
Abstract
Need for increased awareness of specialized age-related neurocognitive care among nurses is increasing but in Saudi Arabia, awareness of the special needs of and approaches to care for this group remains underdeveloped. To illuminate the needs and perceptions of practicing nurses who have experienced the provision of care to acute patients whose cognition ranged from mild to major cognitive impairment. A qualitative study to inquire into the perceptions of 18 Saudi mental health (MH) nursing graduate students with direct experience of mental health care. Participants were divided into two focus groups which met simultaneously. Inductive data was analyzed for thematic content. Four principal themes and subthemes emerged from the data: (i) roles and responsibilities; (ii) barriers; (iii) the need to improve training; and (iv) support services. Nurses with mental healthcare experience emphasized the importance of roles and responsibility in providing care, barriers to providing care, and dissatisfaction with institutional support and professional training related to age related neurocognitive impairment care in acute settings. This study may assist in providing impetus toward much needed evidence-based research related to age-related neurocognitive impairment, attuned to Saudi needs and may provide an important step in developing and delivering care.
Plain language summary
Opportunities for professional education could be seen as a chance to acknowledge and encourage nurses who work with the geriatric population. These experiences would provide an opportunity to enhance their professional skills and felt needs for career advancement and should be offered to all team personnel. The informational needs of all segments of the community cannot be overlooked. Mass and social of all types need to be used to focus on bringing the condition of dementia into the public forum and promote understanding of its characteristics and the needs of affected patients.
Background
Need
It is estimated that minor and major neurocognitive disorders (designated as dementia previous to DSM-5) will affect 80 and 131.5 million individuals worldwide by the years 2040 and 2050, respectively (Chow et al., 2018; Hugo & Ganguli, 2014; Sleeman et al., 2019). The Lancet Public Health (2022) states that, currently, 57.4 million persons worldwide suffer from these disorders, with 10 million cases being added each year and projected to be 152 million persons in 2050 (WHO, 2022) thus affecting one in three persons aged 85 years or more (National Institute of Health—USA, 2021). Based on these data, the need for appropriate dementia care is steadily growing, especially considering that average lifetimes are rising, thereby increasing the proportion of the population most susceptible to cognitive decline or dementia (Knapp & Wong, 2020; Livingstone et al., 2020).
The worldwide economic cost of providing dementia-related care was US $818 billion and US $1 trillion in 2015 and 2018, respectively (Neubauer et al., 2018). In 2015, although estimated to be four times higher, the total amount expended on dementia care worldwide totaled 1.09% of the global gross domestic product illuminating the critical need to address these conditions (Chow et al., 2018).
Overview of Dementia
Cognitive impairment refers to the loss of previous intellectual functional abilities (Farlex & Partners, 2019) and increases in incidence with advancing age (Leung et al., 2021). Aspects of dementia vary between individuals but are generally identified as having behavioral and psychological symptoms of dementia (BPSD; Laks & Engelhardt, 2008). The Diagnostic and Statistical Manual of Mental Disorders (DSM-5) of the American Psychological Association currently classifies neurocognitive disorders as dementia, delirium, amnestic, and other cognitive disorders and “dementia” has been replaced by classifications “major” and “mild neurocognitive disorder.”
Although ANCI is commonly seen by laypersons as Alzheimer’s Disease, there are other types of age-related neurocognitive disorders. Vascular, frontotemporal, and Lewy body neurocognitive disorders also result in cognitive decline and may be exacerbated by delirium. Treatment of neurocognitive disorders is primarily symptomatic and aimed at addressing and ameliorating the functional deficits observed by clinicians, as well as relieving physiological states that might contribute to cognitive mal-functioning (Hugo & Ganguli, 2014; Javaid et al., 2021; Laks & Engelhardt, 2008).
Theoretical Considerations
The present inquiry used Watson’s Philosophy and Theory of Transpersonal Caring to seek an understanding of the caring needs of patients with ANCI (Peterson & Bredow, 2013; Sitzman & Watson, 2018). Watson and Woodward (2020) have suggested that human caring can be linked with knowledge, engagement between individuals, empathy, and translated into developing and sustaining helping, trusting, and authentic caring relationships. This holistic focus on care is at the heart of the patient-centric paradigm and focuses on maintaining or enhancing patients’ quality of life (Fazio et al., 2018). Thus, it is important that curriculum and training for professional nurses include these caring attitudes and competencies (Bauer, 1990; Dyess et al., 2010).
