamic capacity that is strengthened by nurses’ ethical grounding and their confidence in navigating ethically complex situations, rather than generating those traits itself (Ne’eman-Haviv et al., 2025).
To explain why moral resilience might moderate the relationship between ethical climate and moral courage, the present study draws on the COR Theory. According to COR theory, individuals strive to acquire, preserve, and protect valued resources—both external (e.g., institutional support, ethical culture) and internal (e.g., confidence, integrity, efficacy). In ethically challenging work environments, such as those faced by nurses, both types of resources are constantly taxed. When external resources (such as a supportive ethical climate) are present, they can enhance a nurse’s readiness to engage in ethical action. However, the mere presence of an ethical climate does not automatically result in ethical behavior. Nurses must also have internal resources that enable them to act on the values promoted by their environment (Crossan et al., 2013; Hobfoll, 1989).
Moral resilience functions as one such internal resource. It reflects a nurse’s psychological capacity to regulate emotions, remain grounded in personal integrity, and adapt ethically under pressure (Lachman, 2016; Rushton et al., 2022). Within this framework, moral resilience enhances the translational process between perception of a positive ethical climate and the decision to act with moral courage. In other words, moral resilience provides the internal strength and coherence needed to transform ethical norms into courageous action—especially when institutional risk, fear of retaliation, or moral ambiguity may otherwise discourage ethical behavior.
From an organizational perspective, this moderating effect is also rooted in resource complementarity. Even in a supportive climate, a nurse lacking resilience may hesitate to speak up or challenge authority. Conversely, resilient individuals are more likely to engage in courageous behavior even when the ethical climate is moderately or inconsistently supportive, making moral resilience a key moderator in this pathway (Hobfoll, 1989; Kim et al., 2023). Thus, the integration of COR theory into this model helps clarify why moral resilience is not merely an outcome but an enabling psychological resource that strengthens the impact of ethical climate on morally courageous behavior.
Therefore, these four constructs are interconnected in meaningful ways. A supportive ethical climate lays the groundwork for ethical behavior by promoting open dialogue and value alignment. In such climates, nurses are more likely to experience lower levels of moral distress and higher levels of moral courage. However, when ethical climates are neutral or adverse, the presence of moral resilience becomes crucial. Moral resilience may serve as a moderating force, protecting nurses from the negative emotional impact of ethical adversity and enabling them to recover their integrity and continue ethical engagement. This integrated framework provides a foundation for understanding how individual and organizational variables interact to support ethical nursing practice and mitigate the risks of burnout, disengagement, and compromised patient care (Rushton et al., 2022).
This conceptual framework lays the foundation for the study’s hypotheses, which examine the direct effects of ethical climate on moral outcomes and the moderating role of moral resilience
Hypotheses
Previous studies have shown that a supportive ethical climate fosters open communication, professional autonomy, and alignment between organizational and personal ethical values, reducing moral distress and enhancing job satisfaction. This conclusion is supported by the findings of Abou Hashish (2017) and Victor and Cullen (1988), who emphasized that a robust ethical climate provides a foundation for ethical decision-making and promotes a sense of integrity among healthcare professionals. Conversely, unsupportive ethical climates have been linked to increased moral distress, compromised patient care, and reduced nurse retention, as demonstrated by Kim et al. (2023).
Grounded in the preceding theoretical framework, this study investigates the relationships among ethical climate, moral distress, moral courage, and moral resilience among nurses. Ethical climate is conceptualized as nurses’ perception of how ethical behavior is supported, guided, and reinforced in their immediate work environment, regardless of specific climate type. It reflects the extent to which an organization provides a morally coherent and psychologically safe environment that allows ethical decision-making and ethical voice to flourish (Abou Hashish, 2017; Victor & Cullen, 1988).
This conceptualization draws on Virtue Ethics, which posits that moral virtues are best enacted in environments that promote ethical integrity, and on Conservation of Resources Theory (Hobfoll, 1989), which explains how individuals rely on personal and external resources to protect against stress and maintain psychological equilibrium. In this context, moral resilience is theorized to serve as a critical internal resource that enables nurses to recover from morally challenging situations and maintain ethical engagement, particularly when external conditions are ambiguous or strained (Crossan et al., 2013; Hobfoll, 1989).
When nurses perceive a strong ethical climate, they are more likely to experience value alignment, reduced moral adversity, and fewer ethical dilemmas that challenge their integrity. Such environments can mitigate moral distress and support morally courageous behavior. Nonetheless, nurses’ capacity to derive advantages from a favorable ethical climate is contingent upon their individual resilience. Those with higher moral resilience may be more likely to convert ethical support into action (moral courage) and better equipped to withstand ethical strain (moral distress) in less supportive settings. Thus, moral resilience is proposed to moderate these relationships, enhancing positive outcomes and buffering negative ones (Hobfoll, 1989; Rushton et al., 2022).
Based on this reasoning, the following hypotheses are proposed (Figure 1).
Nurses who perceive their work environment as ethically supportive are more likely to maintain or recover moral integrity in response to ethical challenges.
A perception of a supportive ethical climate is expected to be associated with lower levels of psychological discomfort when nurses are unable to act according to their moral beliefs.
Moral resilience may buffer the emotional and psychological impact of a weak or ambiguous ethical climate, reducing moral distress among nurses.
Moral resilience may strengthen the influence of ethical climate on moral courage by enabling nurses to take ethical action, even when organizational support is inconsistent.

Proposed study framework.
Significance of the Study
In the increasingly complex and ethically demanding landscape of healthcare, nurses frequently encounter situations that require not only ethical awareness but also the capacity to act in alignment with professional standards (Abou Hashish, 2017; Abou Hashish et al., 2024; Zhang et al., 2021). The interaction between organizational conditions and individual ethical capacities plays a central role in shaping how nurses experience and respond to these challenges. Four constructs—ethical climate, moral distress, moral courage, and moral resilience—are foundational to understanding ethical behavior and well-being in nursing practice (Aljabery et al., 2024; Sekerka & Bagozzi, 2007).
Ethical climate, moral distress, moral courage, and moral resilience have each been widely studied as individual constructs in nursing research. Prior work has extensively documented the negative consequences of moral distress, including emotional exhaustion, ethical dissonance, burnout, and intent to leave the profession (Aljabery et al., 2024; Dzeng & Curtis, 2018). These effects are often intensified in environments where organizational norms constrain nurses’ ability to act according to their ethical beliefs. As a result, numerous studies have recommended addressing institutional barriers—such as rigid hierarchies, policy conflicts, and lack of ethical support—to reduce moral distress and support ethical decision-making (Kim et al., 2023).
