
Abstract
Electronic health record (EHR) systems have become a basic need in most health care facilities worldwide. However, little can be said about the developing nations’ use of it. Nevertheless, Ghana is one of the very few countries in Africa to start using EHRs. Nursing is a field that has been substantially influenced by the use of hospital electronic information management systems (HEIMS). More importantly, the successful implementation of any mHealth and EHRs critically depends on user acceptance. Therefore, as nurses in Ghana work at the frontline of the health care system in the country with access to vital records about the patients, it is important to assess what motivates them to use the system. This study applied a non-experimental survey design. An electronic platform questionnaire on smartphones was used to collect data on 660 nurses. Statistically, AMOS structural equation modeling (SEM) was employed to examine the research model. “Behavioral intention” (BI) to HEIMS use was significantly predicted by effort expectancy (EE) (p <.001). Notably, EE had an effect on BI, which explains the 37% variance in the intention of nurses to use HEIMS. Likewise, use behavior (UB) of HEIMS was also significantly predicted by performance expectancy (PE) (R2 = .25), EE (R2 = .311), and BI (R2 = .397), and all explained 46% of the variance in nurses’ acceptance of HEIMS. Nurses’ acceptance of HEIMS was significantly predicted by PE, EE, and BI. Based on these findings, hospital administrators should put measures in place that will boost the nurses’ confidence in using HEIMS as well as endeavor to adopt and implement a very user-friendly system.
Keywords
Introduction
The adoption of electronic health records (EHR) systems has become a basic necessity in most health care facilities worldwide (Ancker et al., 2017; Bani-Issa et al., 2016; Hemsley et al., 2018). Yet, not much can be said about the developing nations’ use of it. However, Ghana is one of the very few countries in Africa to have started using EHR systems. EHR systems are meant to guide and assist clinical and nursing group of workers in their day-to-day work via the processing of patients’ data electronically. These electronic systems have the possibility to enhance the accuracy and quality of patient information and minimize the cost of accessing medical care (Hemsley et al., 2018; Vitari & Ologeanu-Taddei, 2018). EHRs have been predicted to exhibit an exceptional influence on health care services in the near future. Thus, they are considered as essential technological platforms for accessing health care presently and in the years ahead (Alquraini et al., 2007; Hemsley et al., 2018).
Though, the services provided by nurses, such as; diagnosing, planning, implementation, and assessment of the care of the affected person, the documentation in the EHRs report ought to mirror these procedures (Mervat & Mary, 2016). Therefore, the Health Information Management (HIM) branch frequently collaborates with the nursing unit in collecting, analyzing, and disseminating data, creating reports and addressing problems associated with the health record of patients. Undoubtedly, in this modern era, the use of “hospital electronic information management systems (HEIMS)” (Zhou et al., 2019) have had great influence on nursing profession. Hence, some literacy in computing and information technology (IT) knowledge have become a career prerequisite in many health care institutions and medical care facilities especially in Ghana.
Ghana as a developing country is doing well in introducing HEIMS in some major government hospitals in the country. The previous paper (Zhou et al., 2019) we published was based on the effect of “social influence and facilitation conditions that support nurses’ acceptance of HEIMS in Ghana” (Zhou et al., 2019). However, this particular paper focuses on the predictive ability of performance expectancy (PE) and effort expectancy (EE) concerning nurses’ readiness in accepting to use the HEIMS based on the Unified Theory of Acceptance and Use of Technology (UTAUT) model (Venkatesh et al., 2003). Research studies reports indicate that some health care professionals (such as nurses) dislike IT use in their health care centers (Alquraini et al., 2007). More importantly, the implementation success of any EHRs and hospital IT critically rely on users’ willingness to accept and use (Vélez et al., 2014). Therefore, as nurses in Ghana are the main frontline workers in the various hospitals (N. Mensah et al., 2015), it is very important to assess what motivates them and their readiness to use the HEIMS. In this study, all forms of health technology (i.e., EHRs, medical health records (MHRs), and electronic information management) platforms were termed as HEIMS.
The UTAUT Model and Hypotheses Development
The UTAUT model was validated appropriately to provide a unified theoretical groundwork from which to promote research on information systems (IS) or adoption of IT and dissemination (Venkatesh et al., 2003). The UTAUT model definition and validation was founded on the fact that quite a lot of the concepts of the current theories were logically comparable.
The main aim of this article is to assess the readiness of the nurses in Ghana to accept and use HEIMS through the consideration of two main constructs of the UTAUT model: (a) their PE and (b) their EE. The original version of the UTAUT model is depicted in Figure 1 (the figure shows the main constructs of the original UTAUT model; Venkatesh et al., 2003). The hypotheses of this study are as follows.