ANCI in Saudi Arabia
Individuals over 60 years of age account for 5.2% of the population of Saudi Arabia (Alkhunizan et al., 2018; Khoja et al., 2017). Based on demographic projections, it is projected that this population segment will comprise 9.5% and 18.4% of the total Saudi population by 2035 and 2050, respectively (Khoja et al., 2017). Based on a study of Saudi community-based primary care outpatients aged 60 years or older, the rates of ANCI were identified to be 38.6% (mild) and 6.45% (major), respectively, although a 70% illiteracy rate among this group may mediate the results of the assessment, (Khoja et al., 2017), resulting in over-estimation of functioning cognitive impairment if testing involves any aspect of literacy skills (Yaghmour et al., 2018). In comparison, the estimated prevalence rates of ANCI worldwide for people over 60 years of age are estimated to be mild and major 5% to 7% and 10% to 20%, respectively (Alkhunizan et al., 2018). Lebanon, a neighboring state, has reported ANCI of all types to be 7.4% among those 65 years or older lending credibility to the Saudi data that estimate a 6.45% incidence rate for major ANCI for that age range (Alsebayel et al., 2022; Phung et al., 2017).
Saudi Patterns of Elder Care
The normative structure for elder care in the Middle East and North Africa Area (MENA) region relies heavily on home-centered care provided by family members (Phung et al., 2017; Yaghmour et al., 2018). Paid assistants provide daily living care to 21 % of elderly people with disabilities (21%), but in most cases (86.5%), home-based elder care is the normative pattern (Phung et al., 2017; Yaghmour et al., 2018) Institutional elder care facilities are limited in number and size, are maintained for indigent, homeless persons without living relatives, and not intended for general use by the population (Hamid, 2018; WAQAR, 2021). Thus, age-related cognitively impaired patients are most commonly in contact with nurses during hospitalization in a critical care facility with a plan for discharge to the home setting upon stabilization.
Care to elderly patients is predominately based on the medical model which emphasizes the physical care of patients. However, delivery of holistic care by medical care professionals working with elders suffering from high acuity and multiple noncommunicable conditions including ANCI is not emphasized (Alswaidan, 2019; Jensen et al., 2019; Kadri et al., 2018; Reilly & Houghton, 2019).
Professional ANCI Care Providers
Healthcare providers in Saudi Arabia are a diverse group, with the vast majority being foreign migrants. In 2018, Saudi Arabia had a total of 184,565 nurses, of which 70,319 (around 38%) were Saudi citizens (Alluhidan et al., 2020). The remainder of the foreign nurses working in Saudi Arabia have come from the Philippines, India, Egypt, Jordan, South Africa, Uganda, Malaysia, the UK, the US, and various other locales.
Each of these nurses belongs to an ethnic group with its own culture, philosophy, and language. In addition to learning about Saudi culture to provide culturally competent care to ANCI patients, they need to learn about each other. Difficulties are encountered with patient care and communication between healthcare providers, patients, their families, and each other (Aldossary et al., 2008). Although they may be competent in caregiving skills, they may not be prepared to communicate with and understand the culturally, socially, and religiously based needs and behaviors of patients, thereby limiting their ability to provide holistic care to them.
When available, indigenous healthcare providers are well acquainted with local cultural and religious patterns and are prepared to provide culturally congruent care (Aldossary et al., 2008). However, indigenous healthcare providers may be limited by inadequate preparation in ANCI care during their professional training because gerontology and the care of patients with ANCIs has only quite recently been included in the curriculum of undergraduate and graduate nursing programs (Asarnow & Miranda, 2014; Princess Nourah Bint Abdulrahman University, 2018; Wortzel et al., 2013; Yaghmour et al., 2018).
