
Abstract
Over a decade, there has been an unprecedented mass exodus of healthcare professionals in Nigeria’s public hospitals. This has put the healthcare sector in crisis. This paper, therefore, examined the effects of human capital flight on services rendered in public health institutions in Nigeria, using the Enugu State University Teaching Hospital, Parklane, Enugu as a study base. The study population is 621 healthcare workers (HCWs) from the four departments selected (medical practitioners/doctors, nurses, laboratory scientists, and pharmacists) in the hospital. The sample size is 243 based on Taro Yamane’s formula at (p < .05) maximum variability level. The theoretical framework used for the analysis of this study is the push-pull theory. Findings show that human capital flight has a significant and devastating negative effect on services rendered in the hospital. The paper recommends the upgrade of public hospitals with modern healthcare facilities; and improving conditions of service and welfare of healthcare workers, if the departure is to be halted.
Plain language summary
Purpose: This study investigated the causes of the crisis of mass exodus (human capital flight) of health workers, the extent of the occurrence of the human capital flight, and its implications on the quality of healthcare service delivery in public hospitals in Nigeria. Methods: A mixed method research approach was used. Therefore, a qualitative and quantitative field survey that leveraged both primary and secondary data was adopted in the study to descriptively content analyze data to arrive at the findings. Conclusion: The poor salaries and other negative conditions of service prevalent in public hospitals in Nigeria resulted in crisis of shortage of health workers, who are emigrating overseas where there are greener pastures (better salaries and good conditions of service). This, however, impacted negatively on the quality of the job performance of the few remaining health workers in public hospitals in Nigeria. Implications: This is a clarion call to revamp public hospitals in Nigeria to guarantee quality health services to the citizens if national development is to be achieved and sustained. Recommendations: Upgrade of facilities in the hospitals and improvement of staff salaries, welfare and conditions of service are recommended as a panacea to overcome the problem of human capital flight in public hospitals in Nigeria. Limitations: Elite corruption, insecurity, poor economy, and other negative living conditions prevalent in Nigeria might not allow many health workers to remain in Nigeria even if their salaries, welfare and other conditions of service are improved.
Keywords
Introduction
Public healthcare facilities across the globe deliver essential services to the people. Hence, hospitals and other crucial means of sustaining citizens’ livelihoods were exempted from the COVID-19 lockdown (Porto et al., 2022). The healthcare system is one of the important formal sectors where highly trained professionals are found in large numbers and various departments, cooperating and working harmoniously to provide adequate healthcare services to the citizens. Health, therefore, facilitates human capital development as a pathway for achieving sustainable growth and development of a nation’s economy (Onah, Asadu, et al., 2023; Okoro et al., 2014). The provisions of timely, efficient, effective, adequate, quality, accessible, affordable, and professional healthcare facilities and services are paramount to achieving development and ensuring collective social progress in a country. This is epitomized by the UN Sustainable Development Goal (UN SDG) Number 3 known as “Good health and well-being” of citizens, as one of the crucial factors in achieving the 17 sustainable development goals agenda (UN SDGs, 2015). The reason is that the quality of population health of the citizens is a delicate factor of national development, without which every other variable in development indices stagnates. Health, therefore, is the first key factor among other indicators of the human development index which education, the capacity to earn income, and the standard of living revolve on (United Nations Development Program, 2023).
In other words, health drives other factors of national development. Therefore, a country seeking holistic growth and development should first and foremost invest more in the health sector to achieve stable healthcare system to ensure adequate provisions of quality healthcare services to the citizens. Abah (2007) pointed that the ability to maximize effectively other resources (machines, finances, properties, mineral deposits, etc.) is subject to developing quality human capital. However, human capital itself anchors on quality health, education, training, skills, talents, knowledge, and patriotic attitudes of citizens who provide labor at the micro and macro-economies levels for national development (Onah, Amujiri, et al., 2023). Thus, there is a paramount need for consistent development of the healthcare sector, especially through research, education, innovation, improvement of conditions of service, incentivization, good salaries, and deployment of modern healthcare facilities. All these guarantee favorable working conditions that motivate and improve health workers’ performance (Attah et al., 2023), but are not provided at a significant level in Nigeria’s public healthcare sector. Alhassan et al. (2013) and Blomberg and Welander (2019) remarked that lack of constant training and retraining of health workers, applications of modern technology in health services, poor working environment, meager salaries and welfare packages, poor leadership, limited career opportunities, and the abuse of human rights are top among the reasons for brain drain in health sector in Nigeria. Unfortunately, the public healthcare sector in Nigeria lacks comfortable working conditions when compared with their counterparts abroad. This is basically due to the neglect of the healthcare sector by the authorities – government, thereby leading to the loss of healthcare professionals migrating from Nigeria to developed countries in Europe and America (Attah et al., 2023).
Despite the overwhelming importance of a stable and quality healthcare system to national development, there has been an enormous neglect of the healthcare system in Nigeria. This is evident in the myriad of human capital flight in the Nigerian public healthcare sector over the past few decades, in what has been euphemistically described as a “brain drain.”Adesote and Osunkoya (2018) noted that Africa has increasingly lost highly skilled workers over the past 30 years to developed countries. Anetoh and Onwudinjo (2020) expressed the view that highly skilled workers are leaving Nigeria at an alarming rate, and maintaining that these movements have created enormous gaps in virtually all sectors of the economy, especially in the healthcare sector. Dohlman et al. (2019) noted that over 70% of Africa’s healthcare practitioners have immigrated to developed countries leaving that sector in tatters in Africa. This according to Akinwale and Olusoji (2023) has resulted in the poor healthcare service delivery suffered by patients in Nigeria hospitals due to shortage and migration of professional healthcare workers.
Human capital flight portrays a significant increase in the amount of highly proficient workers leaving a geographic region which in most cases is their home country of origin to entirely new and different locations (Nevin & Omosomi, 2019). They engage in this movement in search of greener pastures, a better standard of living and life quality, higher salaries, access to advanced technology, and a more stable political climate (Dodani & Lapoite, 2005 in Misaur et al., 2010). In Nigeria, health workers are also frustrated because of the poor state of hospitals. Again, budget allocations by various governments to the health sector in Nigeria have been nothing but inadequate, and the insufficient funds allotted have variously found their way to individual pockets in a corruption process that has since become synonymous with Nigeria (Aduma et al., 2022). Investment in the health sector by the government is abysmal. The Nigeria Federal Ministry of Health (2004) in Aduma et al. (2022) corroborated this assertion by noting that per capital investment in health is about $1.00 per person compared to the internationally recommended standard of $34.00 per person. The same health Ministry maintains that in 2020, the health budget in Nigeria stood at N5.5bn which is less than 5% of the annual budget of the country. This is against the African Union (AU) recommendation of 15% of the annual national budgets of African countries to the health sector. All these factors form the basis for the exodus of huge human capital by these professionals.
