
Abstract
This article examines the extent to which older adult patients’ perceptions of inpatient dimensions of care experiences are associated with their overall satisfaction. A secondary objective is to determine if these specific care experiences differed between elderly female and male patients. Patient satisfaction data from 6,021 older patients (65 years of age and older) were collected by using the Hospital Consumer Assessment of Healthcare Providers and Systems (HCAHPS) Survey through telephone interviews of older patients who were recently discharged. Multiple linear regression analyses with older patients’ HCAHPS dimensions (Communication With Nurses, Communication With Doctors, Responsiveness of Hospital Staff, Communication About Medicines, Cleanliness of the Hospital Environment, and Quietness of Hospital Environment) and gender were conducted while controlling for self-rated health status, age, race, and education. Multiple linear regression analysis showed that all of the HCAHPS dimensions were significantly associated with overall satisfaction. Older female patients reported substantially more positive global evaluations than their male counterparts. However, for older male patients, Communication With Doctors was more influential in their ratings of overall satisfaction than for older female patients. For older female patients, Communication With Nurses was more influential in their ratings of overall satisfaction than for older male patients.
Introduction
Patients’ satisfaction (defined as measuring the needs and wants) has been found to be correlated with the subsequent use of health services, and influences both patient compliance and the continuity of care (Hall, Milburn, & Epstein, 1993; Linn, 1975; MacStravic, 1991; Xiao & Barber, 2008). Patient satisfaction with health care has been examined extensively in different contexts (Crow et al., 2002; Xiao & Barber, 2008). One common target group has been hospitalized patients for at least two reasons. First, admission to a hospital can be a traumatic and frustrating experience for many individuals. Second, admission to a hospital can be associated with high costs for the individual (Quintana et al., 2006). Patient satisfaction and experiences in the hospital setting are considered a cornerstone in the evaluation of health care quality (Danielsen et al., 2010) and have assumed an even greater significance subsequent to the passage of the Patient Protection and Affordable Care Act (PPACA) of 2010 (P.L. 111-148, Section 3001). Under this section of the law, the Hospital Value-Based Purchasing Program, financial incentives are associated with hospitals’ performance on the Hospital Consumer Assessment of Healthcare Providers and Systems (HCAHPS) Survey (Elliott et al., 2012). HCAHPS became a component of Centers for Medicare and Medicaid Services’ (CMS) Reporting Hospital Quality Data for Annual Payment Update (RHQDAPU) program. RHQDAPU instructs that general acute care hospitals that do not report a specific set of quality indicators may have up to a 2% reduction in their annual payment update (Goldstein, Elliott, Lehrman, Hambarsoomian, & Giordano, 2010).
Patients admitted to hospitals are usually old, and, in many cases, have multiple comorbidities and pain that may prevent them from experiencing an optimal stay (Quintana et al., 2006). In most of these studies, a consistent and significant association was found between age and patient satisfaction with older patients (age 65 and older), expressing higher levels of satisfaction compared with younger patients (Peck, 2011). Few studies have examined samples exclusively involving older adults regarding their experiences with care received during their hospital stay. However, mixed results have emerged. Some meta-analyses on hospital patient satisfaction have not shown any gender differences (Sitzia & Wood, 1997), whereas other studies suggest that gender differences do appear (Foss & Hofoss, 2004).
Age has consistently been found to be associated with patient satisfaction scores, with higher age correlated with higher satisfaction scores (Foss & Hofoss, 2004). Among the older hospitalized population, this gender difference could be even more pronounced. Compared with younger patients, older hospital patients have unique needs for the delivery of their care. This is mainly due to the inherent heterogeneity found in this subgroup, the complex health status episodes experiences and the misconceptions regarding health and illness that are prevalent in the elderly population (Carter, McKenna, Martin, & Andrescn, 1989; Ekdahl, Andersson, & Friedrichsen, 2010). Although patient participation in the medical decision-making process has been associated with higher patient satisfaction ratings, research shows that older patients are more likely to assume a passive role in treatment decisions (Breemhaar, Visser, & Kleijnen, 1990). This may be due to the fact that older patients find it more difficult to process complex medical information and are also less likely to maintain their emotional equilibrium while receiving such information (Rahmqvist, 2001).