Family Caregivers
Study of the role of caregivers has not been widely explored in Saudi Arabia, with only one study being found. Alfakhri et al. (2018) reported on caregiver stress based on a cross-sectional study of caregivers of patients receiving care in a Saudi university-based hospital. The results of caregiver MH characteristics have yielded depression rates of 43.2%, 20.3%, and 10.4% for mild, moderate, and moderate to severe incidence while caring for ANCI patients who are classified as mild (22%), moderate (34.9%), and severe (43.1%) in impairment respectively. These data are largely in agreement with those of other locales but may be mediated by the demographic profile of the caregiver. The highest frequency of caregiver characteristics was relationship (mother/father), age (average 46.4 years), gender (60% female), and employment status (70.7% employed). Depression was found to be more likely when caregivers were children of patients compared with others who provided this care (Alfakhri et al., 2018).
Stigma and Attitude Toward ANCI in Saudi Arabia
Care for patients affected by ANCI may be influenced by the cultural and social orientations of their caregivers, families, and society at large (Fogg et al., 2018; Tropea et al., 2017). In a survey of attitudes concerning Alzheimer’s-type ANCI in Jeddah, a large Saudi metropolis, 89% of the participants from a sample of the general population had heard of this condition, while 45% and 46%, respectively, believed that it was a normal part of aging or brain disease (Algahtani et al., 2020). Saudi medical and dental students identified Alzheimer’s disease as a neurodegenerative disease 73.5% of the time and 70.1% acknowledged that study of this condition had been included in their undergraduate curriculum (Arifi, 2020). However, Saudis studying internal medicine failed to successfully recognize and manage geriatric syndromes, including ANCI, at 63 and 67% of the time, respectively and underestimated delirium and undertreatment for pain 49 and 64% respectively (Arifi, 2020).
The basis of local customs in caring for the elderly is rooted in religious and tribal concepts of mutual support and cohesiveness supplemented by religious foundations which intersect with them. Application of these precepts stigmatizes members of the tribe who fail to provide care for members of their group (countrystudies.us, 2014; Dhami & Sheikh, 2000). When Prophet Mohammed (pbuh) was asked about medical care he replied: “Yes, you should seek medical treatment, because Allah, the Exalted, has let no disease exist without providing for its cure, except for one ailment, namely, old age” (Al-Eisa, & Al-Sobayel, 2012) and healthcare is considered a right of the living body which the soul inhabits (Musaiger et al., 2011; O’Brien, 2017) dictating that it is appropriate to address any form of illness with benevolent care. Care of the elderly is firmly rooted in faith by Prophet Mohammad (pubh). When asked about the status of parents: “Who has the greatest right that I should keep company with him with goodness?,” he said, “Thy mother.” And when asked again: “Who then?,” he said, “Thy mother.” And asked again: “Who then?,” he said: “Thy mother.” Finally: “Who then?” he said, “Then thy father” (The Hadith: Bukhari, n.d. 78:2).
Aim of the Study
In lieu of evidence-based research (EBR) focused on healthcare system efforts to address holistic ANCI care for the inpatient population in Saudi Arabia, a qualitative inquiry was designed to illuminate the perceptions of practicing nurses who have experienced caring for patients with ANCI diagnoses in the milieu of Saudi society and the healthcare system.
Method
Study Design
A qualitative descriptive design aimed at exploring the experience of providing nursing care to hospitalized patients affected by ANCI. A qualitative approach is ideal for gathering information in areas that have not been quantitatively explored before (Romm, 2020; Schulenkorf et al., 2020). Focus groups can offer over 80% of emergent themes relating to a specific subject (Guest et al., 2017), providing an understanding of jointly held opinions and a diverse selection of perspectives (Davis, 2019; Nyumba et al., 2018).
Participants and Setting
The participants were 18 professional female Saudi Arabian MH nurses ranging in age from 27 to 40 years engaged in postgraduate study with at least 5 years of direct patient contact practice in delivery of inpatient care. All other volunteers were excluded from participation.
Recruitment was carried out through an advertisement posted by the researchers in the nursing college and by use of the snowball method. The participants were invited to contact researchers aimed at establishing a focus group to discuss ANCI care. Moderators of the groups were university faculty members not engaged in direct teaching of these students.
Ethical Concerns
The study protocol was approved by the affiliated university’s institutional review board. After receiving information about the study, all the participants gave their written informed consent including permission to record the proceedings of the focus group meeting. All the participants were informed of the opportunity to withdraw from the research at any point without consequence. All data including digital data, anonymized transcribed narratives, and informed consent were stored in a locked facility.