The massive exodus of health professionals in Nigeria comes with huge negative consequences on the quality of service delivery among the remnants of the health workers. Also, human capital flights impacts negatively on the patients’ perception of the hospitals in Nigeria, and the capacity of maintaining the health facilities used in administering healthcare services in the hospitals for utmost performance. Therefore, this thesis seeks to investigate the consequences of human capital flight, especially as it concerns the delivery of service in healthcare facilities in Nigeria, using the Enugu State University Teaching Hospital, Park Lane Enugu (ESUTH) as a study base, of a known public hospital that has experienced massive outflow of healthcare professionals. Therefore, any health facility without commensurate and well-qualified human resources to manage the health challenges of the people remains a ruse and a mere white elephant project. Depletion of human resources in Nigeria’s public health facilities due to brain drain can best be described as the “realities of all times” faced by the public health facilities in Nigeria. Thus, the following research questions were raised to guide the study:
What are the drivers/causes of human capital flight in the ESUTH?
To what extent is the human capital flight in the ESUTH?
How does human capital flight affect health workers’ job performance (service delivery) in the ESUTH?
The following hypotheses were raised:
Conceptual and Literature Review
To ensure a better understanding of the dynamics of the human capital flight (brain drain) and service delivery in public hospitals in Nigeria, we interrogated and analyzed the relevant literature thematically – that is, in themes from the perspective of the independent and dependent variables (human capital flight and service delivery) driving the study.
Human Capital Flight (Brain Drain)
The migration of highly skillful, well-trained, and educated individuals for better opportunities in foreign lands is known as human capital flight. Human capital flight is a movement of professional and skilled labor (human resources) that often takes place between less developed countries and developed ones (Okafor & Chimereze, 2020). According to Andrew and Baomin (2015), major four factors are causing the brain drain in Africa, which are: (1) economic factors, (2) social and educational factors, (3) push factors, (4) and pull factors. The economic factor is the deterioration and poor performance of the economy of the less developed countries (LDCs; Docquier & Rapoport, 2012). Social and educational factors occur due to the migration of individuals in the bid for advancement in education (Dodoo & Takyi, 2002). The pull factors are due to wage differentials between the developed and developing countries (Murphy et al., 1989; Todaro, 1969), and the push factors are the high rate of unemployment in the developing economies, political instability, the high cost of running businesses, underdevelopment, lack of research facilities and institutes, political and social unrest, employment discrimination, lack of economic freedom, and poor working conditions (Ngoma & Ismail, 2013).
Human capital flight popularly referred to as brain drain means a bogus exodus of professionals with special technical skills and knowledge who migrate to other nations. The reason is often in search of greener pastures and better conditions of service and living standards. Particularly, Schultz (1981) cited in Haque and Kim (1995) noted that human capital is a critical factor in national development and economic growth. Haque and Kim (1995) asserted that brain drain stagnates the growth rate for sustainable human capital development in an economy and hence, leads to a consistent reduction in a national per capita income growth rate in the home country. Human capital flight occurs more in developing economies, especially in Africa and Nigeria in particular. Muula (2005) articulates two dimensions of human capital such as the loss of healthcare workers (hard brain drain) and the disappearance of quality research findings to utilize in Africa (soft brain drain). Therefore, human capital flight paves the way for a sustained reduction in the economic growth rate of the less developed countries. Olunloyo (2013) corroborated the above assertion on brain drain and thus posited that it leads to the migration of financial resources with cost implications in the economy. The author further noted that the reason is that emigrants leave their home countries with the knowledge value and professional skills acquired from their home countries, which they will deploy to the benefit of the foreign countries of residence.
Service Delivery
Ogonu (2020) sees service delivery as a major need that has to be effectively and efficiently provided by organizations to the satisfaction of clients/customers, as and when due. Service delivery is a component of every business process. It defines the communication/interaction and the level of relationship existing between service providers and their clients. In this business relationship, the provider offers a service and the customer/client either finds value and satisfaction in the service rendered or loses value and dissatisfaction as a result (Ogonu, 2020). Egugbo (2020) sees service delivery in public sector organizations as a contractual relationship between the members of the public and the service provider (government agency). The underlining terms of service level agreement (SLA) in the contractual relationship is that the service provider is to deliver effective and efficient services to the public in the most satisfactory manner, either in terms of utility, cost, quality, communication, timelines, courtesy, and convenience (Egugbo, 2020). Therefore, services rendered by teaching hospitals are numerous such as research, teaching/learning, individual healthcare services, training individuals, and community healthcare services. All these services require well-trained, experienced, and skillful professionals to ensure effective and efficient delivery of quality healthcare to the citizens. Unfortunately, Nigeria is losing her professional workers (Okoro et al., 2014), especially healthcare providers massively in tens and hundreds of thousands to foreign lands, following negligence of the health sector by the government (Akinwale & Olusoji, 2023; Attah et al., 2023).
The implications of losing well-trained and qualified healthcare workers result in the crisis of poor service delivery in public hospitals in Nigeria (Attah et al., 2023); and poor research outputs in teaching hospitals and health-oriented research institutes. Also, the corruption in the public health sector in Nigeria complicates the ability of the health sector to deliver and guarantee quality national health of the population (Eze et al., 2022). These have serious negative multiplier effects on national development such as medical tourism where $millions of dollars are lost yearly in Nigeria to foreign trips in search of treatments for illness due to human capital flight happening as a result of the lack of good hospitals and well-incentivized personnel (Onah et al., 2024). It also dovetails to impair the quality health status of the citizens, causing a lack of knowledge and skill retention in the country, and poverty thereby leading to a low human development index. The continuous occurrence and implications of human capital flight in developing countries are summarily manifesting in their inability to meet the sustainable development goals (SDGs) agenda of the world. Achieving the 17 SDGs pursued by countries around the world centres on having a pool of well-trained and quality citizens to man the critical sectors of the economy to drive home development (Onah, Amujiri, et al., 2023; Onah, Asadu, et al., 2023). Hence, human capital flight hinders the realization of these global goals in the less developed countries of the world, especially the Sub-Saharan Africa.
Good service delivery is paramount to the sustenance of the healthcare sector. Ogonu (2020) remarked that quality service delivery enables the recipients to have access to an increased value that is provided to them. Therefore, service delivery in the healthcare system is a streamlined process where patients receive treatment and supplies required to maintain or have an improved health. To this end, service delivery according to Keyode et al. (2013) implies both tangible and intangible goods and services to be supplied by the government or its agency, to enhance the quality of health of the people. Kayode et al. (2013) also articulated that service delivery is a conglomeration of the relationships existing among the policymakers, service providers, and the people. They maintain that service delivery encompasses supporting structures and institutions regarded as the government’s responsibility. These include but are not limited to social services such as (primary education and basic health services), and infrastructure (water, sanitation, roads, and bridges) that facilitates healthcare service delivery. Bello-Imam and Roberts (2011) quoted in Agbaet al. (2013) align with these dimensions of service delivery when they asserted that service delivery is rendering services geared toward alleviating human suffering, thereby improving the quality of life of the citizens.