Hospital care involves inputs from a variety of different sources such as nursing staff, physicians, staff other than nurses, and “hotel” amenities such as patient’s room. These attributes form the basis for patient-reported quality of care surveys. It is unclear from the literature on HCAHPS which attributes are correlated most with patient satisfaction among hospitalized elderly patients. The primary objective of this study was to delineate the contribution of each of the six key independent variables on overall hospital satisfaction among elderly patients. A secondary objective is to determine if these specific care experiences differed between female and male patients.
Method
Design, Data Source, and Setting
This cross-sectional study was conducted between July 1, 2011, and June 30, 2012. The study collected satisfaction with care data from 70 hospitals that are members of the largest nonprofit health system in the United States. The 70 hospitals are largely located in the Midwest, Southeast, South, Northwest, and Northeast, and represent a wide range of hospitals in size, services, and geography. Critical access, community, and tertiary hospitals are represented in the data set. The health system uses approximately 150,000 associates and 40,000 affiliated and employed physicians. Their operating revenue was US$20.5 billion, and the total assets were US$31.0 billion. They had 21,936 available beds and showed 759,693 discharges in 2014.
Data Collection Instrument
The data were collected by applying the HCAHPS Survey instrument to record regular patient experience at each of the hospitals. HCAHPS was developed by the CMS in collaboration with the Agency for Healthcare Research and Quality (AHRQ) to provide a standardized survey instrument for measuring patients’ perspective on hospital experiences (Centers for Medicare & Medicaid Services, 2013). The HCAHPS Survey was the first national, standardized database on patients’ experiences in short-term, acute care hospitals (Kutney-Lee et al., 2009). HCAHPS data are collected through the CMS-prescribed data collection protocol and include the following eligibility criteria: one or more overnight stays in the hospital, a nonpsychiatric principal diagnosis, and alive when discharged (Elliott et al., 2012). The HCAHPS also includes additional questions measuring patient perceptions about aspects of their experience thought to affect overall satisfaction and loyalty to the hospital provider. The AHRQ had RAND Corporation, Harvard Medical School, and American Institutes for Research, together with Westat, carry out a rigorous, scientific process to develop and validate the HCAHPS instrument, and the results (psychometric properties including validity and reliability, credibility, usefulness, etc.) have been confirmed and published elsewhere (Goldstein, Farquhar, Crofton, Darby, & Garfinkel, 2005; O’Malley, Zaslavsky, Elliott, Zaborski, & Cleary, 2005). Data were collected through telephone interviews conducted on a constant and regular basis for each hospital. Patients discharged from one of the hospitals were randomly selected and contacted (generally within a week), and responded directly to the survey vendor. The survey vendor compiled the raw data and sent a data set to the health system’s central office. Response rates vary by individual hospital, but across all hospitals, the average response rate was 40%. This high response rate was achieved through the multiwave survey technique. This study analyzed only those patients who were 65 years of age or older. For further details on HCAHPS Survey administration, see HCAHPS Quality Assurance Guidelines V5.0 (Centers for Medicare & Medicaid Services, 2010).
HCAHPS Survey Measures
The HCAHPS Survey yields a series of measures of patients’ hospital experience. Moreover, the survey includes stand-alone items and global measures. For the purpose of this study, we selected four composite measures of hospital experience—Communication With Nurses, Communication With Doctors, Responsiveness of Hospital Staff, and Communication About Medicines—each comprised of two or three individual survey questions. We also added two stand-alone report items (Cleanliness of the Hospital Environment and Quietness of Hospital Environment). (See http://www.hcahpsonline.org for the entire survey instrument as well as administration protocols) All of these items have a standard set of response options: never, sometimes, usually, and always. The arithmetic mean of these items was used as a composite index for the independent variable.
