
Abstract
The extensive implementation of Electronic Health Record (EHR) systems marks a significant change in how healthcare is delivered, offering the potential for increased efficiency, better communication between healthcare providers, and improved patient care. Nevertheless, there remains a need for a more comprehensive understanding of these systems and their implications on hospital efficiency and patient outcomes. This systematic review critically examines the contribution of EHR systems implementation in improving hospital efficiency and patient outcomes. We searched three electronic medical databases (namely, PubMed, Scopus, and Web of Science core collections) to find potentially relevant studies. Specific search keywords were used to ensure comprehension and relevancy. Specific inclusion and exclusion criteria were applied, and the results of the selected studies were presented. The study followed the Preferred Reporting Items of Systematic Reviews and Meta-analysis (PRISMA-2020). Drawing on a diverse range of studies spanning 29 years, and various geographical locations, this review synthesizes findings from 26 selected studies. The review employs a narrative synthesis approach, addressing the multifaceted implications of EHR implementation across different healthcare contexts. This review provides valuable insights into the evolving landscape of digital health records in healthcare settings, highlighting both the benefits and challenges of EHR systems. The review reveals a complex picture of EHR systems implementations in improving hospital efficiency and patient outcomes. Notable improvements include enhanced clinical workflow, collaboration, quality of care, and patient safety. However, significant technical challenges persist, and the direct impact on patient outcomes remains unclear, emphasizing the need for further research.
Introduction
The widespread adoption of Electronic Health Record (EHR) systems represents a transformative shift in healthcare delivery, promising improved efficiency, enhanced communication among healthcare professionals, and ultimately, better patient outcomes (Mensch, 2023). This technology holds the potential not only to revolutionize data management but also to enhance connection and, ultimately, to elevate hospital efficiency (Pyron & Carter-Templeton, 2019). The initial stirrings of electronic health documentation can be traced to the 1950s and 1960s when healthcare institutions began experimenting with electronic medical records (EMRs; Krishnan & Neuss, 2023). Early EHR systems aimed to digitize patient information, transitioning from paper-based records to a more organized, accessible, and efficient means of storing medical data (Grimson, 2001). The 1970s and 1980s witnessed the gradual transition from EMRs to more comprehensive Health Information Systems (HIS; Berner et al., 2005). These systems extended beyond individual patient records to include broader functionalities such as administrative and billing components (Tanwar et al., 2020). However, the lack of standardization and interoperability hindered widespread adoption.
The 1990s marked a pivotal period with a growing recognition of the need for standardized health information (Hoerbst & Ammenwerth, 2010). Efforts were made to develop interoperable standards, such as the Health Level Seven International (HL7), to facilitate seamless communication between disparate systems (Sahay et al., 2011). Additionally, advancements in networking technologies and the internet laid the groundwork for more integrated and collaborative health information systems (Berner et al., 2005). The 21st century ushered in a digital health revolution, catalyzed by a confluence of technological advancements and a changing regulatory landscape (Grimson, 2001). The term “Electronic Health Record” (EHR) gained prominence as it encapsulated a more comprehensive and interoperable approach to health information management (Lye et al., 2018). In the United States, the “Meaningful Use” program, initiated in 2009 as part of the Health Information Technology for Economic and Clinical Health (HITECH) Act, played a significant role in promoting EHR adoption (Wright et al., 2013). The program offered financial incentives to healthcare providers who demonstrated the meaningful use of certified EHR technology. This incentivized shift accelerated the adoption of EHRs across various healthcare settings (Colicchio et al., 2019).