Service Delivery Quality in Public Health Institutions in Nigeria
There are three categories of public health institutions in Nigeria. They are: (1) teaching hospitals, (2) pure health-oriented research institutes, and (3) health-oriented nonteaching hospitals. Each of the three public health institutions plays a critical role in rendering health services to the citizens. Public health institutions in Nigeria are government-operated public hospitals which are to provide accessible, cost-effective, specialist services that are safe and respond to individual and community needs, with efficient healthcare delivery (Adenuga & Ibiyemi, 2009). Good patient treatment and care, quality research from health-oriented research institutes, and teaching/learning in teaching hospitals, invariably, come from a pool of committed and professional health workers. In this regard, Wei et al. (2007) observed that a good healthcare system cuts-across departments and every employee, from the paramedics who bring the individual to a hospital, to the nurses who provide caregiving to sick persons, to the doctors and laboratory scientists who diagnose and administer health to the patients, and to the pharmacist who dispenses drugs to the patient. Polsa et al. (2009) in their study noted that patients from public hospitals in Nigeria’s second republic after receiving healthcare perceived service delivery quality from Nigeria hospitals as good or very good. But today, it has become certain that the reverse is now the case. This is evident in the exodus of healthcare professionals from Nigerian healthcare facilities and the surge in medical tourism due to the collapse in medical infrastructure and the lack of competent professionals who are to provide the needed health services in Nigeria (Akinwale & Olusoji, 2023).
However, after two decades the Polsa et al. (2009) study emerged, Africa has continuously lost her skilled and professional workers to developed countries in Europe and America, with Nigeria topping the list (Adesote & Osunkoya, 2018; Lawal et al., 2022). The hot spot destination countries for migrating Nigerian healthcare workers are the United Kingdom, United States, Canada, Australia, and Saudi Arabia (The Emigration of Nigerian Medical Doctors Survey Report, 2018). An insight into a segment of health workers’ brain drain in Nigeria according to the General Medical Council of the United Kingdom (GMC) revealed that about 1,197 Nigerian-trained doctors migrated to the United Kingdom from May 2023 to December 2023, thereby bringing the total number of Nigerian doctors licensed to practice in the United Kingdom to 12,198 (Deborah, 2023). This is only from the United Kingdom and from doctors’ departments only. Therefore, when you figure out the number of Nigerian-trained nurses, pharmacists, and laboratory scientists in the United Kingdom, and other foreign lands, you will be shocked that it might run in hundreds of thousands; whereas their remnants in Nigeria are insufficient.
Dohlman et al. (2019) concurred with the volatile exodus of health workers from Nigeria by stating that over 70% of Africa’s healthcare practitioners are lost to migration, where they currently make up one-fifth of healthcare practitioners in developed countries. As of 2007, there were 52,408 registered medical practitioners in Nigeria but only 14,000 applied for registration to practice. There were also 128,918 nurses and 90,489 of them registered, which translates into about 35 doctors and 86 nurses per 100,000 populations respectively (HSS-FBO Report, 2021). This scenario consequently has depleted the once-perceived service delivery quality in public hospitals in Nigeria. With this bogus brain drain, the emergence of the COVID-19 health crisis, and other push factors (poor service conditions, low salaries, nonpayment of hazard allowance, and lack of prospects for career growth), have created a huge sense of de-motivation that culminates in job dissatisfaction among health providers, thereby negatively impacting healthcare service delivery, medical education and research in Nigeria (Lawal et al., 2022; Oluwafemi et al., 2020).
The sole objectives of hospitals are to treat and cure individuals and communities of sicknesses and diseases. However, with the ever-ongoing massive human capital flight from Nigerian hospitals, by healthcare providers, it is apparent that these objectives are impacted negatively. Quality of services delivered in public health institutions in Nigeria according to Dabota (2020) has been battered due to human capital flight, resulting in occupational burnout, anxiety, and stress, which affect health workers’ job performance, thereby fueling their desires to leave their jobs. Adaka et al. (2020) succinctly averred that patients’ expectations are not realized in public hospitals in Nigeria, currently. Relatedly, Torkula (2020) bluntly postulated that there is an increasing mortality rate in Nigeria, especially in tertiary healthcare hospitals due to depletion in the quality of healthcare services rendered in the hospitals. Most of these poor service qualities are occasioned by the exodus of healthcare providers and a few other challenges.
Public hospitals; healthcare workers, patients, and the entire citizens in Nigeria are suffering the outcome of human capital flight due to its devastating multiplier effects on the Nigeria economy (Ajoseh et al., 2024). Every sector of Nigeria’s economy is witnessing human capital flight, especially in the areas of health, education, engineering, and ICT among others. In these sectors, the best brains, skills, and hands are needed to drive the innovations and development that are revolutionizing and moving the world forward, and no doubt the number and contributions of Nigerian expatriates living and working abroad in various multinational corporations (MNCs) stand out. Human capital flight, therefore, contributes significantly to the economies of the recipients and developed countries in Europe and America that harvest migrating skilled workers from the less developed countries in Africa (Lawal et al., 2022). Global economy and national development thrive on harnessing quality human capital, not the hitherto erroneous assumption that mere possession of land mass, geography, vegetation, and mineral resources are the pivotal for collective social progress of a people (Onah, 2011). Despite this reality, Nigeria is losing her best and usually the brightest workforce daily from all spheres in large numbers, to the extent that the human capital flight in the country has gained popularity with a Yoruba vernacular codenamed “japa”– meaning running away from one’s country to another; at all costs in search of greener pastures and better livelihood due to the non-availability of facilities and conditions that make life better in one’s homeland.
To curb the menace of brain drain in Nigeria hospitals, a lawmaker introduced a bill in 2023 seeking to force Nigerian health workers (doctors and dentists) to remain in Nigeria and practice in the country for at least 5 years after graduating from medical school before being fully licensed to travel to practice abroad. However, following public criticisms of the bill against the fundamental rights of health workers in Nigeria to work without servitude anywhere in the world, the bill was dropped (Adejoro, 2023; Ogundipe, 2023). Presently, the crisis of human capital flight in Nigeria is on a steady increase to the extent that the primary healthcare system in rural areas is collapsing rapidly due to lack of healthcare professionals, absenteeism, and stress emanating from work overload on the remaining staff (Nwosu et al., 2021). The reasons for all these are due to bad governance in Nigeria, corruption in the healthcare sector, and unemployment (Ajoseh et al., 2024; Eze et al., 2022). These no doubt impact negatively on the quality of health of citizens, the average life span of the national population, the human development index, and the GDP of the nation. Therefore, human capital flight contributes immensely to the crisis shaping and influencing the challenges of underdevelopment and the fight against poverty, not only in Nigeria but in the Sub-Saharan African countries (Figure 1).

Conceptual framework.
Theoretical Foundation
The theoretical framework adopted in this study is the push-pull theory. The concept of push-pull was coined by Heberle while studying factors of rural-urban migration (Niu, 2022). The push-pull theory originates from Ravenstein in 1885 through his study of distance influence. Other proponents who contributed to the refining of the theory are Bogue (1958), and Lee (1966). Ravenstein hammered on the fact that several factors helped in pushing people out of their homes or original countries and also that several factors helped in pulling them also to their adopted countries. The push factors according to Ravenstein in Osigbesan (2021) include oppressive laws, unfavorable climate, over-taxation, political instability, poor working conditions, etc. while the pull factors include the wage differential between the developed and developing countries, political stability, higher employment, etc. In Nigeria, the migration of professionals is mostly dependent on push factors which include political and ever-worsening economic instability and poor working conditions of service.