Additional independent variables included demographic characteristics such as the patients’ race, gender, age, educational attainment, and self-perceived health. The race variable was classified as African American, Asian American, American Indian/Alaska Native, and White. Age was classified as an ordinal variable consisting of five categories: 65 to 69 years, 70 to 74 years, 75 to 79 years, 80 to 84 years, and 90 years or older. Similarly, educational attainment was categorized as an ordinal variable: completed eighth grade or less, completed some high school but did not graduate, graduated from high school or earned General Educational Development (GED), completed some college or earned 2-year degree, graduated from a 4-year college, and completed more than a 4-year college degree. Self-perceived health was measured by asking “How would you rate your overall health?” The response options were excellent, very good, good, fair, and poor, and a larger value indicates poorer health.
The dependent variable, which was derived from the HCAHPS, included a single item asking respondents to rate their experience with an overall rating of the hospital with scores ranging from 0 (worst possible hospital) to 10 (best possible hospital). Similar to previous authors who have used HCAHPS, this item was linearly rescaled to a possible range of 0 to 100 for comparability and ease of interpretation so that the transformed score y = 100 × (x − a) / (b − a), where original score x was on a scale from a to b (Elliott et al., 2012).
Statistical Analysis
Descriptive statistics for the respondents and single items and composite indices are presented in Table 1. Hierarchical linear regression analysis was used to assess the independent associations between the older patients’ gender, the six HCAHPS dimensions (hospital experience measures), and overall patient satisfaction while considering potential hospital-level nested effects. All six HCAHPS hospital experience dimensions and gender were entered simultaneously with the control variables (age, race, self-perceived health, and education). Another Level 1 regression model consisted of two-way interaction terms. The interaction effects were analyzed by creating a product term for