However, while the “Meaningful Use” program successfully incentivized EHR adoption, it also brought about its share of complications. Some healthcare providers faced challenges in meeting the stringent criteria for meaningful use, leading to concerns about the program’s impact on workflow efficiency and the diversion of resources from patient care (Heisey-Grove et al., 2014). Additionally, the rapid pace of implementation, driven by financial incentives, occasionally resulted in EHR systems that were not optimally tailored to the unique needs of individual healthcare settings, contributing to usability issues and clinician dissatisfaction (Colicchio et al., 2019). Emani et al. (2017) reported that only one-fifth of the physicians in our study believed that the meaningful use of EHR would improve the quality of care, patient-centeredness of care, or the care they provide. The latter part of the 2010s and into the 2020s saw a global momentum toward EHR implementation (Dillard-Wright, 2019). Many countries initiated large-scale projects to digitize healthcare records, improve data sharing, and enhance patient care coordination (Garrety et al., 2016). Interoperability, however, emerged as a persistent challenge, with variations in standards, data formats, and privacy regulations impeding seamless information exchange (Adams et al., 2017).
Presently, EHR systems continue to evolve. Cloud-based solutions offer scalability and flexibility, enabling healthcare providers to access and update patient records securely (Bahga & Madisetti, 2013). Efforts to address interoperability challenges persist, with initiatives to establish common data standards and frameworks (Adams et al., 2017). Additionally, a growing emphasis on patient engagement has led to the development of patient portals and mobile health applications integrated with EHRs, fostering a more collaborative approach to healthcare (Coughlin, 2022). Despite its promises, the realization of EHR benefits has been hindered by numerous challenges, as highlighted by the findings of this systematic review.
The adoption of EHR systems has gained widespread recognition for its ability to streamline hospital operations and deliver better healthcare outcomes for patients. Previous studies highlighted the multifaceted nature of EHR implementation in healthcare settings. These studies examined multiple facets of EHR adoption, including implementation progress, healthcare professionals’ perceptions and attitudes, barriers to successful implementation, and the impact of EHRs on hospital operations, clinical workflows, care quality, provider collaboration, and adherence to best practices. However, there has been no attempt made to systematically present how the EHR system implementation is contributing to the improvement in hospital efficiency and patient outcomes. As countries undertake significant investments in nationwide EHR system rollouts, it is essential to gain a deeper understanding of how these technological innovations can enhance healthcare delivery, ultimately leading to improved hospital operations and better patient outcomes. This systematic review aims to synthesize existing evidence from diverse studies, investigating the multifaceted implications of EHR system implementation across different healthcare contexts. The review was guided by the research questions “Does the implementation of EHRs enhance hospital efficiency and patient outcomes?” What aspects of EHRs contribute to hospital efficiency and patient outcomes? What obstacles and challenges do healthcare organizations face when implementing and integrating EHR systems into their operations?
Materials and Methods
This research followed the Preferred Reporting Items of Systematic Reviews and Meta-analysis (PRISMA-2020) during the preparation of this systematic review (Page et al., 2021). Due to the large heterogeneity between the reported outcomes in the included studies, results were presented narratively.
Search Strategies
For this systematic review, the author conducted a thorough search on major databases like PubMed, Scopus, Cochrane, and Web of Science until December 2023. The author used specific keywords to find relevant results. These keywords included: “Electronic Health Record,”“Electronic Patient Record,”“Electronic Medical Record,”“hospital,”“healthcare,”“clinic,”“efficiency,” and “patient outcomes.” The author also checked previous systematic reviews and manually searched for additional records to ensure comprehensive coverage. To streamline the screening process, all electronic records were exported to the Endnote software, a citation manager, to enhance selection efficiency.
Inclusion and Exclusion Criteria
From the retrieved results from the databases, we selected the studies that were: (1) written in English, (2) published in peer-reviewed journals, (3) full text available online, (4) investigated the efficiency of EHR in elevating hospital functionality or reporting effects on patient outcomes either directly or indirectly, (5) presenting primary original data. We excluded papers that are (1) written in a language other than English, (2) reviews, and (3) grey literature. The eligibility screening process was conducted in two phases: initially, abstracts were reviewed for eligibility, and subsequently, the full-text articles of the abstracts that met the eligibility criteria were obtained and further screened for inclusion.