Anene et al. (2019) noted that excruciating poverty is the main push factor forcing Nigerians to move abroad. The authors further stated that this is evident in their remittances to assist relatives at home to overcome poverty when they migrate to Europe and America. Therefore, Nigerians are attracted to developed countries due to the better economy, conditions of service, and availability of infrastructure and social services. Isbell and Ojewale (2018) in an Afrobarometer survey findings reported that there are several reasons why Nigerians from the six geopolitical zones emigrate outside the country, which the desire to find better work and to escape poverty/hardship (economic reasons) top the list at 35% and 31% levels, respectively. In application of the theory to this study, it has been proven in several empirical studies that health workers are moving out of Nigeria to abroad due to poor conditions of service (push reactionary), where the working conditions are better (pull factor).
The health workers in public hospitals in Nigeria are finding solace in human capital flight due to negligence by the government. Thus, they migrate abroad where their professional and technical expertise would be adequately recognized and rewarded/compensated. Unlike in Nigeria, where bad governance system perpetrated among the political ruling elite class has crippled every sector of the economy (Onah, 2023), including the health sector. This is evident in the self-serving and unpatriotic political behaviors of Nigerian leaders. Bad policy decisions, poor annual budgetary allocation to the health sector, corruption, and political instabilities culminating in low salaries and wages, poor working conditions, outdated medical facilities, incessant strikes, limited prospects for career growth, and job dissatisfaction that de-motivate health workers in Nigeria, are the end-products of push factors of human capital flight in public hospitals in Nigeria. Based on the inherent assumption driving human capital flight, a country that does not close the gap between push-pull factors through good governance is exposing and making her economy vulnerable to becoming a poaching ground by the multi-national corporations (MNCs), and developed economies for recruitment of international workforce. Notably, developed economies have closed the push-pull reactionary gaps in their countries through good governance, and thus provided attractive job opportunities difficult to resist by foreign nationals who migrate to work in those countries. This trend has remained constant for a long time, thereby paving the way for the human capital flight in the health sector in Nigeria, due to the government’s inability to close the widening gap between push-pull factors that determine migration, development, and the level of socio-economic progress of a society.
Materials and Methods
The Study Methods
This is a quantitative field survey research in which data were sourced using both primary and secondary approaches. The primary data (quantitative) were made up of the 18 structured questionnaire items, focused group discussions (FGDs), and unstructured in-depth interviews (IDIs) from the health workers – respondents from the four major departments (medical practitioners/doctors, nursing/caregiving, laboratory/diagnosis, and pharmacy/drug dispensation) in the hospital selected for the study. The secondary data (qualitative) were materials published such as peer-reviewed journal articles; Government policy documents, Nigerian dailies (Daily Trust, Vanguard, and Punch newspapers, etc.) reportage on the mass exodus of health workers from Nigeria to other countries, Nigerian Medical Association Survey report on brain drain, textbooks, and internet materials useful to understanding the independent and dependent variables (human capital flight and poor service delivery) of the study were carefully gathered and content analyzed descriptively. This process ensures control and accuracy of the data gathered, thereby validating the results of the findings corroborated by the primary data (Onah, Aduma, & Eze, 2023). We adopted the survey research method due to its suitability in eliciting data directly from the respondents, and managing large amounts of data within a short period in this kind of field study (Jones et al., 2013). The primary data elicited from the respondents through the questionnaire were further subjected to statistical analysis; presented in tables, frequencies, percentages, the mean and standard deviation of the measurement items, and one-sample T-test analysis in other to address the hypothesis as stipulated in this study, for ease of interpretation, understanding, and drawing of conclusion.
The Population and Sample Size Selection
The population of the study is (621; Tables 1 and 2). The population distribution is as follows:
The Population of the Selected Four Main Departments in the Hospital in the Year, 2014 and 2023.

Source. Authors’ compilation from data gathered from the Administration Department, ESUTH, 2023.
Population and Sample Size Table From 2023 Data.
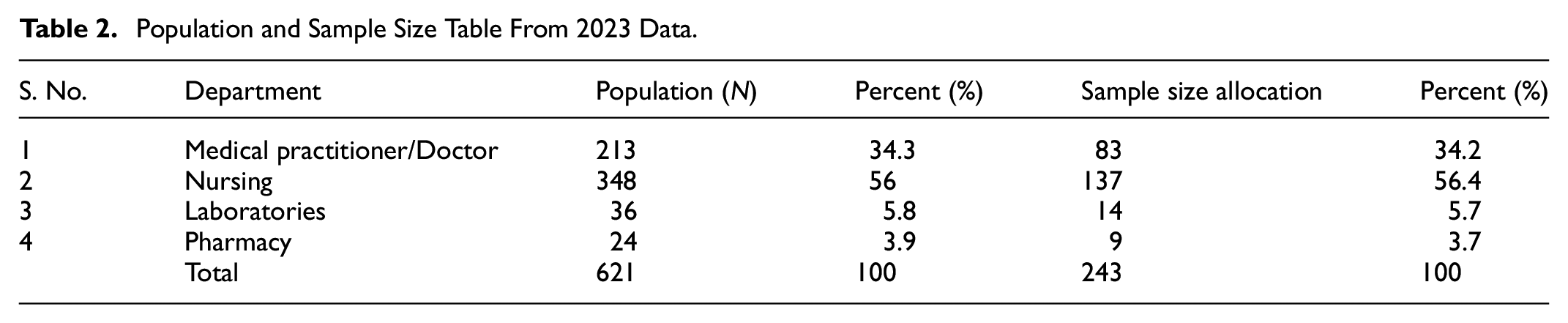
To determine the sample size for the current year (2023) population of the study – 621, we adopted Yamane’s (1967) sample size determination formula; thereby arriving at a sample size of 243, with an 86% to 92% confidence level of maximum variability (p < .05). Hence, a sample size of 243 was eventually adopted. The sample size allocation for the different departments in the ESUTH was estimated using the Kumar allocation formula. However, after the questionnaire distribution, retrieval, cleaning, scoring, evaluation, and analysis, 208 questionnaires were finally used for the study, showing a high rate (85.6%) of instrument return. The respondents were carefully selected from the members of the health workers, who constitute the four major health departments in the ESUTH. Thus, random sampling was adopted, leveraging purposive and multi-stage sampling techniques in selecting and administering questionnaires to the participants. Through the aid of two research assistants, we conducted unstructured in-depth interviews twice with the participants. Also, we conducted FGDs with some of the leaders of the four departments/units, where the top management decisions and implementation strategies were disclosed on the implications of the human capital flight (brain drain) on service delivery in the hospital were discussed in detail.