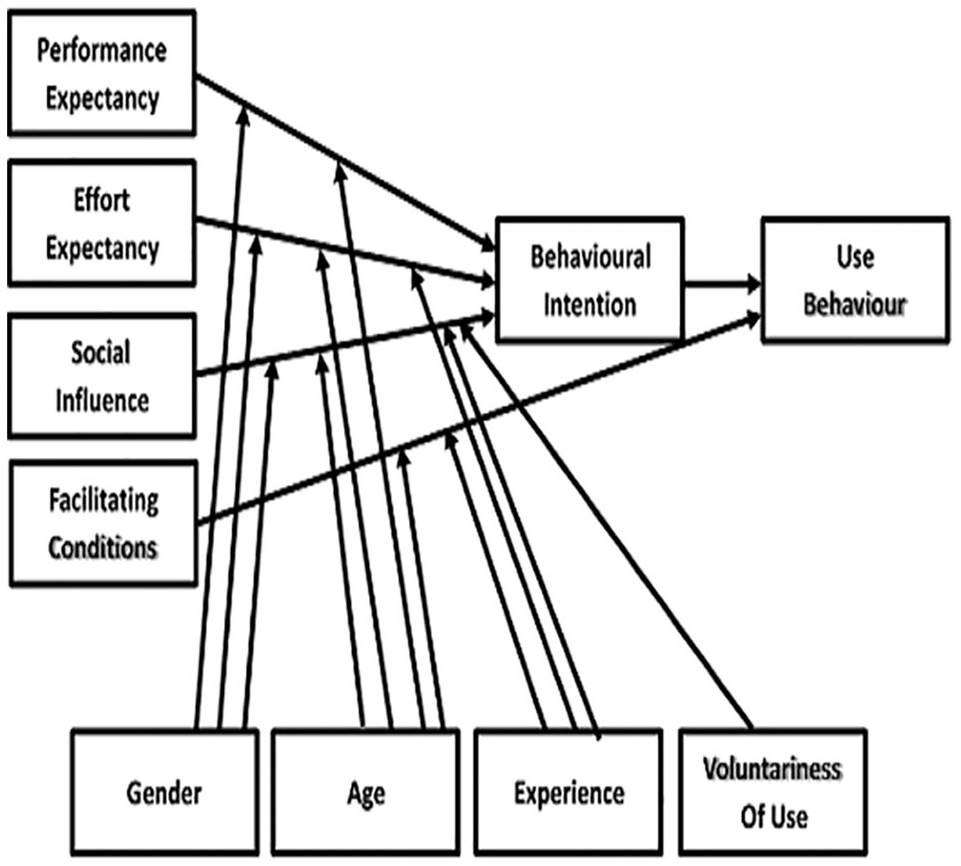
The original UTAUT model.
PE
The PE refers to the extent to which a person believes that the use of the IT system will add up the knowledge to the improvement of his or her work performance. The five different models related to PE have perceived usefulness (technology acceptance model (TAM) and combined TAM and theory of planned behavior (C-TAM-TBP), extrinsic motivation, motivational model (MM), job fitness model of PC utilization (MPCU), comparative advantage innovation diffusion theory (IDT), and result expectation social cognitive theory (SCT) (Venkatesh et al., 2003). The extent to which medical health care professionals (i.e., nurses) are convinced that using hospital information systems (HIS) may help in achieving the expected quality services in taking care of patients and might have an influence on their readiness and intentions to adopt and use HEIMS. Previous studies have shown that PE is a significant predictor of the behavioral intention (BI) to use other technologies (Bawack & Kala Kamdjoug, 2018; Handayani et al., 2017; I. K. Mensah, 2019; Vollmer et al., 2016). However, not much studies have assessed whether PE predicts the use of HEIMS by nurses in developing countries, such as Ghana. Subsequently, hypotheses 1 and 2 were proposed as follows:
EE
The EE refers to the degree of ease associated with the use of the system. Notably, three main variables in the existing model capture the perceptions of expected effort: perceived ease of use (TAM/TAM2), complexity (MPCU), and ease of use (IDT). Pertinently, EE is considered in terms of the user understanding that using new technology will be easy to use (Venkatesh et al., 2003). The way wherein new technology services are adopted and used depends to a large extent on the ability of users (i.e., nurses) to navigate and use such technologies, without any trouble or challenge that may affect their readiness and intentions to use them. Previous studies have demonstrated that EE has a positive significant impact on the BI to use new technologies (Bawack & Kala Kamdjoug, 2018; Nadri et al., 2018; Sharifian et al., 2014; Strudwick et al., 2015; Vollmer et al., 2016). Accordingly, hypotheses H3 and H4 were proposed:
BI
It is a measure of the strength of one’s intention to perform a specified behavior. But, the origin of BI was from the theory of reasoned action (TRA) (Fishbein & Ajzen, 1975). However, BI use as applied to the intention of computer IT usage was initially introduced by Davis in 1989 through his technology acceptance model (TAM). In fact, this model asserts that BI to use ICT is directly and strongly linked to the actual ICT usage. As a matter of fact, behavior and intentions relationship is well documented in the technology acceptance literature. Therefore, it is conclusive and acceptable to be applied in the health care contexts. Hence, hypothesis 5 is proposed as follows:
Figure 2 represents the proposed research model adopted from the UTAUT model.
