
Abstract
This study investigates determinants of adult children’s medical decision preferences for their elderly parents, aiming to optimize healthcare service utilization. Seven influencing factors were identified and a discrete choice experiment was conducted. Data were analyzed with a binary logit regression model. Results highlight treatment effectiveness (p < .001, OR = 5.945), physician attitude (p < .001, OR = 2.740), hospital accessibility (p < .001, OR = 2.136), waiting duration (p < .001, OR = 1.604), and hospital rank (p = .001, OR = 1.409) as key concerns when deciding medical care for older parents. Physician title and online health insurance reimbursement showed no significance. Chinese adult children tend to rationally choose primary healthcare centers and Grade II hospitals for effective therapy and doctor-patient communication, suggesting investments in these facilities to enhance healthcare delivery within a hierarchical medical system.
Keywords
Introduction
The Internet has affected almost all the industries, and the Internet-based healthcare emerges with the rapid development of the Internet and increasing demands for healthcare (Zhang, Deng, Evans, et al., 2018). With more than 10 years’ efforts, online health service industry has prospered in China, and various online health service platforms emerged such as WeDoctor, ChunyuDoctor, and haodf.com. They can not only help patients to find appropriate doctors by the information provided on patient rating websites (Deng et al., 2019; Zhang, Deng, Hong, et al., 2018), but also offers health information to the public (Kummervold et al., 2008; Zhu et al., 2019). Some online platforms allow doctors to diagnose, prescribe, and conduct patient follow-ups online (e.g., chronic patients; Hajli, 2014). Despite significant advancements in the online healthcare industry, research indicates that the target audience for online health services in the Chinese context remains insufficiently prepared, leading to a pronounced digital divide in service utilization. This digital divide has contributed to the widening health disparities among different population groups.
Online Health Service Needs and Utilization Among the Older People
The health needs of the older population have increased exponentially globally, with a significant increase in the health needs of elderly individuals (L. Wang et al., 2021). However, the extant health service received by the older is far from suitable and desiring. The United Nations defined that if a country or region has 10% or more population aged 60 or 7% or more population aged 65 and above, it means that the country or region is in an aging society. The World Population Ageing Report (United Nations, 2020) states that 727 million population aged 65 years or over globally, and this is projected to double to 1.5 billion in 2050. In this social context, there is a rapid increase in the health needs of elderly individuals, making it increasingly crucial to address and meet their health demands.
Compared to developed nations, China’s healthcare support for its aging population falls short, and older individuals in the country exhibit limited internet skills and adoption, lagging behind their counterparts in other countries (Yang et al., 2020). For example, the United States has spent vast efforts in educating the older generation with personalized courses, and Digital Literacy Education Program aimed to encourage them to use online services (Ansello, 2011). In 2018, about 66% of the older in the United States has used the Internet, but for the older in China, their internet use is much lower (Y. Wang et al., 2019). As of March 2020, the number of Internet users aged 60 or above in China only accounts for 6.7% of the total number of Internet users. A Spanish survey on the use of Information and Communication Technologies among the older also suggests that the correlation of age and ICT adoption, “digital divide” (Menéndez Álvarez-Dardet et al., 2020). With the advancement of the online health service industry, the Chinese older become disadvantaged for this medical innovation, and they fail to use the Internet-based health service.
Making Medical Choice for Older Parents Online
Realizing the difficulties of the utilization of online health services for the older in China, they turn to their adult children for help, that is, ask them to make online appointments with physicians, choose a suitable online physician. This is quite different from the surrogate decision, which happens when dying patients cannot make their own medical decisions and have to reply to their surrogates (Torke et al., 2020). In our study, the adult children are proxies pertinent to the utilization of online health services for their older parents, that is, the choice of medical institutions and the choice of doctors. Taking the Chinese transitional culture of Xiao (filial piety) into consideration (He et al., 2021), the adult children could always be the first choice for the older who encounter problems on the Internet use for health reasons. The intergenerational support is critical for the utilization of online health services by the older generation, and the adult children’s role in the proxy is prevalent in current China (Anning, 2018). However, the majority of the extant research has focused on the preference of the older themselves who received the proxy service exclusively, and seldom efforts looked into their adult children’s role in making healthy choices in the digital age. In China, after the children have become adults, they shoulder responsibility to take care of their older parents. The present study aims to provide a different perspective on health service utilization among China’s older generation to fill this research gap.
With a comprehensive analysis of the patients’ preference for physician’s offline and the unique features of online health platforms, this study employs a discrete choice experiment to explore the impact factors of adult children’s decisions for their older parents in an online health environment. This study is one of the earliest efforts looking into adult children’s health decisions for their older parents, and it could provide valuable information for understanding the utilization of the older in China, as well as the optimizing online health service.