Study Selection
The author independently screened the titles and abstracts against the exclusion criteria. Full-text manuscripts were screened, and justifications for inclusion or exclusion were confirmed. As there is a certain overlap of reporting among databases, many duplicate articles were dropped. The criteria for screening the abstract were also applied to the full-text screening of the articles. Once the title and abstract were screened, the data from the full text was extracted and double-checked, and key themes were extracted. The key inclusion criteria were: non-English articles, studies not published in peer-reviewed journals, unavailable full-text online, articles not examining the impact of EHR systems on hospital efficiency and/or patient outcomes, and studies lacking primary data. Ultimately, 26 studies met the inclusion criteria and were included in the review.
Data Extraction
The author developed a data abstraction template in Microsoft Excel to extract data. The template included the extraction of information related to the study authors, country, year of publication, study objectives, study methodology, design participants, data collection methods, setting, and study findings. The findings of the studies were arranged according to their contribution to hospital efficiency and patient outcomes. In addition, critical aspects related to EHR implementation were identified, examined, and analyzed, revealing key challenges and obstacles that hinder the successful adoption of EHR systems.
Risk-of-Bias Assessment
The researcher conducted a systematic evaluation of the risk of bias in the studies, using predetermined criteria outlined in Figure 1. Additionally, the researcher assessed the relevance of the study populations and the impact of EHRs on hospital efficiency and patient outcomes. To evaluate the quality of the included studies, the researcher considered various sources of bias, including selection bias, performance bias, detection bias, attrition bias, reporting bias, and publication bias, as well as issues related to imprecision, inconsistency, indirectness, and duplication.

Risk of bias.
Results
Overview of Included Studies
The search results from three medical databases (688 results from PubMed, 525 results from Scopus, and 321 results from Web of Science core collection) yielded a total of 1,525 records. After removing 432 duplicates by Endnote software, 1,093 papers underwent a two-phase screening process, finally yielding the inclusion of 26 studies (as detailed in Figure 2) spanning 29 years of publication from 1994 up until 2023 reflecting the evolving nature of EHR systems.

PRISMA flow diagram detailing the study selection process.
The included studies exhibited variability in the geographical location at which they were conducted as follows: 12 studies were conducted in the USA: Weir et al. (1994), J. Ash et al. (2001), J. S. Ash et al. (2003), Scott et al. (2005), Houser and Johnson (2008), Crowley et al. (2019), Barnes et al. (2022), Penedo et al. (2022), Sangal et al. (2022), Mou et al. (2022), Simon et al. (2013), Ward et al. (2011); 3 studies in The Netherlands: Aarts et al. (2004), Katsma et al. (2007), Veenstra et al. (2022); 2 studies in England: Cresswell et al. (2012), Takian et al. (2012); and 1 study each in the following locations: Albania: Niaksu et al. (2017); France: Boyer et al. (2010); Gorkha, Nepal: Agrawal et al. (2022); Kenya, Rwanda, Uganda, and Mozambique: Were et al. (2021); Kenya: Ali et al. (2023); Lombardy, Northern Italy: Gastaldi et al. (2012); Serbia: Vekić (2022); Southwest Ethiopia: Ngusie et al. (2022); Sweden: Øvretveit et al. (2007). This distribution shows a significant prevalence of studies conducted in the USA, with a range of other countries contributing to the research on EHR implementation and its contribution to improving hospital efficiency and patient outcomes.
The studies involved a wide range of participants including healthcare professionals, hospital administrators, and in some cases, patients. Studies also encompassed different types of hospitals, from teaching to non-teaching and large university medical centers (Table 1). Several studies reported improvements in hospital efficiency, such as better collaboration and workflow due to EHR implementation. The challenges included technical issues, hardware problems, and software design flaws. In some cases, increased workload and rigidity of systems were also noted (Table 2).
The Characteristics of the Studies Included in This Review.

Main Results From the Included Studies.

Note. POE = physician order entry; CPOE = computerized physician order entry; CIS = clinical information system; EMR = electronic medical record; ED = Emergency Department; EGS = Emergency General Surgery.