At the same time, moral resilience has emerged as a promising construct that enables nurses to maintain or restore their integrity when navigating ethically adverse situations. Scholars such as Rushton et al. (2022) and Lachman (2016) have emphasized the importance of developing individual capacities for ethical recovery, emotional regulation, and professional identity preservation. Similarly, research on moral courage has highlighted its role in empowering nurses to advocate for patient welfare, challenge unethical practices, and act in line with their moral convictions even in the face of institutional resistance or personal risk (Khoshmehr et al., 2020; Sekerka & Bagozzi, 2007).
However, despite growing interest in these concepts, existing literature tends to examine them in isolation, focusing either on the predictors of moral distress or the development of individual traits such as courage or resilience. Few studies have investigated how these constructs interact together within a unified theoretical framework. Even fewer have explored the moderating role of moral resilience in shaping the effects of ethical climate on nurses’ experiences of moral distress and moral courage. Furthermore, most existing research has been conducted in Western settings, with limited application to healthcare systems in the Middle East and North Africa. This presents a critical gap particularly in countries like Egypt, where nurses often face high workloads, restricted autonomy, and limited ethical infrastructure (Abou Hashish, 2017).
By addressing these limitations, the current study contributes to the literature in several important ways. First, it responds to the need for a conceptually integrated model that examines the dynamic interplay among ethical climate, moral distress, moral courage, and moral resilience. Second, it provides theoretical justification for treating moral resilience as a moderator, drawing on virtue ethics and conservation of resources theory to explain its psychological and ethical functions. Third, the study situates this model in an underexplored regional context, offering culturally relevant insights that may not be fully captured in Western-centric frameworks.
Overall, this study’s significance lies in its potential to inform evidence-based strategies that promote ethical engagement, strengthen moral resilience, and reduce moral distress in nursing. The findings may be particularly relevant to organizational leaders and policymakers seeking to implement resilience training, enhance ethical leadership, and cultivate work environments where nurses feel empowered to act ethically. By deepening our understanding of how individual and institutional factors interact to support ethical nursing practice, this research offers actionable pathways for improving nurse well-being, patient outcomes, and organizational integrity.
Aim of the Study
The aim of this study is to explore the relationships among ethical climate, moral distress, moral courage, and moral resilience among nurses, with a particular emphasis on the moderating role of moral resilience in these relationships.
Methods
Research Design, Setting, and Sampling
A descriptive-correlational study was conducted in all inpatient medical, surgical, and critical care units at a University Hospital, adhering to the STROBE cross-sectional reporting guidelines.
The target population consisted of registered nurses employed at the selected hospital. A non-probability, eligibility-based convenience sampling approach was used to recruit participants. Nurses were eligible if they (1) held a valid nursing license, (2) had a minimum of 6 months of clinical experience, and (3) voluntarily consented to participate. The 6-month experience criterion ensured that participants had sufficient familiarity with the hospital’s ethical climate and were likely to have encountered ethically challenging situations relevant to the study’s variables. Nurses who were newly hired or serving as interns were excluded to reduce variability in clinical exposure and maintain consistency in ethical decision-making contexts.
The required sample size was calculated using the RaoSoft online sample size calculator, based on a 95% confidence level and a 5% margin of error. The calculator indicated a minimum sample size of 183 participants to ensure statistical reliability. To account for potential non-responses or incomplete surveys, 350 questionnaires were distributed. A total of 270 nurses completed the survey, yielding a response rate of 77.1%. This final sample size exceeded the minimum requirement and provided sufficient power to analyze the proposed relationships among ethical climate, moral distress, moral courage, and moral resilience.
Data Collection Instruments
Data were collected using four primary tools:
Ethical Climate Questionnaire (ECQ): The ECQ, developed by Victor and Cullen (1988), was used to measure nurses’ perceptions of the ethical climate within their organization. The ECQ consists of 26 items and assesses five dimensions: caring (7 items), law and code (4 items), rules (4 items), instrumental (7 items), and independence (4 items). Responses were rated on a 5-point Likert scale (1 = strongly disagree to 5 = strongly agree). Higher scores indicate a more supportive ethical climate.
Korean Moral Distress Scale-Revised (KMDS-R): The KMDS-R was originally developed by Hamric et al. (2012) and adapted by Chae et al. (2016) to measure moral distress by assessing both the frequency and intensity of distressing situations. The 21-item scale includes five subdomains: futile care (5 items), distress in nursing practice (5 items), institutional factors (4 items), distress in physician practices (4 items), and limitations on ethical advocacy (3 items). Each item is rated on a 5-point Likert scale for both frequency (0 = never to 4 = very frequently) and intensity (0 = none to 4 = great extent), allowing for the calculation of a combined moral distress score by multiplying frequency and intensity scores. Higher scores indicate a higher level of moral distress.
The Professional Moral Courage (PMC) Scale, developed by Sekerka and Bagozzi (2007), assesses moral courage in professional settings. The PMC Scale contains 15 items and evaluates 5 dimensions with 3 items for each: moral agency, multiple values, endurance of threats, going beyond compliance, and moral goals. Responses were rated on a 7-point Likert scale (1 = not true at all to 7 = always true). Higher scores reflect greater moral courage.
The Rushton Moral Resilience Scale (RMRS), developed and validated by Rushton et al. (2022), consists of 17 items and measures moral resilience across four dimensions: Moral Adversity (4 items), personal integrity (4 items), relational integrity (4 items), and moral efficacy (5 items). Responses were rated on a 5-point Likert scale, with higher scores indicating stronger moral resilience.
Translation, Validity, and Reliability
To ensure linguistic and contextual appropriateness, all instruments were translated into Arabic using a standardized forward-backward translation method. Bilingual experts conducted the initial translation and back-translation to confirm semantic and conceptual equivalence. This process considered the educational diversity of the nursing population, including diploma and bachelor’s degree holders.