Justifications of the Study Methods and Procedures
This study is a quantitative field survey research, eliciting data from the study participants from different departments in search of relevant information on human capital flight in the hospital; using structured questionnaire instrument, unstructured in-depth interviews (IDIs), and focused group discussions (FGDs), are apt in probing deeper and obtaining relevant information from the respondents/participants. Each of the questionnaires was sent with a consent letter seeking approval to participate in the study from the health workers in the four departments being investigated. In the consent letter, we stated the intention/objective of the study, ethical compliance, risks, confidentiality, benefits, anonymity, and voluntary nature of the research, which the participants read and understood before granting their informed consent and free will to complete the survey. Confidentiality and anonymity of data were guaranteed by asking the respondents not to write their names, staff numbers, phone numbers, email addresses, and any other means of identification on the questionnaires. They filled the questionnaires in their various offices and laboratories during the rest period; either in the morning or evening, depending on the shift or work schedule a health worker - participant involved in the study underwent during the survey.
The interview sessions helped to probe deeper in corroborating the qualitative data and findings from other scholarly research outputs on the subject matter of the discourse – human capital flight and service delivery in Nigeria’s healthcare sector. These were exposed in the literature on the poor working conditions, low salaries, strikes, short supplies of consumables used in hospitals, backward medical facilities, and lack of motivation, leading to the exodus of health workers. Also, the interview sessions illuminated light on the effects of human capital flight on service delivery such as distortion of work schedules, delay in attending to patients, increase in workload, shortage of health personnel, etc. validating the crisis in the health sector in Nigeria as caused by brain drain and its drivers. The focused group discussions (FGDs) paved the way for extracting executive information from the leaders of the four departments, which such information could not have been gotten through any other means outside the leaders of the departments, who are part of the management cadre of the hospital, taking decisions and managing the crisis of low health workers-patients ratio in the hospital caused by human capital flight.
The interviews and FGDs were prepared, guided, and conducted in specific themes to maintain focus and avoid digression, though the instrument remained interactive and flexible during the sessions. Each of the two different sessions from the two different groups lasted for about 20 to 30 min, while the two research assistants took extensive notes. We did not record the respondents’ interviews and discussions during the sessions because; they insisted that we should not record them due to fear of the unknown. Thus, we respected their choice of anonymity and confidentiality stated from the onset in the consent letter sent to them. This is ethical because once a participant is recorded electronically, he/she loses anonymity and confidentiality, which is a bridge of trust and unethical in research when participants state that researchers should not record them. With all these precautionary measures, and procedures carefully designed and taken cognizance of, reliability and validity of results are assured from the study. Therefore, the findings and conclusions drawn from the qualitative and quantitative data will be accurate in making informed decisions and guiding future research in building a knowledge block on this topic.
Analytical Technique and Procedure
Being a quantitative field survey, the study adopted mixed methods of data collection and analysis, that is, both quantitative and qualitative procedures. This is triangulation and it is encouraged in modern research due to its complementarities especially in data collection and analysis (Attah et al., 2023). We utilized the Statistical Package for Social Science (SPSS) data analytical tool version 28 to code, analyze, and interpret the data sourced from the questionnaire distributed, as responses of the participants in the survey. The data was presented in tables, frequencies, and percentages with standard deviations for ease of understanding, interpretation, and drawing of conclusions.
We tested the hypotheses using one-sample statistics to find out the significance of the relationships stated. On the other hand, we organized, sought, arranged, coded, transcribed, and analyzed the secondary data gathered into themes. Points generated were further carefully placed concerning the themes developed through careful interpretation of responses. Where necessary, quotes made verbatim were adopted from the transcription to validate the primary data. Also, the face and content validity of the instrument was obtained from two psychologists, who are experts in industrial psychology at the Department of Psychology, University of Nigeria, Nsukka. Thus, the validity of the instrument is assured, because the two experts certified that the instrument asked the right questions; seeking and probing deeper into the subject matter of the research – human capital flight and service delivery in public hospitals. On reliability, the Cronbach’s alpha test coefficient was used to determine the outcome, and the associated reliability coefficient of .774 which is above the necessary threshold of .7 was used to confirm the outcome’s reliability. All these strategies deliberately designed and applied validate the methods; the choice of survey, questionnaire, and the instrument used, thereby ensuring the accuracy and authenticity of the data and findings of the study.
Result of Findings
The findings from the research questions and hypotheses tested are also included in this section. The collected data was presented and examined using tables as well as other common statistical methods including simple percentages and one sample T-test. Furthermore, brief explanations are included in the tables to enhance understanding. We used SPSS version 28.0 to carry out the data analysis in this study.
The above Table 3 reveals an analysis of the measures of the variable instrument for the drivers/causes of human capital flight in the ESUTH. The descriptive statistics reveal that low wages and salaries are a significant driver of human capital flight in ESUTH, with 89.8% of respondents strongly agreeing or agreeing. Poor working conditions also emerged as a critical factor, with 90.3% of respondents affirming its influence. Similarly, outdated medical healthcare facilities were identified as a major cause, with 88% of respondents recognizing this as a challenge. These emphasize the urgent need for improved financial compensation, better working environments, and modernized healthcare infrastructure to retain skilled personnel.
Mean and Standard Deviation of the Drivers/Causes of Human Capital Flight in the ESUTH.
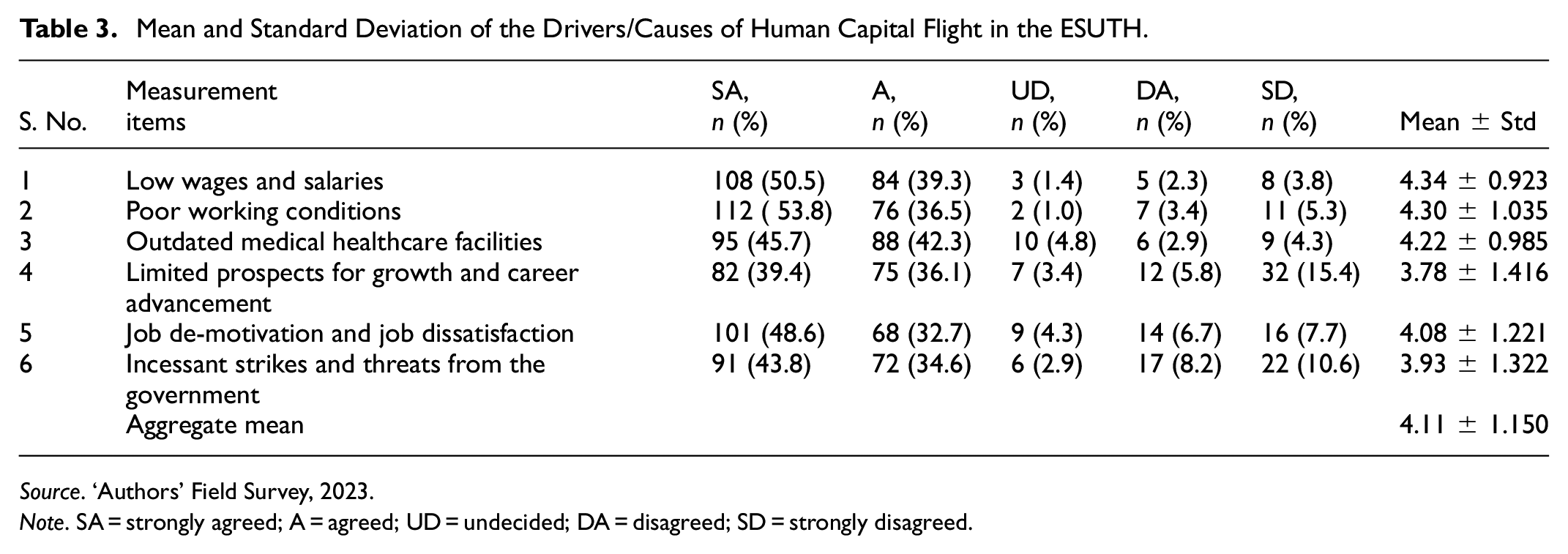
Source. ‘Authors’ Field Survey, 2023.