Literature Review
Theories for Making Medical Decisions for Older Parents
Previous research has employed various theories to investigate differences in decision-making between self and others, including theories such as the construal level theory and regulatory focus theory.
The construal level theory posits that individuals’ perception of psychological distance influences their cognition and behavior. When perceiving greater psychological distance, individuals tend to engage in high-level construal, focusing on core features and ultimate outcomes. Conversely, when perceiving lesser psychological distance, individuals are inclined to employ low-level construal, emphasizing local features and the specific process of implementation (Trope & Liberman, 2003). Due to variations in construal levels, individuals demonstrate inconsistent preferences in decision-making between “distant” and “proximate” scenarios. Prior research has further substantiated this notion, revealing that under high-level construal, individuals concentrate on the value and outcomes of options, tending to favor alternatives with higher value. Conversely, under low-level construal, the focus shifts toward feasibility, leading individuals to opt for solutions that are more easily implementable (J. Z. Xu & Xie, 2012).
When the cognitive object is oneself, psychological distance can be considered as 0, making others psychologically more distant in comparison to oneself. Therefore within the context of this study, divergent preferences in medical decision-making between decisions made for others and those made for oneself may arise due to differences in construal levels.
Regulatory focus theory refers to the individual tendencies during the process of goal attainment, where behavior is regulated by two distinct motivational systems: promotion focus and prevention focus. Specifically, individuals with a promotion focus are concerned with achievement and progress, often experiencing positive emotions. They seek to maximize gains and typically adopt a proactive strategy. Conversely, individuals with a prevention focus prioritize safety, responsibility, and obligations, often remaining in a calm state. They focus on minimizing losses and tend to adopt avoidance strategies to minimize errors (J. Z. Xu & Xie, 2012). Regulatory focus theory has been widely applied in research exploring the differences in self and other decision-making. Studies have shown that consumers making choices for themselves are more concerned with avoiding losses than maximizing gains, compared to consumers making choices for others (J. Lu et al., 2022). In our research, we examine how medical decision-making between adult children and elderly parents may differ as a result of regulatory focus, with implications for promotion focus and prevention focus.
The Factors Influencing Patient's Medical Decision Making
The decision-making process of a patient regarding healthcare is collectively influenced by myriad factors, principally including the characteristics of the healthcare institution and doctor, the individual attributes of the patient, and the health insurance policies. Firstly, the physician’s competency and demeanor strongly influence a patient’s medical decision making. Patients prefer physicians with superior capabilities and favorable attitudes due to the likelihood of better prognoses (Blanchard et al., 1988; Bornstein et al., 2000; Kioko & Requena Meana, 2021). Similarly, a high-reputation hospital with a good brand image enhances the patient’s perception of institutional competency and service quality, thus increasing their preference (Górska-Warsewicz, 2022). Secondly, the patient’s own physical health and familial support also play a pivotal role in selecting healthcare services. Previous research has revealed that the severity of a patient’s illness, age, and level of education can all influence their propensity to seek medical attention (Arora & McHorney, 2000). Thirdly, medical insurance policies significantly sway a patient’s decision in their medical choice. This holds especially true in developing countries, where the level of economic development and the extent to which medical insurance is supplemented are important drivers behind a patient’s decision on medical treatment (Ansari et al., 2023).
Research on Decision-Making for Others
When individuals make decisions for themselves, they pay more attention to the potential harm of risks. However, when making decisions for others, emotional responses to risks are diminished (Batteux et al., 2020). Previous studies have contrasted self-decisions and other-decisions in medical contexts, confirming differences between agent decisions and the patient’s own preference (Fagerlin et al., 2001). When choosing treatment plans for self and others, preferences are influenced by the decision-making role (Zikmund-Fisher et al., 2006). A comparison of physician’s self-decisions and decisions for patients found that physicians tend to choose riskier treatments for themselves, while they opt for more conservative choices for their patients (Ubel et al., 2011).
In an increasingly digitally aging society, a growing number of elderly individuals are showing interest in and demand for online medical services. However, due to limitations in internet literacy among the elderly population and the insufficient availability of online medical platforms tailored for this demographic, when elderly individuals require medical care, they often turn to their adult children for assistance in navigating online platforms to access medical information and make healthcare decisions. In order to effectively address the genuine medical needs of the elderly patient population, it is imperative to understand the preferences of their adult children in making medical decisions.