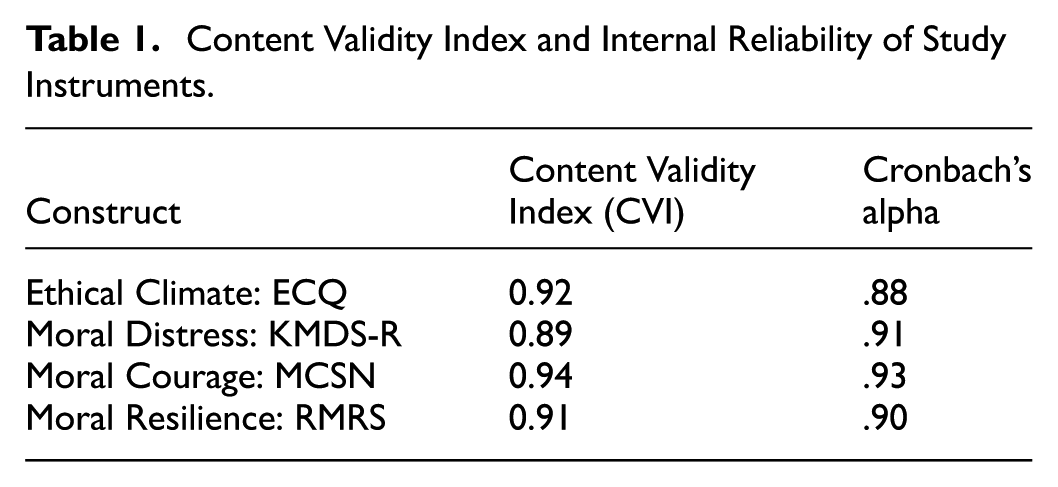
All instruments used in this study were well-established and previously validated in nursing literature. For the current sample and context, content validity was re-evaluated by a panel of three nursing experts, who assessed the instruments for clarity, relevance, and alignment with the target constructs. The resulting Content Validity Index (CVI) scores for all instruments were above 0.89, indicating strong item-level agreement among reviewers. According to Polit and Yang (2016), a CVI of 0.80 or higher is considered acceptable, with scores above 0.90 reflecting excellent content validity. Other psychometric indices such as factor structure or item-total correlations were not assessed, as the study prioritized content validation and internal consistency using established tools (Polit & Yang, 2016).
Internal consistency reliability was evaluated for each instrument using Cronbach’s alpha based on the actual study data. The results showed strong reliability coefficients across all constructs, with alpha values ranging from .88 to .93. These values exceed the minimum recommended threshold of 0.70 for acceptable internal consistency (Nunnally & Bernstein, 1994) and reflect excellent reliability for established instruments used in healthcare and nursing ethics research. Such reliability ensures that the tools consistently and accurately measured the intended constructs within the target nursing population (Polit & Yang, 2016; Table 1).
Content Validity Index and Internal Reliability of Study Instruments.
Data Collection
After obtaining approval from the hospital administration, written informed consent was secured from participants, who were briefed on the study’s purpose and their ethical rights. The researchers distributed Arabic paper-based questionnaires to nurses who consented to participate, providing detailed instructions for completion. Participants were instructed to respond based on their experiences during the previous week. To ensure data accuracy and tracking, each questionnaire was assigned a unique code. Nurses were given 1 week to complete the questionnaires, which were then collected by the researchers during scheduled visits to the units. Completed forms were often left with the unit nurse manager for retrieval. Data collection spanned 4 months, from January to May 2024.
Ethical Considerations
This study involved human participants and adhered strictly to ethical research standards. Approval was obtained from the Ethics Committee of the Faculty of Nursing, Alexandria University (IRB00013322), and the hospital’s administration. To minimize any risk of harm, the study used a descriptive, cross-sectional, questionnaire-based design with non-invasive data collection. No clinical interventions were involved, and the anonymity and confidentiality of all participants were strictly maintained. Participation was entirely voluntary, and nurses were clearly informed that they could withdraw at any time without any consequences. The potential benefits of this research, such as improving understanding of how ethical climate and moral resilience influence nurses’ well-being and ethical practice, were deemed to outweigh any minimal risks related to psychological discomfort from reflecting on ethical challenges. These risks were mitigated by framing the survey items sensitively and assuring participants of confidentiality. Written informed consent was obtained from all participants after explaining the study’s objectives, procedures, and their rights. Data were anonymized and securely stored, with access restricted to the research team.
Data Analysis
The collected data were cleaned, coded, and analyzed using IBM SPSS Statistics version 26. Initial data screening and handling of missing values ensured data integrity. Descriptive statistics (means, standard deviations, frequencies, and percentages) were computed to summarize demographic and key study variables. Internal consistency reliability for each instrument was assessed using Cronbach’s alpha coefficient.
To explore associations among the main study variables—ethical climate, moral distress, moral courage, and moral resilience-the Pearson correlation coefficient was calculated. To assess the extent to which ethical climate and moral courage were statistically associated with moral resilience, multiple regression analysis was conducted. To examine the moderating role of moral resilience in the associations between ethical climate and the two outcome variables (moral distress and moral courage), Hayes’ PROCESS macro (Model 1) was employed. Moderation was tested by evaluating interaction terms and indirect effects with 95% confidence intervals using bootstrapping procedures. All statistical tests were two-tailed, with a significance level set at p ≤ .05.
Results
Participants’ Characteristics
The majority of nurses were female (n = 343, 98.0%), with a mean age of 33.05 years (SD = 8.66). The largest age group comprised those aged 20 to less than 30 years (45.1%), followed by those aged 30 to less than 40 years (33.7%). Most participants were married (n = 233, 66.6%), and a significant proportion held a diploma in secondary technical nursing (n = 216, 61.7%), while 22.6% held a bachelor’s degree. Nearly half of the participants (49.7%) worked in intensive care units, with others distributed across medical and surgical units. The mean years of nursing experience was 13.14 (SD = 6.94), with nearly one-quarter having 20 or more years of experience. A notable majority (n = 285, 81.4%) worked rotating shifts, reflecting standard scheduling practices in hospital-based nursing. See Supplemental Table 1 for detailed demographic and professional data. These characteristics provided a diverse sample that allowed for further analysis of how such factors may be associated with ethical climate, moral distress, moral courage, and moral resilience, as examined in the subsequent analyses (see Table 4).
Descriptive Statistics for Study Variables
Table 2 highlights a moderately supportive ethical climate, with an overall mean score of 3.85 ± 0.75. Among the dimensions, the caring dimension recorded the highest mean score (4.00 ± 0.70), reflecting a strong emphasis on compassion and support. Both the rules and law and code dimensions shared the same scores (3.70 ± 0.65), indicating a balanced reliance on internal policies and external professional standards. The instrumental dimension had the lowest score (3.10 ± 0.65), suggesting a minimal focus on self-serving interests, which aligns with a positive ethical culture. These findings collectively indicate a well-rounded ethical climate, with notable strengths in fostering care and adherence to ethical guidelines.