each independent variable (e.g., Communication With Nurses) and being female (with being male serving as the reference group) while controlling for the same background variables. The different combining processes of patients with gender and each hospital experience scale were assessed with the significance levels of the coefficients of the product terms. In all analyses, p < .05 was considered statistically significant. All statistical analyses were performed using SPSS v. 22.
Sociodemographic Characteristics of Respondents.

HS = high school; GED = General Educational Development.
Results
The descriptive statistics for the older patient characteristics are presented in Table 1. In brief, the majority of the older patient participants were female (58.7%). Most of the patients were White (90.3%). The largest proportion of patients was found in the 65- to 69-year-old group (25.4%), followed by the 70- to 74-year-old group (23.4%). With reference to educational attainment, the most common category included those who earned a high school diploma or the equivalent (37.4%). Three in 10 of the respondents rated their health as “fair to poor.”
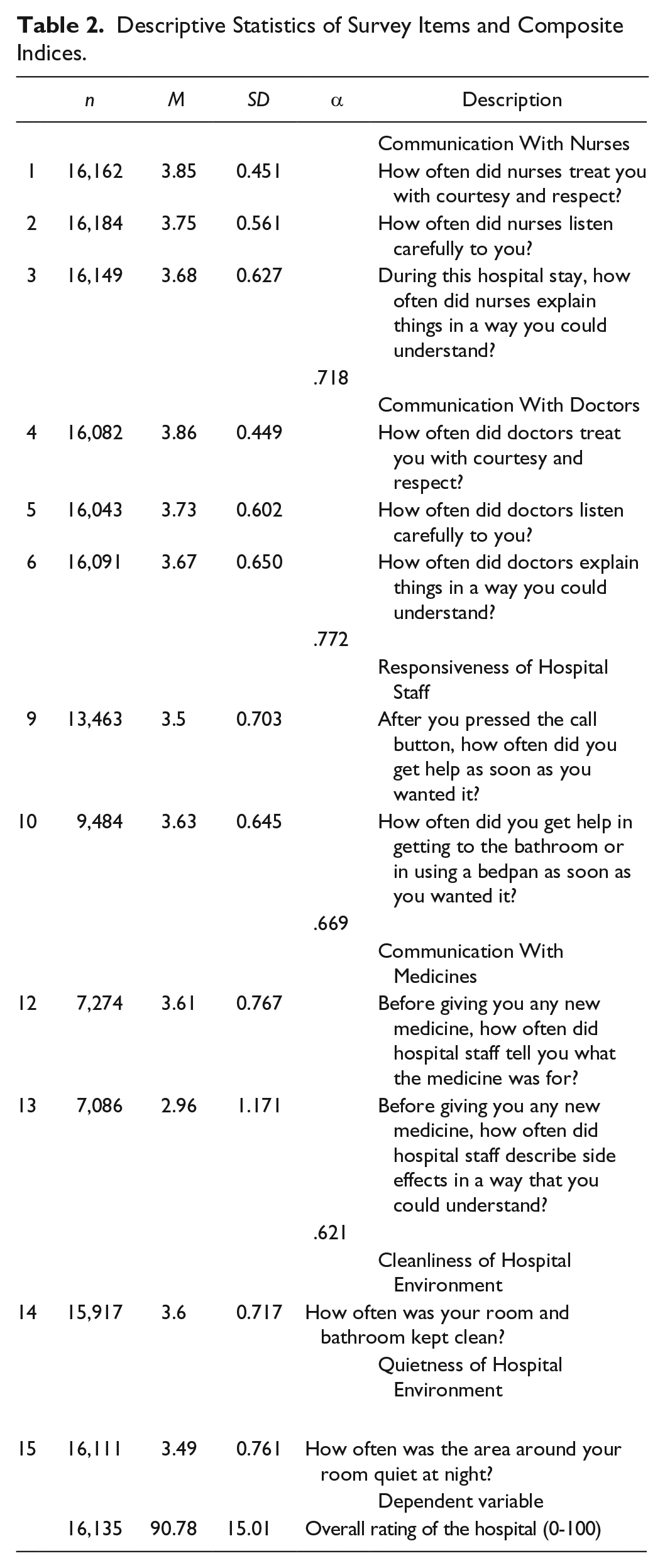
The descriptive results for the single items and composite indices are shown in Table 2. The reliability (Cronbach’s alpha coefficients) of each of the composite indices is also shown in Table 2. Note that the numbers of responses vary because patients did not respond to all items. All survey items in the HCAHPS’s domains show positive patient responses ranging from 2.96 to 3.86, with a score of 4 indicating the strongest level of rating. Each of the composite indices demonstrated good reliability (with Cronbach’s alpha coefficients ranging from .621 to .772). The dependent variable of “overall rating of the hospital” has a mean of 90.78 (range 0-100, with 100 representing the best possible score) and a standard deviation of 15.01.
Descriptive Statistics of Survey Items and Composite Indices.
Multilevel Regression Results
Table 3 summarizes results from the multilevel regression model. To assess the nested effect of hospitals, intraclass correlation coefficient (ICC) was obtained.
Parameter Estimates of Attributes and Control Variables.
