
Abstract
In order to mitigate job burnout among medical staff and enhance their physical and mental well-being, this study proposes the construction of a hospital gym as a solution to address the issue of physical inactivity among medical professionals. Against the backdrop of China’s “National Fitness Program,” this research develops a game model that encompasses various scenarios involving hospitals and medical staff, both with and without government incentives. Our findings demonstrate interdependence in the decisions made by government entities, hospital administrators, and medical staff regarding gym construction and use. Hospitals’ commitment to gym construction positively influences medical staff’s willingness to engage actively. Two stable equilibrium strategies emerge: one where hospitals and medical staff do not engage with gyms, and the other where both hospitals and medical staff actively utilize them. Government incentives are crucial in promoting a balanced strategy. Additionally, various factors significantly impact the strategy choices of each stakeholder. This study offers valuable benefits to stakeholders, including hospital administrators and medical staff, by exploring how gym construction can lead to reduced burnout, improved work efficiency, and better health outcomes. The research highlights the critical role of government incentives in supporting the successful implementation of such facilities, ensuring that hospitals and staff can reap long-term benefits from these interventions.
Introduction
Healthcare professionals, including doctors, nurses, and other medical staff, form the backbone of any healthcare system (Weinberg & Creed, 2000). Their roles are demanding, often characterized by long hours, high-pressure situations (Ooms et al., 2022), and the need for immediate and accurate decision-making, all of which are necessary to ensure patient care and safety (Bijani et al., 2021). Over time, these factors contribute to increased physical strain and mental fatigue (Kisely et al., 2020; Rana et al., 2020). Studies have consistently shown that healthcare workers are particularly susceptible to job burnout, which manifests as a combination of emotional exhaustion (Wang et al., 2021), depersonalization (Miguel-Puga et al., 2021), and a reduced sense of personal accomplishment (Bridgeman et al., 2018). Burnout in this critical sector not only impacts the well-being of the professionals themselves but also undermines the overall quality of care, leading to higher turnover rates and reduced patient satisfaction (Shanafelt et al., 2018).
Addressing the physical and psychological health of healthcare workers is, therefore, paramount for the sustainability of healthcare systems globally (El Keshky et al., 2020). Numerous interventions have been explored to mitigate burnout, ranging from organizational reforms to psychological support systems (West et al., 2016). One of the most effective and widely endorsed solutions is increasing access to regular physical activity. Research has shown that engaging in physical exercise can alleviate stress, reduce anxiety (Pieh et al., 2020), improve emotional regulation (Chan et al., 2019), and enhance both physical and mental well-being (Faulkner et al., 2021). Physical activity also plays a vital role in improving job satisfaction and enhancing work performance, making it a practical tool for addressing both the personal health of medical staff and their professional output (Fang et al., 2019). Despite these benefits, healthcare workers often find it difficult to engage in regular physical exercise due to systemic barriers such as irregular working hours, shift work, and the lack of access to on-site fitness facilities (Saridi et al., 2019). These obstacles not only diminish the opportunity for healthcare workers to maintain their health but also exacerbate the physical and psychological toll of their profession.
Irregular working hours are not only a challenge for healthcare professionals but are also common in sectors such as emergency services, manufacturing, and transportation (Karhula et al., 2020). However, in healthcare, where high-stakes decision-making and patient interactions are frequent, the consequences of such schedules may be particularly severe (L. J. Taylor et al., 2019). The combination of long working hours, emotional demands, and physical fatigue leaves little opportunity for healthcare workers to engage in physical activity, which could otherwise serve as a preventive measure against job burnout (R.-T. Lin et al., 2021). Studies have shown that healthcare workers experience higher levels of job stress and burnout when there are insufficient opportunities for rest, recovery, and physical exercise (Appelbom et al., 2024). Therefore, addressing these scheduling constraints by providing on-site fitness facilities in hospitals could be an effective strategy to promote regular physical activity and improve the overall well-being of healthcare workers.
In light of these challenges, this study proposes the construction of dedicated gym facilities within hospitals as a potential solution to improve accessibility to physical activity for medical staff. Providing on-site fitness options offers healthcare workers the flexibility to incorporate exercise into their routines, even within the constraints of demanding schedules. By encouraging participation in physical activities, hospital administrators can expect not only a healthier workforce but also improvements in work efficiency, reductions in burnout, and better overall performance outcomes for the hospital. The idea is that physical activity can become a core aspect of employee well-being, with direct benefits for hospital operations. While external policies, such as China’s “National Fitness Program,” encourage broader societal engagement in physical activity (Tan, 2015; Zheng et al., 2022), this study focuses on the internal dynamics within healthcare institutions that influence the decision-making process around implementing gym facilities.
This study proposes that hospital administrators can improve the accessibility of physical activity by constructing gym facilities and encouraging medical staff participation. Such participation can benefit hospital administrators as well, including reducing medical staff burnout, enhancing work efficiency, and generating more favorable outcomes for the hospital. Previous research on medical staff’s involvement in physical activities has primarily focused on aspects like physical activity and anxiety (Kua et al., 2022), stress awareness (Kumar et al., 2020), and health and lifestyle (Anderson & Durstine, 2019). These studies often employ structural equation modeling, interviews, and qualitative research methods to examine the relationship between physical activity and other variables (Aperribai et al., 2020; Dahlberg et al., 2018; Kang et al., 2018; Maugeri et al., 2020; Mohammadi et al., 2021; Ross et al., 2023). However, human behavioral patterns are dynamic, and static analysis may struggle to elucidate decision-making processes and psychological struggles (Vairavasundaram et al., 2022).
To address this research gap, our study introduces evolutionary game theory for the first time to explore medical staff’s engagement in physical activity, offering dynamic insights into stakeholder behavior. While previous research employing game theory has touched upon issues involving medical staff, such as medical disputes (Zeng et al., 2018), nurses allotment (Dash & Sahu, 2022), and the efficiency of artificial intelligence-internet of things in hospitals for medical workers (Kumar et al., 2020), there has been no scholarly exploration of game theory’s application to the physical activity of medical workers.
While this research considers the context of China’s “National Fitness Program,” the model and findings are broadly applicable to healthcare systems in various countries. The core focus is on the interactions between hospital administrators and medical staff and their decision-making processes regarding gym construction and usage, which have relevance regardless of regional or policy-specific contexts. This study provides insights that could be applied globally, as the interactions between hospital stakeholders are universally significant in addressing healthcare workers’ well-being.
The objectives of this study are to examine the strategic interactions between hospital administrators and medical staff regarding gym construction, analyze the influence of government incentives, and evaluate the long-term impacts on staff well-being and hospital efficiency.
The remainder of this paper is structured as follows: Section 2 introduces the relevant policies and theoretical framework that underpin this study. Section 3 outlines the methods, including problem description, basic assumptions, model construction, and analysis. Section 4 presents the results using phase diagrams and numerical simulations to illustrate and verify the model’s construction. Section 5 discusses implications for future research, emphasizing the roles of the government, hospitals, and medical staff. Section 6 concludes by summarizing the study’s findings and discussing limitations and potential future directions.