Descriptive Statistics for Ethical and Moral Variables Among Nurses.

Note. SD = standard deviation.
Moral distress had an average score of 2.90 ± 0.80, with the highest distress reported in the futile care sub dimension (3.10 ± 0.85) and the lowest in the institutional factors sub dimension (2.60 ± 0.75). Moral courage was notably high among participants, with an overall average of 3.95 ± 0.65. The highest score was in the moral agency area (4.05 ± 0.68), followed by scores for going beyond compliance, moral goals, multiple values, and endurance of threats, showing that participants had a strong and deeply ingrained sense of moral responsibility. Lastly, moral resilience showed a mean score of 3.75 ± 0.70, with the response-to-response adversity and personal integrity sub dimensions slightly higher than others (3.85 ± 0.68; 3.80 ± 0.65), suggesting that participants were equipped to handle ethical challenges effectively. See Figure 2 for the overall mean comparisons of ethical and moral variables among nurses.

Overall mean score of ethical and moral variables among nurses.
Correlation and Regression Analysis With Moral Resilience as Moderator
Standardized regression and correlation analyses were conducted to examine the associations among ethical climate, moral distress, and moral courage, and to explore the potential moderating role of moral resilience (see Table 3 and Figure 3). Ethical climate was significantly and negatively associated with moral distress (β = −.30, p < .001) and positively associated with moral courage (β = .36, p < .001). Moral resilience was also significantly associated with lower moral distress (β = −.27, p < .001) and higher moral courage (β = .31, p < .001).
Standardized Regression and Correlation Among Ethical Climate, Moral Distress, and Moral Courage, With Moral Resilience as a Moderator.

Note. Model fit parameters: RFI = 0.92, NFI = 0.91, IFI = 0.93, CFI = 0.94 (acceptable above 0.90), RMSEA = 0.065 (good if ≤0.06). LL = lower limit; UL = upper limit; CI = confidence interval.
p Significant at ≤.05.

Standardized associations among ethical climate, moral distress, and moral courage, with moral resilience as a moderating variable.
The moderation analysis revealed that moral resilience partially moderated the relationship between ethical climate and both moral distress and moral courage. Specifically, the indirect association between ethical climate and moral distress via moral resilience was statistically significant (indirect effect = 0.16, p < .001), as was the indirect association with moral courage (indirect effect = 0.19, p < .001). While the moderation was evident in both pathways, the association between ethical climate and moral courage appeared to be more strongly conditioned by moral resilience.
Model fit indices supported the adequacy of the hypothesized model: RFI = 0.92, NFI = 0.91, IFI = 0.93, CFI = 0.94, and RMSEA = 0.065, all of which meet or exceed recommended thresholds (CFI, NFI, IFI ≥ 0.90; RMSEA ≤ 0.08), indicating a well-fitting model.
These results suggest that while moral resilience is consistently associated with both reduced distress and enhanced moral courage, it may play a more pronounced role in facilitating ethical action (moral courage) than in buffering emotional strain (moral distress). This nuanced pattern invites further reflection and is explored in greater depth in the discussion that follows.
Perceived Difference in Variables by Socio-Demographics
Table 4 demonstrates significant variations in nurses’ perceptions of ethical climate, moral distress, moral courage, and moral resilience across socio-demographic characteristics. Nurses aged 30 to less than 40 years reported the highest scores across all variables, with significant differences observed in ethical climate (p = .005), moral distress (p = .001), moral courage (p = .032), and moral resilience (p = .017). Although gender differences were minimal, male nurses reported significantly higher moral courage than female nurses (p = .045), with no significant differences in ethical climate or moral distress.
Perceived Difference in Variables by Socio-Demographics.

p Significant at ≤.05.
Married nurses showed significantly higher scores in all four variables compared to single, divorced, or widowed counterparts (p-values ranging from .001 to .007), suggesting that family support might influence ethical coping mechanisms. Educational qualification also played a role; nurses with a bachelor’s degree perceived a more supportive ethical climate (p = .029), experienced higher moral courage (p = .024), and reported greater resilience (p = .011) than diploma holders.
Work setting influenced perceptions as well. Nurses in intensive care units reported significantly higher scores in ethical climate (p = .007), moral distress (p = .003), moral courage (p = .012), and moral resilience (p = .006) compared to those in medical or surgical units. Similarly, those working rotating shifts showed higher levels across all four variables compared to nurses on fixed shifts, with statistically significant differences in ethical climate (p = .009), moral distress (p = .005), moral courage (p = .002), and moral resilience (p = .003).
Finally, years of experience were significantly associated with all outcome variables, where mid-career nurses (5 to <10 years) demonstrated the highest levels of moral courage (p = .001) and resilience (p = .004). These results highlight the importance of personal and professional characteristics in shaping nurses’ ethical behavior and adaptive capacity within challenging healthcare environments.
Discussion
Ethical challenges are an inherent part of nursing practice, and understanding the factors that influence perceptions of ethical climate, moral distress, moral courage, and moral resilience is vital for enhancing ethical decision-making and professional well-being.
Descriptive Level of Ethical Climate, Moral Courage, Moral Distress, and Moral Resilience
This study revealed that nurses perceived a moderately supportive ethical climate, with the caring climate emerging most prominently, followed by the rules-based and law and code climates. The lowest score appeared in the instrumental climate, suggesting that nurses encountered minimal emphasis on self-serving or hierarchical interests. This pattern indicates that Egyptian nurses likely operate in a system where professional collaboration and patient-centered care are prioritized over authoritarian or utilitarian values. These results may reflect institutional frameworks in Egypt that encourage ethical awareness, despite systemic constraints in staffing or infrastructure. The finding could be supported by Abou Hashish (2017), who found that Egyptian nurses perceived a moderately supportive ethical climate, particularly characterized by caring and rule-oriented values, while the instrumental climate was least emphasized. Nurses tended to align their behavior with professional norms and standards aimed at delivering quality patient care, rather than focusing on organizational self-interest.
Likewise, these findings are consistent with studies from multiple contexts. For instance, Abou Hashish and Awad (2019) in Egypt reported that participants often associate ethical climates with interpersonal respect and clear ethical guidelines. Similarly, Elliethey et al. (2024) found that positive ethical climates are rooted in professional values, moral accountability, and trust-based leadership. Kang et al. (2023) emphasized that when organizational and individual values are harmonized, moral engagement and staff retention increase. Essex et al. (2023) also concluded that ethical climates are significantly linked to job satisfaction and reduced turnover. Maffoni et al. (2020) noted that an ethical workplace enhances resilience by reducing moral conflict. These cross-cultural findings reinforce the notion that cultivating an ethical climate is globally recognized as essential for quality care and workforce well-being.
