
Abstract
This study aimed to assess nurses’ knowledge to control infection transmitted by intensive care units. Specifically, the study focused on the constructs of nurse’s knowledge, such as guidelines, personal practices, and preventive practices to control contagious diseases in intensive care units’ patients. A descriptive cross-sectional study design was utilized in this study. A convenience sample of 209 nurses from intensive care units was included in the analysis. The study was carried out at the intensive care units of five hospitals of the Aseer Health Authority, Saudi Arabia. The self-administrated questionnaire was adapted to assess the knowledge of safety guidelines, personal safety measures, and preventive practices among the study participants. The findings suggested a significant knowledge gap regarding the nurses’ knowledge of guidelines and prevention practices. F statistics showed a significant gender-based differences in nurses’ knowledge about guidelines, personal practices, and healthcare-associated infections prevention practices (F = 9.78, p < .05; F = 13.45, p < .05; F = 2.47, p < .05, respectively). There is little information available about standards, behavior patterns, and ways to stop infections from spreading to intensive care units’ patients. In order to illustrate significant results and provide additional recommendations for future research, this work attempted to close the gap between previous findings and the findings of this investigation. The study highlighted the fundamental relevance of infection control practices in healthcare, particularly in intensive care units, in ensuring patient safety.
Plain Language Summary
The study highlighted the fundamental relevance of infection control practices in healthcare, particularly in intensive care units, in ensuring patient safety. Inadequate comprehension of these practices by nurses might have serious repercussions, such as healthcare-associated infections (HAIs), increased expenses, and longer hospital stays. The research focused on Aseer Health Authority nurses, revealing that while knowledge about personal practices is relatively better, gaps persist in understanding guidelines and prevention practices. However, no pronounced variations were noted among demographic factors except for age and marital status, which insignificantly influenced knowledge. The findings suggested a significant knowledge gap regarding the nurses’ knowledge of guidelines and prevention practices. These findings indicated the need for targeted interventions, ongoing training, and sharp awareness campaigns to boost infection control knowledge among nurses, ultimately contributing to safer healthcare environments and improved patient outcomes.
Introduction
Infection control is one of the critical components in healthcare facilities. The significance of implementing infection control measures within healthcare facilities, especially in intensive care units (ICUs), cannot be emphasized enough (Mukhopadhyay, 2018). The complex medical procedures performed in ICUs make them high-risk areas for the spread of infections, thus making infection prevention and control a top priority. As the primary caregivers in ICUs, nurses play a critical role in ensuring patients are safe from infections. Evaluating their knowledge and understanding of infection control measures is essential in determining the success of infection control programs in healthcare facilities (Sole et al., 2020). Research conducted in Saudi Arabia revealed that while nurses understand the importance of infection control, their knowledge of specific guidelines and protocols for HAI prevention in ICUs is limited (Yaseen & Salameh, 2015). Similarly, a study conducted in India also reported a lack of knowledge about the guidelines for infection control among nurses working in ICUs (Barker et al., 2017). A study by AlJohani et al., 2021) assessed the level of infection control knowledge among nurses in Saudi Arabia and found that while the overall knowledge level was high, there were still knowledge gaps in specific areas, such as hand hygiene and isolation precautions. Another study by Alsahafi et al. (2021) examined the association between infection control knowledge and practices among nurses in the Eastern Province of Saudi Arabia and found a significant positive correlation. Similarly, a study by Alhazmi et al. (2019) investigated the level of infection control knowledge among nurses in a tertiary hospital in Saudi Arabia and found that while the overall knowledge level was satisfactory, there were gaps in knowledge related to standard precautions and disinfection. In the wider Gulf region, a study by Alnasser et al. (2021) investigated the knowledge, attitudes, and practices of infection control among healthcare workers in Bahrain and found that while the overall knowledge level was high, there were still knowledge gaps related to isolation precautions and antibiotic resistance.