Note. SA = strongly agreed; A = agreed; UD = undecided; DA = disagreed; SD = strongly disagreed.
Limited prospects for growth and career advancement were also highlighted, with 75.5% of respondents agreeing that this contributes to human capital flight, although this item had slightly higher levels of disagreement compared to others. Job de-motivation and dissatisfaction received strong support, with 81.3% of respondents agreeing that it is an important driver. These results point to the importance of fostering career development opportunities and creating motivating work environments to reduce employee turnover.
Lastly, incessant strikes and threats from the government were identified as another critical factor, with 78.1% of respondents affirming their impact. While this item also had a relatively higher level of disagreement, it highlights the destabilizing effect of workplace unrest and governance issues. The descriptions in the table show the mean and standard deviation generated for all the statements on the questionnaire. The results indicate that all of the respondents agreed with the instruments. This is based on the aggregate mean score and standard deviation which is above the minimum acceptance mean of 3.0 obtained from the usage of five Likert scales. Overall, the results highlight systemic challenges within the ESUTH that drive human capital flight and stress the need for strategic interventions to address these underlying causes.
The descriptions in Table 4 show the mean and standard deviation generated for all the statements on the questionnaire. The descriptive statistics indicate that the extent of human capital flight in the ESUTH is most pronounced among medical practitioners and nurses. For medical practitioners/doctors, a combined 87.5% of respondents rated the extent as very high or high, underscoring a critical issue. Similarly, 84.6% of respondents indicated that the extent of nurses leaving the institution is very high or high. These results highlight the significant departure of these essential healthcare professionals, suggesting a severe challenge to the hospital’s capacity to deliver quality healthcare services.
Mean and Standard Deviation of the Extent of the Human Capital Flight in the ESUTH.
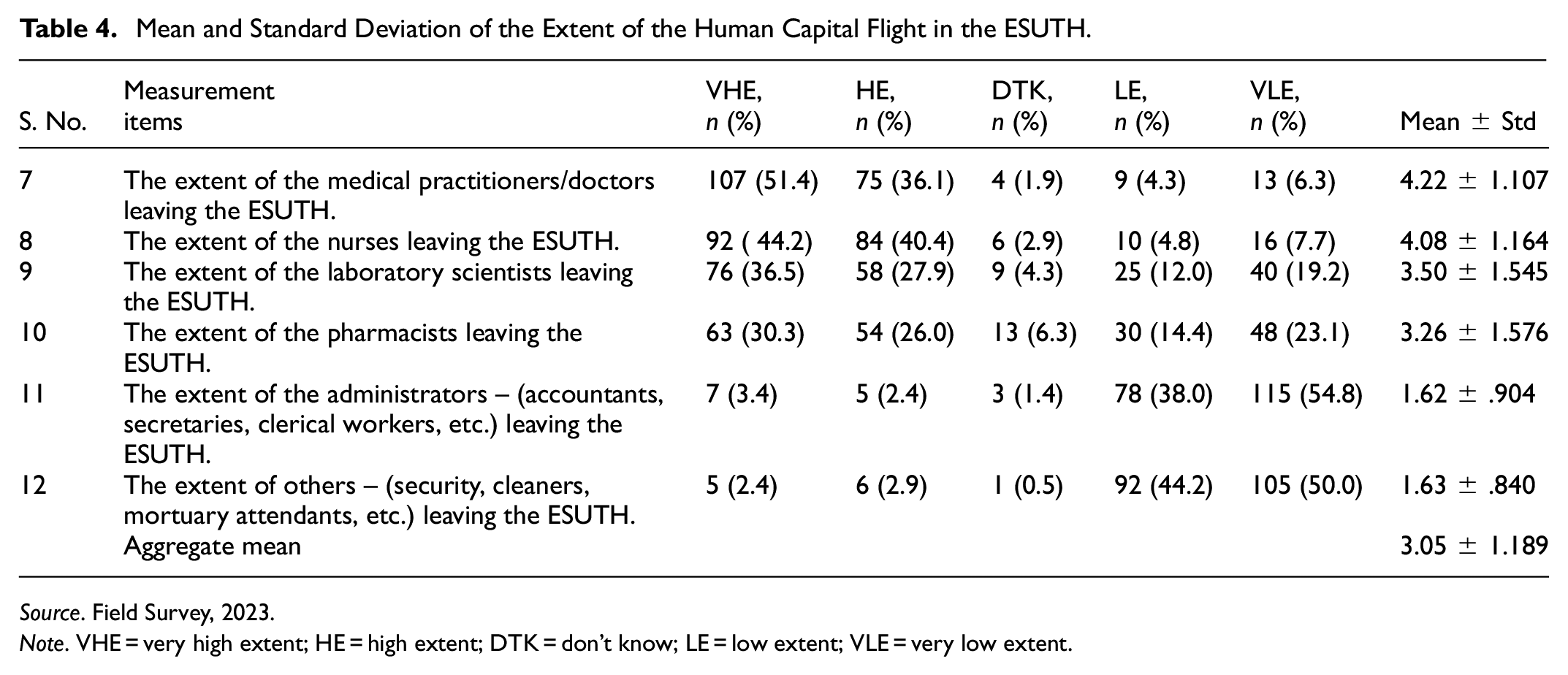
Source. Field Survey, 2023.
Note. VHE = very high extent; HE = high extent; DTK = don’t know; LE = low extent; VLE = very low extent.
The extent of laboratory scientists and pharmacists leaving the ESUTH is also notable but relatively less severe. A combined 64.4% of respondents rated the departure of laboratory scientists as very high or high, while 56.3% gave similar ratings for pharmacists. However, the higher proportions of responses indicating low and very low extents for these groups (31.2% and 37.5%, respectively) suggest that the issue, while significant, is less acute compared to doctors and nurses. This variation might reflect differences in job satisfaction or external opportunities across these professional groups.
The departure of administrative staff (accountants, secretaries, clerical workers) and non-clinical staff (security, cleaners, mortuary attendants) appears to be minimal. For administrators, 92.8% of respondents rated the extent as low or very low, and for non-clinical staff, 94.2% provided similar ratings. In summary, the result indicates that the majority of the respondents agreed with the instruments except for measurement items 11 and 12 where the respondents disagreed with the instruments claiming there is a low extent of the administrators and others (accountants, clerical workers, security, cleaners, etc.) leaving the ESUTH. This is based on the aggregate mean score and standard deviation of (3.05 ± 1.189) which is above the minimum acceptance mean of 3.0 obtained from the usage of five Likert scales. These findings suggest that the human capital flight is concentrated primarily in clinical roles, highlighting an urgent need for targeted strategies to retain medical and nursing staff who are essential to the hospital’s operations and service delivery.