Study Objectives and Design
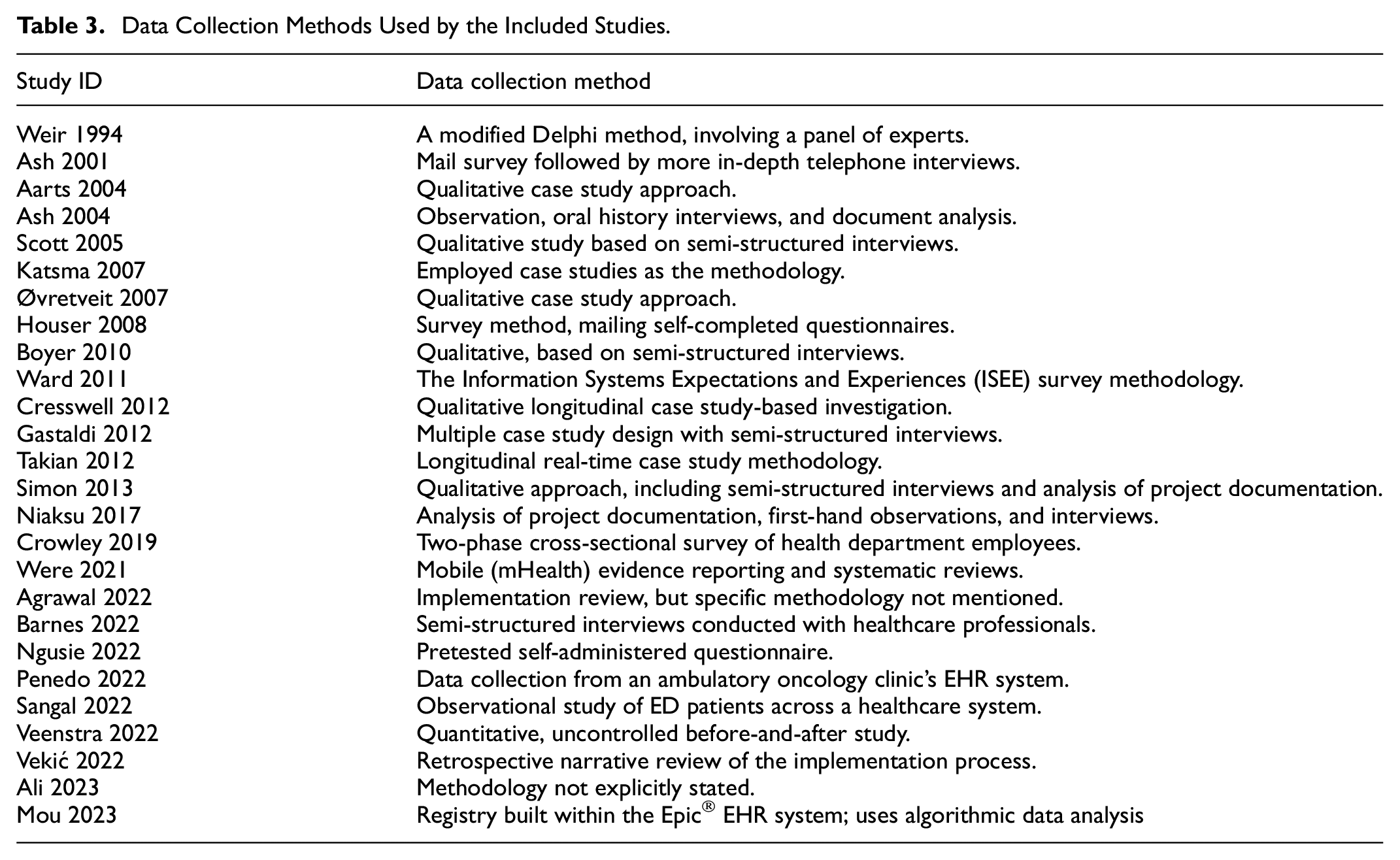
The objectives and designs of the studies on EHR system implementation varied widely, reflecting diverse approaches to understanding EHR systems’ role in improving hospital efficiency and patient outcomes. For example, the study by Weir et al. (1994) aimed to identify variables associated with the successful adoption of integrated order entry systems, using a modified Delphi method with questionnaires across six hospitals. J. Ash et al. (2001) investigated Computerized Physician Order Entry (POE) through a series of studies, focusing on its implementation, usage, and impacts, employing a mail survey and qualitative multi-center studies.
