
Abstract
This study utilizes the demographic metric of Literate Life Expectancy (LLE) to evaluate Vietnam’s 70-year journey of social development across birth cohorts. By analyzing the Life Table (2019) and Age-specific Literacy Rates (2020), the magnitude of the gap in LLE between women and men is calculated to provide insights into the progress of healthcare initiatives and literacy improvement. A narrow women-men gap in LLE indicates a society with higher mortality rates and a significant literacy gap between women and men. Conversely, a wide women-men gap in LLE illustrates a society with lower mortality rates and apparent gender equality in literacy. Findings reveal three distinct stages of social development in Vietnam. Stage 1 (1935–1945) indicates LLE for women being lower than that of men which reflects slow pace of social progress during colonization. Stage 2 (1945–1975) illustrates LLE for women surpassing that of men, marking developing social progress after Vietnam’s declaration of independence from colonization. Stage 3 (1975–2004) shows a widening women-men gap in LLE, reflecting rapid social development with revolutionary reforms in healthcare and education after the Vietnam War. The discussion section outlines a compilation of basic education and primary healthcare policies corresponding to stages of social development in Vietnam.
Plain language summary
This study examines how social development in Vietnam has changed over the past 70 years by looking at different generations. We use a measure called Literate Life Expectancy (LLE), which combines life expectancy with literacy rates, to understand these changes. By analyzing the differences in LLE between women and men, we can explore Vietnam’s social development across generations, which corresponds to historical milestones. A small gap in LLE between women and men suggests higher mortality rates and a large difference in literacy between genders, while a larger gap indicates lower mortality rates and better gender equality in literacy. Our findings show three stages of social development in Vietnam: Stage 1 (1935–1945), during which LLE for women was lower than LLE for men, indicating slow progress during colonization; Stage 2 (1945–1975), when, after gaining independence, LLE for women surpassed LLE for men, showing developing social progress; and Stage 3 (1975–2004), where the gap between LLE for women and LLE for men widened, reflecting rapid social development with significant improvements in healthcare and education following the Vietnam War. The study also discusses various education and healthcare policies that correspond to these stages of social development in Vietnam.
Keywords
Introduction
Prominent research on measuring social development has extensively applied physical quality of life index (PQLI) (Morris, 1978), human development index (HDI) (Sagar & Najam, 1998) and social development index (SDI) (Mazumdar, 1996). While these indicators require a large amount of information, complicated mathematical calculations and are used for cross-country comparisons, the emerging demographic indicator to assess social development, which is simplified and utilized for within-country and gender analysis, is called literate life expectancy (LLE). LLE was introduced by Professor Wolfgang Lutz for measuring social development and it is defined as the “average number of years a man or a woman lives in a literate state (i.e. the ability to read and write) under current mortality and literacy conditions.” This indicator is a composite indicator that combines life expectancy and literacy to create a single summary measure, therefore, it is computed by using specific data sets related to age-specific mortality rates (for life expectancy) and age-specific literacy rates (for literacy). LLE is advantageous in being clear, reflective of real-life experiences of individuals, applicable for future projection, and standing alone in absolute value over a period of time (Lutz & Goujon, 2004).
Vietnam, a lower-middle-income nation with a notable milestone of approximately 100 million population in 2024 (Population Pyramid, 2024), has experienced a special social development corresponding to historical periods which is marked by a series of significant events such as colonization (Nørlund, 1991), declaration of independence from colonization (Katsiaficas, 2016), Vietnam War – one of the most brutal and controversial military conflicts in 20th century (Duong, 2023), and the North-South reunification of the country (Ang, 2005). Previous studies about social development in Vietnam have concentrated on review policies and process of changes (Dinh, 1999), the intersection with history, education and political economy (Huong & Fry, 2004), as well as socio-economic points of view (Kien & Heo, 2008). In recent years, Vietnam has primarily utilized the Human Development Index (HDI), which includes data on life expectancy at birth, expected years of schooling, mean years of schooling, and gross national income per capita, to compare itself globally (United Nations Development Programme, 2018). In general, these indicators or measurements necessitate extensive data and complex mathematical computations to assess economic and social development simultaneously. As far as the authors are aware, no research has specifically explored the use of demographic tools to evaluate social development in Vietnam independently of economic factors.
To address the research gap, this study adopts a straightforward measurement approach, utilizing a purely demographic analysis to assess Vietnam’s social development, as previously mentioned. Rather than relying on complex indicators and methodologies, this measurement method is uncomplicated, as it utilizes literacy and life expectancy—two fundamental and well-defined indicators. It captures the basic education and the survival of individuals to a specific age to examines the women-men gap in Literate Life Expectancy (LLE) across birth cohorts to evaluate social development over Vietnam’s 70-year timeline. This period encompasses key historical phases, including colonization, the declaration of independence, and revolutionary reforms in healthcare and education following the Vietnam War. A narrow women-men gap in LLE reflects lower social development, characterized by higher mortality rates and significant gender disparities in literacy. In contrast, a wider gap indicates higher social development, marked by lower mortality rates and greater gender equality in literacy. Utilizing the latest data from the 2019 Vietnam Life Table provided by the World Health Organization and age-specific literacy rates from 2020 by the Vietnam General Statistics Office, the study aims to provide insights into using a demographic indicator to comprehensively understand Vietnam’s social development over time. Furthermore, the study discusses a range of fundamental education and primary healthcare policies to explain each stage of Vietnam’s social development.