In terms of moral courage, this study found high overall levels among nurses, with the highest scores observed in the moral agency dimension, followed closely by going beyond compliance and moral goals. These findings suggest that nurses are not only ready and willing to act ethically (moral agency) but are also inclined to uphold moral standards beyond routine compliance and set ethically driven goals in their practice. The strong scores in multiple values and endurance of threats further indicate that nurses are adept at integrating both personal and professional values into decision-making and are resilient in the face of ethical risks or external pressures (Abou Hashish, 2017, 2020).
Supporting this, Atia and Abdelwahid (2023) found that Egyptian nurses who received ethical training were more likely to demonstrate moral courage. Similarly, Abou Hashish and Awad (2019) noted that institutional empowerment and a values-based culture support advocacy and ethical action. International research echoes these findings: Wang et al. (2024) linked moral courage to supervisor support and ethical leadership, while Taraz et al. (2019) confirmed that a positive ethical climate fosters moral courage. Pajakoski et al. (2021) associated moral courage with professional integrity and institutional trust. Across these contexts, these findings affirm that moral courage is shaped by both internal ethical traits and external organizational conditions, reinforcing the importance of supportive work environments and continuous ethics education in sustaining nurses’ moral performance.
Nurses in the current study also reported high levels of moral resilience, particularly in managing morally adverse situations. This resilience may be attributed to emerging educational and policy efforts in Egypt that aim to equip nurses with psychological tools to navigate adversity, especially after the COVID-19 era (Abou Hashish & Ghanem Atalla, 2023). The finding aligns with multiple studies that emphasize the importance of resilience-building initiatives, ethical awareness, and moral decision-making for both current and prospective nurses (Abou Hashish, 2017; Abou Hashish et al., 2024; Elliethey et al., 2024). Moreover, the strong presence of relational and personal integrity as indicated in the findings suggests that nurses draw strength from values rooted in cultural and religious commitments to ethical caregiving. This result supports global findings. For instance, Rushton et al. (2022) in the USA emphasized that moral resilience is vital for restoring ethical integrity under stress. In South Korea, Yi et al. (2024) showed that moral efficacy and relational integrity are essential to reducing burnout. Lachman (2016) highlighted moral resilience as a necessary ethical competency, particularly in hierarchical or resource-constrained systems paralleling conditions found in Egyptian hospitals.
Conversely, moral distress was reported to be moderate among nurses, with the highest levels associated with challenges and distress in futile care situations. This finding underscores the significant emotional and ethical strain nurses face when required to provide care they perceive as unnecessary or ineffective. The relatively lower scores in the institutional factors sub dimension suggest that systemic constraints are less significant contributors to moral distress in this context. These findings could be attributed to the inherent nature of nursing roles, particularly in inpatient care settings where ethical dilemmas are frequent and complex. This aligns with findings of Aljabery et al. (2024), who reported that nurses experience profound emotional conflict when required to continue non-beneficial treatments. Similar patterns have been observed globally. Salari et al. (2022) and Babamohamadi et al. (2021) in Iran reported that the frequency and severity of moral distress among nurses were moderate and had a detrimental impact on nurse well-being and job satisfaction. These studies identified several contributing factors, including heavy workloads, low nurse-to-patient ratios, conflicts with families’ requests, limited collaboration among care team members, and end-of-life care decision-making responsibilities.
The highest source of severity and frequency of moral distress found in our study was described as “futile care.” This agrees with Mills and Cortezzo (2020), who indicated that “futile care” against nurses’ own beliefs was a cause for moral distress. In alignment with these findings, Ganz et al. (2013) emphasized the importance of empowerment and structured support in alleviating moral distress, highlighting the need for strategies that enable nurses to manage ethical conflicts effectively. Additionally, Plouffe et al. (2023) and Hussein and Abou Hashish (2023) highlighted the critical role of organizational support in reducing moral distress, noting that workplaces with robust ethical frameworks help mitigate the emotional strain associated with ethical conflicts.
In response to these challenges, the American Association of Critical-Care Nurses (2020) has identified moral distress as a priority issue, developing the 4 A’s approach as a practical framework for addressing it. This approach includes Ask (recognize feelings of moral distress), Affirm (identify threats to moral integrity), Assess (evaluate the ethical dilemma and possible actions), and Act (create and implement an action plan). By empowering nurses to navigate ethical conflicts, this framework plays a vital role in mitigating moral distress. The findings of this study underscore the urgent need for systemic interventions to address moral distress in nursing. Key priorities include ethical education, counseling, and the strengthening of institutional frameworks to support nurses in ethically challenging situations.
Correlation and Regression Analysis Among Variables With Moral Resilience as Moderator
The current findings reveal that ethical climate was negatively associated with moral distress while being positively associated with both moral courage and moral resilience. These associative relationships support Hypotheses 1 and 2 and indicate that when nurses perceive their organizational climate to be ethically supportive emphasizing caring, fairness, and transparency, they are less likely to experience internal ethical conflict and more likely to act courageously and maintain resilience. Also, Abou Hashish et al. (2024) noted a positive correlation between ethical climate and organizational support, which play a pivotal role in fostering advocacy and courage among nurses.
This aligns with the conservation of personal resources as proposed by the COR theory (Hobfoll, 1989), which posits that environments rich in external resources such as ethical support protect individuals from stress and facilitate adaptive coping responses.
In Egypt, where nurses often face constraints related to authority structures and limited autonomy, a supportive ethical climate becomes even more crucial (Abou Hashish, 2017, 2020). Organizational policies that prioritize ethical practice, foster open communication, and value professional integrity may reduce nurses’ exposure to moral adversity. This aligns with Atia and Abdelwahid (2023), who reported that Egyptian nurses in ethically guided environments experienced less distress and demonstrated higher moral courage. Similarly, Wang et al. (2024) highlighted the role of structural and psychological empowerment in supporting nurses’ ethical performance, while Taraz et al. (2019) in Iran confirmed the positive association between ethical climate and moral courage.
Likewise, Xu et al. (2025) found that nurses perceived a moderately supportive hospital ethical climate and reported significant positive correlations among ethical climate, moral sensitivity, and ethical decision-making. Their findings emphasize the crucial role of a well-established organizational ethical environment in fostering essential moral competencies among nurses. This underscores the importance of cultivating supportive ethical climates as a means not only to enhance workplace morale but also to advance the ethical development and decision-making capacity of nursing professionals.