Houser and Johnson (2008) aimed to explore healthcare professionals’ perceptions of EHR utility in a single hospital, using a questionnaire-based survey. Crowley et al. (2019) assessed the impact of EHR on healthcare quality and patient safety, employing a mixed methods approach with a pre-post-intervention study. Barnes et al. (2022) focused on evaluating the effectiveness of EHR systems in improving healthcare delivery and patient outcomes using a quantitative approach with data analysis. The variability in the study designs and data collection methods is summarized in Table 3.
Data Collection Methods Used by the Included Studies.
EHR Implementation and Hospital Efficiency
The role of EHR system implementation in improving hospital efficiency encompasses a range of outcomes across various studies. In Weir et al. (1994) factors such as supportive administration, direct physician involvement, and adequate hardware were identified as facilitators for successful hospital operations. J. Ash et al. (2001) highlighted that clinicians saw Physician Order Entry (POE) systems as more advantageous for hospital administrators than for themselves, citing issues with response time and total time spent on order entry. Additionally, organizational, and personal aspects such as varying perceptions among clinicians, administrators, and IT staff about POE, trust, leadership style, and the concern of additional time spent on POE were brought to light (Veenstra et al., 2022).
Aarts et al. (2004) found significant contributions to hospital efficiency from the implementation of the Computerized Physician Order Entry (CPOE) system, including improvements in medication safety, reduction in medication errors, and increased efficiency in medication ordering and administration. J. Ash et al. (2001) found that the POE system led to improved collaboration and communication among healthcare professionals, as well as shifts in power dynamics and adjustments in clinical practices. These changes underscored the importance of organizational culture, trust, and active clinician engagement in successfully adopting new technology. Cresswell et al. (2012) discussed the impact of a top-down implementation that limited customization, leading to increased workloads and the necessity of workarounds. Gastaldi et al. (2012) found that implementing the EMR system enhanced knowledge asset dynamics, leading to improved performance in cost rationalization and quality improvement. Takian et al. (2012) reported positive changes in work practices and patient care due to EHR systems but did not specify how these changes affected overall hospital efficiency. Simon et al. (2013) emphasized the importance of governance, preparation, support, health professionals’ perceptions, and consequences for the successful implementation of EHR system. Finally, Niaksu et al. (2017) highlighted improved patient demographic data collection and flow control and minimizing paperwork for patient registration.
Effects of EHR on Patient Outcomes
The contribution of EHR implementation in improving patient outcomes shows varied effects across different healthcare settings. In the study by Were et al. (2021) mUzima, a mobile health application, was noted to improve access to health data and quality of care, demonstrating effectiveness across multiple countries and care domains. Vekić (2022) reported that the implementation of EHR in Serbia led to improvements in healthcare services, as evidenced by Serbia’s improved ranking in the European Healthcare Consumer Index, and positively impacted most segments of the Serbian healthcare system. Penedo et al. (2022) examined the implementation process of EHRs, suggesting that improved assessment of patient needs and symptoms could have a positive indirect impact on patient outcomes. Ali et al. (2023) highlighted that EHRs help provide comprehensive and safe care to patients and improve the provider experience. These findings from recent studies indicate that while EHR systems have the potential to improve patient care and healthcare service quality, the direct impact of EHR system implementation on patient outcomes is often not the primary focus of these studies. Instead, they tend to highlight improvements in healthcare processes and provider experiences, which can indirectly influence patient outcomes. This shows that future studies on this topic need to consider the direct effects on patient care as the primary outcome through which they measure the effectiveness of EHRs.