Research Questions
This research aims to address two key questions: (1) How does the trajectory of the women-men gap in LLE vary across birth cohorts, thereby reflecting Vietnam’s social development across historical milestones? (2) What are the principal educational and primary healthcare policies associated with the stages of social development identified through the women-men gap in LLE in Vietnam?
Literature Review
The Global Application of Literate Life Expectancy
Literate life expectancy (LLE), introduced by Professor Wolfgang Lutz in 1995, is utilized to primarily assess social development from demographic perspective based on two basic aspects of the standard of living which are life expectancy and literacy. It is different from traditional indicators for measuring socioeconomic development like Gross Domestic Product (GDP) per capita and HDI which include economic components. The great advantages of LLE are straightforward calculation based on ordinary life table technique and readily available data sources for age-specific mortality rates and age-specific literacy rates. Regarding its application, LLE was constructed across genders and birth cohorts from 1970 to 2005 for more than 50 developing and industrialized countries, and the projection of LLE to 2030 was made for 13 world regions to illustrate social development (Lutz & Goujon, 2004). In Mexico, the examination of LLE was utilized for national context analysis, regional approach and state-level analysis (Medina, 1996). In India, LLE was employed to assess social development in major states of India and gender differences in both rural and urban regions, and make comparison with HDI (Chattopadhyay & Sinha, 2010). Besides, LLE was also applied to measure social development in China (Huang & Nanjo, 1998), invent dynamic literate life expectancy in India (Sharma, 2018), illustrate gender differences in LLE between rural and urban regions in Bangladesh (Khan & Asaduzzaman, 2007), compare social development for specific age groups between 2 years based on LLE (Rahaman Khan et al., 2016) and measure the potential of demographic dividend in Pakistan (Nasir et al., 2013).
The Vietnamese Context of Life Expectancy at Birth and Literacy
Before calculating literate life expectancy in Vietnam, it is crucial to understand the national context of two key indicators, namely life expectancy at birth and literacy rates. While life expectancy at birth demonstrates the mortality pattern of a population across all age groups (World Health Organization, 2023a), literacy rates illustrate the proportions of a population aged 15 years and above that can read and write with the comprehension of a simple statement about daily life (World Health Organization, 2023b).
Life Expectancy at Birth in Vietnam
In 2021, life expectancy at birth in Vietnam was 78.24 years old for women and 69.12 years old for men on average (O’Neill, 2023). Figure 1 illustrates life expectancy at birth in Vietnam by gender differences (period of 1950–2020 and the projection to 2100). It is evident that life expectancy at birth for women consistently exceeds that of men in Vietnam. The trajectory of life expectancy at birth can be delineated into three key phases, spanning from 1950 to 1960, the period after 1960 through the 1970s, and from 1975 onward. First, in 1950, life expectancy at birth for women surpassed that of men by approximately 10 years, with women averaging 55 years old and men being 44 years old. Over the subsequent decade, both genders witnessed a considerable rise in life expectancy, reaching a peak of about 64 years for women and 53 years for men in the early 1960s. Second, the following period from the 1960s through the 1970s saw a sharp decline and significant fluctuation in life expectancy at birth for both genders in Vietnam, with men experiencing a more pronounced decrease. This decline culminated in a low point at the end of the 1960s and early 1970s. Third, from 1975 onward, life expectancy at birth in Vietnam exhibited remarkable progress that indicates improvements in living standards, healthcare access, and overall well-being for the population.

Life expectancy at birth in Vietnam by gender differences (period of 1950–2020 and the projection to 2100).
Literacy Rates in Vietnam
In 2020, literacy rate of population aged 15 years and above in Vietnam stood at 95.40% for the whole population, specifically reaching 96.70% for men and 94.10% for women (General Statistics Office and UNFPA Viet Nam, 2021). Table 1 provides literacy rates of adult men and women (percentage of men and women aged 15 years and above) from 1979 to 2019 (10-year interval). Overall, Vietnamese men consistently have had higher literacy rates than that of women over a period from 1979 to 2019. Since 1979, more than 90% of Vietnamese men aged 15 years and above were literate, while the percentage of literate women only reached this target from 2009 onwards. The gap in literacy rates between Vietnamese men and women has been narrowing in recent years. The literacy rate of Vietnamese men increased steadily, reaching 97% in 2019; whereas, this percentage of Vietnamese women experienced a more dramatic increase from 78.14% in 1979 to 94.57% in 2019 (The World Bank, 2022a, 2022b).
The Literacy Rates by Genders in Vietnam from 1979 to 2019.