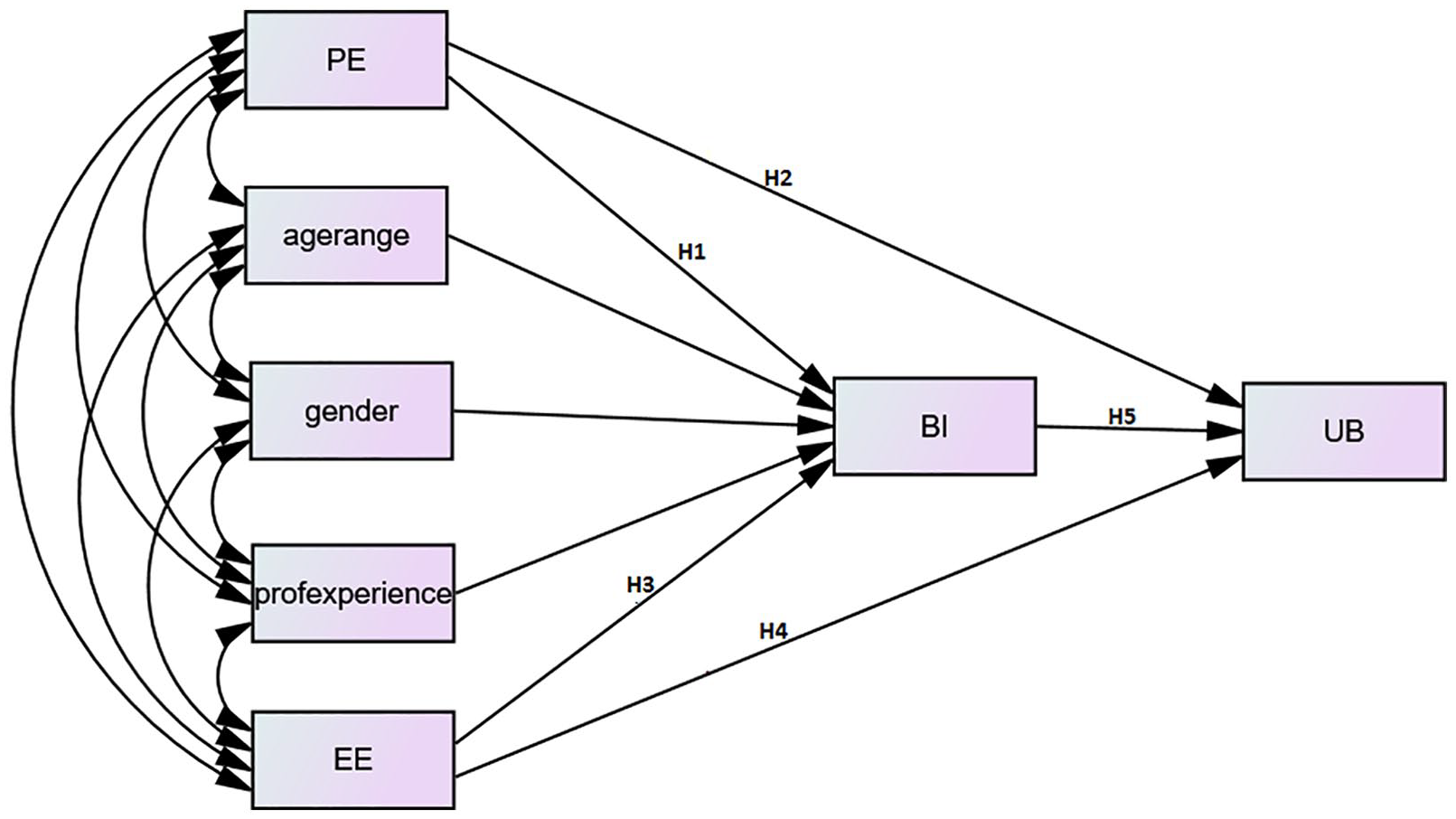
Conceptual model.
Method
Research Design, Population, Settings, and Sampling
A descriptive cross-sectional study design was adopted in conducting this study. The design of the study and data collection were carried out during the period of January 15 to February 28, 2019. The survey design was applied to evaluate the nurses’ readiness to use HEIMS. Primary data through survey from nurses in five major government hospitals in Ghana was the main source of data for this study. These hospitals were the main health facilities where HEIMS was being applied for patient care. The nurses who were willing to participate from the aforementioned medical facilities were selected. Selection of respondents (nurses) was done through simple random sampling method. However, a purposive sampling approach was first used in selecting five public hospitals comprising two regional and three teaching hospitals that use HEIMS in Ghana. In all, 660 nurses were selected comprising 404 females and 256 males.
Research Tool for Data Collection
The tool for data collection was a Likert-type scale rating type of questionnaire. The questionnaire was converted to an electronic type using a mobile application called open data kit (ODK) (Zhou et al., 2019). In fact, previous research studies have demonstrated that the UTAUT model Likert-type scale type of data collection tool has been good enough to be used in cross-cultural surveys outside the country of origin (Venkatesh & Zhang, 2010). Hence, the original English version questionnaire from the UTAUT model was modified and adopted to fit the objectives of this study (Guillemin et al., 1993): The related items for the measurement of the constructs in the questionnaire were established using a 1 to 7-point Likert rating scale which ranged from “Strongly disagree (1)” to “Strongly agree (7)” for SI, FC and BI. Likewise, usage behavior was evaluated through a 1 to 8-point Likert rating scale that ranged from “Have not used (1)” to “Almost every day (8).” Notably, extra information like age, gender, experience and voluntariness of use was obtained from the respondents using the questionnaire to serve as the moderators. (Zhou et al., 2019)
Data Collection and Statistical Analysis
The collection of data was done using an electronic questionnaire with the measurement items based on the original English version of the UTAUT model constructs validated using Likert-type rating scale (Venkatesh et al., 2003). Smart mobile phones and tablets were used in obtaining the electronic data from the nurses. The structured questionnaire was coded with ODK mobile phone application (Wright et al., 2015). Pretesting of the electronic questionnaire was done several times. The feedback from the pretesting helped the authors to fine-tune the questionnaire to suit this study settings before sending them out for the main study data collection. Preliminary analysis of reliability, accuracy, and validity of the modified survey questions were tested. In fact, all the respondents (the nurses) were contacted at the time of their working shifts (morning and afternoon). However, they were engaged either through a mobile phone (for night shifts) or verbally to take part in this study. But the electronic questionnaire was shared with the nurses through smart mobile devices personally by the authors and other supporting data collectors. The respondents were briefed on how to answer and submit the electronic questionnaire. All the questionnaires were automatically delivered to our ODK Google aggregate server (www.odkproject-1333.appspot.com) upon completion. The questions were written in simple understandable English language. Hence, it took about a minimum of 4 and maximum 10 min for respondent to complete a questionnaire. The study employed SPSS and IBM AMOS structural equation modeling (SEM) (version 22.0) to analyze the data collected. The assessment of the “internal consistency reliability” (ICR) of parameters such as “Cronbach’s alpha” (CA) was applied to examine the one-dimensionality of a group of the survey questionnaire measurements. Moreover, additional analysis such as “average variance extracted” (AVE) and “Composite reliability” (CR) for the individual construct provides coefficients which confirmed the reliability of the survey (Abdalla Mohammed & Muhammed Pandhiani, 2017). In this regard, 0.70, 0.70, and 0.50 were estimated as the respective recommended values (Bagozzi, 1986). The linear correlation coefficient (R2) of each dependent construct in the model was generated to assess whether the model fit well to the hypothesized relationship (Zhou et al., 2019).