Challenges and Drawbacks of EHR Systems
Past studies have extensively discussed the challenges, and issues related to EHRs providing valuable insights for researchers, scholars, and healthcare professionals. A significant concern is the limited digitalization of health data due to the unavailability of EHRs, which can be addressed by leveraging information communication technologies (ICT) in healthcare organizations (Boyer et al., 2010). Other challenges include inadequate training post-EHR implementation (Crowley et al., 2019) high implementation costs, and technical issues such as power supply, networking, and software customization (Agrawal et al., 2022; Were et al., 2021). Physicians face issues related to autonomy in using EHR software for decision-making (Barnes et al., 2022). Furthermore, healthcare workforce motivation, independence, and work nature can be impacted (Veenstra et al., 2022).
Organizational challenges include employee resistance, lack of motivation, and limited flexibility in adopting new changes (Vekić, 2022). Additional problems include inexperienced staff, limited resources, planning concerns, and user errors (Ali et al., 2023).
These studies collectively underscore the multifaceted challenges of EHR systems, ranging from technical and usability issues to organizational, cultural, and workflow-related hurdles, underscoring the complexity of implementing and integrating these systems effectively in healthcare settings.
Discussion
The main objective of this review is to critically examine the contribution of EHR systems implementation in improving hospital efficiency and patient outcomes. Healthcare organizations worldwide have recognized the importance of EHRs, leading to increased adoption and implementation (Alzghaibi et al., 2023). EHRs provide accurate and up-to-date information, enabling healthcare professionals to make informed decisions and improve patient care. The use of EHRs enhances physician efficiency, hospital efficiency, and patient satisfaction. It is also recognized that EHRs help address common challenges like overcrowding and time constraints by providing accurate information for decision-making (Mughal et al., 2024) reducing costs and enhancing financial performance (Nair et al., 2024). Overall, the adoption of EHRs can increase the value of healthcare organizations (Kundi, 2023).
This systematic review reveals a complex picture of EHR system implementation in improving efficiency in healthcare settings. EHR systems have shown promise in improving hospital efficiency through enhanced data management, administration, and workflows. Studies A. A. M. Alharbi et al. (2023) consistently highlight distinct improvements in hospital operations, including workflow management, collaborative practices, medication order accuracy, and access to patient information. These enhancements facilitate efficient clinical decision-making and promote care coordination among healthcare professionals across various specialties and settings.
Implementation of EHRs can lead to cost reduction by streamlining administrative processes and decreasing operational costs. Few studies (Mughal, 2024) show that EHRs save healthcare providers time and effort, while others (D. N. Alharbi & Kundi, 2024) demonstrate that EHR adoption helps hospitals reduce expenses and increase revenue. By automating administrative tasks, EHRs enable healthcare providers to focus more on patient care. These findings are aligned with previous reviews (Ghaffar, 2024) that identified improvements in administrative efficiency and data accessibility. Studies, such as Lee et al. (2022) demonstrate that hospitals implementing EHRs outperform those that do not, showing positive effects on efficiency, profitability, and service quality. However, earlier studies may have been less conclusive due to the early stages of EHR implementation and varying technological sophistication.
This review highlights the uncertain impact of EHRs on patient outcomes. While some studies suggest improvements in patient care, patient safety, service quality, and satisfaction, other studies focus on healthcare processes, such as clinical workflows and provider-patient communication, rather than direct patient outcomes. These findings are consistent with the findings of a study (Subbe et al., 2021) which found that EHRs often report process measures rather than patient-level safety outcomes, suggesting a limited and unclear impact of EHRs on safety outcomes. Few studies (Vekić, 2022) suggest that EHR implementation improves care quality by providing healthcare professionals with immediate access to comprehensive patient data. This facilitates accurate diagnostic procedures, informed decision-making, reduced medical errors, and medication safety (Menachemi & Collum, 2011). Reviews by Tabche et al. (2023), Gatiti et al. (2021), and Campanella et al. (2016) confirm that EHRs improve doctor-patient relationships, patient safety, and healthcare quality. EHRs also enable timely, equitable, and patient-centered care. However, a qualitative analysis by Upadhyay and Hu (2022) revealed mixed results, with nurses reporting improved efficiency, while other healthcare professionals found EHRs time-consuming. Similar findings were also revealed by a study in Saudi Arabia (Jha et al., 2009).