Data Collection
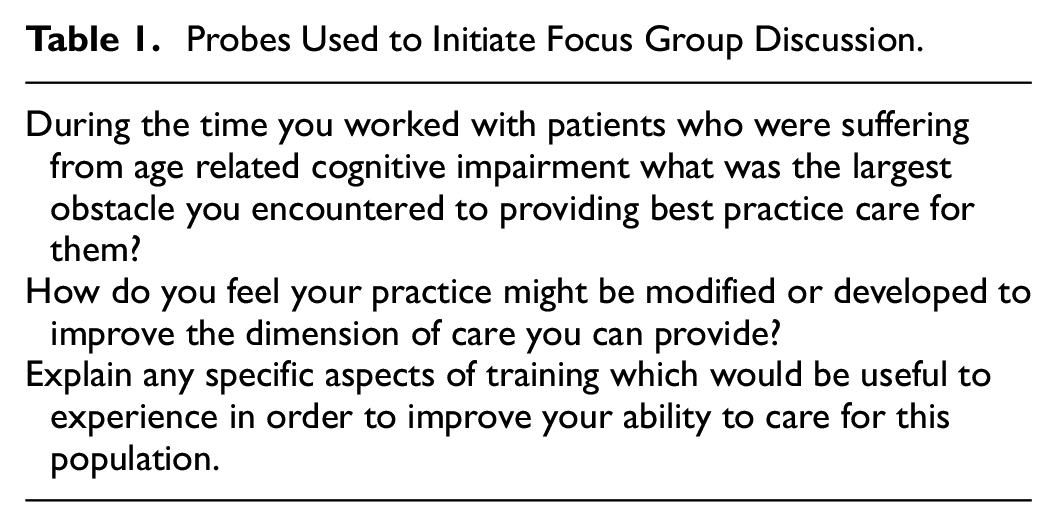
Participants were divided into two focus groups of nine members which met simultaneously in a conference room of the college for approximately 2 hr. The focus groups started with a semi-structured format of probes, which were subsequently modified to utilize theoretical sampling as inductive data emerged. The questions posed by the moderators probed the nurses’ experiences of providing care for patients with ANCI, aiming to understand the nurses’ roles, experiences of previous training, and gaps in their knowledge, along with their personal worries, perceptions of obstacles, and feelings experienced in the clinical setting. Table 1 is a display of the probes employed to initiate the meetings.
Probes Used to Initiate Focus Group Discussion.
Saturation was signaled by cessation of production of new inductive data. Member checking was employed to clarify the data at conclusion of the sessions. Digital data was transcribed to a WORD document and anonymized. Transcripts, digital records, and field notes were stored in a locked location.
Data Analysis
Inductive codes were evaluated with the assistance of NVivo software version 10.1 (QSR International, Doncaster, Victoria, Australia). Output from the software was reviewed for the primary themes that emerged and were organized by the researchers into a comprehensive framework that represented the final principal themes.
Rigor
By conducting semi-structured interviews and unstructured dialogues, a detailed understanding of the participants’ opinions, perceptions, and subjective interpretations was obtained. The researchers conducted an evaluation of coding classifications. Formulation of themes was assisted by two peer faculty researchers. Trustworthiness including dependability and credibility of the data was built on participant experience in the MH clinical setting and professional nursing status. Peer checking, member checking and reflection were employed to further enhance credibility and dependability. Audit trails and researcher field notes were employed to provide confirmability. Transferability of conclusions and recommendations for future practice may be addressed by considering the characteristics of populations of interest.
Findings
Following the transcript analysis, four principal themes emerged from the data: (i) roles and responsibilities; (ii) barriers; (iii) the need to improve training; and (iv) support services.
When replying to probes the participants talked about their previous involvement in pertinent training opportunities, their experience in caring roles, and the nature of their links with the multi-disciplinary healthcare team and healthcare structure.