Despite the abundance of research on patient preferences in healthcare decision-making, the majority of studies focus exclusively on patients making decisions for themselves. While these studies have acknowledged the discrepancies between self-other decision-making in healthcare scenarios, an investigation into the preferences of adult children making medical decisions for their elderly parents has been notably absent. Our study integrates the theory of self-other differences to explore the factors influencing adult children’s decisions regarding medical care for their elderly parents. This not only enriches the application of self-other decision-making differences theory within healthcare settings but also fills a gap in the research on decision preferences for medical care on behalf of elderly parents. Moreover, our study’s outcomes hold significant practical implications. By addressing the needs of vulnerable groups such as the elderly in the digital age, our research contributes to meeting their genuine requirements more effectively. This study bridges the theoretical framework of self-other decision-making differences with the practical context of healthcare choices, thus offering substantive real-world significance.
Factors Affecting Medical Choice of Older Parents
Files of literature have explored the factors affecting patients’ choice for health service, and we have divided the influencing factors into several categories, one of the factors pertinent to the healthcare institutes, such as healthcare institute accessibility, waiting duration. Another factor is pertinent to the healthcare providers, like physicians’ attitudes, and treatment effect. Patients’ personal characteristics can also affect their choices, such as age, gender, education (Fotaki et al., 2008). Besides, health policies like health insurance programs and referral policies influence patient healthcare utilization (Mosadeghrad, 2014).
Factors Pertinent to Healthcare Institutes
Through the information sharing of the online medical community, users can learn about the medical experience of other patients to choose the most suitable health service. Previous studies on patient preference for online health service suggest that patient evaluation and rating of doctors and medical institutions affect other users’ choice. This evaluation mainly focused on waiting time, physician attitude, treatment effect, treatment cost, hospital, and doctor’s status (i.e., hospital rank and doctor’s title; Lin et al., 2020; Yang et al., 2015). In the context of advancing online medical services, for patients with mild symptoms and strong ability to use the online service, we can utilize online consultations as a means to engage with physicians for the purpose of diagnosis and treatment (Hong et al., 2019). With the popularity of private cars in China, the distance between medical institutions has no longer a significant impact on patient choice. While, for the older generation, this may still be an important factor since they prefer healthcare service within close distance.
Rank of Healthcare Institute
Hospitals are the most referred health care institutes in China, and the hospital rank is critical for the evaluation of its capability (Kim et al., 2018; C. Lu et al., 2019). The role of hospitals varies based on their function and size. Previous research showed that hospital rank has a significant impact on patient satisfaction and their healthcare utilization (Lee et al., 2018; Young et al., 2000). Currently, China has three ranks for hospitals based on their ability to provide healthcare-related services, including primary, secondary, and tertiary. Usually, the higher the rank, the better the health service.
Healthcare Institute Accessibility
Healthcare institute accessibility pertains to individuals’ perception on convenience of visiting a given healthcare institute, and it is often measured by the geographical distance between the healthcare institute and individuals’ residence. Empirical evidence demonstrate that the closer the distance between one’s residence and the healthcare institute, the higher the patient satisfaction is, and the location of the hospital can affect patient’s behavior (Chen et al., 2016; Gage, 2007).
Waiting Duration
Waiting duration is an instrument for rationing the demand for health services, it has a significant impact on healthcare service adoption (Löfvendahl et al., 2005). A survey on the influencing factors of waiting duration in rural medical institutions in Haiti that shortening waiting duration for medical services can improve patient satisfaction (Altema et al., 2020). The World Health Organization data shows that the waiting duration for outpatients worldwide is mostly between 30 min and 2 hr, and more than 30 min on average is regarded as long waiting duration (Altema et al., 2020).
Health Insurance Policy
Health insurance policy refers to a system that solves residents’ health problems, allocates medical resources, and ensures health equity through the financing mechanism of individual contributions or social subsidies (Pan et al., 2016; Wu et al., 2020). The health insurance system in China consists of public and private health insurance, and there are three types of public health insurance: Urban Employees’ Basic Medical Insurance (UEBMI), the Urban Residents’ Basic Medical Insurance (URBMI), New Cooperative Medical Scheme (NCMS), private health insurance (PHI; Hou & Zhang, 2017). In China, health services provided by non-designated facilities cannot be reimbursed by public insurance, and patients are prone to choose designated medical service institutions. With the development of the “Internet + medical insurance,” China has gradually made the insured patients’ medical treatment process optimized, medical insurance payment fast, convenient and cross-provincial medical treatment settlement become a reality (Ma et al., 2020).
Factors Pertinent to Healthcare Providers
Physicians’ Attitude
Patients perceive their physicians’ attitudes through various clues, such as speech tune, volume, and body language during their interaction. Research showed that physicians with a good attitude toward patients can improve patient satisfaction, patient compliance, and treatment effect (Tokunaga et al., 2000). If the perceived attitude of the physician is relatively poorer, patients are likely to switch their physicians (Leonard, 2008).
