
Abstract
Patient rights support patient autonomy and is an important bioethics issue that has been on the healthcare agenda in recent decades. Patients exercising their rights is one of the factors that positively affect the care and treatment process. The aim of this study is to determine the attitudes toward patients exercising their rights, factors affecting it, and to raise awareness on the subject. This cross-sectional descriptive study was conducted with 421 patients hospitalized in a university hospital in Turkey. Data were collected using the Scale of Patient Rights Using Attitude (SPRUA) and 16 questions identifying the demographic characteristics of the participants and information that is thought to affect attitudes toward patient rights. Each statement on the SPRUA, a Likert-type scale, is scored from 5 to 1. The total score that can be obtained from the scale ranges between 29 and 145. The total score on the scale determines the attitude toward using patient rights. The Shaphiro wilk test, Student t test, One Way ANOVA, Tukey multiple comparison tests, Kruskal Wallis and All pairwise tests were used to evaluate the data. Participants’ total mean score on the SPRUA was 117.50 ± 22.72. Some socio-demographic variables and experiences during the illness affected the participants’ attitudes toward exercising patient rights. There was a significant difference between the participants’ the mean SPRUA score and the following factors: age, education level, place of residence, clinic hospitalized in, chronic disease status, knowledge about patient rights, duration of hospitalization. The participants had high mean scores on the scale.
Introduction
An extension of human rights, patient rights have been an issue of discussion in the last decades. Human rights are defined in three generations according to their development and quality. The first generation is the human rights which include rights such as freedom, equality, personal safety, and life. The second-generation human rights which developed later include economic, cultural, and social rights which include health and educational rights. After the second half of the 20th century, third generation human rights, which include consumer rights, children’s rights, and patient rights have come to the fore (Daher 2016; Hoving et al., 2010; Rothman, 2001).
Effects of technological advancements in the field of medicine, healthcare services and health professional-patient relationship have a key role in bringing patient rights to the fore.
The right to health is defined as the right to seek services for the protection and improvement of a person’s health from the society or government, to be treated in case of illness and to benefit from social and health services (Backman et al., 2008; Hunt, 2016). Patient rights have come to the fore frequently as an extension of the right to health as patient autonomy has been prioritized (Sarıkaya & Altunışık, 2019).
Bioethics Glossary defines patient rights as rights individuals have, just because they are human which are guaranteed by international treaties, constitutions, laws, and other legislations (Oğuz et al., 2005). Therefore, patient rights emphasize the rights that patients have at every stage of health care (Hunt, 2016). Patient rights include concepts such as being informed about diseases, being respected for values, making autonomous choices about the treatment process, obtaining/giving informed consent, privacy, dignity, psychosocial and moral values (Çobanoğlu, 2009). An important factor that increases the quality of the treatment and care is for patients and healthcare professionals to know their rights and responsibilities. In the context of medical ethics, patient rights are closely related to the principles of autonomy and respect for autonomy, benefit, non-harm, and justice (Çobanoğlu, 2009; Peled-Raz, 2017; Putturaj et al., 2020). There are legal regulations regarding patient rights in Turkey. Patient rights are discussed in The Patient Rights Regulation of 1998 and the Regulation Amending the Patient Rights Regulation in 2014 under titles Right to Benefit from Health Services, Right to Information about the Health Status, Protection of Patient Rights, Consent of the Patient in Medical Intervention, Consent in Medical Research, and Respect for Human Values and Right to Complaint and Lawsuit (Patient Rights Regulation, 1998).
For patients to know, become aware of and exercise their rights while receiving health care services is an implementation of basic human rights in the healthcare system. Some of the basic approaches in improving patient rights are contributing to the individual wellbeing of the patient, supporting the patient’s autonomy, and providing an opportunity to the patient to actively participate in the decision instead of taking a passive stance (Cohen & Ezer, 2013).
It is important for healthcare professionals, institutions and governments to take responsibility and inform people about patient rights. In addition, it is important for patients to know their rights and demand health services within this framework. This mutual approach will increase service quality and satisfaction and contribute to the sharing of responsibility (El-Shimy et al., 2020).