Reliability and validity of measurement
The Cronbach’s Alpha for testing the overall reliability for the measurement items was 0.949, while the Kaiser-Meyer-Olkin Measure (KMO) of sampling adequacy was 0.928. The individual constructs validity and reliability testing results are shown in Table 3 and narrated in the results section (Lulin et al., 2020; Zhou et al., 2019).
Results
Demographic Statistics
An initial survey targeted 700 participants; however, 660 respondents availed themselves to answer and submitted their questionnaire representing a response rate of 94.3%. This was enough and representation of the entire population is based on the sample size calculation. Although participation was completely voluntary, the innovative use of smart mobile devices ensured easy and fast answering of the questionnaire, which resulted in the high response rate. Remarkably, most of the nurses in Ghana are females and so it was not surprised that 61.2% of the participants were female nurses. A summary of the background information of the respondents is indicated in Table 1. The majority of the respondents were staff nurses (58.4%). All the respondents had at least a diploma degree with most (52.4%) of them between the ages of 20 and 30 years. Notably, almost all of the respondents have had at least 1 year experience of using HEIMS in Ghana (Zhou et al., 2019).
Demographic Characteristics of Respondents.

Source. Zhou et al. (2019).
Note. HEIMS = hospital electronic information management systems; LHIMS = Lightwave Health Information Management Systems; HAMS = Hospital Administration Management Systems.
The Measurement Models
The measurement items of the model are composed of nine observed variables, namely PE, EE, attitude toward the use of technology (ATUT), SI, self-efficacy (SE), FC, computer anxiety (ANX), BI, and UB with 34 items in totality. The overall goodness of fit was assessed via some model fit measures. The results of the goodness-of-fit statistics are presented in Table 5. The standard measurements of goodness-of-fit index (GFI), comparative fit index (CFI), normed fit index (NFI), non-normed fit index (NNFI), and incremental fit index (IFI) were greater than or equal to the proposed 0.9 benchmarks (Schuenemeyer, 1989). In this regard, the instrument’s psychometric properties were evaluated regarding the “discriminant validity” (DV), “convergent validity” (CV), and reliability. The findings of the items’ loadings, means, and standard deviation statistics are depicted in Table 2. Likewise, Table 3 displays the results of mean, standard deviations, variances, CA, CR, AVE, and DV as well as the Kaiser–Meyer–Olkin (KMO) measure of the sampling adequacy of the constructs. The CA for all the constructs was above the 0.7 thresholds ranging from 0.709 to 0.980. The assessment of the inner consistency of the measurement model was through the calculation of the CR of the constructs which ranged between 0.824 and 0.985 but exceeded the cut-off of 0.70 as recommended elsewhere by Chen and Hsiao (2012). In the current report, the construct validity was measured in terms of the usage of AVE and DV. Fornell and Larcker (1981) proposed that the common AVE number exceeds 0.5 and is larger than every square correlation with recommended sufficient CV and DV. From Table 3, it can be observed that the AVE of the measurements ranged from 0.546 to 0.944, which surpassed the endorsed value (AVE > 0.5) (Fornell & Larcker, 1981). This indicated a remarkable CV which is considered as one key criterion for acceptable DV (Chen & Hsiao, 2012). This study discovered that all AVE values were larger than every square correlation, demonstrating the exact DV as indicated in Table 3 (the square root of AVE) as proven with the aid of Chen and Hsiao (2012). The data obtained in this study had adequate CA, CR, and DV. The sampling adequacy (KMO) of all the constructs was also more than 0.5 (Zhou et al., 2019).
Result of Items Loadings and Descriptive Statistics of Constructs.