The review reveals that the benefits of EHRs are often offset by significant challenges. Recurring issues include technical problems, integration complexities, increased workload, and escalating implementation costs. Additional challenges encompass low staff perception of EHR usefulness, concerns about information sharing and confidentiality, hardware issues, inadequate training, and resistance from physicians and staff. Few studies (Weir et al., 1994) highlight specific challenges, including software issues, integration difficulties, and user dissatisfaction. Other studies J. Ash et al. (2001) highlighted the resistance from physicians and other staff including cultural resistance becomes a challenge to EHR implementation. These challenges can impede EHR’s potential, affect hospital efficiency, and impact healthcare provider morale and productivity. To maximize EHR benefits, careful planning, adequate staff training, and thoughtful integration strategies are essential.
The ambiguity in the findings of existing studies on the impact of EHRs on hospital efficiency and patient outcomes highlights the complexity of this issue. Furthermore, the challenges of implementing EHRs in various healthcare settings underscore the necessity for additional investigation. Future research should focus on establishing a clearer link between EHR usage and hospital efficiency and patient outcomes, as well as identifying strategies to overcome the challenges faced by healthcare professionals in adopting these systems. This may involve more targeted studies on healthcare provider user experience, EHR effectiveness in different clinical contexts, and the long-term advantages and disadvantages of EHR implementation on patient care and hospital operations.
The review also emphasizes the importance of considering the unique contexts and needs of different healthcare settings when implementing EHR systems. Factors such as organizational culture, healthcare provider attitudes, and existing infrastructure play a crucial role in determining the success of EHR implementation. Furthermore, the rapid evolution of technology and healthcare regulations requires EHR systems to be highly adaptable and flexible, enabling them to respond effectively to the dynamic needs of healthcare delivery.
This review has several strengths, including its diverse range of settings and participants, methodological rigor, and focus on practical outcomes. However, it also has some limitations: Firstly, the studies examined had varying levels of focus and depth, with some concentrating on the implementation process rather than patient outcomes. Secondly, the reliance on self-reported data in many studies introduces potential biases and subjective interpretations, particularly in studies exploring healthcare professionals’ perceptions. Thirdly, the lack of longitudinal data limits our understanding of the long-term impact of EHR implementation on hospital efficiency and patient outcomes. Lastly, the findings may not be generalizable to other contexts due to regional or setting-specific differences, which restricts the applicability of the results.
Conclusion
The systematic review paints a multifaceted and intricate picture of the impact of EHR system implementation in improving hospital efficiency, and patient outcomes. While there are notable improvements in clinical workflow, streamlined administrative process, reducing the burden of paperwork, health professional collaboration, cost savings, and access to patient information significant challenges persist, especially in technical and software aspects. While EHRs present significant opportunities for improving hospital efficiency, their successful implementation requires addressing various challenges at institutional, technological, and human resources levels. Although EHR systems have the potential to enhance patient care, safety, and healthcare quality, their direct impact on patient outcomes is still uncertain and requires further investigation. Most studies tend to highlight improvements in healthcare processes, patient safety, service quality, and provider experiences, which can indirectly benefit patient outcomes. Despite the benefits of EHRs highlighted in the reviewed studies, there are still significant gaps in understanding their impact on hospital efficiency. Targeted research is needed to address these gaps and optimize EHR use. Future studies should prioritize investigating the direct impact of EHRs on patient outcomes and explore how EHR features can be leveraged to empower patients and promote their involvement in care processes.
Footnotes
Acknowledgements
The author would like to express his sincere gratitude to the reviewers and editor for their valuable suggestions. Additionally, the Researcher would like to thank the Deanship of Graduate Studies and Scientific Research at Qassim University for financial support (QU-APC-2025).
Ethical Considerations
Ethical approval was not required as the study did not involve human participants.
Consent to Participate
This article does not contain any studies with human or animal participants. There are no human participants in this article and informed consent is not required.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
All data generated or analyzed during this study are included in this published article and its supplementary materials.