Literature Review
National Fitness Program
China’s “National Fitness Program” is a policy aimed at promoting nationwide fitness, first introduced in 1995 and continuously strengthened through a series of laws and policy documents (D. Lin et al., 2024). The legal basis for this program includes documents such as the “Sports Law of the People’s Republic of China” and the “Regulations on National Fitness.” These regulations clearly outline the responsibilities and obligations of government departments at all levels in promoting public fitness (Cai & Ye, 2023). Specifically, the “Regulations on National Fitness” emphasize the establishment of fitness facilities and the provision of policy incentives to encourage participation in physical activities (Zheng et al., 2022), especially among high-stress occupational groups such as healthcare workers. The government supports the construction of fitness facilities by offering financial subsidies and tax incentives, aiming to improve employees’ physical well-being and work efficiency.
Feasibility of Applying Evolutionary Game Theory
Game theory was originally developed by the American mathematician von Neumann and the economist Oscar Morgenstern. They believed that game theory is a framework for studying behavioral interactions and decision-making among individuals with vested interests. Subsequently, game theory gradually entered the field of biology, laying the foundation for evolutionary game theory. Nash (1951) proposed the “explanation of group behavior” and elaborated on a relatively complete evolutionary game theory. Lewontin (1961) used the concept of strategic interaction to construct a game model of competitive evolution between organisms. In order to analyze the laws of biological evolution, Smith and Price (1973) transformed the payoff function in traditional game theory into a biological fitness function and introduced mutation mechanisms, proposing the classical concept of evolutionary stable equilibrium. P. D. Taylor and Jonker (1978) and Smith (1988) introduced selection mechanisms and constructed the famous replicator dynamics equation. Subsequently, Friedman (1991) further explored the application of evolutionary games in the economic field, making important contributions to the analysis of stable equilibrium in evolutionary games. Weibull (1997) provided a comprehensive exposition of evolutionary game theory. Since then, evolutionary game theory has rapidly developed and has been frequently applied in the field of management, receiving widespread attention. Many scholars have used evolutionary game theory to analyze the behavioral interactions and decision-making processes between parties with vested interests, such as the impact of government subsidies and taxes on the performance and behavior of supply chain enterprises (Mahmoudi & Rasti-Barzoki, 2018); the strategic adjustments of governments and shared mobility platforms in achieving stable equilibrium by reducing costs (Sun et al., 2019); the impact of government incentive measures on enterprises’ strategies for developing green buildings (Fan & Hui, 2020); and the strategic choices for public transportation under government incentives and penalties (Chen & Li, 2024).
In this study, whether the hospital builds a gym and whether medical staff use the gym are both decisions involving benefits and drawbacks. Therefore, both the hospital and medical staff will weigh the costs and benefits when making decisions. Over time, as stakeholder decisions evolve, the hospital and medical staff may adjust their decisions, leading to a long-term and repetitive game process. Moreover, as the initiator of policies, the government has a strong incentive effect and can strengthen the willingness of the parties through various incentive policies. Therefore, using evolutionary game theory to explore the decision-making interaction between hospitals and medical staff under different scenarios, with or without government incentives, is both feasible and scientific.
Method
Problem Description
Medical staff constitute a high-risk group for job burnout (Piko, 2006; Vincent et al., 2019). This study posits that hospital administrators can motivate medical staff to engage in physical exercise, thus mitigating job burnout, by establishing gym facilities. However, this change will inevitably alter the existing pattern of benefit distribution. Hospital administrators and medical staff, as rational actors with subjective agency, must engage in a competitive process concerning matters related to gym construction and utilization.
For hospital administrators, constructing a gym entails considerations of cost, including construction and operational expenses, as well as the potential loss of benefits due to reduced work hours for medical staff engaging in fitness activities. Furthermore, the efficiency of medical staff’s gym usage should be factored in. High utilization rates could yield greater benefits for hospital administrators by enhancing the work efficiency of medical staff. Conversely, medical staff members must weigh the benefits of physical activity, such as reduced burnout and improved work efficiency, against potential income losses due to reduced working hours. Thus, hospital administrators and medical staff engage in a decision-making process involving trade-offs between costs and benefits. This decision-making process unfolds as a long-term and recurring dynamic process with varying strategies for each participant at different points in time. The government’s “National Fitness Program” serves as a suitable mediator, given its role as the instigator of national fitness and its vital role in providing incentives. Policy innovation and other methods can alleviate the concerns of hospital administrators and medical staff and bolster their commitment.
Therefore, this study conducts an evolutionary game analysis by establishing game models between hospitals and medical staff under different scenarios of government incentives and non-incentives. Next, we will use phase diagram analysis and numerical simulation to carry out in-depth discussions. On the one hand, we aim to clarify the interaction patterns and key influencing factors between hospitals and medical staff in the construction and use of fitness centers. On the other hand, we seek to verify the positive role of the government’s national fitness policy in increasing the willingness of the parties in this game system.
Firstly, this study conducts an evolutionary game analysis between hospitals and medical staff under different government incentives. The first step is to set factor variables and construct models to demonstrate the general decision-making and game processes between hospitals and medical staff under different government incentive scenarios. The second step involves using the expected return function and replicator dynamic equations to analyze the equilibrium strategies and stability of the game process. Thirdly, we apply partial derivative methods to analyze the specific impact of various factors on hospitals and medical staff.
Secondly, this study uses phase diagram analysis, which visually displays and describes in detail the equilibrium strategies and stable points derived from evolutionary games within the phase diagrams.
Finally, numerical simulation is performed. We set specific numerical values for the factor variables, substitute them into the replicator dynamic equation, and use MATLAB to verify the impact of each factor on the various decisions made by hospitals and medical staff. The specific process is shown in the following flowchart (Figure 1).
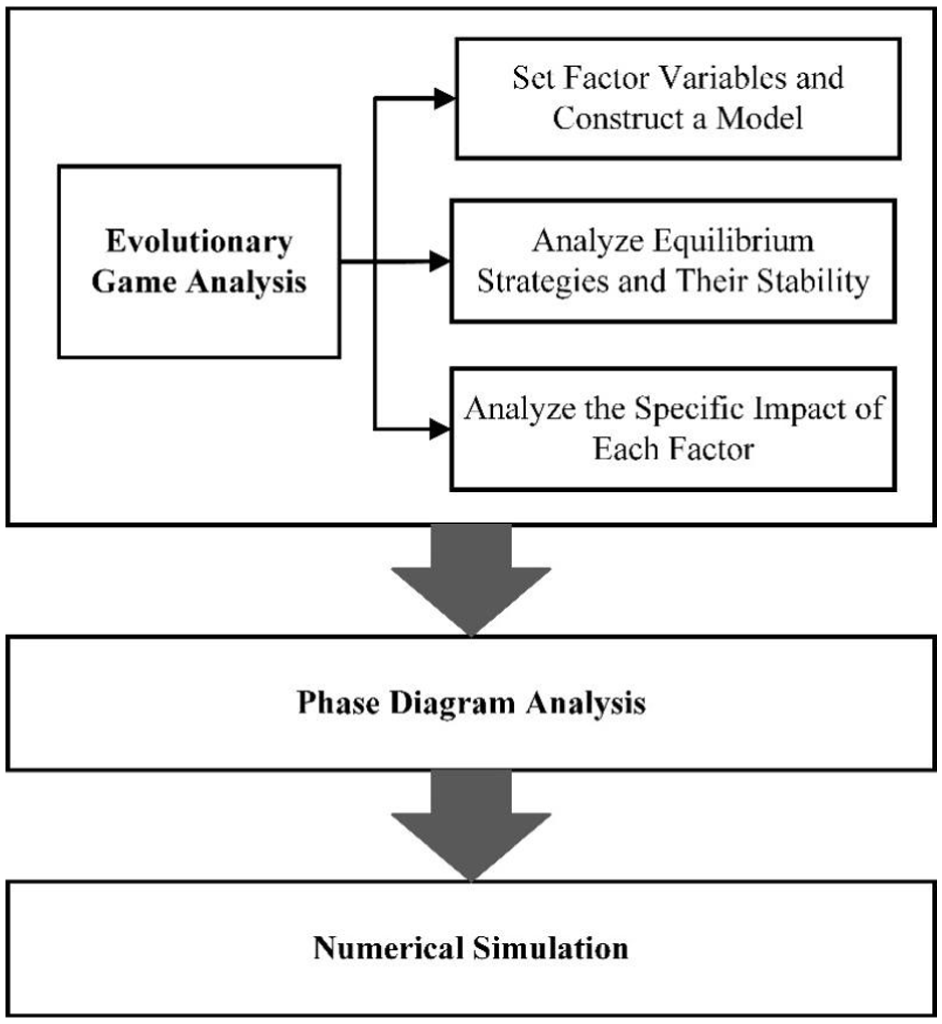
Flowchart.
Basic Assumptions
The behaviors, strategic choices, and influencing factors concerning the participating subjects - hospital administrators and medical staff - are intricate, rendering them challenging to encompass and refine. To facilitate research, this paper proposes the following assumptions:
Due to the absence of publicly available empirical data on hospital-based gym construction and usage, the parameters used in this model were not derived from real-world datasets or case studies. Instead, they were established based on theoretical logic and internal consistency, with the aim of exploring the strategic behaviors and evolutionary trends of stakeholders under different policy conditions. These parameter values represent simplified hypothetical scenarios rather than empirically validated figures. Although this limits the empirical generalizability of the results, it allows the model to serve as a conceptual tool that reveals the dynamics of incentive mechanisms and provides testable hypotheses for future empirical research. This simulation-based approach is particularly useful in the early stages of policy development, where real-world data are scarce but theoretical insights are needed to guide decision-making.
Construction and Analysis of the Game Model
Based on the above assumptions, the game matrix between hospital and medical staff under the two conditions of whether the government incentivize is established is as follows (Table 1):
Game Matrix for Hospital Administrators and Medical Staff.