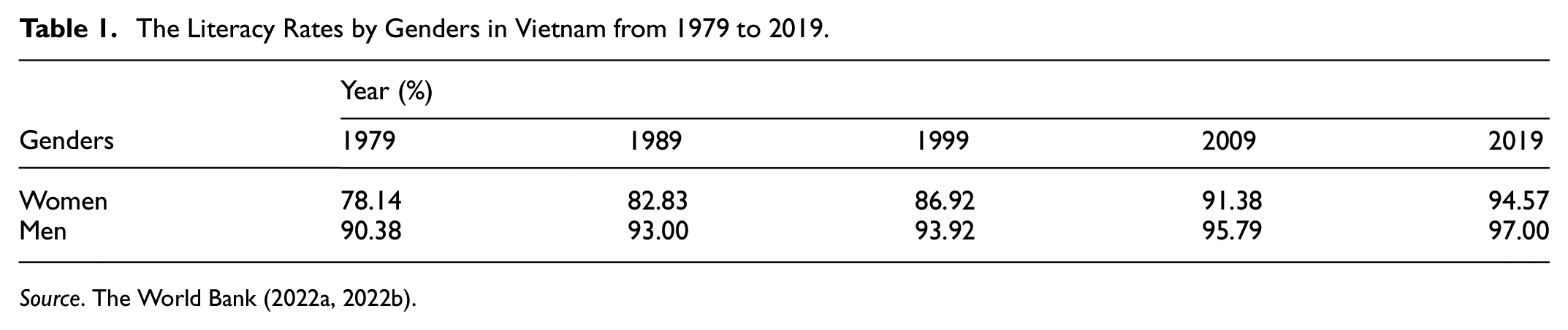
Source. The World Bank (2022a, 2022b).
Theoretical Framework
This study employs the demographic analysis method introduced by Professor Wolfgang Lutz in the year 1995 to calculate Literate Life Expectancy (LLE) based on Life Table and Age-specific Literacy Rates data, and subsequently compares the LLE gap between women and men as an indicator of social development (Lutz & Goujon, 2004). This analytical technique was first applied by Lutz and Goujon (2004) to assess social development across 50 countries. In subsequent years, it has been used to evaluate social development levels across regions in countries such as Mexico, India, China, Bangladesh, and Pakistan (Chattopadhyay & Sinha, 2010; Huang & Nanjo, 1998; Khan & Asaduzzaman, 2007; Medina, 1996; Nasir et al., 2013; Rahaman Khan et al., 2016).
Accordingly, Life Table and Age-specific Literacy Rates data were employed to compute Literate Life Expectancy (LLE) in Vietnam across different birth cohorts. Subsequently, a comparison of LLE between women and men across these birth cohorts was conducted to evaluate social development over time which aligns with the specific age groups. The unique advantage of both life table and age-specific literacy rates lies in their detailed breakdown by specific age groups, which range from less than 1 year old to above 85 years old for life table and from 15 years old to above 80 years old for age-specific literacy rates. Therefore, by comparing Literate Life Expectancy (LLE) between women and men across different birth cohorts—from the 15–19-year-old cohort to the 80–84-year-old cohort—we can depict the social development of a country over a historical period. This method involves three main steps: (1) extracting data from the Vietnam Life Table and age-specific literacy rates, (2) calculating LLE, and (3) analyzing the women-men gap in LLE across birth cohorts to assess Vietnam’s social development over time.
Methodology
Study Design
This study adopts a demographic approach to evaluate Vietnam’s social development by examining age cohorts in 5-year intervals. Since the analysis relies on purely demographic calculations, no statistical tests are used. To be more specific, demographic analysis employs its own mathematical formulas and presents results through descriptive tables, figures, and graphs to track changes in indicators across age cohorts (Wachter, 2014). As a result, the indicators used in this study are strictly demographic, meaning statistical tests are not applicable, unlike in other studies. This approach is akin to the methods used to calculate the Physical Quality of Life Index (PQLI), the Human Development Index (HDI), and the Social Development Index (SDI) for measuring and comparing the socio-economic development of countries, without the need for statistical testing.
Data and Methods
Applying the demographic technique of Lutz and Goujon (2004), first, we utilize the latest Vietnam Life Table from 2019, sourced from World Health Organization (2020), for both women and men. The life table (or the mortality table) is a statistical tool in demography and actuarial science to illustrate the mortality experience of a specific population (Namboodiri & Suchindran, 1987). John Graunt was the first person to demonstrate the dying out of a cohort in his work “The London Bills of Mortality” which laid the foundation for life table analysis. However, John Graunt’s life table was based on a cohort without considering the age at death of individuals. The first life table based on actual age-at-death data was developed by Edmond Halley in a population believed to be stable (Connor, 2022). In epidemiology, life table techniques have been utilized by Sullivan to construct the “Healthy Life Expectancy” indicator – a single measure to understand average population health (Salomon et al., 2012). In demography, “Literate Life Expectancy” invented by Wolfgang Lutz using life table method is an indicator to measure social development which is also the main focus of our study. In particular, Vietnam Life Table is organized into 5-year age intervals from less than 1 year old to 85 years old and above which covers key components including nMx (age-specific death rate between ages x and x + n), nqx (probability of dying between ages x and x + n), lx (number of people left alive at age x), ndx (number of people dying between ages x and x + n), nLx (person-years lived between ages x and x + n), Tx (person-years lived above age x), ex (expectation of life at age x). The mathematical operation of life table is applied to calculate LLE. Description and formulas of each element in the ordinary life table are presented in the works of Preston et al. (2000) and Wachter (2014). Please refer to Tables A1 and A2 in the Appendix for the Life Tables of Vietnamese men and women.