The quality of care and prevention practices highly depend on the nurse’s commitment to their patients. In this regard, Vaismoradi et al. (2020) conducted a systematic review to evaluate nurses’ practices, adherence, and devotion to patient safety principles. The study found that nurses’ practices, such as proper use of equipment, collaboration with other nurses, and standardized care processes, increased and minimized HAIs, thus improving overall patient safety. The study, which also involved a systematic review of articles published between 2010 and 2019, found that significant factors such as healthcare providers’ knowledge, attitudes, education, and provision of regular feedback positively impact patient safety principles (Vaismoradi et al., 2020).
Studies have revealed the importance of hand hygiene and protective clothing in the prevention of healthcare-associated infections (HAIs) in intensive care units (ICUs; McLaws et al., 2015; Casaroto et al., 2022). However, compliance with these practices among nurses is lacking (McLaws et al., 2015). A study in Iran reported that nurses knew the importance of hand hygiene, but there was still room for improvement in adherence to hand hygiene protocols (McLaws et al., 2015). The results of Şenol et al. (2022) found that training on protective clothing usage resulted in higher levels of compliance among nurses. Environmental cleaning and disinfection practices in the ICU setting were also identified as areas of limited knowledge among nurses (Mitchell et al., 2013). Nurses were knowledgeable about isolation precautions, but compliance with these practices was lacking (Ghazanfari et al., 2022).
The literature review has found that HAIs have been widely discussed by various authors, healthcare professionals, and researchers due to the impacts they bring on patients’ outcomes, hospitals regarding elevated health costs, and overall public health. In addition, the phenomenon of healthcare-associated infections is widespread, as there exist various infections with which patients of ICUs are most likely to suffer. However, despite this in-depth knowledge and comprehension of the matter, the various aspect of knowledge which is entirely needed for healthcare nurses serving in the intensive care unit of hospitals is missing. Knowledge of guidelines, personal practices, and prevention practices of infection spread to patients in ICUs is limited. In this concern, this work aimed to bridge the gap between existing findings and this study’s findings to depict meaningful outcomes and further suggestions for future research.
This study aimed to investigate the level of familiarity among nurses in the Aseer Health Authority, Saudi Arabia concerning infection control measures and to assess how this knowledge may affect the overall standard of care given to patients.
Methods
The study utilized a cross-sectional survey design. The participants were nurses who work in intensive care units (ICUs) in five hospitals in the Aseer Health Authority, Saudi Arabia. The participants were selected using a convenience sampling method and included 209 nurses. Participants were informed about the purpose of the study and asked to give their informed consent to participate.
The self-administrated questionnaire was adapted to assess the knowledge of safety guidelines, personal safety measures, and preventive practices among nurses (Fashafsheh et al., 2015; Geberemariyam et al., 2018). The questionnaire is divided into four parts:
The first part contains five demographic questions about the participants: gender, age, marital status, level of education, and years of experience.
The second part includes six questions related to nurses’ knowledge about guidelines. For example, “I have attended a training course on infection control.” Responses were recorded as “Yes” or “No.”
The third part focuses on nurses’ knowledge regarding personal practices with five items. For example, “Gloves should be worn if blood or body fluid exposure is anticipated.” The questions were closed-ended with yes or no answers from the participants.
The fourth part includes five items to measure nurses’ knowledge regarding disease and risk prevention practices. For example, “Do you use all Personal Protective Equipment (PPE) to prevent the risk of acquiring and/or transmitting infection?.” The questions were closed-ended with yes or no answers from the participants.
Data was analyzed using the SPSS statistical software. Frequency analysis was performed to determine the frequency of responses for each question on the questionnaire. Descriptive statistics such as mean, standard deviation, and frequency were also used to summarize the participants’ demographic information and knowledge of infection control practices. An F-test was conducted to examine the relationship between participants’ knowledge of infection control practices and their demographic characteristics. This test compares the mean scores for knowledge of infection control practices between different demographic groups, such as age, gender, and years of experience working in ICUs.