Patient rights are the set of rules that govern the patient in patient-health professional interaction. Patient rights affect the quality of healthcare and define the patient’s role in healthcare (Cohen & Ezer, 2013; El-Shimy et al., 2020; Sarıkaya & Altunışık, 2019). Today’s medical understanding adopts an approach that emphasizes patient autonomy which allows the patient to actively exercise patient rights. In the literature, the knowledge and awareness levels of patients about patient rights vary (Abiiro et al.,2020; Gurung & Sapkota, 2019; P. Mohammadi, Naderiravesh, et al., 2018; M. Mohammadi, Larijani, et al., 2018; Wrześniewska et al., 2017).
The basis of the health professional-patient relationship is good communication. The main purpose of this communication is to help the patient be aware of his condition, to determine his own health values, and to choose treatment methods. In this process, it is important to know the rights and responsibilities of both the physician and the patient in strengthening the interaction between them. When we look at patient rights in context of medical ethics, the principle of autonomy and respect for autonomy is intertwined with the principles of benefit, non-harm, and justice (Peled-Raz, 2017; Putturaj et al., 2020). A limited number of studies have been conducted that determine patients’ attitudes and awareness of their rights on a national scale. These studies emphasize the importance of increasing patients’ awareness of their rights. The starting point of this study is to determine the attitudes of patients about exercising their rights and to raise and increase awareness about patient rights.
Purpose of the Study
The aim of this study is to determine the attitudes toward exercising patient rights and the affecting factors and to raise awareness on the subject.
Method
Study Design
The research was conducted as a cross-sectional descriptive study.
Study Setting
The research was carried out at a University Training and Research Hospital in Turkey between May and September 2018. Clinic, polyclinic, intensive care, and emergency services are provided in the hospital. The study was conducted with patients hospitalized in internal and surgical clinics.
The Universe and Sample of the Research
The universe and sample of the study consisted of patients hospitalized in the internal and surgical clinics of a university training and research hospital. The population of the study consisted of the patients (N = 22,801) hospitalized in the internal medicine (n = 9,525) and surgical wards (n = 13,276) at X University Training and Research Hospital. The sample of the study was calculated using the sample selection formula (n = N.(t1-α)2.(
Data Collection Tools
The data collection form used consisted of two parts. The first part had 16 questions to determine the demographic characteristics of the participants and the information that is thought to affect their attitudes toward exercising patient rights. These questions included age, gender, place of residence, economic status, status of having a chronic disease, level of knowledge about patient rights, sources of information about patient rights, hospital experience, and length of stay in the hospital. The questions were prepared by the researchers after conducting literature study (Erbil, 2009; Öztaş & İyigün, 2016; Zaybak et al, 2012).
The Scale of Patient Rights Using Attitude (SPRUA) developed by Erbil was used in the second part. The validity and reliability study of the scale was carried out by Erbil (Erbil, 2009). SPRUA is a measurement tool with 29 items and 7 sub-dimensions. Each statement on the scale developed in the Likert type was scored from 5 to 1. Five points were given to the “I always use it,” 4 points to “I usually use it,” 3 points to “I sometimes use it,” 2 points to “I usually do not use it,” and 1 point to “I never use it” response.
The lowest score that could be obtained on the scale is 29, and the highest possible score is 145. The total score on the scale indicates the attitude toward exercising patient rights. A high score is interpreted as having a positive attitude toward exercising patient rights (Erbil, 2009).
The sub-dimensions on the Scale of Patient Rights Using Attitude are: (1) right to informed and respectful care (8 items); (2) right to choose/change medical personnel and access to medical records (7 items); (3) right to visitor, companion, safety, and complaint (4 items); (4) right to consent to and refuse treatment (2 items); (5) right to have personnel provide appropriate medical services and obey prohibitions (4 items); (6) right to consent to medical and pharmaceutical treatment (2 items); (7) right to consent to organ tissue transplantation, use of family planning, and terminate pregnancy (3 items). The Cronbach Alpha reliability coefficient of the scale was .88 (Erbil, 2009). Total item- point correlation was determined between .21 and .60 and were found significant at the level of importance p = .000. (Erbil, 2009). The Cronbach’s Alpha reliability coefficient in this study was .94 in total and between .46 and .96 for the sub-dimensions.