Theme One: Roles and Responsibilities
Consensus arose among the participants that managing and encouraging other personnel was a major task. The participants perceived that their responsibilities were extremely complicated within settings where there was not much support, they felt alone, and poor levels of esteem were attached to their practice. Lack of collegial supervision from nurse managers was a concern of most of the group. Several participants were unhappy about having to abandon the empathetic patient-centric aspects of nursing because of time constraints: Nurses are mainly involved in delegating duties to others and don’t have time to interact with the patients. (Participants 7, 12, and 15) It is very difficult to individualize patients because many are past the stage where they can have a conversation and express their concerns and needs. [Participants 4, 10, and 15] We need someone who can mentor us and help us through rough patches [Participant 6]
The emphasis on tasks and management resulted in several nurses remorsefully stating that they felt that they had lost their caring abilities and opportunities to give care. This was expressed by several nurses as follows: It can be wretched, with the nursing job requiring a lot of documentation and legal work. Unhappily, we do less nursing and cannot attend to the patients as we would like. [Participant 11] The mechanics of keeping records and custodial care goes on whether or not dementia is present. [Participants 3 and 9)
Being unable to be part of the patients’ practical care appeared to give rise to weaker personal engagement with patients, the medicalization of patient care, and an erosion of caring skills and activities: It is challenging to know how to respond. I perceive that we are losing the ability to engage with the patients and make them aware that there really is someone there who cares about them. [Participant 5 and 11] We don’t get an opportunity to give them a feeling of well-being. This leads to more behavioral problems. [Participants 9, 18, and 12]
Theme Two: Barriers to Caring
The participants felt that opportunities to attain professional development or specialist status were absent, despite their desire to gain knowledge and improve their skills and status: I consider that most of the time, there is no special educational requirement for the kind of care we give. However, I would hate to feel awkward about being a bit ungainly and slow in getting ready. [Participant 16] Nothing we learned in our courses prepared us for what we must do for these people. [Participant 1] At times, I was required to take part in a course to improve my skills, but I also had to go to my job. There was no compensation for the time spent nor reward for participation such as advancement. I was so fatigued that I failed to manage all my responsibilities, so I had to give up at that point. [Participant 4] When you engage with e-learning you don’t get a chance to apply it. [Participant. I attempted to get involved with this online learning, but it was mostly videos and discussion sessions, and did not address our needs adequately. We need additional resources or workshops. [Participants 6, 18, and 15]
When we participated in this type of learning, we were not given recognition, credit, or a change in status so it just wasn’t worth the trouble. [Participants 2 and 14]
Some participants expressed empathetic reactions toward negative attitudes of nurses toward patients and their families when discussing patient behavior. Several of the group felt that it set a negative climate in the work setting: I try to consider ways to deal with difficult attitudes toward patients and their families, such as hostility, but the staff members require education. [Participant 2] Several of us are not able to engage with the patients and their relatives in satisfactory ways, and we don’t know how to cope with that. [Participants 15 and 16] Individuals suffering from dementia can no longer express themselves adequately. How can we talk with them? [Participant 9]
Theme Three: Improve Training
The study participants were offered the opportunity to voice their views on their acceptance of planned future education aimed at improving their readiness to address patients’ needs. Over half of the group expressed the view that communicating with patients and their families was difficult and needed to be addressed through additional workshops.
Relatives appeared to need empathy from the nursing staff. When relieved of the task of routine daily care given to patients at home, family members took on a new job of double-checking the actions of the nursing staff during care, which resulted in resentment and occasional unpleasantness or even violence.
Several nurses are challenged when it comes to talking to families, and it can be a very delicate matter. We need some orientation in this area. [Participant 13] I think this is another talent or skill that would assist and encourage nurses to manage hard discussions because some nurses are worried by this. [Participant 8]
At least half of the study participants noted the importance of education and information sharing being accessible to all personnel involved in ANCI care, irrespective of their clinical role. Many of the non-professional staff which are involved in providing custodial care are untrained and need a different type of training than the nurses. This gap places an added burden on the nurses who are responsible for supervising the caring activities of this group in addition to their own duties.
These workers they send to us are just not well enough trained to be providing patient care, especially to some of our patients who are not able to speak out for themselves. This affects patient physical safety. [Participant 1]
This situation puts more strain on the nurses who supervise them to assure that the necessary custodial work is being performed. [Participant 9]
Nurses note that much of their training is the result of informal processes such as contact with personnel from other settings: If you are in a group, you meet other staff from a range of settings, and when you are talking among others, you learn from what you hear [Participant 18] I feel that when carers are working on an identical job, uniformity in communication is more constructive. [Participant 12]
Other participants believed that learning experiences from their caring experiences rather than structured learning experiences had a very important instructive role.