The literature from diverse contexts affirms these relationships. In Turkey, Salari et al. (2022) showed that ethics-oriented nurses experience lower moral distress when personal values align with institutional norms. Elliethey et al. (2024) also emphasized the importance of managerial support and professional independence in preventing ethical exhaustion, findings that resonate with data from the current study. In Italy, Ko et al. (2018) highlighted that ethically grounded organizational cultures significantly alleviate the emotional strain linked to moral distress. Rushton et al. (2022) in the USA similarly emphasized that moral clarity and shared ethical frameworks foster resilience and reduce distress.
A key contribution of this study lies in its moderation analysis, which demonstrated that moral resilience significantly moderated the relationships between ethical climate and both moral distress and moral courage. This finding supports Hypotheses 3 and 4 and reflects the essential buffering role of moral resilience as a psychological resource. Nurses with high levels of moral resilience were better able to maintain low levels of moral distress and demonstrate moral courage, even when ethical climates were less than ideal. Drawing on COR Theory, this suggests that moral resilience operates as an internal protective asset, preserving nurses’ moral integrity and enabling ethical action despite adversity.
The current results also align with emerging international research. Kovanci and Atli Özbaş (2025) found that moral resilience was inversely related to moral distress among Turkish nurses. In Philippine, Berdida and Grande (2023) reported that moral resilience was not only negatively correlated with moral distress but also positively associated with moral courage, suggesting its central role in ethical nursing practice. Shuai et al. (2024) in China further confirmed that moral resilience partially mediated the relationship between moral distress and compassion fatigue, reinforcing its emotional and ethical protective function.
In line with these insights, Babamohamadi et al. (2021) documented a strong link between resilience and moral courage, advocating for the cultivation of a moral climate that supports ethical agency and professional courage. Likewise, Wang et al. (2024) emphasized that resilient nurses exhibit stronger advocacy and are more capable of challenging unethical practices. From a virtue ethics lens, moral resilience reflects the internal cultivation of virtues such as integrity, honesty, and courage traits that empower nurses to act ethically even when institutional structures are unsupportive (Lachman, 2016; Rushton et al., 2022).
Importantly, this study revealed that moral resilience significantly moderated the relationship between ethical climate and moral courage but did not show a significant moderating effect with moral distress. This asymmetry merits deeper reflection. Drawing on COR theory (Hobfoll, 1989), moral resilience may serve more effectively as a resource-enabling ethical action (i.e., courage) rather than buffering against emotional depletion (i.e., distress). Moral courage is forward-looking and action-oriented, often emerging when individuals feel empowered to uphold their ethical values despite risk. In contrast, moral distress typically arises when nurses are unable to act due to institutional constraints or conflicting obligations (Gallagher, 2011), making it less amenable to internal buffering alone.
Additionally, Rushton et al. (2022) and Lachman (2016) have emphasized that moral resilience is critical for navigating adversity, yet its effectiveness depends on the presence of supportive ethical environments. In unsupportive or highly constrained contexts, resilience alone may not neutralize the cumulative emotional toll of unresolved ethical conflict. Furthermore, Yin et al. (2024) suggested that resilience is more closely tied to proactive coping and ethical action (such as courage) than to the passive endurance of unresolved distress. Measurement differences may also play a role, as moral distress scales often assess emotional burden, while moral courage captures behavioral intention and ethical commitment (Sekerka & Bagozzi, 2007).
This divergence reinforces the idea that moral resilience may not operate uniformly across all moral outcomes. Rather, its influence appears context-dependent, most effective when aligned with environments that allow ethical expression. Tailored interventions should therefore aim not only to foster individual resilience but also to dismantle systemic barriers that perpetuate moral distress. These findings highlight the nuanced, interactional nature of ethical functioning in clinical practice.
Perceived Difference in Variables by Socio-Demographics
The findings reveal that socio-demographic characteristics significantly influenced nurses’ perceptions of ethical climate, moral distress, moral courage, and moral resilience. These results offer critical insight into how personal and professional backgrounds shape ethical behavior and psychological coping in nursing practice.
Age was a notable factor, with younger nurses (aged 20–30) reporting lower levels of moral distress and higher levels of moral resilience compared to older cohorts. This may suggest that younger nurses might possess greater adaptability or have benefited from more recent exposure to resilience-building initiatives integrated into modern nursing education (Abou Hashish & Awad, 2019). Generational differences in coping styles and professional socialization may also contribute to these findings. This aligns with Wang et al. (2024) in China, who observed-that younger nurses often demonstrate higher adaptability when facing ethical challenges. However, findings in the literature remain varied. For instance, Hatamizadeh et al. (2019) in Iran found that older nurses experienced less moral distress due to their accumulated experience, while Wenwen et al. (2018) in China reported the opposite-that older nurses experienced greater distress. Ghasemi et al. (2019) in Iran found no significant association. These differences may reflect how organizational expectations, societal roles, and support structures vary across cultures.
Gender differences were also evident in moral courage, with male nurses scoring significantly higher than their female counterparts. This could reflect social norms within healthcare settings that attribute assertiveness and advocacy to male leadership traits. In male-dominated organizational structures, men may be perceived or encouraged to take more ethically assertive roles. Hanifi et al. (2019) in Iran found similar patterns, linking male nurses’ assertiveness with increased moral courage. Similarly, Maffoni et al. (2020) in Italy argued that workplace culture, more than biological sex, shapes perceived ethical efficacy, suggesting gendered expectations in clinical roles may affect how courage is expressed and evaluated.
Marital status was associated with significantly higher scores in ethical climate, moral courage, moral distress, and moral resilience among married nurses. This may reflect the influence of social expectations in Egyptian culture, where marital status is associated with maturity, responsibility, and emotional stability—qualities that may support ethical reflection and professional accountability. Supportive relationships at home may also buffer the emotional impact of ethically distressing situations. This interpretation is consistent with cultural frameworks in Middle Eastern contexts, where marriage is often linked to increased social respect and perceived moral responsibility. Abou Hashish et al. (2024) supported this finding, noting that individuals with robust personal support systems tend to be more resilient, engaged, and ethically aware in their professional environments.