Game Analysis Between Hospital Administrators and Medical Staff Without Government Incentives
Expected Return Function Construction
The next step is to construct the expected return function. The anticipated benefits of the hospital are given by:

Where:


By substituting (2) and (3) into (1), we obtain:

The expected benefits of medical staff are represented as:

Where:


By substituting (6) and (7) into (5), we obtain:

Copy Dynamic Equation Construction
According to the Malthusian dynamic equation, the replication dynamic equation can be derived from the expected return function. For instance, the dynamic replication equation for when hospital administrators choose to build a gym is as follows:
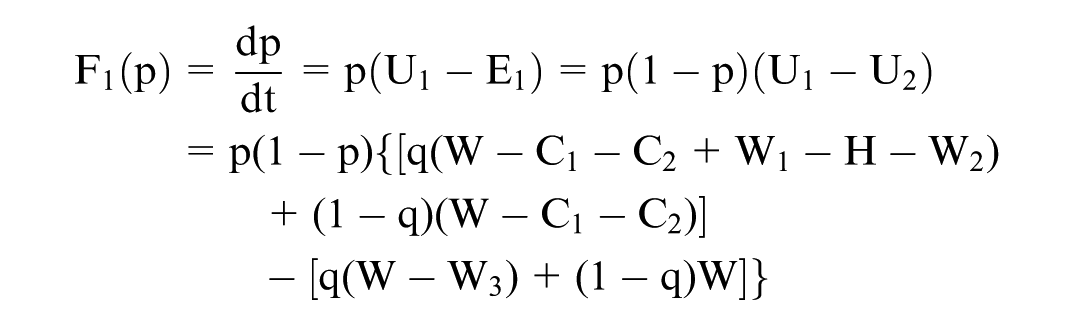
Arrange to get:

The replication dynamic equation for medical staff choosing to actively use the gym is:
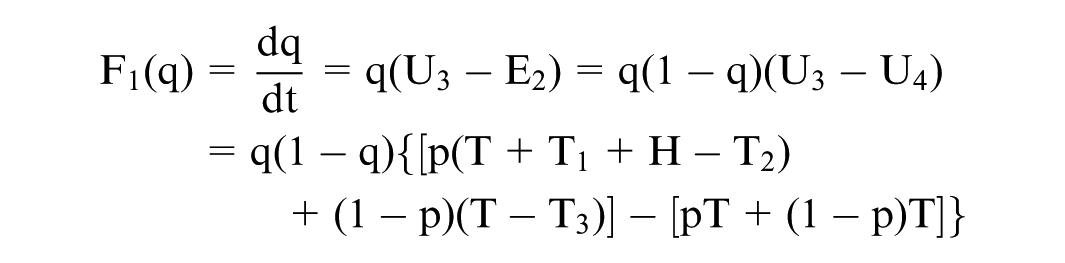
Arrange to get:

Equilibrium Strategy and Its Stability Analysis
By duplicating the dynamic equation, the two-dimensional dynamic system Dt1 of hospital administrators and medical staff without government incentives can be obtained:
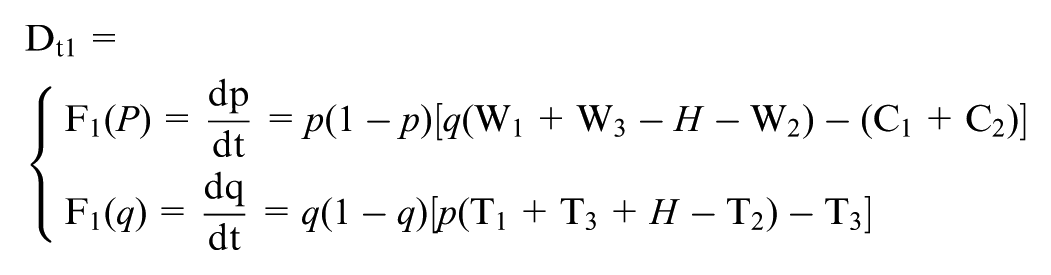
Let F1(p)=0, F1(q)=0 in the system Dt1, resulting in five partial equilibrium points of the game system: A1(0,0); B1(0,1); C1(1,0); D1(1,1);
However, not all equilibrium points are stable equilibrium strategies of the game system. According to Friedman (1991), stability can be determined by evaluating the determinant of the Jacobian matrix Det(J1) and the trace Tr(J1).
The Jacobian matrix J1 calculated from (9) and (10) is given by:

Therefore, we can get:
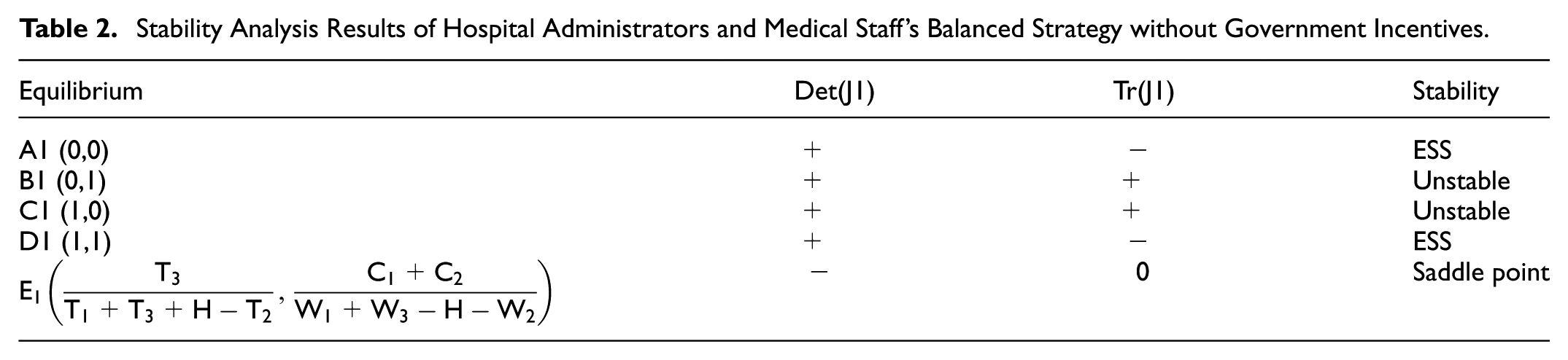
Five equilibrium points are considered in terms of Det (J1) and Tr(J1) for stability analysis, as presented in Table 2 below.
Stability Analysis Results of Hospital Administrators and Medical Staff’s Balanced Strategy without Government Incentives.
Analysis of Influencing Factors
In this analysis, we consider the area of A1B1E1C1 as S1 and the area of D1B1E1C1 as S2. The evolution of decision-making by hospital administrators and medical staff depends on the comparison of these two areas.

The following formula is used to analyze the factors that affect the tendency of the game system’s stable equilibrium strategy when the government does not implement incentive measures.
(1) The increased income T1 of medical staff due to their active exercise improves their work efficiency.
Taking the partial derivative of S1 with respect to T1, we get:

It can be seen that S1 is a monotonically decreasing function of T1. When T1 increases, S1 decreases, while S2 increases, and the stable equilibrium strategy tends toward D1 (build, active use). The higher the income of medical staff due to improved work efficiency after active exercise, the stronger their willingness to exercise, and hospital administrators are more inclined to build a gym.
(2) Loss of income T2 for medical staff due to reduced working hours as a result of active exercise.
Taking the partial derivative of S1 with respect to T2, we get:

It can be seen that S1 is a monotonically increasing function of T2. When T2 increases, S1 increases, and the stable equilibrium strategy tends toward A1 (not build, not actively use). The more income medical staff lose, the less willing they are to exercise, and hospital administrators also become less inclined to build a gym.
(3) Income T3 for medical staff due to reduced burnout.
Taking the partial derivative of S1 with respect to T3, we get:

It can be seen that S1 is non-monotonic with respect to T3, and the influence of T3 on the tendency of the stable equilibrium strategy cannot be determined.
(4) Incentive rewards H from the hospital for medical staff to actively exercise.
Taking the partial derivative of S1 with respect to H, we get:

It can be seen that S1 is non-monotonic to H, and the influence of H on the tendency of the stable equilibrium strategy cannot be determined. While higher incentives and rewards obtained by medical staff through active fitness increase their willingness to exercise, the hospital’s costs also rise, reducing the willingness of hospital administrators to build a gym. Therefore, the strategies of the involved parties are inconsistent, and the final stable equilibrium strategy trend cannot be determined.
(5) The cost C1 of building a gym in a hospital.
Taking the partial derivative of S1 with respect to C1, we get:

It can be seen that S1 is a monotonically increasing function of C1. When C1 increases, S1 increases, and the stable equilibrium strategy tends toward A1 (not build, not actively use). The higher the cost of building a gym, the lower the willingness of hospital administrators to build one.
(6) Approval costs C2 for hospital applications to build a gym.
Taking the partial derivative of S1 with respect to C2, we get the following:

It can be seen that S1 is a monotonically increasing function of C2. When C2 increases, S1 increases, and the stable equilibrium strategy tends toward A1 (not build, not actively use). The higher the approval costs for building a gym, the lower the willingness to build it.
(7) Increased hospital revenue W1 due to higher work efficiency after medical staff actively exercise.
Taking the partial derivative of S1 with respect to W1, we obtain the following:

It can be seen that S1 is a monotonically decreasing function of W1. When W1 increases, S1 decreases, S2 increases, and the stable equilibrium strategy tends toward D1 (build, actively use). The greater the benefits of medical staff actively exercising, the more willing hospital administrators are to build a gym.
(8) Hospital revenue lost W2 due to reduced working hours caused by medical staff’s active exercise.
Taking the partial derivative of S1 with respect to W2, we obtain the following:

It can be seen that S1 is a monotonically increasing function of W2. As W2 increases, S1 also increases, and the stable equilibrium strategy tends to A1 (not build, not actively use). The greater the reduction in the benefits to medical staff from active fitness, the lower the willingness of hospital administrators to build a gym.
(9) Income W3 of the hospital after easing medical staff burnout.
To find the partial derivative of S1 with respect to W3, we obtain the following:

It can be observed that S1 is a monotonically decreasing function of W3. As W3 increases, S1 decreases while S2 increases, and the stable equilibrium strategy shifts toward D1 (build, actively use). The greater the benefits of alleviating medical staff burnout, the more willing hospital administrators are to reduce burnout by building a gym.
Game Analysis Between Hospital Administrators and Medical Staff With Government Incentives
Expected Return Function Construction
The next step is to construct the expected return function. The anticipated benefits of the hospital are:

Among them:

Substituting (13) and (14) into (12), we get:
The expected benefits of medical staff are:

Among them:


Substituting (17) and (18) into (16), we get:

Copy Dynamic Equation Construction
According to the Malthusian dynamic equation, the dynamic replication equation can be calculated from the expected return function. For example, hospital administrators choose to replicate the dynamic equation for building a gym:
Arrange to get:

The replication dynamic equation for medical staff choosing to actively use the gym is:
Arrange to get:

Equilibrium Strategy and Its Stability Analysis
By duplicating the dynamic equation, the two-dimensional dynamic system Dt2 of hospital administrators and medical staff with government incentives can be obtained:
Let F2(p) = 0, F2(q) = 0 in the system Dt2, five partial equilibrium points of the game system can be obtained: A2 (0,0); B2 (0,1); C2 (1,0); D2(1,1);
The Jacobian matrix J1 calculated from (20) and (21) is:

We can calculate:
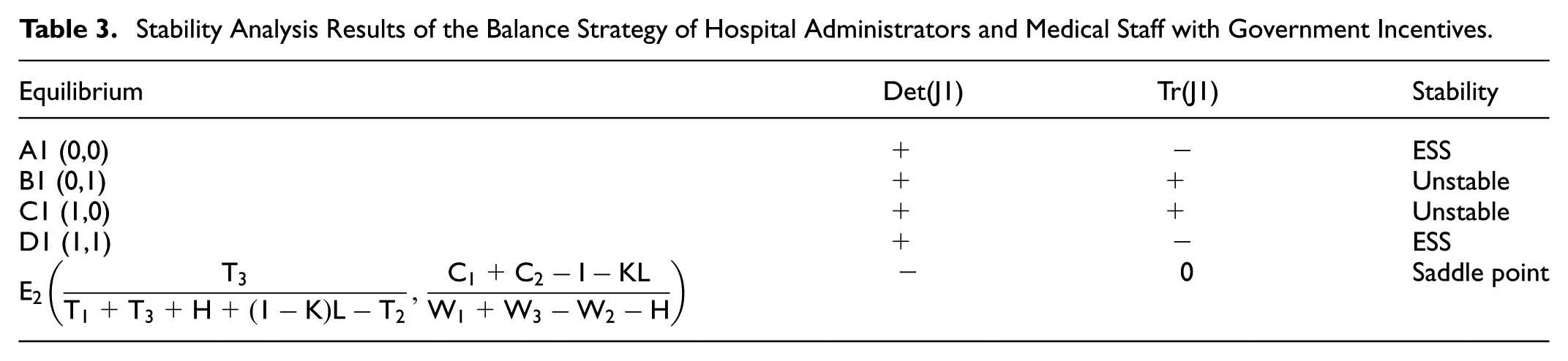
The stability analysis results of the equilibrium points are shown in Table 3.
Stability Analysis Results of the Balance Strategy of Hospital Administrators and Medical Staff with Government Incentives.
Analysis of Influencing Factors
Assuming that the area of the A2B2E2C2 area is S3, and the area of the D2B2E2C2 area is S4, the evolution of the decision-making state of hospital administrators and medical staff depends on the comparison of the size of the two areas:

The following formula is used to analyze the factors that affect the tendency of the game system’s stable equilibrium strategy when the government implements incentive measures.
(1) Proportion K of government financial and tax subsidies received by the hospital.
To find the partial derivative of S3 with respect to K, we obtain the following:

It can be observed that S3 is non-monotonic with respect to K, and the effect of K on the stable equilibrium strategy cannot be definitively determined.
(2) Fiscal and tax subsidies L for government incentives.
To find the partial derivative of S3 with respect to L, we obtain the following:
It can be observed that S3 is a monotonically decreasing function of L. As L increases, S3 decreases while S4 increases, and the stable equilibrium strategy shifts toward D2 (build, actively use). The higher the government incentives and tax subsidies, the greater the benefits for hospital administrators and medical staff, and the stronger their willingness to engage.
(3) Cost savings I from reducing administrative approval with government incentives.
To find the partial derivative of S3 with respect to I, we obtain the following:

It can be observed that S3 is a monotonically decreasing function of L. As L increases, S3 decreases while S4 increases, and the stable equilibrium strategy shifts toward D2 (build, actively use). The greater the cost savings achieved by the government through reducing administrative approval, the stronger the willingness of hospital administrators to build a gym.
Results
Phase Diagram Analysis
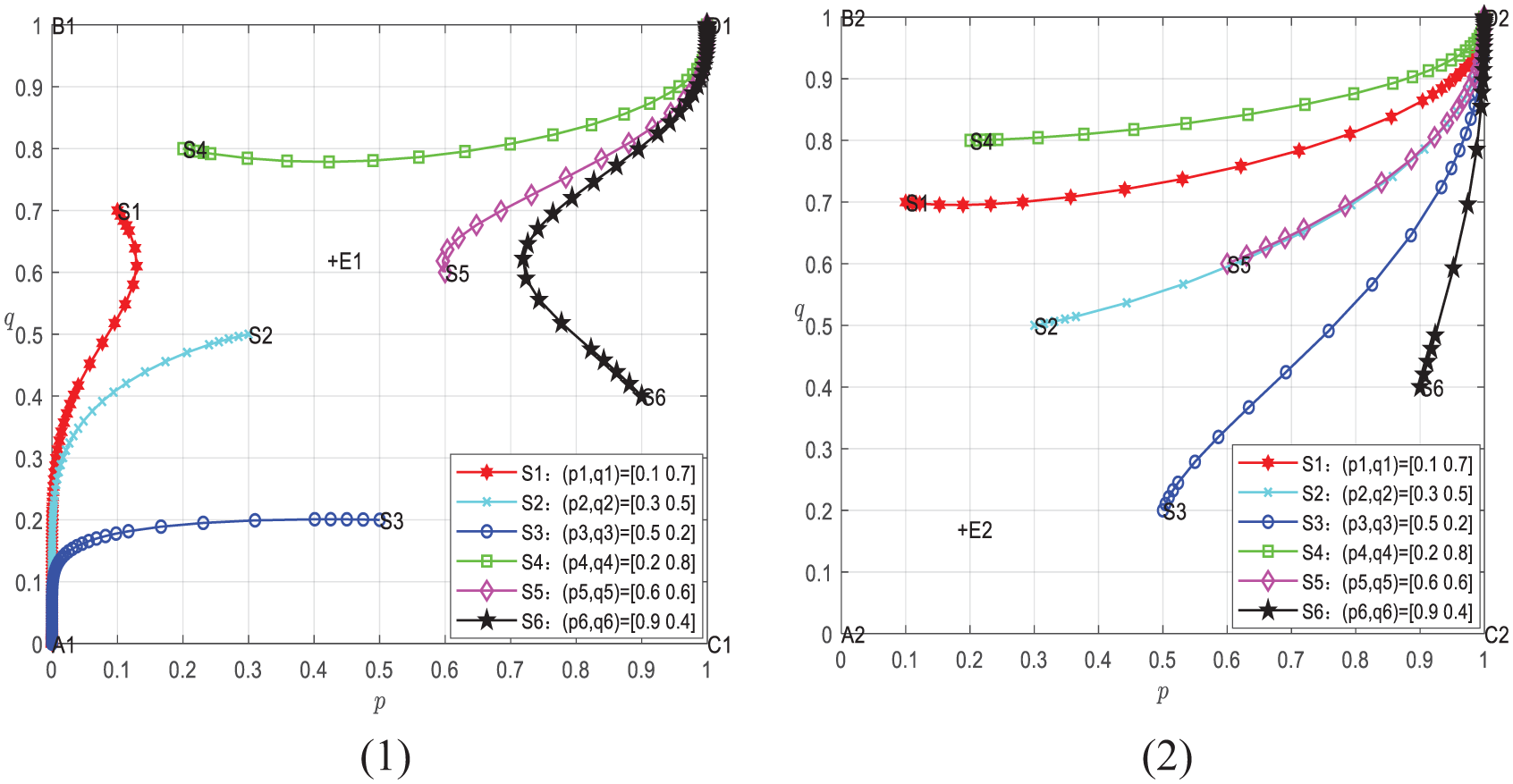
Figure 2 shows the phase diagram of the dynamic evolution of strategy selection between hospitals and medical staff, in which (1) is when the government has not implemented incentive policies, and (2) is when the government has implemented incentive policies.