We are discussing the need to be pragmatic; we are giving care to patients with dementia, which requires a hands-on approach. [Participant 3]
Theme Four: Support Services—Multidisciplinary Team
As already implied, patient care in critical care hospitals, clinics, and other palliative facilities that treat patients with ANCI and associated cognition disorders is fragmented and non-cohesive. In principle, a holistic approach to patient care should be offered in these settings, but the nurses had failed to find this in practice as members of the multidisciplinary care team.
There are hospitals where dementia is not even considered in the SBAR assessment and planning activities. This means that the patient may be admitted to a ward in the hospital when their mental state is not considered in the treatment plan. [Participant 4] This is an especially critical consideration when the patient is diagnosed as terminal. [Participants 2 and 17]
Participants overwhelmingly shared the opinion that they need to work as a team to ensure that the emergent requirements of the patient and family were being provided: It is about continuity between the major institutions and hospitals, to facilitate holistic terminal care to patients and their families. [Participant 16] It is not only about healthcare; it incorporates social and out-of-hospital care teams to offer a good standard for individuals with dementia. [Participant 8] If the nurse shows empathy, additional disciplines must recognize that. At the end of the day, nurses are a unified body that should work in concert, not just individually. [Participant 13]
As anticipated, the participants noted that the interaction of sectors of the multidisciplinary team did not have the same connotations for everyone. The best way suggested to serve patients with ANCI in accordance with their conditions was expressed by the participants as the smooth “joining up” of healthcare and development of structured patterns of interaction and cooperation between professionals to optimize both intra- and interorganizational communications to provide holistic care for patients at the end of life. This joining was envisaged as multidisciplinary teamwork across the general and specialist clinical sectors to achieve good care with mental health nurse practitioners (MHNP) fulfilling an indispensable role in addressing needs of patients and their families.
Discussion
Holistic nursing is aimed at meeting patients’ physical, mental, social, and spiritual requirements (Whitlatch & Orsulic-Jeras, 2018). ANCI may precipitate a situation of crisis in which there is mental and spiritual pain and distress (Hirakawa et al., 2020). Nurses often presume that they offer a holistic nursing approach but frequently confess to knowing little about how to meet their patient’s overall requirements (Kilpatrick et al., 2020), particularly in the case of individuals suffering from ANCI (Hirakawa et al., 2020).
Roles and responsibilities of MH care nurses need to be recognized as a professional specialization. Guidance for codification of this professional role may be guided by international nursing organizations and judicious consideration of the needs of the local population. The Institute of Medicine (2011) emphasized that PMHNs should be active members of the care team, striving to improve inefficient and harmful systems of care and to work as full partners in the design of health care. This recommendation implies that nurses not only work with physicians and other health care professionals, but that they also actively provide input and implement change in their sphere of professional influence. Nurses need to be oriented toward understanding and meeting the unique problems related to caring for patients with ANCI conditions.
Currently, psychogeriatric or geriatric nursing may not be sufficiently identified in Saudi Arabia as a specialty in the profession of nursing. Course content has very recently been implemented for Saudi nursing curriculum (Princess Nourah Bint Abdulrahman University, 2018), but foreign nurses of various nationalities may have a wide range of beliefs, practices, and competencies which comprise their ability to provide ANCI to satisfactory levels. The presence of these inconsistencies points to the need for training initiatives for all practicing nurses to receive comprehensive training and orientation in ANCI care practices to achieve consistent MH caring competencies.
Addressing Barriers to the Provision of ANCI Care by PMHNs
In the current study, many participants were required to manage other personnel. This resulted in distance between themselves and the patients in their care. The nurses were increasingly required to work in administrative positions, thus limiting their opportunities to interact with individual patients. Consequently, the participants felt that their skills in direct care were gradually becoming degraded and deteriorating, without having the opportunity to improve and develop professionally for themselves and their staff. This situation may exacerbate stress, emotional exhaustion, and dissatisfaction, as well as reducing nurse effectiveness (Aldossary et al., 2008; Alreshidi et al., 2021; Al-Turki et al., 2010; Felemban et al., 2014).