Application of Data Collection Forms
Data were collected from the participants who met the inclusion criteria and agreed to participate in the study between May and September 2018. It took about 15 to 17 minutes to complete the data collection forms. The data collection forms were given in person by the researchers to the hospitalized patients who agreed to participate in the study.
Data Analysis
SPSS Windows version 24.0 was used for statistical analysis. The data were tested with Shaphiro wilk test for normal distribution and Student t test to compare normally distributed properties in two independent groups. In addition, for comparison of numerical data in more than two independent groups, One Way ANOVA and Tukey multiple comparison tests were used for properties showing normal distribution. Kruskal Wallis and All pairwise multiple comparison tests were used for features that did not normally distribute. Cronbach alpha coefficients were calculated in order to evaluate the validity and reliability. As descriptive statistics, mean ± standard deviation for numerical variables and number and percentage values for categorical variables were given. Statistical p value <.05 was considered significant.
Ethical Aspect of the Research
Permission was obtained from X University Clinical Research Ethics Committee. (Decision No: 8 dated 22.03.2018). Written informed consent was obtained from the patients who met the inclusion criteria and who agreed to participate in the study. In addition, written permission was obtained from the relevant author to use the scale.
Results
The average age of the participants was 53.25 ± 18.02 and 43.9% were 58 years or older. Almost half of the participants (46.1%) were women, 59.1% were primary school graduates and 44.9% lived in the city. When asked about their income levels, 56.1% stated it was equal to expenses; 54.4% of the participants were hospitalized in surgical clinics, 45.6% in internal clinics, and 55.8% had a chronic disease. In addition, 81.5% of the participants stated they did not have information about patient rights.
Only 78 participants (18.5%) answered the question about the source of information about patient rights; 56.41% of those who answered stated that they received information about patient rights from healthcare workers and 24.35% from radio/TV/newspaper. A majority of the participants (81.9%) stated that they had previous hospital experience; at the time of the study 71.7% stated that they were hospitalized between 1 and 5 days. 88.6% of the patients stated that they were not educated on patient rights during their last hospitalization.
Table 1 contains the scale sub-dimension and total scale score averages of the participants. Participants’ total score average was 117.50 ± 22.72, right to information and respectful service sub-dimension mean score was 34.82 ± 6.79, right to choose/change personnel, review records mean score was 24.85 ± 6.89 and right to visitor, companion, safety, and complaint mean score was 17.08 ± 3.04 (Table 1).
Distribution of the Patients’ SPRUA and Sub-Dimension Mean Scores (n = 421).