Results
Participants Demographic
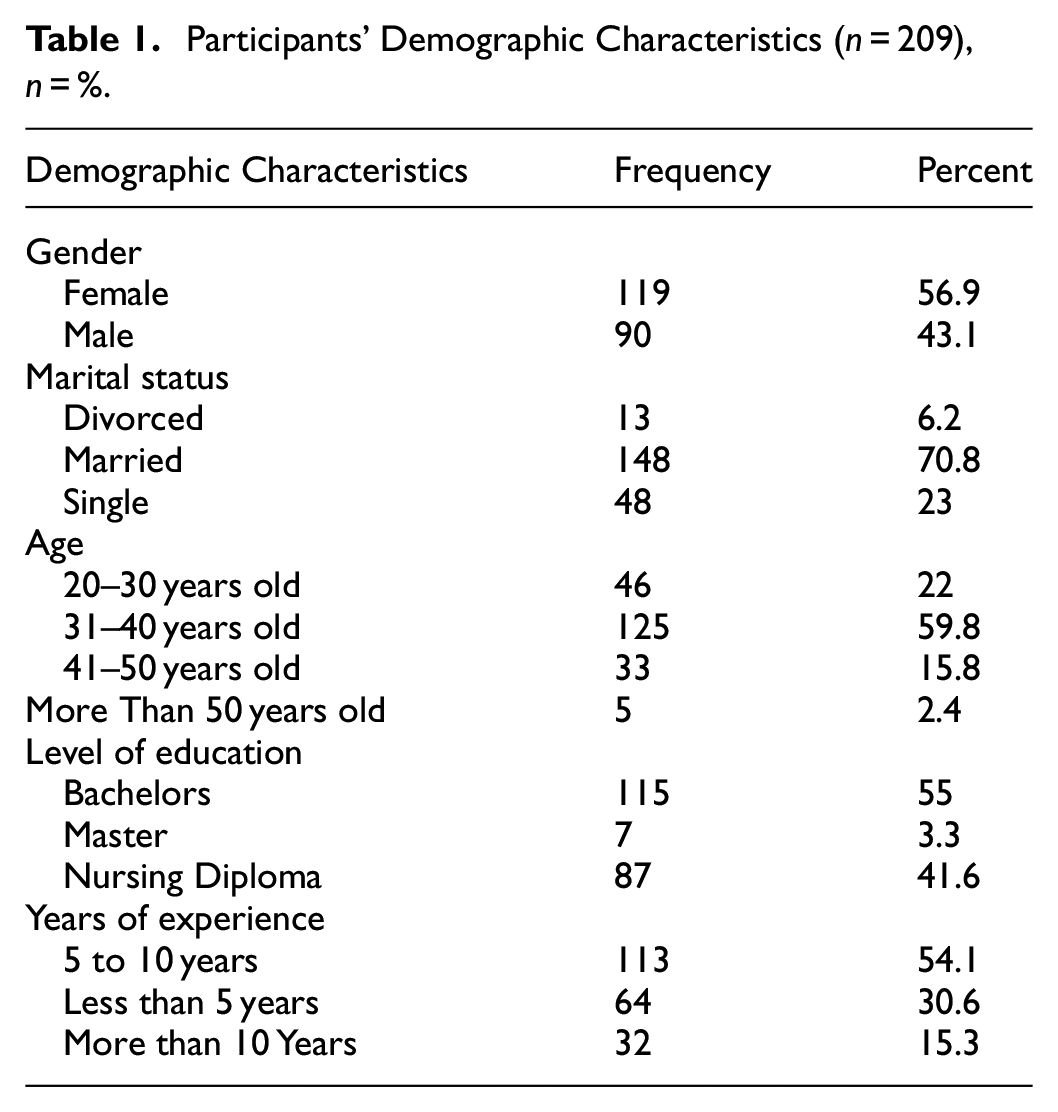
According to Table 1, more than half of the nurses who completed the survey were female 56.9%, while 43.1% were male. Most of the participants reported being married 70.8%, 23% were single, and 6.2% were divorced. Majority of the participants 59% were in the age group between 31 and 40 years. Concerning the nurses’ level of education, most of the participants claimed to have a bachelor’s qualification with 55%, nurse’s diploma with 41.6%, post-graduation 3.3%. Most nurses reported having 5 to 10 years of nursing experience with 54.1%, less than 5 years of experience with 30.6%. Only 15.3% of nurses reported having more than 10 years of nursing experience.