Second, LLE is calculated separately for men and women based on ordinary life table method. The age-specific literacy rates (PLx) in 2020 from the Vietnam General Statistics Office is utilized to calculate LLE for both men and women across age groups of 5-year interval, ranging from 15 years old to 80 years old and above. This 5-year age interval is accurately aligned with the age interval in the Vietnam Life Table of World Health Organization in 2019 (General Statistics Office and UNFPA Viet Nam, 2021). We assume that there would not be significant changes in the age-specific literacy rates in Vietnamese context in 2019 and 2020. The methodology of this study is similar to the original methodology developed by Lutz and Goujon (2004). In the study of Lutz and Goujon (2004), literacy data in 2000 and mortality data in 2001 were applied to calculate literate life expectancy for birth cohort from 1970 to 2000, and projection for birth cohort from 2000 to 2005. In addition, we extract the value of
Literate life expectancy is calculated as follows:
• Step 1: Calculate literate person-years lived

-
-
-
• Step 2: Calculate literate life expectancy

-
-
-
Literate Life Expectancy (LLEfemale) for Vietnamese Females.

Source. Authors’ calculation from Vietnam Life Table 2019 and Age-specific literacy rates 2020.
Literate Life Expectancy (LLEmale) for Vietnamese Males.

Source. Authors’ calculation from Vietnam Life Table 2019 and Age-specific literacy rates 2020.
Third, we calculate the women-men gap in LLE across birth cohorts to examine social development of Vietnam over historical period of time (Table 4). From LLE for women, we subtract LLE for men to illustrate the difference in LLE between women and men for each birth cohort. The magnitude of the gap in LLE between women and men can provide insights into the progress of health care initiatives and literacy improvement. A narrow women-men gap in LLE indicates society with higher mortality rates and a significant literacy gap between women and men. Conversely, a wide women-men gap in LLE illustrates society with lower mortality rates and apparent gender equality in literacy (Lutz & Goujon, 2004). Thus, we are able to evaluate Vietnam’s social development via birth cohorts, from 1935–1939 to 2000–2004, simply by analyzing Vietnam Life Table in 2019 and Vietnam age-specific literacy rates in 2020.
Female-Male Gap of Literate Life Expectancy (Years) for Vietnamese Males and Females.

Source. Authors’ own calculation.
Findings
Figures 2 and 3 illustrate LLE in Vietnam for both genders across birth cohorts from 1935–1939 to 2000–2004, corresponding to age groups ranging from 15–19 to 80–84 years old. Overall, there is a consistent improvement in LLE for both women and men across all age groups from the 1935 to 1939 birth cohort to the 2000 to 2004 birth cohort. While the maximum LLE for women stands at about 57.88 years old and its minimum for women is about 2.85 years old, the maximum and minimum LLE for men are approximately 53.69 years old and 3.39 years old respectively. Across birth cohorts from 1945 to 2004 or age groups from 15 to 74 years old, LLE for women is consistently higher than that of men. In contrast, for those born before the year 1945 which belongs to the oldest-old aged 75 to 84 years, men exhibit higher LLE than women. Comparing genders within cohorts, women have the highest LLE in the youngest cohort and the lowest LLE in the oldest cohort. In particular, LLE for women aged 15 to 19 years in the 2000 to 2004 birth cohort is nearly twice that of women aged 45 to 49 years in the 1970 to 1974 birth cohort (approximately 57.88 years old and 29.66 years old, respectively). Similarly, LLE for the youngest men is roughly 54 years old for the 2000 to 2004 cohort, slightly over double that of middle-aged men (45–49 years old) in the 1970 to 1974 cohort (approximately 53.69 years old and 26.54 years old, respectively). Regarding the older population, both men and women in the old-old (aged 70–79 years for the 1940–1949 birth cohort) and oldest-old (aged 80–84 years for the 1935–1939 birth cohort) groups exhibit LLEs of less than 10 years.

Literate life expectancy in Vietnam across birth cohorts.

Literate life expectancy in Vietnam across age groups.
Figures 4 and 5 display line graphs illustrating the women-men gap in LLE across age groups and birth cohorts in Vietnam. Generally, the women-men gap in LLE widens with younger cohorts. This gap keeps increasing without sudden changes across birth cohorts. The largest gap in LLE between women and men is observed in the youngest cohort aged 15 to 19 years in the birth cohort 2000 to 2004 and 20 to 24 years in the birth cohort 1995 to 1999, at about 4.19 years and 4.02 years respectively. The trend suggests that as social development increases, the gap in LLE between women and men becomes more pronounced in Vietnam. Among individuals in the oldest-old age group (75–84 years old) belonging to the birth cohort 1935 to 1944, LLE for men surpasses that of women, resulting in a women-men gap of less than 1 year. However, this gap is minimal which implies that LLE for Vietnamese women and men is nearly identical within the oldest-old population. Notably, for the birth cohort spanning from 1935 to 1974 (aged 45–84 years) which was before the war ended in 1975, the narrowing women-men gap of LLE unveils a sluggish period in social development. Conversely, for the cohort born after 1975 until recent years (aged 15–44 years) when the war officially ended, the widening women-men gap of LLE suggests a faster pace of social progress.