The dynamic evolution phase diagram of the strategic choices of hospital administrators and medical staff.
As illustrated in Table 2, points A1 and D1 represent ESS points, which denote the stable strategy points within the evolutionary game system. These correspond to the two strategy outcomes for hospital administrators and medical staff: (not build, not actively use) and (build, actively use), respectively. Conversely, points B1 and C1 signify unstable strategy points, associated with hospital administrators and medical staff’s choices of (not build, actively use) and (build, not actively use). Additionally, E1 represents the saddle point. As depicted in Figure 1 below, when the initial decision-making position of hospital administrators and medical staff falls within the lower left quadrant of the line connecting the unstable points B1, C1, and saddle point E1, that is, the area A1B1E1C1, the system converges toward point A1. This indicates that hospital administrators and medical staff are more likely to opt for the strategy of (not build, not actively use). Conversely, when the initial position falls within the upper right quadrant of the line connecting B1, C1, and E1, corresponding to the D1B1E1C1 area, the system converges toward point D1. In this scenario, hospital administrators and medical staff tend to choose (build, actively use) strategies.
As shown in Table 3, in the presence of government incentives, the stable and balanced strategies of hospital administrators and medical staff remain unchanged as (not build, not actively use) and (build, actively use). However, the position of the saddle point has shifted significantly, with the A2B2E2C2 area being considerably smaller than the A1B1E1C1 area, while the D2B2E2C2 area is larger than the D1B1E1C1 area. Consequently, the system is more likely to converge on point D2 during this time, indicating a higher likelihood of hospital administrators and medical staff choosing the strategy (build, actively use). In other words, government incentive measures promote the stability and optimality of the (build, actively use) strategy for hospital administrators and medical staff.
Numerical Simulation
Numerical simulations of the game system were conducted using MATLAB software to visualize the evolutionary game dynamics among the various stakeholders. Additionally, these simulations shed light on the interactions between hospital administrators and medical staff, the evolution of stable equilibrium strategies, and the influence of relevant factors on the selection of primary strategies and the tendencies of stable equilibrium strategies under conditions of both government incentives and non-incentives. Essential parameters were set as follows: T1 = 170, H = 200, T3 = 50, T2 = 300, W1 = 1,250, W3 = 100, W2 = 500, H = 200, C1 = 250, C2 = 150, K = 0.6, L = 400, I = 50.
Analysis of the Interactive Influence of Hospital Administrators’ and Medical Staff’s Strategic Choices
Figure 3 presents dynamic evolution diagrams illustrating the impact of hospital administrators on the strategic choices of medical staff under conditions of incentives and no incentives, respectively. When hospital administrators’ willingness to build a gym varies, the strategic decisions of medical staff also differ. In Figure 3(1), when no government incentives are present and hospital administrators have a relatively low willingness to build a gym (p = .2, .4), the propensity of medical staff to actively use the gym gradually decreases over time, eventually approaching q = 0. Conversely, when p = .6, .8, the likelihood of medical staff actively using the gym increases over time, ultimately tending toward q = 1. Notably, a stronger inclination of hospital administrators toward gym construction leads to a quicker convergence of medical staff’s desire to exercise to q = 1. In Figure 3(2), even under government incentives, medical staff’s inclination to actively use the gym eventually tends toward q = 1, even when hospital administrators’ willingness to build is low. This underscores that, in the absence of government incentives, when hospital administrators have a low propensity to construct a gym, the optimal strategy for medical staff is to reduce their desire to use the gym actively. In contrast, when hospital administrators exhibit a strong willingness to build a gym, the optimal strategy for medical staff is active gym usage. Government incentives significantly enhance medical staff’s inclination to actively use gyms.
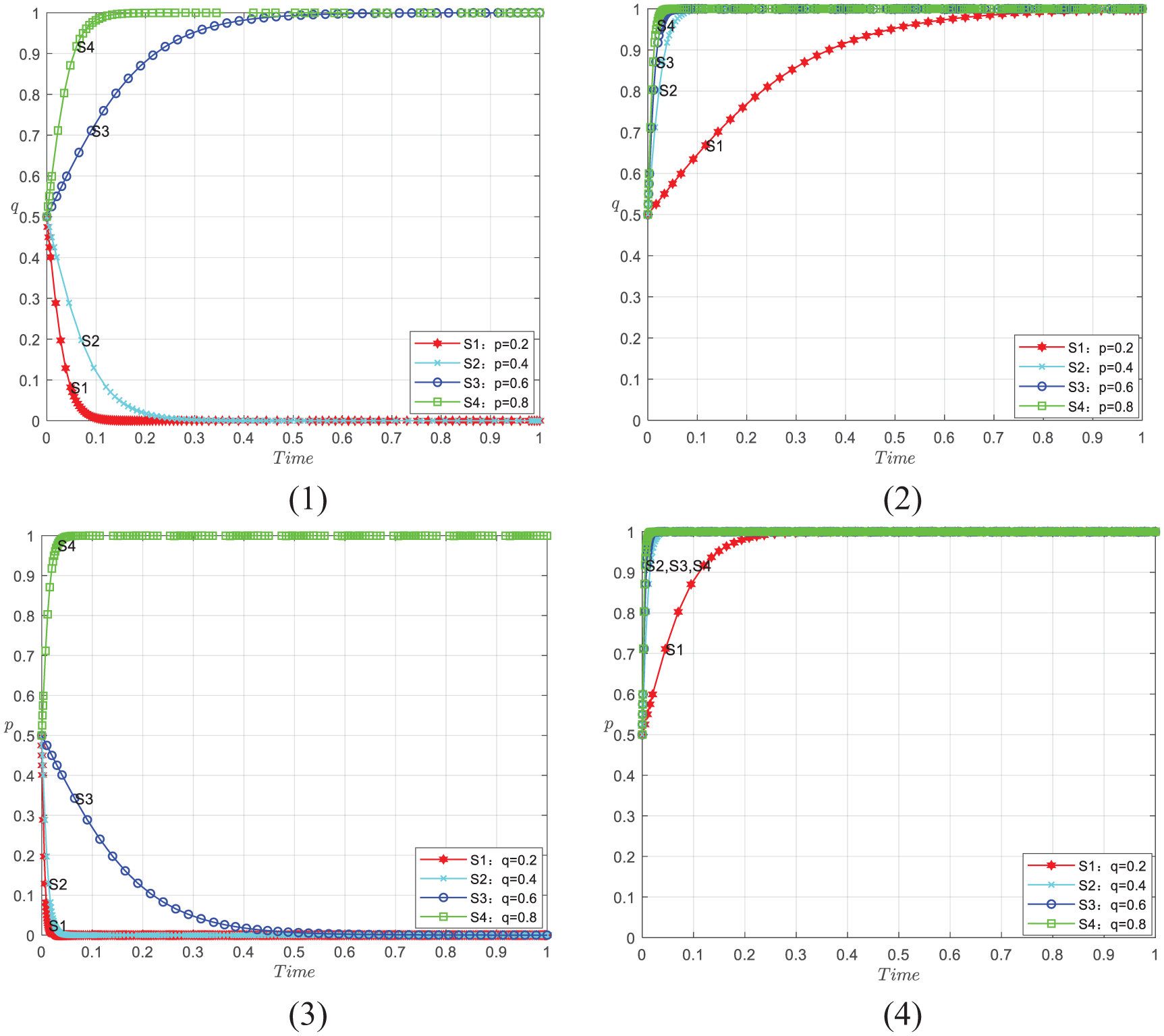
Dynamic evolution diagram of medical staff’s strategic choices.
Figure 3 represents dynamic evolution diagrams illustrating how medical staff’s choices influence the strategic decisions of hospital administrators under government incentives and no incentives, respectively. When medical staff’s willingness to use the gym differs, the strategic choices of hospital administrators also vary. In Figure 3(3), without government incentives, when medical staff’s willingness to use the gym is relatively low (q = .2, .4, .6), hospital administrators’ inclination to build a gym gradually decreases over time, eventually reaching p = 0. However, when medical staff’s willingness to use the gym is relatively high (q = .8), hospital administrators’ willingness to build a gym increases over time, ultimately reaching p = 1. A similar trend is observed in Figure 3(4), where government incentives ensure that p = 1 is eventually realized, even when medical staff’s willingness is low. This underscores that when the government does not incentivize medical staff to use the gym, the optimal strategy for hospital administrators is not to build a gym. Conversely, when medical staff actively uses the gym, the optimal approach for hospital administrators is to construct a gym. Government incentives substantially boost hospital administrators’ willingness to build gyms.
Overall, in this game system, the behavioral strategies of the subjects, namely hospital administrators and the medical staff, influence each other, and government incentives can strengthen the positive impact between the subjects. This observation aligns with the findings presented above.
Trend Analysis of Stable and Balanced Strategies of Hospital Administrators and Medical Staff
Figure 4 depicts dynamic evolution diagrams illustrating the stable and balanced strategies of hospital administrators and medical staff under government incentives and no incentives, respectively. As shown in the figures, the game system ultimately converges to different points based on the probabilities, denoted as p and q, selected by hospital administrators and medical staff at the outset.
Dynamic evolution diagram of stable equilibrium strategies.