Participants’ Demographic Characteristics (n = 209), n = %.
Knowledge About Guidelines
The construct of knowledge about guidelines contained six items through which the variables of guidelines of nurses were assessed. In the given construct, most participants agreed to its items, such as with a mean value of 0.87 and SD 0.34, participants agreed to attend a training course on infection control. Moreover, with recording the same average value, that is, 0.89 and SD 0.32, most participants claimed in favor of hearing about infection prevention principles. Similarly, participants believe the safety box should be closed or sealed when three-quarters are filled with a mean value of 0.95 and SD 0.21. Nurses also claimed to know how to prepare a 0.5% chlorine solution with a mean value of 0.74 and SD of 0.44. Additionally, participants did not believe there is zero need to change gloves between patients as long as there is zero visible contamination. They recorded a mean value of statement 0.18 and SD 0.38. The lesser mean value indicated that the participant reported a no in response to the item statement. Lastly, participants highly agreed that tuberculosis (TB) is carried in airborne particles generated from patients with active pulmonary tuberculosis and remarked 0.93 mean value and SD 0.23.
Knowledge Regarding Personal Practices
Correspondingly, the construct of nurses’ knowledge regarding personal practices indicated similar outcomes, such that nurses agreed that hand washing is necessary before procedures are performed, with a mean value of 0.98 and SD 0.15. Likewise, nurses also believed gloves should be worn if blood or body fluid exposure is anticipated and remarked a mean value of 0.94 and SD 0.23. Other nurses also claimed that using an alcohol-based antiseptic for hand hygiene is as effective as soap and water if hands are not visibly dirty, with a mean value of 0.89 and SD of 0.32. Moreover, with a mean value of 0.98 and SD 0.15, nurses agreed to wash their hands with soap or use an alcohol-based antiseptic to decrease the risk of transmission of healthcare-acquired infections. Lastly, the same sample size of nurses obtained a mean value of 0.74 and SD of 0.44, while claiming gloves cannot provide complete protection against the transmission of infections. Hence, the more excellent mean value of each item of the personal practices constructs indicated that the participants' agreed ratio in response to the statement was higher.
Knowledge Regarding Disease and Risk Prevention Practices
The results showed that nurses agreed to incinerating or burying used sharp materials with a mean value of 0.75 and SD 0.43. In contrast, nurses disagreed with mixing dry and liquid healthcare wastes and obtained mean and SD values of 0.17 and 0.38, respectively. Nurses also claimed to use all Personal Protective Equipment (PPE) to prevent the risk of acquiring and/or transmitting infection and remarked 0.27 SD value and 0.92 mean value simultaneously. Moreover, the nurses also reported practicing high-level disinfection where sterilization was not applicable, with a mean value of 0.77 and SD of 0.43. Lastly, upon obtaining 0.92 mean and 0.27 SD values, the nurses agreed to apply antiseptic hand rub to clean hands. Overall, the variability in the mean value and SD indicated divergence in the response of nurse participants’ knowledge of the infection control practices in ICUs of Aseer Health Authority.