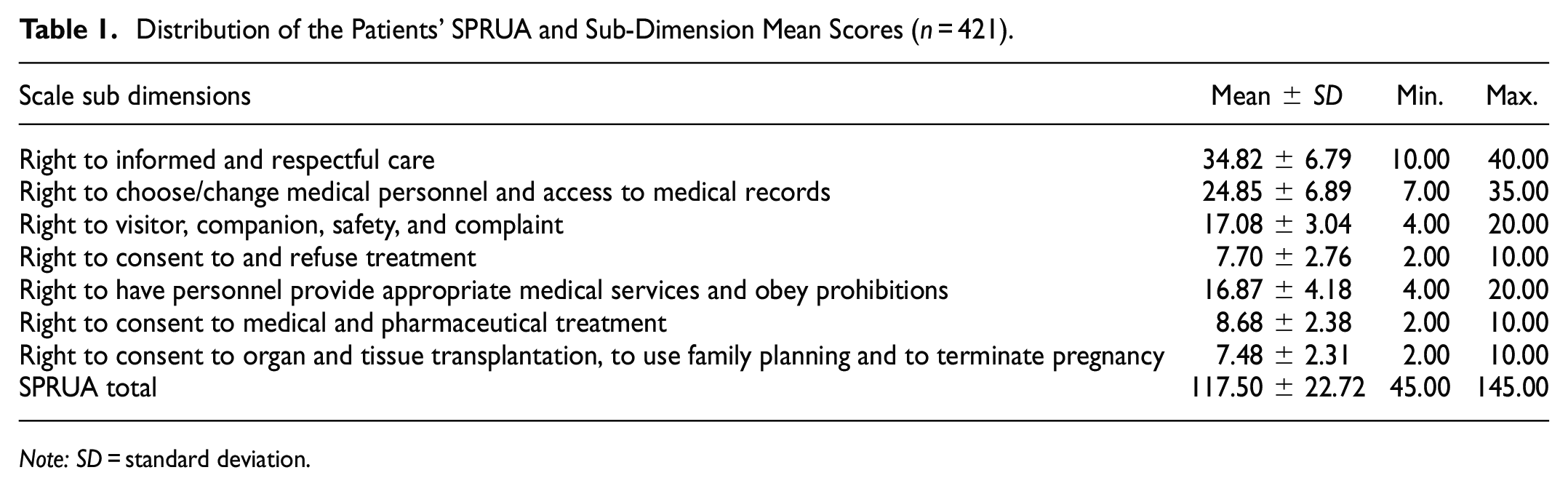
Note: SD = standard deviation.
Table 2 shows the comparison of the mean scores according to the sociodemographic characteristics of the participants. There was a significant difference between the participants’ age and the mean score (p = .000). According to further analysis performed, the difference was due to patients 58 years old and above (p < .05). Average scale score of patients 58 years and over were lower than other age groups.
Distribution of SPRUA Scores According to Patients’ Sociodemographic Characteristics.

Note. t = student t test; KW = Kruskal Wallis; F = one way ANOVA; SD = standard deviation.
The difference between the education level and the total mean score was significant (p = .000). According to the advanced analysis using All pairwise test, the difference was due to illiterate and literate patients (p < .05). The mean score of these two groups was lower than the patients with other education levels. Also, there was a significant difference between the place of residence and the mean score (p = .000). According to the Tukey test, the difference was due to the patients living in villages/towns (p < .05). The mean score was lower for the patients living in villages/towns than those living in the province and city. There was no significant difference between gender and economic status and the mean score (p > .05).
Table 3 shows the comparison of the mean scores according to the hospital experiences of the participants. The difference between the clinic patients hospitalized in and the mean score was significant (p < .05). The mean score of the patients hospitalized in surgical clinics was higher. The difference between the status of having a chronic disease and the mean score was significant (p < .05). Total scale score average of those without a chronic disease was higher. The difference between the knowledge of the participants about patient rights and the mean score was significant (p < .05). The total score average of the participants who were informed about patient rights was higher. Also, the difference between the hospitalization time and the mean score was significant (p < .05). The mean score of patients with 1 to 5 days of hospital stay was higher than those with 6 or more days. The difference between the participants’ source of information about patient rights, previous hospitalization experience, state of being informed about patient rights at the last hospitalization and the mean score was not significant (p > .05).
Distribution of SPRUA Score Averages According to Patients’ Hospital Experiences.

Note. t = Student t test; KW = Kruskal Wallis; SD = standard deviation.
Discussion
Patient rights are an important element in health professional-patient communication and interaction during the delivery of health services. The awareness of patients about their rights has a key role in providing better health care. In our study, more than three fourths of the participants stated that they had no knowledge of patient rights. Approximately one-fifth of the participants answered the question about the sources of information about patient rights. More than half of those answered stated that they received information from healthcare professionals and one fourth from radio/TV/newspaper. Different studies concluded that sources of information about patients’ rights as doctors, nurses, doctors-nurses, posters, media, and internet (Çelik & Taşhan, 2014; Erer et al., 2018; E. S. Mohammed et al., 2017; Unnikrishna et al., 2017; Wrześniewska et al., 2017). In a different study, the importance of the role that healthcare providers such as physicians, nurses, and administrative staff have in informing patients about their rights and the exercising of patient rights and creating awareness was emphasized (P. Mohammadi, Naderiravesh, et al., 2018).