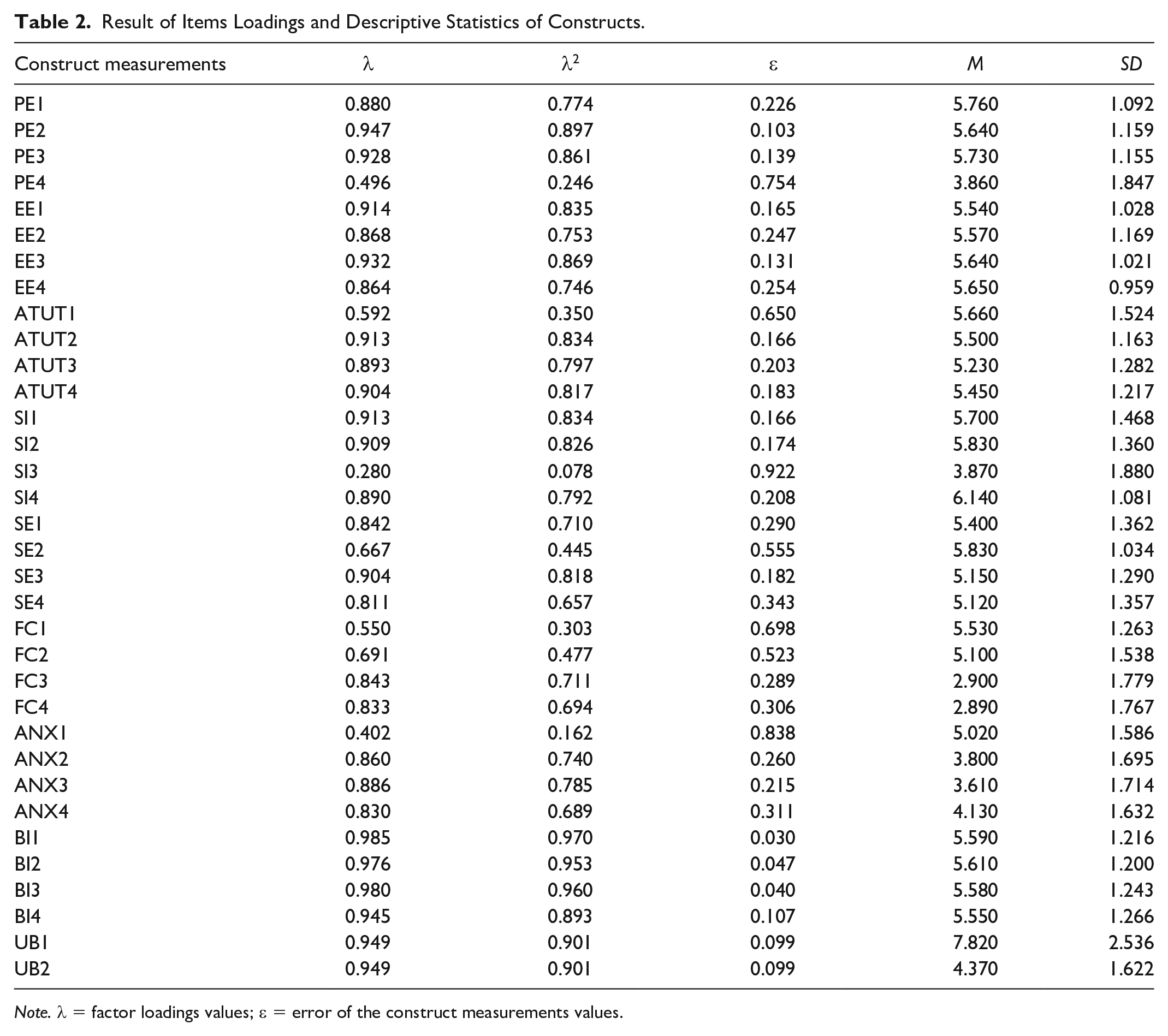
Note. λ = factor loadings values; ε = error of the construct measurements values.
Measurement Model: Results of AVE (Convergent Validity), CR, CA (Reliability Testing), and KMO (Sampling Adequacy Test).
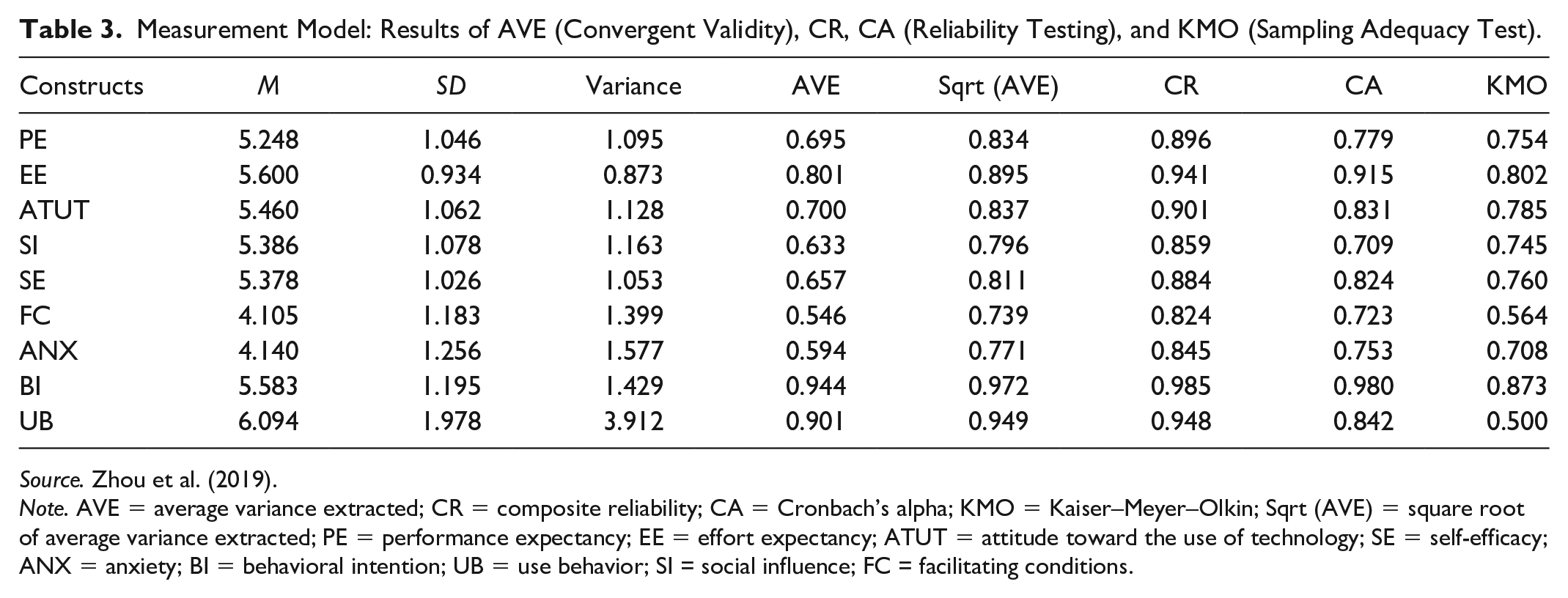
Source. Zhou et al. (2019).