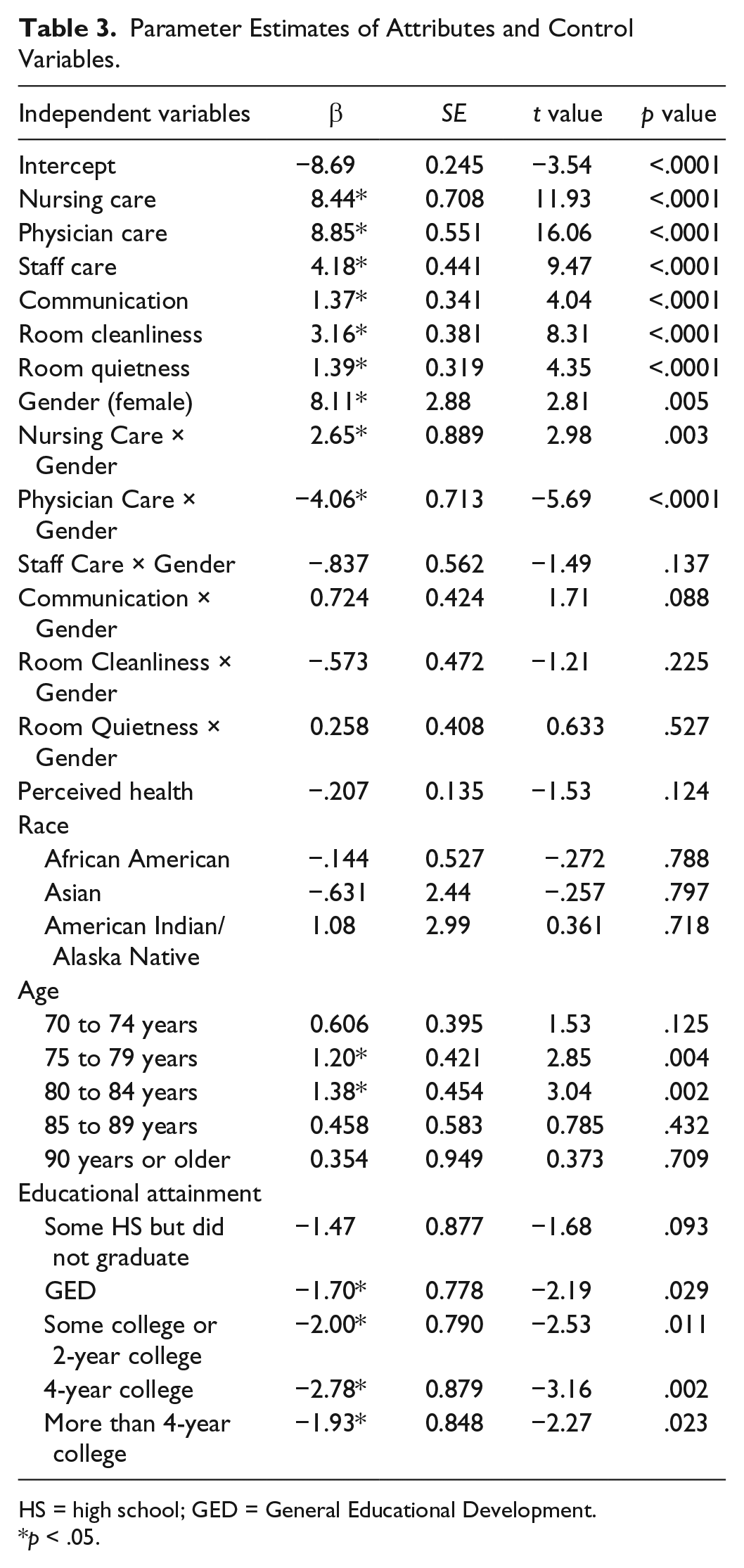
HS = high school; GED = General Educational Development.
p < .05.
ICC = 2.717552 / (2.1717552 + 222.907942) = 1.2%. The value of 1.2% indicates that a small portion (1.2%) of the total variance occurs between hospitals, and thus, most of variance occurs within hospitals.
Being an older female patient was associated with an 8.1-point increase in overall satisfaction after adjusting for hospital experiences, age, race, education, and self-rated health status. All six hospital experience indicators were significantly associated with overall satisfaction. For example, older patients who reported more positive experiences with communicating with the doctors and with the nurses were associated with an 8.8-point and an 8.4-point increase, respectively, in overall satisfaction. Older patients who reported a more positive experience with the responsiveness of the hospital staff were associated with a 4.2-point increase in overall satisfaction. As compared with patients aged 65 to 69 years, older patients aged 75 to 79 years and those aged 80 to 84 years were associated with a 1.2-point and 1.4-point increase in overall satisfaction.