Educational qualifications significantly influenced nurses’ perceptions of ethical variables. Nurses with a bachelor’s degree scored higher in ethical climate and moral courage compared to those with technical or secondary nursing diplomas. This finding underscores the critical role of formal education in developing nurses’ ethical reasoning and confidence in decision-making. In Egypt, baccalaureate programs include ethics as a standalone course, in addition to communication, patient advocacy, and caring courses, which together instill moral principles and empower nurses to navigate complex ethical situations. Yin et al. (2024) emphasized the positive impact of advanced nursing education on moral resilience and moral courage. Furthermore, previous literature (Abou Hashish & Awad, 2019; Abou Hashish & Ghanem Atalla, 2023) consistently recommends embedding ethical reasoning early in nursing curricula to enhance nurses’ professional identity and integrity. This suggests that diploma holders may benefit from continuous ethics education and professional development to close the ethical competency gap.
Years of experience played a nuanced role. Nurses with 5 to 10 years of experience reported the highest levels of both moral distress and moral resilience. This may reflect a developmental stage in professional practice where nurses are experienced enough to recognize ethical tensions but may not yet have developed the deeper coping mechanisms of more seasoned colleagues (Aljabery et al., 2024). Salari et al. (2022) found similar outcomes, noting that mid-career professionals face increasing responsibilities without always having corresponding institutional autonomy or support. These findings support the idea that resilience-building strategies and ethics-based mentorship may be especially valuable for this cohort.
Working units also influenced ethical perceptions. Nurses working in intensive care units (ICUs) reported significantly higher levels of moral distress and moral resilience than those in medical or surgical units. The ICU setting involves frequent end-of-life decisions, complex family dynamics, and high patient acuity—factors that can provoke ethically challenging dilemmas. Yet the same high-pressure context may foster resilience through repeated ethical engagement. Mills and Cortezzo (2020) in the USA emphasized the emotional burden of ICU nurses managing futile care and the moral conflicts that arise. Similarly, Shuai et al. (2024) confirmed that ICU nurses who face intense moral adversity often develop higher moral resilience as a protective adaptation. These findings affirm the importance of structured ethical support systems tailored to high-risk units.
In a related study, Talebian et al. (2022) reported that critical care nurses often face elevated levels of moral distress due to the demanding nature of their clinical roles. However, resilience appears to play a key role in helping these nurses adapt to the physical and emotional challenges associated with caring for critically ill patients. Their study also found a significant positive association between work experience and resilience. This result suggests that as moral distress intensifies, critical care nurses are more likely to rely on resilience as a coping mechanism to maintain their engagement and continued presence within the organization.
Work shift emerged as another significant factor influencing both moral distress and moral resilience. Nurses working rotating shifts reported higher levels of moral distress and resilience compared to those on fixed schedules. Rotating shifts—often involving night duties, irregular hours, and communication challenges may contribute to increased ethical tension and emotional fatigue. However, the adaptability required for navigating such schedules may also enhance coping mechanisms and psychological flexibility. Hatamizadeh et al. (2019) noted that frequent exposure to ethically ambiguous situations during night or understaffed shifts may simultaneously elevate moral distress and foster resilience. Similarly, Alsayed et al. (2022) highlighted the impact of occupational fatigue and extended working hours on error rates, patient safety, and care quality. In parallel, Abou Hashish and Ghanem Atalla (2023) found that compassion fatigue and emotional exhaustion are common among nurses providing continuous patient care. Collectively, these findings underscore the need for resilience-building interventions and the implementation of well-structured shift scheduling systems to support nurses’ ethical and emotional well-being (Hussein & Abou Hashish, 2023).
In sum, these findings highlight the complexity and interdependence of demographic variables in shaping nurses’ ethical and psychological experiences. Recognizing how age, gender, marital status, education, clinical setting, and shift work intersect with moral behaviors is essential for designing context-sensitive interventions. Tailored strategies such as ethical mentoring for early-career nurses, resilience programs for ICU staff, and inclusive leadership to empower all genders can help foster a workforce that is ethically grounded, psychologically resilient, and capable of high-quality care. As Taraz et al. (2019) and Abou Hashish (2017), Abou Hashish and Awad (2019), and Abou Hashish and Ghanem Atalla (2023) noted, ethics education and structured reflection play a central role in empowering nurses to act with courage, uphold professional integrity, and maintain their moral agency across diverse work environments. Likewise, Abou Hashish et al. (2025) highlights the importance of ongoing professional development, curriculum integration, and institutional support in cultivating a culturally competent and ethical nursing workforce.
Conclusion
This study examined the interrelationships among ethical climate, moral distress, moral courage, and moral resilience among nurses in an Egyptian teaching hospital. Using a cross-sectional survey design and validated instruments, data from 350 nurses revealed that a supportive ethical climate was significantly associated with lower moral distress and higher expressions of moral courage and moral resilience. Moral resilience emerged as a key moderating factor, buffering the emotional strain of ethical challenges and reinforcing ethical engagement, particularly when organizational support was less robust.
Framed by Virtue Ethics and COR theory, the findings highlight how both organizational environments and internal psychological resources shape ethical behavior in nursing. Virtue Ethics emphasizes the cultivation of moral character traits such as integrity, compassion, and courage, while COR Theory explains how personal resources like resilience help nurses manage the emotional demands of ethical conflict. Together, these frameworks offer a robust explanation of how ethical climate and moral resilience interact to support nurses’ moral functioning.
The study also identified meaningful differences in perceptions and outcomes across socio-demographic and professional groups including age, marital status, educational background, clinical experience, and work units, which emphasizes the value of tailored interventions. For example, resilience-building programs may be especially beneficial for mid-career nurses, while enhanced ethics education can strengthen moral reasoning among diploma-prepared nurses. Notably, bachelor’s programs in Egypt already integrate ethics courses and training in communication and caring, which may explain higher moral competence among these nurses. Hospital management should implement ongoing training and educational programs that emphasize inter-professional collaboration to enhance patient experience and effective teamwork (Ashour et al., 2025).
By contextualizing these findings within the Egyptian healthcare setting and comparing them with international evidence, this study adds to the global understanding of moral capacity in nursing. The results call for institutional investments in ethical climate development, ethics education, and support systems that address nurses’ moral and psychological needs. In increasingly complex clinical environments, fostering a culture of ethical excellence and psychological resilience is essential not only for improving patient outcomes but also for protecting nurses’ well-being and sustaining organizational integrity. Future research using longitudinal or multi-method designs is recommended to deepen understanding and validate these relationships across diverse healthcare systems.