In a study conducted to determine the attitudes of hospitalized patients about exercising patient rights, the rate of those who knew half of the patient rights was 51.1%; almost all patients knew the names of their physicians, and only 28% knew the rights to privacy and confidentiality (Agrawal et al., 2017). In a study by Farzianpour et al., conducted to determine the awareness of female patients about different aspects of patient rights, the first three patient rights with the highest score average were providing adequate information about the disease, protecting privacy, and patient’s right to make a decision (Farzianpour et al., 2016). In our study, the rights exercised the most among the participants were “the right to consent in medical and drug applications,”“right to visitor, companion, safety and complaint,” and “the right to consent to and refuse treatment.” Priority order of the issues related to patient rights differs between societies. While the “right to consent to medical and pharmaceutical treatment” was prioritized in our study, “right to be informed” and “right to choose/change medical personnel” were rated more important in other studies. This difference may be related to the cultural factors.
In our study, the average scores of our participants were high. In a study by Çelik and Taşhan (2014), the total score average of the individuals’ attitudes toward exercising patient rights was higher than the findings in our study. In other studies, patients had a more positive attitude toward patient rights (El-Shimy et al., 2020; P. Mohammadi, Naderiravesh, et al., 2018). In a study conducted in Egypt, three quarters of the patients did not know that there was a regulation about patient rights and only 40% of the patients were aware that they deserve to be informed about their rights and responsibilities in a manner they can understand (E. S. Mohammed et al., 2017). In different studies conducted with patients, the level of knowledge and awareness of the participants about patient rights was insufficient (Abiiro et al.,2020; Wrześniewska et al., 2017; Younis et al.,2017). It is important for the patients to know and exercise their rights in their relationship with the healthcare professionals since expressing their expectation/desire from health services will contribute positively to their treatment.
In our study, participants in the 18 to 27 age group had the highest mean scores (p < .05). In a different study that used the same scale, the average score of individuals 31 to 43 age group was the highest (Çelik & Taşhan, 2014). The percentage of 18 to 35 year old patients in a different study who knew their right to consent, to provide feedback about the treatment process, to privacy and confidentiality of patient information, to know treatment options, and the approximate length of stay in the hospital was higher (Agrawal et al., 2017). Studies have found a significant relationship between age and attitude toward exercising patient rights (S. A. Mohammed et al., 2015; Öztaş & İyigün, 2016). These results are similar to our results. Age is an important factor in knowing and using patient rights. Patients of different age groups tend to exercise different patient rights depending on their level of knowledge and importance attached to the subject.
In our study, participants’ attitudes toward exercising patient rights became more positive as the level of education increased. Other studies had similar results (Agrawal et al 2017; Çelik & Taşhan, 2014; Çetinkaya et al., 2013; Dadashia et al., 2019; Ghazanfari et al.,2018; Hifnawy et al., 2017; Sharifzadeh et al., 2019). Education is an important factor in how people obtain information about the subject and know how to exercise patient rights. Patients with higher education levels are expected to have more awareness and positive attitudes about patient rights.
In our study the significant difference between the place where the participants lived, and their mean score was due to the low scores of those living in small residential areas. In a study conducted with diabetic patients, Sharifzadeh et al. (2019) determined a significant relationship between the place where the patients lived and their perspective on patient rights (p = .001); those living in the town had a more positive perspective than those living in the village. In Ghazanfari et al.’s (2018) study, a significant relationship was found between attitudes of females toward patient rights regulations and the place of residence (p < .001); the attitudes of urban residents were found to be more positive. These results are similar to ours. Socio-cultural characteristics may be a factor in the awareness about patient rights.