Assessment of Nurse’s Response
The evaluation of the nurses’ response was done under this analysis. It showed the criteria of nurses choosing between yes and no to each item statement of constructs. Table 2 presented the assessment of nurses’ responses to various statements related to infection control and prevention practices. The responses are categorized as Yes or No, and the corresponding percentages are provided. The first section focuses on the knowledge about guidelines, where most nurses (86.6%) have attended a training course on infection control, and an even higher percentage (88.5%) have heard about infection prevention principles. However, there is a significant gap in knowledge regarding specific guidelines, such as preparing 0.5% chlorine solution (only 74.2% answered Yes) and the need to change gloves between patients (only 17.7% answered yes). Notably, most (93.3%) correctly identified that tuberculosis is carried in airborne particles. The second section assesses knowledge about personal practices, where an overwhelming majority (97.6%) recognize the importance of hand washing before procedures. Similarly, most nurses (94.3%) acknowledge the need for gloves when anticipating blood or body fluid exposure. However, there is a disparity in understanding the effectiveness of alcohol-based antiseptics for hand hygiene (only 88.5% answered Yes). Affirmatively, almost all nurses (97.6%) understand that washing hands with soap or using an alcohol-based antiseptic decreases the risk of transmission of healthcare-acquired infections. The third section evaluates prevention practices, where a significant proportion (75.1%) incinerate or bury used sharp materials, and an even higher percentage (92.3%) use all Personal Protective Equipment (PPE) to prevent the risk of acquiring and/or transmitting infection. However, there is room for improvement in practices such as mixing dry and liquid healthcare wastes (only 17.2% answered No) and applying antiseptic hand rub to clean hands (92.3% answered Yes).
Nurses Response Assessment.

Association Between Participants Demographic Data and Their Knowledge about Guidelines, Personal Practices and Prevention
To gain insights into the differences between study variables such as Knowledge guidelines, personal practices, and prevention among demographics of participants, F-statistics was used. The results are shown in Table 3.
Difference Between Study Variables Among Participant Demographic.

F statistics were found to be significant for the gender, indicating significant differences in knowledge about guidelines, personal practices, and prevention practices between the genders of the nurses (F = 9.78, p-value < .05; F = 13.45, p-value < .05; F = 2.47, p-value < .05, respectively). This indicated that males are more likely to know guidelines, prevention, and personal practices. No evident results were found for other demographic characteristics of the participants, thus depicting no difference in nurses’ marital status and years of experience. However, a slightly significant difference was found for nurses’ age and marital status for knowledge of guidelines and personal practices, while there was insufficient evidence of prevention practices knowledge.
Discussion
Nurses’ knowledge about guidelines, personal practice and prevention were assessed. Under knowledge about guidelines, although the results mostly disagreed by the respondents, nurses comparatively agreed more with the response regarding active pulmonary tuberculosis (mean 0.93 and SD = 0.25), while weak responses were observed on the issue of gloves between patients with (mean = 0.18 and SD = 0.38). Such strongly disagreed outcomes about guidelines were also supported by the previous research by Barker et al. (2017), whose study found knowledge of protocols for HAI prevention in ICUs to be incomplete. Likewise, descriptions of knowledge about personal practice received better results among all. For instance, concerning hand wash received (mean = 0.98 and SD = 0.15). Moreover, none of the responses received less than 0.5 regarding personal practices. Despite such results, the knowledge of guidelines still seems limited, which is agreed by the previous study of Yaseen and Salameh (2015). Lastly, prevention practices have a comparatively high mean value, especially on the usage of personal protection and application of antiseptic hand with values (mean = 0.92 and SD = 0.27). However, the results are far from the mean value of 4, indicating a knowledge gap for prevention practices. This was agreed by Alhazmi et al. (2019), whose study revealed the existence of gaps in the knowledge regarding protective equipment. In general, the average value and standard deviation fluctuations indicated a divergence in how nurse participants perceive their knowledge of infection control practices in ICUs within the Aseer Health Authority in Saudi Arabia.
The study results provided important insights into healthcare workers' awareness of infection control practices in Aseer Health Authority ICUs. Under the complete assessments, 181 responses of Yes were attained while the remaining respondents denied the overall construct with 28 No. Regarding knowledge about guidelines, a high count of yeses was attained for the response to the safety box with 199 Yeses, while the response to the change of gloves received a low number of Yeses. Similarly, under the matter of knowledge about personal practices, a highly accepted response was related to hand washing before procedures, with almost 204 Yeses and only 5 Noes. Lastly, 16 Nos and 193 Yes were received for personal protective equipment under knowledge about personal practices. Overall, the responses concerning knowledge about personal practices received large numbers of acceptance.