Focus group participants acknowledged the requirement for hands-on, practical educational resources to deal with deficiencies in their skillsets; they mentioned needing assistance in developing skills in communicating well with patients and their relatives and reacting appropriately in stressful situations (Alyousef & Alhamidi, 2022). As demonstrated in this work and the paper by Scerri et al. (2020), methods to resolve these issues are complex but can be effectively addressed if a coordinated approach with healthcare providers and patients’ families can draw on the knowledge the family members have in addressing patients’ individual needs (Palmer, 2012).
Numerous experiences and hindrances to providing high-quality nursing care to patients affected by ANCI were recognized in the focus group; these potential barriers may originate from organizational impediments throughout the healthcare system to adequately address ANCI care as a discrete entity. This situation may be because of communication and interaction failures among differing healthcare disciplines, low levels of academic and clinical preparation for this type of care among healthcare providers, and difficulties in the systemization of services.
Patient Care Issues
Patients suffering from ANCI are rarely consulted regarding their own care. Although this may be true of those suffering from major neurocognitive disorders, patients who are in the earlier stages of ANCI need to be individualized during planning for their care.
Staff, families, and the community require education and training regarding assistance with activities of daily living and palliative care for patients who cannot advocate for themselves (Beck et al., 2016; Van der Steen et al., 2016). Education that can motivate advance care planning among patients and their families which would dictate the way they wish care to be delivered may add to enhanced satisfaction among all types of care providers, including professional nurses, custodial caregivers, families, and the patients themselves, which can be done by encouraging them to develop individualized, culturally competent care plans. This assumption of shared decision making and cooperation for ANCI care among patients, their families, healthcare providers, and the community may provide higher satisfaction in all sectors and less discord during the interactions between them (Alsaleem et al., 2018; Beck et al., 2016; Lai et al., 2019).
Multidisciplinary Approach
The participants’ emphasis on the need for a multidisciplinary approach to care for patients with ANCI that includes all members of the healthcare system echoes the findings by Beck et al. (2016) in the UK for their NICE protocols; these protocols emphasize cooperation between all persons who participate in ANCI care mapping in caring for ANCI patients. This process is intended to include all involved parties, including patients who are able, aiming to provide highly individualized care plans based on specific patient needs and preferences. There is also recognition that planning and training are not sufficient for a satisfactory outcome without organizational support use of EBR in instituting change, recognition to staff and caregivers for achieving an improvement of care quality.
To this end, the Saudi Arabian Ministry of Health (2024) has launched an initiative in elderly care that includes specialized training that can improve skills and competencies, including workshops and training courses for elder care teams employed in the healthcare system using EBR to serve in designing viable care options. Furthermore, universities have begun to add geriatric care to the curricular requirements for professional nurse training signaling its importance for addressing emerging needs to meet demographic changes in the Saudi population (Princess Nourah Bint Abdulrahman University, 2018).
Recommendations
Because of the presence of ANCI in the general patient population, nurses in all areas of practice need to be equipped to successfully interact with patients with ANCI and their loved ones. Based on the environment of ANCI care in Saudi Arabia, initiatives need to focus on improved outcomes based on the following:
○ An effective assessment of individual patient status and care needs, along with the implementation and evaluation of person-centered, individualized care (Karrer et al., 2020; Lee et al., 2020);
○ Empowerment of the patient’s family in providing appropriate care through caregiver education (Bahrami et al., 2019).
○ An increase in physical comfort based on assessed need and avoidance of excessive restraint (Bahrami et al., 2019; Brown et al., 2020; Hamers & Huizing, 2005).
○ Fostering efforts to maintain dignity and self-realization through encouraging autonomy, participation as far as able, and sensitivity to individual patient wishes (Brown et al., 2020; Hedman et al., 2019; Nygaard et al., 2020).
○ Monitoring of medications with the goal of minimizing polypharmacy and introducing protocol-based prescribing (Salih et al., 2013);
○ Recognition of pain in patients who are unable to advocate for themselves and establishing systematic and objective protocols for administration of pain medication (Alswaidan, 2019; Parkman et al., 2021; Starr & Magan, 2020).
○ Implementation of EBR when designing care planning, facilities, provision of funding, and staff training for ANCI care (Karrer et al., 2020).
○ Specialized training for ANCI care in continuing, undergraduate, and graduate nursing education curricula, including the initiation of geriatric nursing specialties that comply with the recommended competencies of the American Association of Colleges of Nursing (AlSenany & AlSaif, 2014; American Association of Colleges of Nursing, 2010; Kuening-Plantigna et al., 2020).