In Figure 4(1), when there are no government incentives, the saddle point’s position is approximately at E1 (0.42, 0.62) after parameter adjustments. At this point, the initial positions located within the lower-left quadrant of the saddle point gradually converge toward the outcome A1 (0, 0), signifying (not build, not actively use). Conversely, initial positions within the upper-right quadrant of the saddle point eventually tend toward the result D1 (1, 1), indicating (build, actively use).
In Figure 4(2), when government incentives are in place, the evolution of the leading strategy choice is influenced. The original dynamic game trajectory shifts, and the saddle point position changes to approximately E2 (0.18, 0.17). Here, all initial positions are situated above and to the right of the saddle point. Consequently, all final outcomes tend toward D2 (1, 1), consistent with the findings mentioned earlier.
Analysis of the Main Parties’ Strategy Choices and Influencing Factors on Stable Equilibrium Strategies
During the game between hospital administrators and the medical staff, the changes in many related factors will impact the leading strategy choice and its stable equilibrium trend. Therefore, the following simulation process is performed. Except for the analyzed factor, the rest of the parameter settings remain unchanged.
Figure 5 illustrates the dynamic evolution of several factors influencing the strategy choices of hospitals and medical staff. S1, S3, and S5 represent the dynamic evolution trends of hospital strategy selection, while S2, S4, and S6 represent the dynamic evolution trends of medical staff’s strategy selection. Notably, when factors such as T1, W1, W3, L, and I gradually increase, S1, S2, S3, S4, S5, and S6 exhibit a rise in trends, with p and q converging to 1 more quickly. Conversely, when T2, C1, C2, and W2 gradually increase, these trends decline, and p and q tend to 0 more rapidly. Consequently, T1, W1, W3, L, and I promote the stable and balanced strategy of hospital and medical staff, tending toward (build, actively use). On the other hand, T2, C1, C2, and W2 lead to the stable and balanced strategy of hospital and medical staff, tending toward (not build, not actively use), consistent with the findings mentioned above.
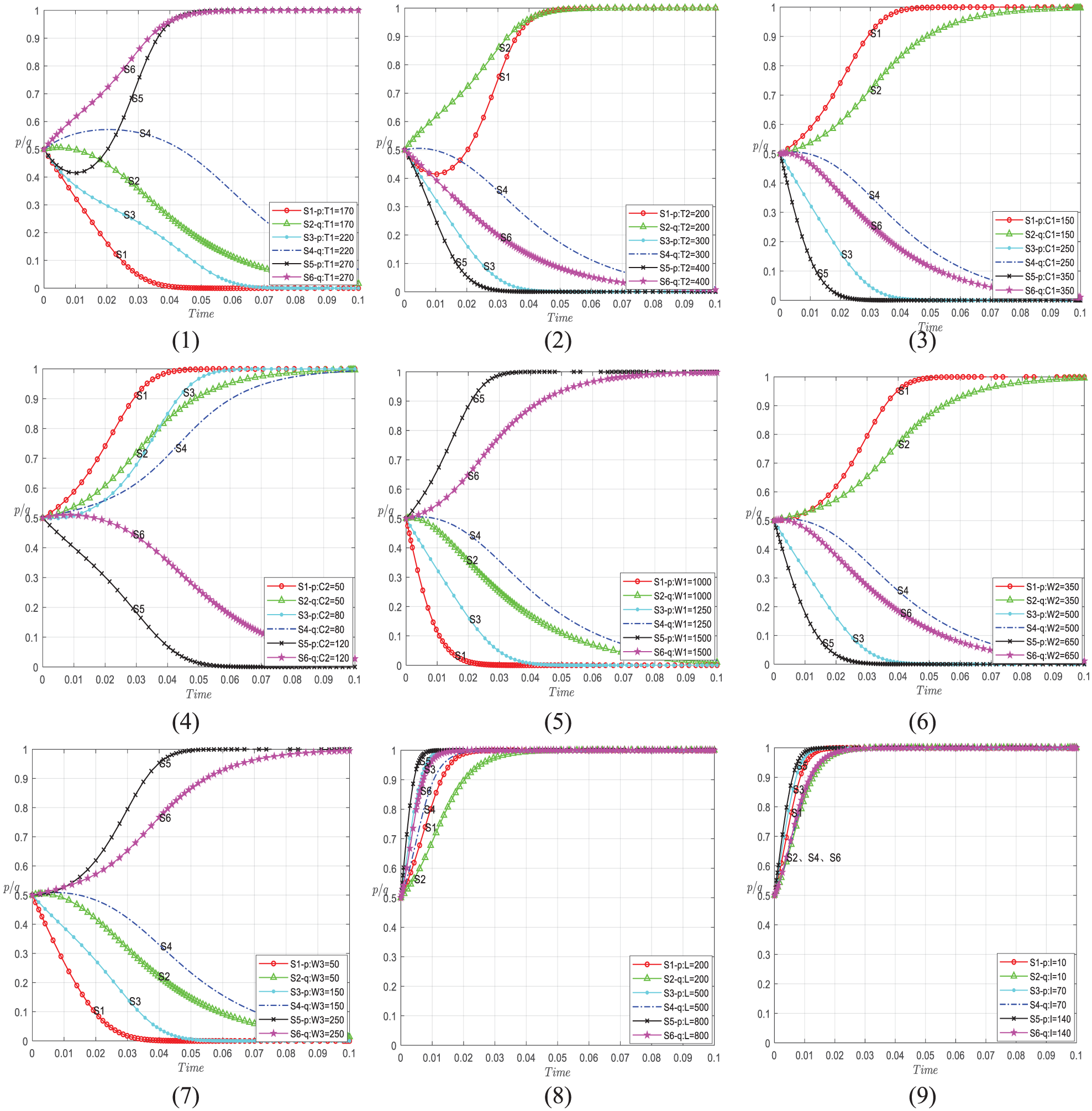
Dynamic evolution of factors influencing strategy choice in hospitals and medical staff.
Discussion
Job burnout is a well-recognized challenge among healthcare professionals due to the highly stressful and demanding nature of their work (Fares et al., 2016). Numerous studies have demonstrated that job burnout is associated with various factors, such as work environment, age, work experience, and workload (Mansour & Abu Sharour, 2021; Ndetei et al., 2008). These factors can often be mitigated through reforms in organizational culture, occupational protection, psychological intervention, and even specific training like Balint sessions (Kjeldmand & Holmström, 2008; Klein et al., 2020). However, as highlighted in this study, physical activity offers an effective approach to reducing burnout (Gerber et al., 2013). Our research extends this understanding by incorporating the strategic interactions among government, hospitals, and medical staff to show how the construction of gyms in hospitals can be a mutually beneficial solution.
Theoretical Implications
The findings from this study also contribute to the theoretical understanding of healthcare workforce management by integrating economic, psychological, and policy perspectives into a single framework. This study builds upon and expands previous literature on job burnout by highlighting the role of physical activity in mitigating burnout (Gerber et al., 2013) and offering an innovative approach through the application of evolutionary game theory. Unlike previous studies that primarily focus on organizational or individual interventions, this research emphasizes the strategic decision-making dynamics among hospitals, medical staff, and the government, illustrating how collaborative efforts can enhance outcomes.
Additionally, the study introduces new insights into how government policies, such as the “National Fitness Program,” influence internal hospital decisions. This contributes to the broader literature on policy-driven health interventions, showing that strategic government incentives can shape organizational behaviors. This finding aligns with previous research showing that top-down policy support is crucial for institutional changes, particularly in high-stress environments like healthcare (Fang et al., 2019; Mansour & Abu Sharour, 2021).
By focusing on the interaction between economic factors (e.g., gym construction costs) and behavioral factors (e.g., motivation, social support), this study provides a more comprehensive understanding of the factors influencing fitness program success in healthcare settings. Future theoretical frameworks on job burnout and health promotion could benefit from incorporating these interdisciplinary aspects to capture the complexity of decision-making in healthcare environments.
Practical Implications
The practical implications of this research are significant, as they provide hospitals with actionable strategies to reduce job burnout through physical activity interventions. Hospitals can benefit from constructing gyms to encourage physical activity, which is shown to reduce job burnout, improve well-being, and ultimately enhance work efficiency. This is especially relevant as hospitals face the challenge of balancing operational costs with staff well-being. Our findings indicate that with appropriate government incentives—such as fiscal support or tax benefits—hospitals are more likely to invest in gym construction. These findings suggest that policy intervention plays a crucial role in the practical success of such initiatives, as government support can alleviate financial barriers for hospitals, making gym construction more feasible.
Moreover, addressing psychological and behavioral factors is key to the long-term success of fitness programs. Motivation, habit formation, and social support are critical to sustaining medical staff engagement in physical activity. Practical strategies, such as offering intrinsic and extrinsic incentives (e.g., enjoyment of activity and financial rewards), help reinforce the effectiveness of gym construction. Hospitals that actively engage staff through clear communication and offer incentives, such as flexible gym hours or financial subsidies, can overcome resistance and ensure consistent gym usage.
Limitations and Future Research
While this study provides valuable insights into the dynamics of fitness programs within healthcare settings, several limitations must be acknowledged. Firstly, the evolutionary game model developed in this study is an idealized representation, focusing solely on the interactions between government, hospitals, and medical staff. In reality, other stakeholders, such as patients, insurance companies, and even private fitness organizations, may influence decisions related to gym construction and utilization. Future studies could expand the model to include these additional stakeholders, providing a more holistic view of the system.