Note. AVE = average variance extracted; CR = composite reliability; CA = Cronbach’s alpha; KMO = Kaiser–Meyer–Olkin; Sqrt (AVE) = square root of average variance extracted; PE = performance expectancy; EE = effort expectancy; ATUT = attitude toward the use of technology; SE = self-efficacy; ANX = anxiety; BI = behavioral intention; UB = use behavior; SI = social influence; FC = facilitating conditions.
Structural Model: Hypothesis Testing Results.

Note. Only one out of the five hypothesis result was rejected. R2 = square root of correlation coefficients of the intercepts; SE = standard error; CR = critical ratio; BI = behavioral intention; PE = performance expectancy; UB = use behavior; EE = effort expectancy.
p < .001.
Partial Correlation Matrix of Constructs.

Note. The bold values on the leading diagonal show the square root of the average variance extracted shared by the constructs and their measures while the non-diagonal values are the correlation coefficients between the constructs. PE = performance expectancy; EE = effort expectancy; BI = behavioral intention; UB = use behavior.
p < .01.
The Structural Model
After examining the research model through the application of SEM procedures for this study, three latent variables (PE, EE, and BI) were tested to evaluate their influence on the actual use (UB) of HEIMS. The construct (PE) was examined with the effect of moderators (age and gender). The analysis result showed that PE had an explained variance of 25.7% (R2 = .257) of the actual use of HEIMS (Table 6). The construct (EE) was also moderated by age, gender, and professional experience. The analysis result of EE had an explained variance of 37% (R2 = .37) of the actual use of HEIMS (Table 6). The research model constructs (PE and EE) entirely recorded an explained variance of 37.2% of BI to use HEIMS (Table 6). The constructs (PE and EE) explained 25% and 31.1% of the variance, respectively, in terms of UB of HEIMS (Table 6). The intentions of the nurses (BI) explained 39.7% of the variance of UB of HEIMS (Table 6). The total explained variance of the three independent variables (PE, EE, and BI) on the dependent variable (UB) of HEIMS was 46% (Table 6). The standardized path coefficients are depicted in Figure 3. These coefficient values indicate the significant structural relationship between the tested parameters. The data showed that PE did not significantly influence (p = .10) BI to use HEIMS; hence, the null hypothesis was accepted, rejecting the alternative hypothesis (H1) (Table 4). Inversely, hypothesis (H2) was accepted because the construct (PE) directly and significantly influence the UB of HEIMS (p < .001), thereby rejecting the null hypothesis (Table 4). Moreover, H3 and H4 were all accepted. The construct (EE) had a significant influence on the intentions of the nurses to use HEIMS (p < .001) and also significantly influenced UB of HEIMS (p < .001). Finally, H5 was also accepted because the influence of BI on UB of HEIMS was significant (p <.001) (Table 4).
Explained Variance of Constructs.

Note. R2 is the amount of variance in the dependent variable (DV) that is accounted for or explained by the independent variable(s) (IV). PE = performance expectancy; BI = behavioral intention; EE = effort expectancy; UB = use behavior; NA = not applicable.