The descriptions in Table 5 show the mean and standard deviation generated for all the statements on the questionnaire. The descriptive statistics highlight the significant impact of human capital flight on health workers’ job performance and service delivery at the ESUTH. A major concern is the “shortage of health workers and imbalances in patients-health workers’ ratio,” where an overwhelming 96.2% of respondents strongly agree or agree that this issue exists. This result underscores the critical strain on healthcare delivery, as the departure of staff directly affects patient care capacity. Additionally, “infrequent attendance to patients and delays in healthcare service delivery” is highly significant, with 94.8% of respondents agreeing that human capital flight disrupts the timeliness and efficiency of healthcare services.
Mean and Standard Deviation of How Human Capital Flight Affects Service Delivery in the ESUTH.

Source. Field Survey, 2023.
Note. SA = strongly agreed; A = agreed; UD = undecided; DA = disagreed; SD = strongly disagreed.
Human capital flight also leads to increased workload and stress among the remaining employees. For the measurement item “increases employees’ work overload and stress,” 90.8% of respondents strongly agree or agree, suggesting that health workers face excessive demands from the management and patients due to staffing shortages. Similarly, the distortion of shift duties and work schedules was identified as a major issue, with 80.8% agreeing. This demonstrates that staffing gaps disrupt the coordination and organization of duties, further impacting service delivery quality. Other effects include the truncation of succession plans and a decline in medical research, innovation, and publication, with 74.1% and 85.1% of respondents, respectively, agreeing or strongly agreeing with these impacts. These findings reveal the broader, long-term implications of human capital flight on institutional development and knowledge production. The results indicate that all of the respondents agreed with the instruments. This is based on the aggregate mean score and standard deviation which is above the minimum acceptance mean of 3.0 obtained from the usage of five Likert scales. Overall, the results emphasize the urgent need for measures to retain skilled professionals and mitigate the negative consequences on healthcare delivery and organizational growth at the ESUTH.
Hypotheses Testing
Hypothesis 1
Interpretation and Decision
The analysis in Tables 6 and 7 shows that the probability associated with the calculated value of significance level was .000, which is less than .05. This implies that it was significant. In other words, the null hypothesis should be rejected. Decision: At a 5% level of significance; there is a significant effect of drivers/causes of human capital flight in the ESUTH.
One-Sample Statistics.

One-Sample Test.

Hypothesis 2
Interpretation and Decision
The analysis in Tables 8 and 9 shows that the probability associated with the calculated value of significance level was .002, which is less than 0.05. This implies that it was significant. In other words, the null hypothesis should be rejected. Decision: At a 5% level of significance; the extent of human capital flight in the ESUTH is statistically significance.
One-Sample Statistics.

One-Sample Test.

Hypothesis 3
Interpretation and Decision
The analysis in Tables 10 and 11 shows that the probability associated with the calculated value of significance level was .000, which is less than .05. This implies that it was significant. In other words, the null hypothesis should be rejected. Decision: At a 5% level of significance; there is a significant effect of human capital flight on health workers’ job performance (service delivery) in ESUTH.
One-Sample Statistics.

One-Sample Test.

Discussion of Findings
The lack of availability of the right quality and quantity of human capital in hospitals, and the push factors (inadequate funding, poor conditions of service, lack of globally competitive salaries, job dissatisfaction, etc.) driving human capital flight determines the state of public healthcare facilities in Nigeria, as exposed from Table 3, and corroborated from the literature and the research findings of other scholars (Adesote & Osunkoya, 2018; Akinwale & Olusoji, 2023; Lawal et al., 2022; Oluwaseyi & Oluyemi, 2020). In other words, brain drain by healthcare providers reduces the quality and quantity of services rendered in hospitals (see Table 5 on research question 3). Therefore, the occurrence of human capital flight in Nigeria is increasingly alarming and not abating. It has been on a steady increase. The data (2014 – 908, and 2023 – 621) from the population (see Table 1) of the study vividly depicts the high rate of human capital flight in the hospital throughout a-10 year outlook. This gap (908–621 = 287) occurred despite that the ESUTH had recruited its workforce twice (in 2014 and 2023) respectively, within the 10 years under review. So, it is very clear that many of the health workers left the ESUTH based on human capital flight; and a few others on attrition. Also, Table 12 below depicts the number of healthcare providers (doctors, nurses, laboratory scientists, and pharmacists) that have left the Enugu State University Teaching Hospital (ESUTH) in a decade and sums up the dilemma.
A-10 Year Outlook of Human Capital Flight of Health Workers in ESUTH, Between 2014 and 2023.

Source. Authors’ compilation from data gathered from the Administration Department, ESUTH, 2023.
The above figures and illustrations are alarming realities of the yearly erosion of human capital flight (brain drain) of health workers at the ESUTH from 2014 to 2023 (Figures 2 and 3). The depletion of these medical professionals according to our findings (see Table 4) has naturally led to the rendering of inadequate and poor healthcare services by the few remaining medical personnel that are inadequate both in number and in expertise (see Akinwale & Olusoji, 2023; Premium Times Agency Report, 2021). This has led to a high mortality rate in hospitals and medical tourism abroad by the rich with negative economic consequences. What is more, the situation is not abating but rather exacerbating. More medical professionals are finding their way out of the system, especially doctors and nurses, followed by laboratory scientists and pharmacists, whereas other categories of employees in the ESUTH such as administrative personnel and auxiliary staff do not embark on human capital flight as evident in the primary data that addressed research question 2 (see Table 4) containing the expositions.

A bar chart showing the 10-year (2014–2023) outlook of the human capital flight of health workers (doctors, nurses, laboratory scientists, and pharmacists) in ESUTH.