Women-men gap of literate life expectancy across age groups in Vietnam.

Women-men gap of literate life expectancy across birth cohorts in Vietnam.
Discussion
This study plays a crucial role in advancing the comprehension of Vietnam’s social development across different birth cohorts. It achieves this objective through the analysis of the LLE indicator, utilizing the most recent Life Table and Age-specific literacy rate data in Vietnam. Finding reveals consistent progress in LLE for both men and women in Vietnam, spanning all demographic cohorts from the 1935 to 1939 birth cohort to the 2000 to 2004 birth cohort. Therefore, it reflects the steady improvement in Vietnam’s journey of social development over a nearly 70-year period. In particular, LLE for women is higher than LLE for men across age groups 15 to 74 years old who belong to birth cohort from 1945 to 2004. The difference in LLE between women and men keeps widening continuously with younger cohorts in Vietnam and this gap starts becoming evident from the birth cohort 1945 to 1949. By examining the trajectory of the women-men gap in Literate Life Expectancy from 1935 to 2004, the study identifies three distinct stages of social development in Vietnam corresponding to historical milestones, which can be attributed to a series of fundamental education and primary healthcare policies.
Stage 1, which is characterized by LLE for women being lower than that of men in Vietnam for birth cohorts from 1935 to 1945, reflects slow social progress during colonization. This phase coincided with Vietnam’s period of colonization, spanning from 1884 to 1945 under French rule (Anh, 1985). The period from 1940 to 1945 marked by Japanese occupation of Vietnam (Anh, 2002). In the mid-1940s, Vietnam, which was a primarily agrarian society, faced immense poverty and underdevelopment. The majority of the Vietnamese population resided in rural areas, however, a significant portion of peasant households (roughly 60%) did not acquire any land ownership for cultivation (Boothroyd & Pham, 2000). During the period of 1944 to 1945, North Vietnam experienced a number of devastating disasters. In the summer of 1944, a series of natural disasters resulted in the destruction of main season harvest, particularly in Thai Binh – province in North Vietnam where overpopulation and malnutrition were rampant (Chieu, 1986). The Great Famine in 1944 to 1945, partly due to the Japanese and French policies regarding rice collection for war preparation, led to the death of up to 2 million North Vietnamese, causing the high crude death rate before 1945 at 24.2 per 1,000 people (Barbieri et al., 1996; Trinh, 2018). This famine was well-known as one of the great events in the history of 20th century of the world (Huff, 2019). Regarding basic education, colonization caused most of Vietnam’s population to be illiterate by the 1940s, at around 80 to 95% of the population (Malarney, 2012). In 1936, it was estimated that only 1% of Vietnamese people had the opportunity to receive formal education under the French educational system (Q. H. Le, 2023). Especially, French colonial education policies of the “crudely transplanted colonial education” led to the illiteracy of the Vietnamese living in rural and ethnic minority areas reaching to 100% (Wang, 2023). French colonial education policies limited Vietnamese access to French schools and educational system being similar to French education. There were a myriad of policies from the colonial government such as advocating a campaign to prevent Vietnamese wealthy families sending their kids to France for studying abroad, denying scholarships for the Vietnamese to study abroad, sending letter to European schools to ask them not admitting Vietnamese students and imposing a list of strict criteria for studying abroad to restrict the flow of Vietnamese students to France (Kelly, 1977). Regarding primary healthcare, poor healthcare resources and impoverished public health practices led to high mortality of the country. The inadequacy of healthcare facilities during the early 1940s in Vietnam was significant, with physician-to-population ratio being 1:180,000, only 47 hospitals, 9 maternity homes, and a mere 4,000 beds available for a population of approximately 18 million Vietnamese population. In 1936, life expectancy of the country stood at only 34 years old; high infant and maternal mortality reached 300 to 400 per 1,000 live births and 20 per 1,000 deliveries, respectively (Ladinsky & Levine, 1985).