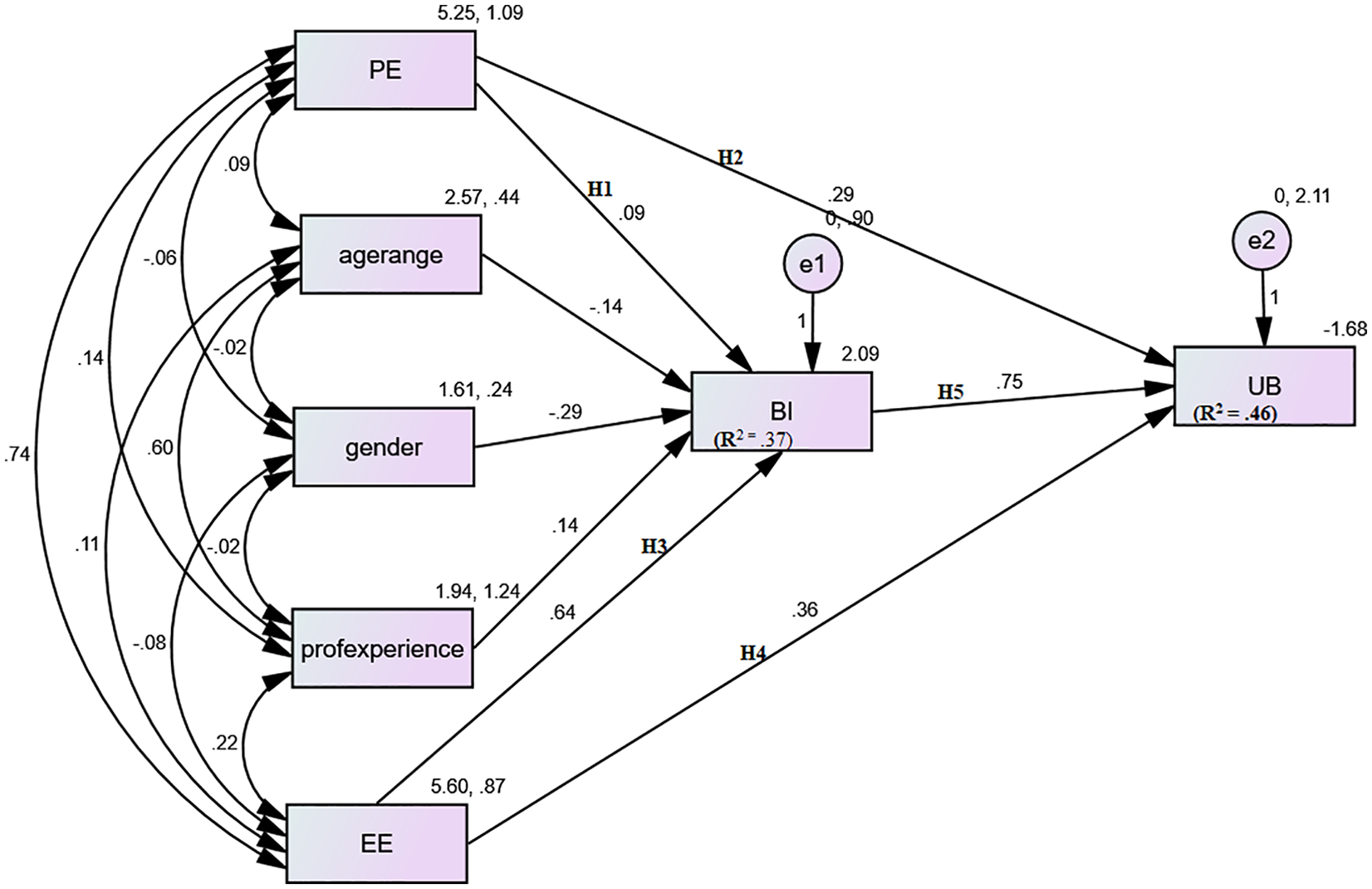
Standardized values of structural model.
Discussion
The study key findings are summarized as follows: (a) The direct influence of PE (moderated by age and gender) on the UB of nurses to accept and use HEIMS was significant (Bawack & Kala Kamdjoug, 2018; Handayani et al., 2017; I. K. Mensah et al., 2019; Vollmer et al., 2016). (b) The influence of the construct (EE) also moderated by age, gender, and professional experience on BI to use HEIMS was also significant. (c) However, the parameter’s (PE) direct influence on BI to use the system was not significant. (d) The independent variable’s (EE) direct influence on UB of nurses to accept and use HEIMS was significant. (e) Finally, the variable’s (BI) direct influence on the use behavior of HEIMS was also significant as indicated in Tables 4 and 5. Although nurses are known to resist using health IT (Alquraini et al., 2007), their intention to use HEIMS is high and had significant influence. The age of majority of the respondents (90.4%) ranged from 20 to 40 years (Table 1), which could mean a broad exposure to the various health technologies especially in this era of smart mobile phone technology advancement. This is probably due to the introduction of the basic concepts of nursing informatics and general knowledge in computing to the nursing curriculum in Ghana.