○ Research of ANCI related care is very limited in the Middle East. Although the Eastern Mediterranean region is generally considered a high-income area of the world, budgetary allocation for MH care is low. This restricts development of specialized ANCI care based on EBR which would illuminate ways to develop best practices in this region (Alsebayel et al., 2022; Elyamani & Hammoud, 2020).
Limitations
The data gathered in the present study were provided by a focus group of nurses who have provided care for patients with ANCI and their families in acute care settings in Saudi Arabia. All the participants were female because of mandatory gender separation in educational settings in Saudi Arabia and may affect outcome if a mixed gender inquiry is made. Additional studies with increased numbers of participants and additional methods of gathering and examining data may illuminate the results of this study or add additional outlooks. The transferability of conclusions to other populations may require careful examination of demographic, social, and cultural congruence with the group studied.
Conclusions
The nurses in the current study, from a range of clinical situations, emphasized the importance of the roles and responsibility in providing care, barriers to the provision of care, and dissatisfaction with institutional support and professional positions in ANCI care in acute settings. Sources of barriers to providing high quality ANCI care were identified by participants as paucity of EBR included poor professional preparation, low levels of awareness of incidence of ANCI, the stigma of ANCI in the community and among healthcare professionals, and low levels of cooperation between sectors within the healthcare sectors.
Professional preparation in principles of geriatrics and ANCI care based on EBR among healthcare providers has recently been added to university curricula and continuing education programs in Saudi Arabia. Yaghmour et al. (2015) found that practicing nurses, although confident in their skills in identifying and managing depression, expressed the need to be better prepared to deal with patients suffering from delirium and ANCI. The need to provide care to demented patients and their families in acute settings is an area of ANCI care that has not been widely addressed in EBR and may require further attention.
Worldwide, many locales depend on long-term institutional care in nursing care centers, which are especially designed to meet the needs of patients with ANCI. However, the focus of ANCI care in Saudi Arabia is different, with the normative pattern of care for this type of patient is provision of care in private homes. In this setting, care is provided by family members or paid attendants. Skills required by caregivers in the environment of private homes may be considerably different. This framework for the provision of care for patients with impaired executive function has not been frequently explored, and further attention to the care needs of this group may benefit healthcare providers, patients, their families, and the community at large because a large number of citizens in the Arab Gulf area and perhaps elsewhere are being affected by demographic changes, such as extended life expectancy, decreased numbers of families living in extended living arrangements, and lower birth rates thus decreasing availability of caregiving family members thereby perhaps causing changes in ANCI caring patterns which may need to be considered through the lens of EBR.
The provision of opportunities for professional education could be seen as a chance to acknowledge and encourage nurses who work with the geriatric population. These experiences would provide an opportunity to enhance their professional skills and perceived needs for career advancement and should be offered to all team personnel.
The informational needs of all segments of the community cannot be overlooked. Mass and social media of all types need to focus on bringing the condition of ANCI into the public forum, modifying the stigma, and promoting an understanding of its characteristics and the needs of patients and their families who are affected.
Footnotes
Acknowledgements
We thank King Saud University for its cooperation in making their facilities available for us during the study.
Accessible Summary
Opportunities for professional education could be seen as a chance to acknowledge and encourage nurses who work with the geriatric population. These experiences would provide an opportunity to enhance their professional skills and felt needs for career advancement and should be offered to all team personnel.
The informational needs of all segments of the community cannot be overlooked. Mass and social of all types need to be used to focus on bringing the condition of dementia into the public forum and promote understanding of its characteristics and the needs of affected patients.
Worldwide there is widespread dependence in many locales on long-term institutional care in nursing care centers specially designed to meet the needs of dementia patients. However, the focus of dementia care in Saudi Arabia is different, with the normative pattern for this type of patient being the provision of care for them in private homes. In this setting, care is provided by family members or paid attendants. This framework for the provision of care for patients with impaired executive function has not been frequently explored, and further attention to the care needs of this group may benefit healthcare providers, patients, their families, and the community at large as numbers of citizens in the Arab Gulf area and perhaps elsewhere are affected by demographic changes such as extended length of life, decreased numbers of families living in extended living arrangements, and lower birth rate.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Data Availability Statement
Data is available upon request from the corresponding author.