Stage 2, which is characterized by LLE for women being higher than that of men for birth cohorts from 1945 to 1975 in Vietnam, reflects developing social progress after Vietnam’s independence declaration from colonization. By 2nd September in 1945, Vietnam proclaimed its independence and established Democratic Republic of Vietnam in Northern Vietnam (Hac, 2019). Regarding basic education, in post-1945, the revolutionary “Mass Education” campaign (Bình Dân Học Vụ), which was a central policy implemented by Northern Vietnamese Communists, was conducted to improve literacy of the population, thus succeeding in increasing literacy rate by 93.4% by the late 1950s (Malarney, 2012). A number of illiterate people enhanced their literacy capability by self-study or attending evening classes offered by educational programs (Fraser, 1993). The elimination of illiteracy for minority ethnic people was strongly advocated by North Vietnamese government, as evidenced by a number of educational policies such as guidelines for the development of education in the hinterlands in 1964 issued by the Central Party Secretary, the enlargement of school network (especially primary and secondary schools for minority children) and the training for ethnic minority people to staff mountain schools (Schrock, 1972). In South Vietnam, in 1945, the French government made an official decision to transfer the management of Vietnam’s education system to the Vietnamese government headed by Emperor Bao Dai (Vu, 2021). The triumph of “Dien Bien Phu” battle in 1954 marked the key historical event of Vietnam gaining independence from the First Indochina War (Showalter, 1998). Accordingly, the Geneva Accords in 1954 divided Vietnam into two separate entities along the 17th parallel, namely the Democratic Republic of Vietnam (North) and the Republic of Vietnam (South). During the period from 1954 to 1975, while the former followed the Soviet model of education, the latter adopted a system influenced by the United States ( Y. T. H. Nguyen & Sukontamarn, 2022). The establishment of the Republic of Vietnam led to a number of education and anti-illiteracy campaigns being implemented to provide basic education to a wide range of students, regardless of age, region and ethnicity. Article 26 of the South Vietnam Constitution 1956 highlighted the government’s commitment to provide compulsory and free education to all citizens. Additionally, in 1956, an anti-illiteracy campaign was launched, emphasizing the collaborative efforts of different stakeholders to eradicate illiteracy in the country. Those efforts resulted in a remarkable reduction in illiterate population from more than 2 million illiterate people in 1954 to only around 600,000 by 1961 in South Vietnam (Duyen, 1962). Regarding primary healthcare, during the 1950s to the 1960s, the Northern Vietnam government implemented significant healthcare improvements following the devastating famine crisis in 1945. These efforts included expanding public health and maternity stations at the village level to reduce infant mortality, improving local cleanliness through initiatives such as well-digging for drinkable water and constructing animal dung heaps to combat fly infestation, and importing vaccines from the Soviet Union to prevent epidemics like polio. Concurrently, the Southern Vietnam government adopted healthcare models from European countries, especially being concentrated in Sai Gon (Banister, 1985). These concerted efforts led to a substantial increase in life expectancy at birth during this period. However, the intensification of conflict over North-South reunification in the late 1960s and early 1970s resulted in significant mortality among Vietnamese, particularly men (Teerawichitchainan, 2009). Southern Vietnam suffered from the destruction of health care infrastructure due to the warfare, further exacerbating mortality rates (Banister, 1985).
Stage 3, which is characterized by a widening women-men gap in LLE for birth cohorts from 1975 to 2004 in Vietnam, reflects rapid social progress in healthcare and basic education in post-Vietnam War. After the North-South reunification of Vietnam by 30th April in 1975 which led the country to be free from the Vietnam War, a series of reforms were enacted to drive the growth of the country after the war. After 1975, Vietnam underwent a rapid progress in social development, including improvements in education and healthcare, which contributed to the overall enhancement of the quality of life for its population (Nghia, 2020). Thanks to the revolution of the economic reform in “Doi Moi” era in 1986, Vietnam’s real GDP per capita experienced a tremendous growth, making Vietnam as “East Asian Miracle” economy in the 1990s. Regarding basic education, the growth of economy facilitated well for the expansion of schools, educational services and teacher development (Phan & Coxhead, 2022). Along with the remarkable economic reform “Doi Moi” in 1986 transitioning the country from centrally planned economy into socialist-oriented market economy, Vietnam undergone remarkable education initiatives such as “Education for All” (Biddington & Biddington, 1997) and nationwide anti-illiteracy campaign in the early 1990s (Banister, 1992). Such efforts resulted in 98% enrollment in primary schools and significant improvements in universal education for the entire population after the first 9 years of “Doi Moi” reform. The target in universal education for the entire population has been met since 2000 for primary education which made significant contribution in eradicating gender inequality in basic education (A. V. Le et al., 2022). However, after the Fall of Saigon in 1975, children in the families associated with the former government of the Republic of Vietnam faced certain discrimination and limited access to education (N. H. C. Nguyen, 2013). This could potentially lower the educational attainment level among a segment of the population in Southern Vietnam. Regarding primary health care, since the 1990s, health policy of allowing hospitals a certain degree of autonomy to set fees has contributed to the development of the private healthcare sector, thus leading to the increase in national healthcare standards and the reduction for the burden on public hospitals (Quan et al., 2023). Law on People’s Health Protection, entacted in 1989, mandated that the responsibility of the government was to provide healthcare to all its citizens (Truong & Schmid, 2023). In 1992, social health insurance in Vietnam was initially implemented with an aim to facilitate universal health coverage. Since 1998, there has been a notable increase in enrollment rates thanks to the expansion of social health insurance to include coverage for impoverished individuals (Q. N. Le et al., 2020). In 1993, almost every Vietnamese urban resident and up to 75% Vietnamese rural citizens had access to basic primary healthcare. In 1990, Vietnam had one of the highest per capita physician supplies in developing nations, with 1 physician for every 2,694 citizens and 1 nurse for every 760 citizens. With 167 health centers per million people in 1992, Vietnam had one of the most favorable hospital bed-to-population ratios in developing countries, including both polyclinics and specialized health centers (Gellert, 1995).