Table 3 also presents the statistically significant interaction terms from the model. For the older patients, a positive and statistically significant interaction effect was found for nursing care and being a female patient. In other words, for older female patients, relationship with nurses was more important in their ratings of overall satisfaction, compared with older male patients. Conversely, a negative and statistically significant interaction effect was found for physician care and being a female patient. That is, for older male patients, relationship with physicians was more important in their ratings of overall satisfaction than for older female patients. The two interaction terms (Responsiveness of Hospital Staff Care × Gender, Communication About Medicines × Gender, Cleanliness of the Hospital Environment × Gender, and Quietness of Hospital Environment × Gender) were not statistically significant.
The last column in Table 3 also shows the level of statistical significance for gender and inpatient dimensions of care experiences, and overall satisfaction. The statistically significant hospital-specific care experience correlates, in order of importance, were Communication With Doctors (p < .0001), Communication With Nurses (p < .0001), Responsiveness of Hospital Staff (p < .0001), Cleanliness of the Hospital Environment (p < .0001), Quietness of Hospital Environment (p < .0001), and Communication About Medicines (p < .0001). Overall, all of the variables accounted for 47% of the variance in hospital rating.
Discussion
In this study, we examined reports of patients’ perceptions of their hospital experience, specifically among older (65 years and older) individuals. More specifically, this is one of the very few studies that examined the relationship between six key hospital attributes—Communication With Nurses, Communication With Doctors, Responsiveness of Hospital Staff, Communication About Medicines, Cleanliness of the Hospital Environment, and Quietness of Hospital Environment—and overall patient satisfaction in a large, geographically dispersed U.S. sample of hospitalized elderly patients. Assessing patient satisfaction is salient because it measures how hospitalized older patients feel about the care they receive. Hospital experience and overall satisfaction was measured by HCAHPS, the first national, standardized survey instrument and data collection methodology for assessing patients’ perceptions of their hospital experience in the United States (Goldstein et al., 2010). Secondarily, we investigated if these specific care experiences differed between elderly female and male patients. Our findings indicate that all six hospital experience measures were significantly associated with overall satisfaction. However, all six were not equally influential. These findings further suggest that a one-size-fits-all strategy to improve patient overall rating of the hospital would not work well. The regression model in the present study explained 47% of the variation in overall patient satisfaction. This explanatory power is comparable with other studies that have incorporated patient-reported experiences and sociodemographic variables as predictors (Bjertnaes, Sjetne, & Iversen, 2012).
Overall, Communication With Doctors was the strongest correlate of overall satisfaction, with the second most influential being Communication With Nurses. These findings are similar to a Norwegian study of 63 hospitals in five health regions, which found that experiences with nursing services and experiences with doctor services were the most important predictors of patient satisfaction for hospitalized patients (Bjertnaes et al., 2012). Thus, the communication with providers (both physicians and nurses) more than the other domains is more important with overall satisfaction, a finding consistent with other studies (Andersen, Rice, & Kominski, 2001). Furthermore, older patients have a better experience with their hospital care when the hospital environment is both clean and quiet.
We also found that older female patients reported considerably greater overall satisfaction than their male counterparts. This finding is contrary to a previous study with HCAHPS data, which found that female patients tended to report worse experiences than men (Elliott et al., 2012). A plausible reason for the difference in the finding is that our study specifically examined patients 65 years or older, whereas Elliott and colleagues (2012) used patients 18 years or older at time of admission. Moreover, our data were more recent (collected from the period 2011-2012), whereas Elliott et al.’s (2012) study used data from the period 2007-2008.
This study found that patients combined their attribute reactions differently depending on their gender. For older male patients, Communication With Doctors was more influential in their ratings of overall satisfaction than for older female patients. This finding suggests that when a hospital admits patients who are older men, the hospital needs to consider and maintain optimal communication by physicians. Conversely, the present study found that for older female patients, Communication With Nurses was more influential in their ratings of overall satisfaction than for older male patients. These findings are in contrast to some studies that found that women report less positive interactions than men with nurses but better interactions with physicians (Elliott et al., 2012). The clear gender differences in our study underscore the need for a gender-sensitive approach in the encounters between older male and female patients by physicians and nurses, respectively (Foss & Hofoss, 2004). The remaining four other HCAHPS patient experience domains and gender interaction effects were not statistically significant.