Secondly, the factors and variables used in the model, although essential, are simplified. For example, while we consider financial incentives and basic psychological factors like motivation, the complexity of human behavior and institutional decision-making processes could involve other variables not captured in our model. Future research could explore additional influencing factors, such as organizational culture, leadership style, and workplace dynamics, which could affect staff participation in fitness programs and the decision-making process in hospitals.
Thirdly, due to the lack of publicly available empirical data on hospital-based gym construction and usage, the numerical parameters used in this model were not derived from real-world datasets or case studies. Instead, they were established based on theoretical logic, simplified assumptions, and general structural relationships found in the existing literature on health policy simulation and behavioral economics. While this limits the empirical generalizability of the results, the model is intended to serve as a conceptual tool that reveals the dynamics of incentive mechanisms and provides testable hypotheses for future empirical research. We have revised our discussion to emphasize that our findings are not predictive conclusions but rather theoretical insights to guide early-stage decision-making. We agree that empirical validation is essential and encourage future studies to collect real-world data—such as gym construction costs, employee participation rates, and hospital-level return on investment—to calibrate and test the model. Moreover, incorporating qualitative methods such as interviews or surveys could help refine parameter assumptions and enhance the model’s practical relevance.
Lastly, our study is framed within the context of China’s “National Fitness Program,” which has specific cultural, organizational, and policy characteristics. This raises questions about the generalizability of the results to other national or regional settings. While we believe the core principles derived from our study—particularly the importance of government incentives and hospital-driven fitness initiatives—are widely applicable, testing similar models in different cultural and policy environments (e.g., the U.S., Europe, and Australia) would further clarify the conditions under which hospital-based fitness programs can effectively mitigate job burnout and promote physical activity among healthcare professionals.
Conclusion
This study constructed an evolutionary game model to analyze the strategic interactions between hospitals, medical staff, and government incentives regarding gym construction and use to promote physical activity and reduce job burnout. Through our model, we identified two stable equilibrium strategies: one where hospitals do not build gyms and medical staff do not participate in fitness activities, and one where hospitals build gyms and medical staff actively use them. Government incentives were found to play a critical role in promoting the latter, more desirable outcome, as they encourage both gym construction by hospitals and participation by staff.
The strategic decisions of hospital administrators and medical staff are highly interdependent. When hospital administrators exhibit a stronger willingness to construct gyms, medical staff are more likely to engage in physical activity, and vice versa. Government incentives, such as fiscal policies and streamlined approval processes, significantly enhance this willingness by alleviating concerns about construction costs and income loss due to reduced working hours.
However, this study has several limitations that need to be further explored. Firstly, the model we constructed is idealized, focusing on the interactions between the government, hospitals, and medical staff, while in reality, other stakeholders, such as patients, may influence the dynamics. Secondly, the factors and variables in the model are relatively simplified compared to real-world conditions, and data collection presents challenges. Thus, this study relied on numerical simulations. Future research should address these limitations by using empirical and case analysis methods to validate the model and exploring additional influencing factors, such as psychological and behavioral habits. Expanding the model to include other stakeholders would also provide a more comprehensive view of the system.
Lastly, we urge governments and hospitals to fully consider the key factors identified in this study, such as the balance between costs and benefits, when promoting the active participation of medical staff in physical activities through gym construction. Government incentives through fiscal and tax policies can alleviate financial concerns, while hospitals can implement internal incentive mechanisms to encourage staff to engage in fitness activities. These measures will help ensure the effective implementation of fitness programs, promote the physical and mental well-being of medical staff, and enhance the overall efficiency and service quality of healthcare institutions.
Footnotes
Acknowledgements
The authors gratefully acknowledge the reviewers.
Ethical Considerations
This research did not involve human subjects, animals, or any biological materials which typically require ethical review. Instead, the study is based on computational modeling and simulation, focusing purely on theoretical or technical aspects that do not engage with ethical concerns typically associated with experimental research. Consequently, an ethics review was not applicable for this study.
Author Contributions
H.W. and H.F. contributed to conception and design of the study. H.F. organized the database. H.W. and H.F. performed the statistical analysis. H.W. and H.F. wrote the first draft of the manuscript. Z.X. and Y.L. wrote sections of the manuscript. All authors contributed to manuscript revision, read, and approved the submitted version.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by the Hunan Provincial Social Science Achievement Review Committee (No. XSP2023JJZ001) and the Scientific Research Fund of Hunan University of Science and Technology (No. E52203).
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
This study does not involve issues of data sharing, as no datasets were generated or analyzed during the current study. The research discussed is simulation-based, not empirical studies reliant on actual data collection and analysis. In simulation research, researchers use computational models to simulate and predict phenomena without depending on collected real-world data. Consequently, there are no data sharing issues because no actual datasets were created or required for analysis.