In comparison with other countries in regional context, our findings provide three major implications. First, the trend of LLE for women being higher than LLE for men observed in Vietnam (birth cohort 1945–2004) bears strong resemblance with the trend of LLE in Thailand (birth cohort 1995–2005), Sri Lanka (birth cohort 2000–2005), South Korea (birth cohort 1990–2005) and Philippines (birth cohort from 1970–2005) but contrasts with China, Malaysia, Singapore, India and Indonesia where LLE for women is always lower LLE for men (birth cohort 1970–2005) (Lutz & Goujon, 2004). This finding reveals gender discrimination against women regarding social development in countries with LLE for women being lower than that of men during the period from 1970 to 2005. For example, the one-child policy resulted in the rapid growth of sex imbalances at birth in son-preference society of China in the late 1980s. This led to significant ethical debates due to the millions of missing females (Nie, 2011). India and Indonesia have been grappling with a concerning gender disparity in literacy rates, with women consistently lagging behind men (Harahap et al., 2020; Katiyar, 2016). Malaysia and Singapore’s literacy efforts only began since the 1960s after gaining independence from colonization, therefore, illiteracy still exists among older population (Lutz & Goujon, 2004). In this light, LLE serves as valuable indicator to demonstrate the social development of countries ranging from lower-income to high-income nations without considering the economic component. Second, the pattern of women-men gap in LLE getting widening with the younger cohort in Vietnam is similar to that of Thailand, China, South Korea, Singapore, Malaysia, Sri Lanka, and Indonesia (Lutz & Goujon, 2004). This indicates that those countries showcased efforts to implement initiatives in social development for women across periods of time. Third, Vietnam’s LLE for women (birth cohort 2000–2004) is around 57.88 years old which is higher than that of women in birth cohort 2000 to 2005 in China (47.2 years old), India (25.1 years old), Indonesia (47.8 years old), and Malaysia (52 years old). However, LLE for Vietnamese women (birth cohort 2000–2004) is lower than that of women in birth cohort 2000–2005 in Philippines (60.4 years old), Singapore (60.6 years old), Sri Lanka (59.6 years old), and Thailand (58.6 years old) (Lutz & Goujon, 2004). Therefore, Vietnam’s social development for women from 2000 to 2004 ranks higher than that of China, India, Indonesia, and Malaysia from 2000 to 2005 but lags behind that of the Philippines, Singapore, Sri Lanka, and Thailand from 2000 to 2005.
Conclusion
This study introduces a novel demographic approach by using LLE to assess social development in Vietnam over the historical period of time. The analysis of women-men gap in LLE across birth cohorts serves as a valuable insight to grasp full comprehension of Vietnam’s 70-year journey of social development. In addition, LLE can be useful in making comparison and understanding about social development of other countries in regional context. We conclude key insights from this study as follows.
First, consistent progress in LLE for both men and women in Vietnam, spanning all demographic cohorts from the 1935 to 1939 birth cohort to the 2000 to 2004 birth cohort, reflects the steady improvement in Vietnam’s journey of social development over a nearly 70-year period. There are three distinct stages of Vietnam’s social development from 1935 to 2004. Stage 1 (from 1935 to 1945), with LLE for women being lower than that of men, Vietnam was in the period of colonization, along with a series of natural disaster and great famine as well as the colonial education policies to hinder the literacy of the population, causing high mortality and high illiteracy of the country. Stage 2 (from 1945 to 1975), when LLE for women started to be higher than that of men, Vietnam experienced developing social progress. During this period, the country proclaimed its independence from colonization and established two countries, namely the Democratic Republic of Vietnam (North) and the Republic of Vietnam (South). A number of initiatives in basic education and primary healthcare of two separate countries in Vietnam started to be implemented to drive the social development for the population. Stage 3 (from 1975 to 2004), when the women-men gap of LLE keeps widening which is in favor of women, the country showcased the rapid social development. Vietnam witnessed a significant historical event which was the North-South reunification by 30th April in 1975 to be free from the Vietnam War. Since the post-Vietnam War, the country experienced tremendous growth with a myriad of revolutionary reforms in basic education and primary healthcare.
Second, in comparison with other countries in regional context, LLE indicates certain forms of gender inequality in social development in countries with LLE for women being lower than that of men. The prime examples are the excess female child mortality as a result of one-child policy in China, women’s low level of literacy in India and Indonesia and illiteracy among older women in Malaysia and Singapore (birth cohort 1970–2005). In the case of Vietnam, trend of LLE showcases that social development for women in Vietnam from 2000 to 2004 is proved to be better than China, India, Indonesia and Malaysia from 2000 to 2005 but poorer than Philippines, Singapore, Sri Lanka and Thailand from 2000 to 2005.
Given that LLE is rarely explored in the literature, future research should explore LLE as a valuable demographic instrument for assessing social development, independently of economic factors within a nation. By analyzing LLE across various birth cohorts and examining the gap between women and men, policymakers can glean insights into the trajectory of social development over historical periods. Moreover, this demographic approach extends beyond examining the social development of a country as a whole; it can also evaluate social development among different demographic groups, such as urban-rural, regional, or provincial differences, and even project future scenarios. Finally, the women-men gap in LLE can be utilized in studies to compare social development between countries, similar to other indices like the Physical Quality of Life Index (PQLI), the Human Development Index (HDI), and the Social Development Index (SDI).