Strengths and Limitations
This study offers a robust and integrated examination of the relationships among ethical climate, moral distress, moral courage, and moral resilience, framed through the dual theoretical lenses of Virtue Ethics and COR theory. By grounding the investigation in both moral philosophy and psychological resource management, the study advances a comprehensive understanding of how nurses navigate ethically challenging environments. The use of well-validated instruments, rigorous statistical analysis, and adequate sample size enhances the reliability and credibility of the findings. Moreover, the inclusion of a range of demographic and professional variables provides nuanced insights into how personal and contextual factors shape nurses’ ethical perceptions and responses.
However, several limitations should be acknowledged. The cross-sectional design limits the ability to draw causal inferences, as the relationships observed represent associations at a single point in time. Additionally, the use of self-reported measures for both predictors and outcomes may raise concerns about common method variance. Although methodological safeguards—such as the use of previously validated scales, voluntary participation, and confidentiality assurances—were in place to mitigate potential bias, future research could further address this issue through the use of time-lagged designs, multi-source data, or additional procedural controls.
The study was also conducted in a single Egyptian teaching hospital, which may constrain the generalizability of findings. Nevertheless, the structural and operational features of this institution—such as hierarchical governance, public funding, and standardized nursing roles—are comparable to many healthcare settings across the Middle East and North Africa (MENA) region and other similar contexts. As such, the findings may still offer relevant insights for institutions operating under similar organizational conditions.
To strengthen future research, longitudinal and multi-site studies are recommended to explore how ethical climate and moral constructs evolve over time and across varying healthcare environments. Incorporating qualitative or mixed-methods approaches may also deepen understanding of the underlying dynamics shaping moral resilience and ethical behavior in nursing practice.
Implications and Recommendations for Practice and Future Research
The findings of this study offer critical implications for nursing practice, education, and organizational policy. Given the significant relationships identified among ethical climate, moral distress, moral courage, and moral resilience, healthcare institutions must take deliberate action to cultivate environments that support ethical behavior and psychological well-being.
Recommendations for Practice
Healthcare organizations should prioritize the development and maintenance of supportive ethical climates. This includes establishing clear ethical guidelines, fostering transparent and inclusive communication, and ensuring consistent role modeling of ethical behavior by leaders. A strong ethical climate not only reduces moral distress but also enhances moral courage and resilience, enabling nurses to act with confidence even in ethically complex situations.
Institutional efforts should also focus on integrating resilience training into ongoing professional development programs. These initiatives should include skill-building in emotional regulation, moral decision-making, and ethical reflection. Drawing from the Conservation of Resources Theory, such training can help nurses protect and replenish their psychological resources in times of moral adversity. Recognizing the influence of demographic and professional factors, tailored empowerment strategies should be implemented. For example, mid-career nurses, who often report higher moral distress, may benefit from structured peer support and ethics coaching. Female nurses may require leadership development opportunities to strengthen their advocacy voice within hierarchical healthcare systems. Similarly, diploma-prepared nurses could be offered bridging programs to enhance ethical reasoning and resilience, aligning with the higher competencies observed among baccalaureate-prepared nurses who already receive formal ethics education in Egypt.
At the policy level, institutional frameworks should be re-evaluated to ensure that ethical concerns raised by nurses are addressed promptly and without fear of reprisal. Embedding ethics committees, mentorship schemes, and well-being support systems within hospitals can reinforce a culture of ethical integrity and trust.
Recommendations for Future Research
To build on these findings, future research should adopt longitudinal designs to clarify the causal relationships between ethical climate, moral resilience, moral courage, and moral distress over time. Tracking changes in these constructs across different career stages and organizational settings would provide a more dynamic understanding of nurses’ ethical development.
Further investigations should assess the effectiveness of targeted organizational interventions, such as mentorship programs, structured ethics rounds, and resilience-building workshops. Evaluating their impact on both ethical outcomes and psychological well-being will provide evidence-based guidance for scalable implementation.
Given the influence of cultural and systemic context, comparative studies across regions—especially in low- and middle-income countries—are needed to explore how cultural norms, healthcare structure, and educational curricula shape nurses’ moral behavior and coping strategies. For instance, future research could explore how Islamic or collectivist cultural frameworks influence moral courage or resilience in Arab and Asian settings.
Additionally, intervention-based research should examine the impact of demographic-specific programming, such as resilience training tailored by years of experience or gender, on nurses’ ethical engagement and retention. Understanding these variations will allow for the design of context-sensitive programs that enhance moral competence and job satisfaction across diverse nursing populations.
In summary, advancing ethical nursing practice and professional sustainability requires both organizational transformation and research-driven innovation. By fostering supportive climates, developing individual resilience, and addressing demographic needs, healthcare systems can empower nurses to uphold ethical standards, safeguard their well-being, and deliver high-quality patient care in increasingly complex clinical environments.
Supplemental Material
sj-docx-1-sgo-10.1177_21582440251381063 – Supplemental material for Navigating Connections: How Moral Resilience Shapes Ethical Climate, Distress, and Courage Among Nurses
Supplemental material, sj-docx-1-sgo-10.1177_21582440251381063 for Navigating Connections: How Moral Resilience Shapes Ethical Climate, Distress, and Courage Among Nurses by Ebtsam Aly Abou Hashish and Noura Mohamed Fadl Abdel Razek in SAGE Open
Footnotes
Acknowledgements
We would like to thank all the nurses who agreed to participate in this research study.
Ethical Considerations
This study involved human participants and adhered strictly to ethical research standards. Ethical approval was obtained from the Ethics Committee of the Faculty of Nursing, Alexandria University (IRB00013322), as well as the hospital’s administration. To minimize any risk of harm, the study used a descriptive, cross-sectional, questionnaire-based design with non-invasive data collection. No clinical interventions were involved, and the anonymity and confidentiality of all participants were strictly maintained. Participation was entirely voluntary, and nurses were clearly informed that they could withdraw at any time without any consequences. The potential benefits of this research—such as improving understanding of how ethical climate and moral resilience influence nurses’ well-being and ethical practice—were deemed to outweigh any minimal risks related to psychological discomfort from reflecting on ethical challenges. These risks were mitigated by framing the survey items sensitively and assuring participants of confidentiality.
Consent to Participate
Written informed consent was obtained from all participants after explaining the study’s objectives, procedures, and their rights. Data were anonymized and securely stored, with access restricted to the research team.
Author Contributions
E.A.A.H. and N.M.F.A.R. have substantial contributions to conceptualization, methodology, software, data curation, and writing—original draft preparation. E.A.A.H.: final manuscript draft and correspondence.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data are available upon the request from the corresponding author.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.