Among the other independent variables, age and educational attainment were found to be statistically significant. For the age variable, the age groups of 75 to 79 and 80 to 84 years were found to report greater overall satisfaction than the reference age group of 65 to 69 years. In other words, patients aged 75 to 84 years were more likely to rate their overall hospital stay as positive compared with patients aged 65 to 69 years. In terms of educational attainment, greater educational attainment tended to be inversely associated with overall satisfaction. As compared with those with less than an eighth-grade education, patients in the following groups had lower satisfaction scores: high school (or equivalent), some college, a 4-year college education, and more than a 4-year college education. For instance, respondents with a 4-year college education, the group with the strongest magnitude, were associated with a 2.77-point decrease in overall satisfaction.
Study Limitations
Some important caveats of the present study need to be mentioned. First, the cross-sectional design of this study does not inform us about causation. Future research should use longitudinal designs that would better assess causality in addition to unmeasured variables. Second, our analysis was limited to a certain number of hospitals that voluntarily submitted HCAHPS data during the time frame delineated in the study. In other words, the hospitals used in the present study may not be representative of all hospitals in terms of location and bed size. As reported elsewhere (Lehrman et al., 2010), rural hospitals with fewer than 100 beds and those in the Plains region were underrepresented among hospitals that voluntarily participated in the HCAHPS data reporting. Third, we were unable to control for the consumers’ attitudes toward physicians and nurses before their hospital stay. Future research should collect data that examine consumers’ attitudes before and after their hospital stay. From a health plan perspective, an ultimate outcome measure of patient satisfaction is whether or not enrollees choose to switch plans (Cunningham & Kohn, 2000). Future studies can use the patient satisfaction data as a predictor of plan switching in older hospitalized adults.
Fourth, the data available precluded us from considering patient loyalty (“a personal commitment that contributes, or at least can be expressed in terms of contributions, to the success and survival of a health care provider, either an individual practitioner or an organization”), an important variable linked to overall satisfaction (MacStravic, 1991, p. 61). Hospital loyalty, expressed as intention to return to or recommend the hospital they used most recently, is typically reported to be quite high. However, the intention to return to a hospital tends to fade with time, subject to significant attrition in 3 to 6 months, and such a decision differs between men and women (Fisk, Brown, Cannizzaro, & Naftal, 1990). Future research should consider loyalty and, in particular, differences between men and women. Finally, our data precluded us from controlling for a series of patient health status characteristics. With the exception of self-rated health status, we were unable to control for other health-related variables of the patients, including number of admissions in the past year or so and length of stay in the hospital.
Implications
Despite these study limitations, our data have distinct value and offer some important implications. Our study is one of the few that described older patient hospital experiences and satisfaction with care by using a validated HCAHPS instrument among a large U.S.-based private, not-for-profit hospital system. Findings from our study have implications for treating geriatric patients. Overall assessments of older patients in hospitals can be improved by assuring good communication by nurses and doctors, as well as maintaining responsiveness of staff to older patients’ needs and ensuring clear communication by staff.
It is plausible that findings from this study may be attributed to multiple factors found in the older adult patient population such as previous experiences with inpatient care, a relatively low level of knowledge regarding medical issues, and a strong tendency to provide socially acceptable responses to survey questionnaires. Some studies suggest that the positive perception of health care quality in older patients could possibly stem from the fact that health care providers are in reality more responsive to their needs resulting in a more patient-centric experience (Bjertnaes et al., 2012). Behavioral research has shown that older patients are less demanding and more prone to resigning themselves to their fate. Thus, lower expectations and higher acceptance of their condition may also influence overall satisfaction with hospital care among older adults.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research and/or authorship of this article.