Footnotes
Appendix
Age-Specific Proportions Literate
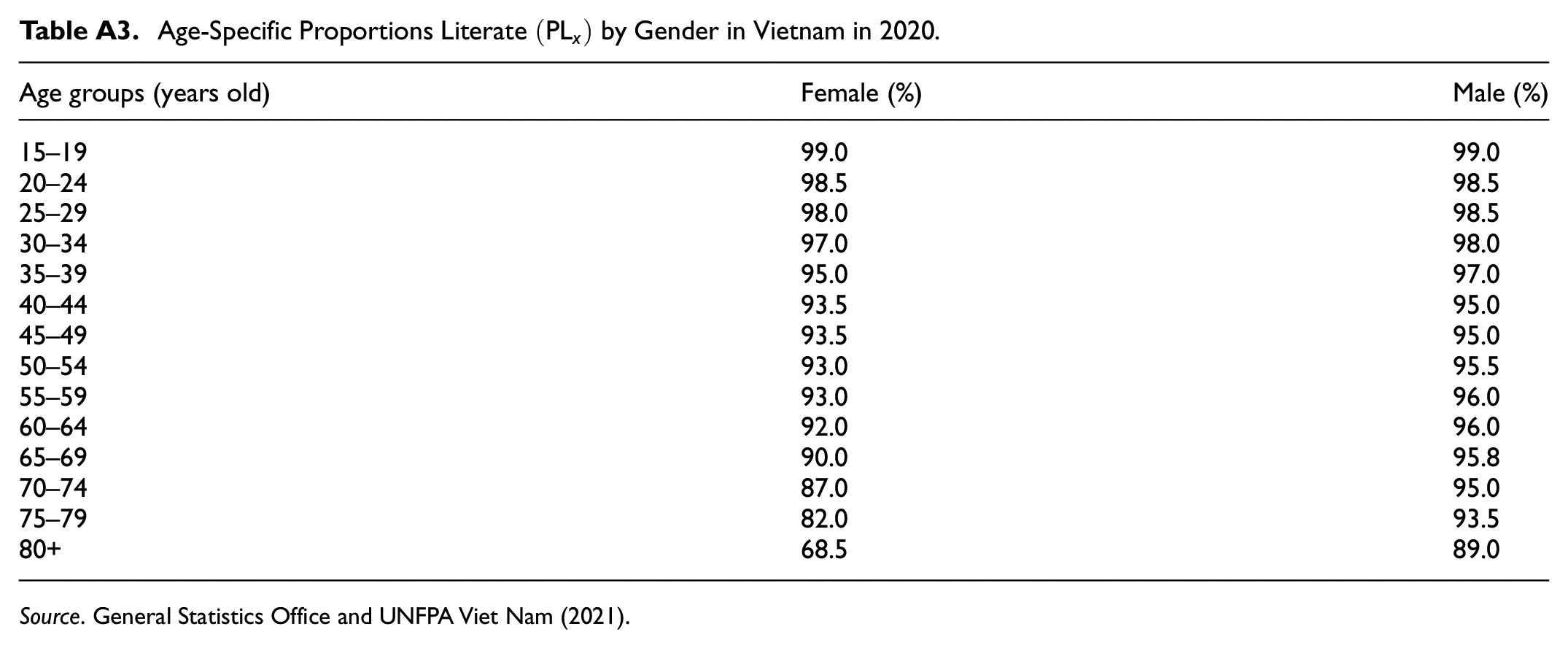
| Age groups (years old) | Female (%) | Male (%) |
|---|---|---|
| 15–19 | 99.0 | 99.0 |
| 20–24 | 98.5 | 98.5 |
| 25–29 | 98.0 | 98.5 |
| 30–34 | 97.0 | 98.0 |
| 35–39 | 95.0 | 97.0 |
| 40–44 | 93.5 | 95.0 |
| 45–49 | 93.5 | 95.0 |
| 50–54 | 93.0 | 95.5 |
| 55–59 | 93.0 | 96.0 |
| 60–64 | 92.0 | 96.0 |
| 65–69 | 90.0 | 95.8 |
| 70–74 | 87.0 | 95.0 |
| 75–79 | 82.0 | 93.5 |
| 80+ | 68.5 | 89.0 |
Ethical Approval
This study used only secondary data and no personally identifiable data was used in the analysis or dissemination of the results of this study. Statistical computing techniques and demographic analysis are used based on numbers. Therefore, ethics approval is deemed unnecessary.
Author Contributions
All authors contributed to the study conception and design. Material preparation, data collection were performed by both authors. Truc guided the analysis and outlined the structure of the entire study. Introduction, country context and data analysis were performed by Hang. Discussion and conclusion were written by Truc. All authors read and approved the final manuscript.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Life Table 2019 is publicly available on the website of World Health Organization https://apps.who.int/gho/data/view.main.61830?lang=en. Age-specific proportions literate 2020 is publicly available on the website of General Statistics Office ![]()