Findings of this study showed a significant gender-based differences in nurses’ knowledge about guidelines, personal practices, and HAIs prevention practices (F=9.78, p < .05; F = 13.45, p < .05; F = 2.47, p < .05, respectively). These results followed the outcomes of the study by Barker et al. (2017), which showed a lack of knowledge about the guidelines for infection control among nurses in India, hence the need for more training and education for control practices. However, no significant gender difference was seen in prevention practices (F = 2.47, p > .05). Other demographic factors showed no substantial impact, except for nurses’ age and marital status, which slightly affect knowledge of guidelines and personal practices. Prevention practices' knowledge lacks clear distinctions across demographics.
Study Limitations
Despite the significant findings of the current study, potential limits are being observed. The first limitation is sampling bias. This study focuses only on nurses in the Aseer Health Authority in Saudi Arabia, which might not be representative of the larger population of nurses in different parts of Saudi Arabia. This makes it hard to generalize the results. Secondly, the study relied on a small size of only 209 participants. Because of the small sample size, conclusions may be limited in their applicability to a larger context within Saudi Arabia or other nations. Moreover, the specific characteristics and practices of nurses in the Aseer Health Authority could differ from those in other regions, potentially affecting the external validity of the results.
Implications for Practice, Policy, and Research
Implement comprehensive training programs for nurses that regularly address the most recent infection control recommendations, best practices, and new risks. These programs should be adapted to ICU settings and address specific issues that ICU nurses experience.
Encourage teamwork among nurses, doctors, infection control specialists, and other healthcare providers to facilitate knowledge sharing, best practice integration, and improved communication for better infection control outcomes.
In ICUs, conduct routine audits of infection control practices and give positive comments to nurses. This process helps identify areas for improvement and ensures adherence to established protocols.
Encourage and support research initiatives focusing on infection control practices in ICUs. Research can lead to the development of context-specific strategies and innovative solutions to address challenges.
The launch focused on targeted awareness campaigns to emphasize the significance of infection control practices. To successfully reach nurses, these campaigns might use a variety of channels, including posters, seminars, and internet platforms.
Conclusion
This study assessed the knowledge of infection control practices among nurses working in intensive care units in Saudi Arabia, providing valuable insights into the current state of infection control knowledge and practices among this critical healthcare workforce. While nurses demonstrated a good understanding of some aspects of infection control, such as the importance of hand washing and personal protective equipment, there were significant gaps in knowledge and practices, particularly regarding specific guidelines and prevention practices. Male nurses had more knowledge about guidelines, prevention, and personal practices, suggesting a potential gender-related factor influencing infection control knowledge. Other demographic characteristics, such as age, marital status, level of education, and years of experience, had limited influence on nurses’ knowledge and practices. The study’s findings highlight the need for targeted education and training programs to enhance nurses' knowledge and practices in infection control, particularly where gaps were identified, to ensure optimal patient care and safety in Intensive Care Units in Saudi Arabia. Furthermore, the findings highlighted the importance of ongoing professional development and quality improvement initiatives for maintaining and improving infection control standards. Addressing these gaps and improving infection control knowledge and practices can help healthcare facilities reduce the risk of healthcare-associated infections, improve patient outcomes, and improve overall care quality.
Footnotes
Acknowledgements
The author, Nawal A. Alissa, gratefully acknowledges the support provided by the Ongoing Research Funding Program (ORF-2025-1315) at King Saud University, Riyadh, Saudi Arabia.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by the Ongoing Research Funding Program (ORF-2025-1315) at King Saud University, Riyadh, Saudi Arabia.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data supporting the findings of this study are available from the corresponding author upon reasonable request.