Previously, PE has been described as “the extent to which an individual conceives that using a particular system might help him/her to attain a position (such as promotion) in job performance” (Venkatesh et al., 2003). However, the research structural model estimates and the p-values showed that PE was not significant enough to have any influence on the intentions of nurses to use HEIMS, and the significance level (p-value = .10) was greater than the expected value of p < .05 or .01 (Table 4). In view of this, the hypothesis that PE has direct influence on BI of nurses to use HEIMS was not accepted. All the same, the independent variable (PE) had a strong positive relationship with BI (Table 5). This is an indication that when nurses are well trained in ICT, they will be more ready and eager to adopt and use new and advanced health IT in the near future. A linear relationship (Pearson correlation) was observed between PE and BI to use HEIMS; however, it did not reach the significance level as indicated by the structural model tested. However, this result is in contrast with the conclusion made by previous studies (Sharifian et al., 2014; Venkatesh et al., 2003; Venkatesh, Sykes, & Zhang, 2011) which suggested that PE within individual constructs was the strong predictor of BI. PE recorded explained variance of 25.7% associated with BI with age and gender as moderators (Table 6). The degree of ease associated with the use of HEIMS is known as EE (Venkatesh et al., 2003). This study discovered that EE (p < .001) influenced BI significantly compared with PE (p = .10). The coefficient of determinants (R2 = .37) points out that the model explains 37% (Table 6) of the variance associated with BI to use HEIMS among the nurses. This result depicts that EE is a major contributing factor to the readiness of nurses in Ghana to accept and use HEIMS. The significant influence of EE on BI conforms with similar results from studies elsewhere (Venkatesh, Sykes, & Zhang, 2011; Venkatesh, Thong, et al., 2011). The linear correlation between the constructs EE and BI was also significant (p < .01). The hypothesis was accepted, inferring that the structural model results of EE with moderating effects had significant positive influence on BI (Table 4). This result was consistent with other studies (Bawack & Kala Kamdjoug, 2018; I. K. Mensah et al., 2019; Nadri et al., 2018; Sharifian et al., 2014; Strudwick et al., 2015; Vollmer et al., 2016). Based on the aforesaid finding, it can, therefore, be concluded that BI to use HEIMS by nurses in Ghana is influenced markedly by their expected efforts. This result can also suggest that the nurses expect the usage of the systems to be easy to understand and interact with. Hence, a user-friendly HEIMS could easily be accepted and used by Ghanaian nurses. In this report, the direct positive influence of PE on usage behavior (H2) was investigated. This hypothesis was not part of the original five hypotheses set out by the original UTAUT model (Venkatesh et al., 2003). It was observed that PE positively and significantly influenced usage behavior (Table 4). It also explains the 25% of the variance (R2 = .25, Table 6) observed to associate with the usage behavior. Also, PE had a substantially positive correlation with usage behavior (Table 5). Although PE had no significant influence on BI, it had a significant influence on usage behavior (Table 5). Thus, this result confirms that PE could have direct effect on the use of HEIMS among the nurses. The possibility of EE to have a direct influence on UB of HEIMS was tested (Figure 3). The research structural model result of the hypothesis testing indicates that EE has a significant influence on usage behavior of HEIMS. Therefore, the hypothesis was accepted after the testing. The R2 of .311 indicates that the model explains 31.1% (Table 6) of the variance associated with the usage behavior of HEIMS. There is also a direct positive significant (p < .01) correlation between EE and the usage behavior (Table 5). Actually, EE significantly influenced BI and also showed a direct positive substantial impact on usage behavior. This finding suggests that majority of the nurses expect a system that is easy to use and understand. In all both performance and EE wholly explained 37.2% of the variance associated with BI. So, the independent variables’ (PE, EE, and BI) direct influence on the readiness of the nurses to use HEIMS explained 46% of the variance. This means that the performance and effort expectancies as well as their BIs have a great role to play on the readiness of the nurses to use HEIMS in the Ghanaian hospitals.
Practical Implications
Importantly, HEIMS has the potential to improve the efficiency, quality, and patient safety and reduce the cost of medical care. Nevertheless, these systems are not widely available, and even if available are not properly utilized. The UATUT model was adopted out of eight different theories. These theories are needed to enlighten us on the influential parameters that contribute to the readiness of staff in the medical field to adopt and use HIS and other health technologies. Even though some researchers have classified the factors for the barriers to use IT in the health care settings, there is a scantiness of scientifically rigorous research on acceptance and utilization of ICT within the medical care settings. As this is the first of its kind in the assessment of nurses’ technology use behavior in Ghanaian hospitals, it will serve as a guide for revising nursing training curriculum to meet the standard for training nurses toward the adoption of hospital technologies in Ghana.
Conclusion
The testing of the research model results demonstrates that nurses’ intentions on their readiness in accepting and using HEIMS was influenced by their EE. However, their performance and effort expectancies, as well as their intentions to use HEIMS, had the strongest impact on the actual use behavior of HEIMS. In this regard, health facility managers must put procedures in place that will boost the nurses’ confidence in using HEIMS as well as endeavor to adopt and implement a very user-friendly system. The study also provides some empirical and scientific contributions to argument the behavioral issues of health professionals that resist the implementation and use of new technologies.
Limitations
There are some limitations that cannot be avoided when conducting a survey type of study. Hence, this study has some unavoidable limitations. For instance, the nurses answered the questionnaire based on how they understood it, their level of experiences, and their perceptions. Due to this, the outcome of this study may not be generalized for other health professionals. On the contrary, the quality of the data collected was satisfactory with regard to the nature of the report. Besides, the subjects were voluntarily recruited for this survey. Also, it is evident from the literature that this did not negatively affect the results because the study design has been usually employed in this field (Yontz et al., 2015).
Footnotes
Acknowledgements
We would like to thank all the nurses who avail themselves for the success of this study. We would also like to thank the National Natural Science Foundation of China.
Author Contributions
Z.L. and J.O.-M. conceived and designed this study. Z.L. is the overall supervisor of the research team. J.O.-M. designed the electronic form of the questionnaire in the open data kit (ODK) platform to be uploaded to the android platform smart mobile phones. J.O.-M., X.X., and M.O.A. contributed to the writing of this manuscript from literature searching, data collection, analysis, and the final write-up. H.A.A. contributed to the write-up and editing of this paper.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National Natural Science Foundation of China (Grant no. 71974079) during the design of the study and data collection period.
Consent for Publication
All authors have approved the manuscript for submission and publication.
Ethical Consideration
This study was approved by the Ghana health service research ethical committee (No. GHS-ERC:05-12-18). The Health facility Directors/Managers also gave approval before data were collected. Participants were guaranteed of response anonymity. The consent of the respondents was sought though participation was voluntary. Respondents also filled consent forms and signed before answering the electronic questionnaire.