In our study, patients hospitalized in surgical clinics had more positive attitudes toward exercising patient rights. In a study conducted with patients and their relatives, there was a significant difference between the mean scores based on the clinic in which the patient was hospitalized in and the information sub-dimension (Toygar et al., 2015). In a study about patient rights by Agrawal et al. (2017), awareness of the patients with less than 6 days of hospitalization was higher which is similar to our results. In our study, mean scores of patients who had no previous hospitalization experience and had 1 to 5 days of hospitalization were found to be significantly higher. A study conducted to determine the awareness about patient rights and responsibilities of patients diagnosed with tuberculosis revealed that participants did not have a full understanding of patient rights, but they accepted their responsibilities and concluded that not understanding patient rights was an important obstacle in tuberculosis management (Atif et al., 2016). In a different study, patients with high number of hospitalization days (7 or more) had higher patient rights attitude scores (S. A. Mohammed et al., 2015). In a study conducted with surgical patients, the total scale scores were significantly higher in patients who were informed about patient rights than those who were not (Öztaş & İyigün, 2016). Patients being informed about patient rights is an important element in terms of medical ethics. The awareness of patients about their rights and their conscious exercise of these rights while receiving healthcare services are among the factors that will positively affect the physician-patient relationship and the treatment process.
In our study, those participants who had previous knowledge about patient rights had a significantly higher score. Studies conducted about patient rights have emphasized the fact that awareness of patients about their rights and regulations regarding patient rights need to be increased. Also, evaluating patients’ views on the observance of their rights and to receiving patient feedback is an integral component of service quality and medical ethics (Abedi et al., 2017; Agrawal et al., 2017; Farzianpour et al., 2016; Krennerich, 2017). It is important for healthcare professionals and the institution to inform patients in order to raise awareness about patient rights. In addition, studies on patient rights should be conducted in all segments of the society and to ensure patient autonomy and that rights are exercised consciously by patients.
In their study with hospitalized patients, Gurung and Sapkota (2019) stated that most of the participants knew the right to know the treatment, to receive respectful and safe services, to know treatment alternatives, to receive continuous care, to complain about health services, and to confidentiality. Shevchuk et al. (2020) emphasized that the patients’ right to receive complete and reliable information about their health is an indispensable right. Perić et al. (2018) reported that patients who underwent surgery received sufficient verbal information and did not read the consent form because they trusted their doctors; the reason for not reading the consent form was that the patients evaluated the situation as urgent and were not given the opportunity to think.
Implications to Practice and Future Research
Having a positive attitude about patient rights will guide the patients to know and exercise their rights and responsibilities. With a large sample, this study revealed the attitudes about patient rights of adult patients who applied to a university hospital in the southern region of the country and received inpatient service in internal and surgical clinics. This study will increase patients’ awareness about patient rights in daily practice. Also, it will have a positive effect on patient knowledge and exercise of patient rights. This study should be conducted with a larger sample to reveal the attitudes of different patient groups.
Conclusion
Knowing and exercising patient rights is a factor that will positively affect the healthcare professional-patient relationship and the treatment process. It is important for medical practice that patients know and exercise their rights. Awareness and exercise of patient rights is an approach that supports patient autonomy. Therefore, informing patients about their rights and raising awareness are among the responsibilities of health professionals. In our study, participants’ attitudes toward patient rights were positive. Some sociodemographic variables (age, educational status, place of residence) and experiences (clinical service received, presence of chronic disease, knowledge about patient rights, duration of hospitalization) affected attitudes toward exercising patient rights. Health professionals should be encouraged to provide information fulfilling their role as patient advocates.
Limitation
The location and sample of this study is a limitation. The research was carried out with patients hospitalized in a university hospital in the southern region of Turkey. The result of the study is limited to the responses of the participants.
Footnotes
Acknowledgements
We thank Serpilay Mum and Döne Saçar for their contributions.
Author Contributions
Conceptualization, writing—original draft preparation; RCO, HT
Investigation, methodology; RCO
Funding acquisition, supervision; RCO, HT
Formal analysis; HT
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.