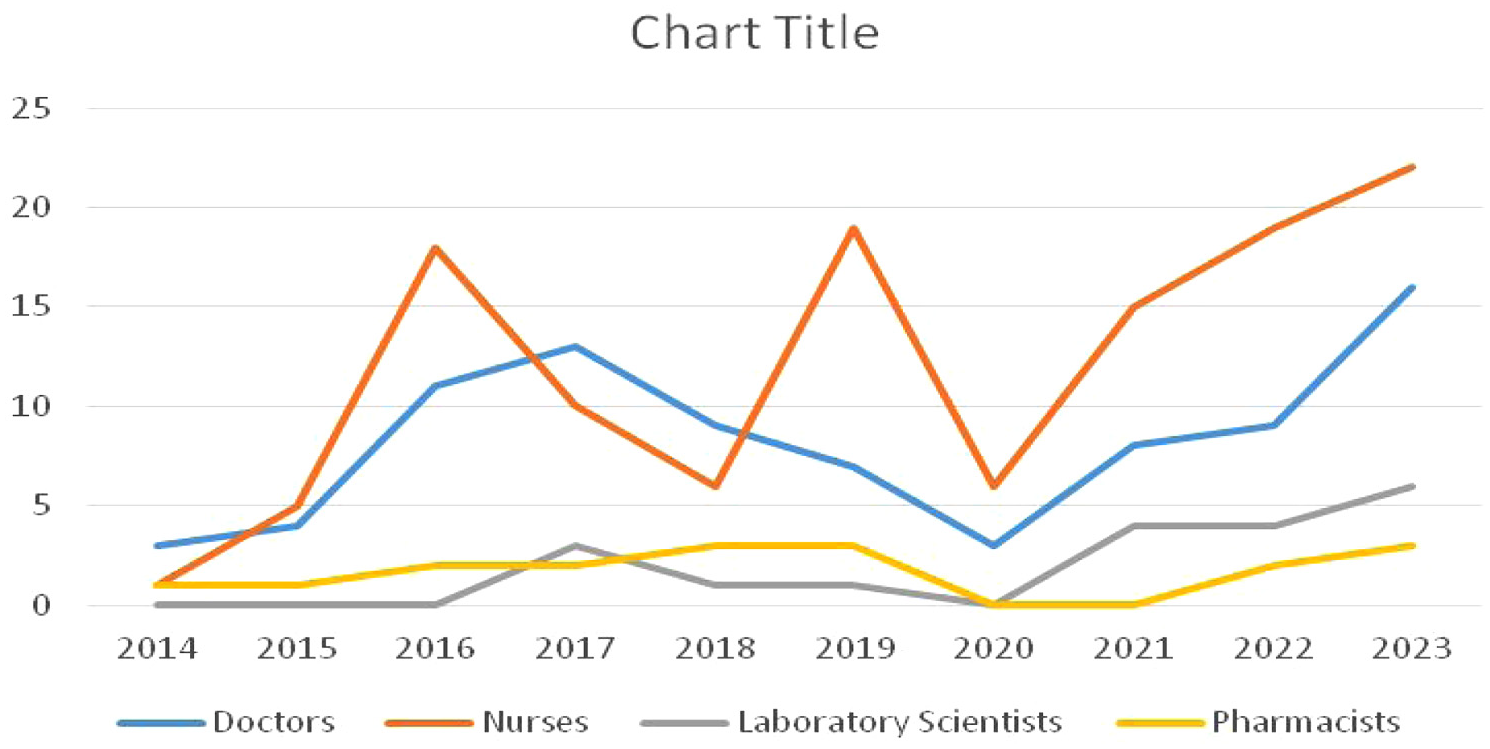
A cluster population representation of the 10-year (2014–2023) human capital flight of health workers (doctors, nurses, laboratory scientists, and pharmacists) from ESUTH.
Hotels in Nigeria, especially in Abuja and Lagos, are now being used by foreign health agents, who occasionally come into Nigeria to conduct recruitment (brain drain) exercises of health workers who emigrate to Saudi Arabia (Akor & Adeuyi, 2021; Deborah, 2021) due to push-pull factors in the health sectors and economies of both countries. Health professionals are leaving Nigerian hospitals and health institutions in drones to the extent that fear grips management. This was revealed by the leadership of the four departments during focused group discussion as one of them stated that “the only health workers they are confident on not leaving or processing their documents to leave are the older colleagues who are 50-55 years and above. The younger ones are leaving our facilities to the extent that it has become a crisis for the management of the hospital.” The situation might continue until the government sits up and addresses the push factors.
Addressing the push factors will help to retain Nigerian health workers at home, instead of trying to pass a bill in the National Assembly, seeking to ban Nigerian doctors from engaging in human capital flight after graduating from medical schools, until they work up to 5 years in Nigerian hospitals (Anuku, 2023). However, due to its untenability based on encroachment on the fundamental right of the health workers and public outcry, the bill has not scaled through. Yet, human capital flight persists in drones, whereas the government has done little or nothing significant to curb or arrest the ugly human capital flight situation in Nigeria.
Conclusion and Recommendations
The health sector in Nigeria is in crisis and needs urgent intervention. Interventions from dilapidated and inadequate infrastructure; increase in funding, improvement of conditions of service to ameliorate the human capital flight of health workers from the health facilities in Nigeria, and the general state of things in the health system. Medical personnel in Nigeria are exiting public hospitals in alarming numbers yearly, and this has turned public hospitals into centers of poor services. Looking at the trend for migration in the mainstream health sector in Nigeria, doctors and nurses are the most affected categories of healthcare providers embarking on human capital flight, respectively. This is followed by the laboratory scientists and pharmacists who are the second category of health workers who embark on human capital flight. Whereas, other categories of staff that are not professionals and skill-oriented personnel working in the hospital such as administrators, security, cleaners, and so on do not significantly embark on human capital flight. Thus, it is the highly trained professionals and experts with specialized and scarce knowledge in the mainstream health sector that Nigeria is losing to foreign lands due to push-pull factors resulting in human capital flight, thereby exposing patients and the entire health system delivery to the risk of poor services. The multiplier effect of human capital flight has a significant negative impact on the critical sectors of the economy thereby hampering national development.
Public hospitals in Nigeria are witnessing gross inadequate healthcare services that have brought about poor treatment and care of patients, high mortality rate, and zero trust and confidence in the country’s health system by the citizens. This ugly trend can, however, still be remedied for it is not yet too late to start a rehabilitation process aimed at aggressive improvement of the push factors in Nigerian healthcare facilities to halt brain drain in the health sector. We suggest that the government should embark on massive development of public hospitals and enhancement of the conditions of service of medical personnel. In that regard, physical infrastructure in public hospitals should be facelifted, and more modern ones constructed, there should be a massive drive in the training and development of medical personnel and provision of state-of-the-art medical equipment in public hospitals. Very importantly, welfare packages and conditions of service for medical personnel should be enhanced to compete with what is obtainable in the Western world. By so doing, the mass exodus of healthcare workers will drastically reduce, and consequently reposition Nigerian hospitals for efficient and effective service delivery.
The challenges of implementing these strategies aimed at restoring public hospitals in Nigeria are mainly the lack of funds and corruption. The government can source funds to revamp the health sector in Nigeria through a similar arrangement with the tertiary education financing in Nigeria; where a body known as the Tertiary Education Trust Fund (TETFund) was created to fund tertiary education by collecting 2% of assessable profits of companies’ tax generated in Nigeria; disbursing the funds; providing infrastructure, teaching and learning materials, manpower training, and sponsorship geared toward developing public tertiary institutions in the country. This TETFund arrangement has worked well and contributed enormously to improving the quality of tertiary education in Nigeria. Therefore, such funding arrangements could be extended to the public health sector or a similar body created to assume responsibility for funding the health sector in Nigeria. Also, the corruption in the health sector among the top personnel should be seriously dealt with through legislation, constant monitoring, and prosecution of offenders to ensure deterrence. Otherwise, the management of public hospitals in Nigeria if left unchecked could loot resources or frustrate whatever measure deployed by the government to revamp public hospitals in Nigeria.
Footnotes
Author Note
No AI was used in writing the manuscript.
Ethical Considerations
No risk to the human participants, thus no ethical approval required.
Consent to Participate
Informed consent was secured from the participants who voluntarily took part in the study as respondents.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Data available on reasonable request from the corresponding author.