Treatment Effect
In general, treatment effect is defined as the degree to which the treatment result reaches the expected value of the patient, including the degree of discomfort relief, the accuracy of diagnosis and the duration of treatment (El-Guebaly et al., 1983). The reviews of the treatment effect on the online medical website provide information to adult children when choosing the doctor for their parents, and good comments have a positive impact on their choice (Y. Xu et al., 2016).
Physicians’ Professional Title
Physicians’ professional title reflects physicians’ qualification, including primary professional title (resident), intermediate professional title (attending physician), deputy senior professional title (deputy chief physician), and senior professional title (chief physician) in China. While in the United States, physicians’ professional title includes “resident” and “attending.” Previous research showed that patients treated by residents were more often likely to rate their experience as “worse” compared with those treated by the attending physician (Issa & Kim, 2012).
Materials and Methods
Discrete choice experiment is a research approach for measuring consumer preferences, and it has been widely used to measure patients’ preferences for two or more options (Lancsar & Louviere, 2008). By DCEs, the estimation of the relative importance of multiple attributes simultaneously is possible, it has greater face validity than other approaches, that is, traditional standard gamble or time tradeoff exercises (Hazlewood, 2018). To measure the influence of different factors on adult children’s choice for their older parents, our study adopts DCE approach.
Study Design
Firstly, we recruit eligible participants who were over 18 years old through “wjx.cn” (the largest questionnaire website in China), and participants were asked to fill in the background information, including age, gender, education level, income, the experience of online health service, etc.
After completing the basic information, a fictional medical scenario is presented to the participants. The participants will have 2 min to read and answer how they will make medical decisions for their parents based on the information of the hospital and doctors. The scenario is as follow: Supposing you and your parents don’t live in the same city, your father or mother feels uncomfortable and need to go to the hospital. You can only help him or her to recommend and select a treatment plan through the relevant information on the Internet. Through the comments of netizens on the Internet and the relevant information on the medical website, you must determine one choice from the two plans. The details of the two options are as follows. Which one would you choose for your parent?
Referring to relevant literature studies, we selected seven possible factors for their children to choose medical care for their elderly parents, and each factor was assigned two levels. The number and level of influencing factors determine the design of discrete choice experiment questionnaire. To determine the primary and secondary effects of these 7 influencing factors, it is necessary to formulate experimental schemes of corresponding factors, such as a multi-factor complete scheme. However, it will require 72 = 49 times of experiment in our study. To avoid this issue, our study employs the orthogonal design of experiment. It can greatly reduce the number of experiments and improve the experimental efficiency by testing the most combinations of factors with the least computation(Tyagi et al., 2020). Table 1 presents the details. We assigned one as the reference group (Plan A), and paired with the other group (Plan B) to form a question. Each question has three choices: A, B, and none of the two. Table 2 presents the details. When participants read the hypothetical scenario, they were asked to choose the preferred option in each question. Since almost no one will refuse to find a physician for their older parents openly in the widely acknowledged Xiao Culture, we have eliminated the choice as none of the two, which rendered only two choice for the participants.
Orthogonal Experiment Design.

Question Demonstration.

Data and Sampling
From April 5 to April 15, 2020, we randomly solicited 336 questionnaires via wjx.cn, the largest survey platform in China. After discarding those with excessively long or short completion times or anomalous data, we amassed 301 effective questionnaires, yielding an effectiveness rate of 89.6%. For data analysis, we used Statas 16 to perform a binary logit regression model to analyze the influencing degree of each factor, and a hierarchical logit regression model to differentiate the medical choice preferences among varying adult children groups.
All our independent and dependent variables follow a dichotomous scale of measurement. Independent variables encompass attributes that exert influence over respondents’ decisions when seeking medical care, whereas the dependent variable indicates whether respondents choose a specific healthcare option. In the process of data analysis, the act of selecting a particular healthcare option is denoted as “1,” whereas declining that option is represented as “0.” When handling the dependent variable, attributes reflecting the relatively advantageous aspects of a healthcare option are designated as “1,” while attributes representing relatively disadvantageous aspects are assigned “0.” To illustrate, in the context of “Hospital accessibility,” assigning “1” denotes “Within walking distance,” whereas “0” signifies “Long distance.”
Likewise, when conducting comparative analyses on various demographic characteristics of respondents, we categorize respondent features as binary variables. These encompass gender (male = 1, female = 0), educational level (high education level = 1, low education level = 0), and parents’ marital status (the single aged = 1, the aged with a spouse = 0).
Results
General Overview
Our study shows that 68.77% (207/301) of the adult children surveyed had used online health service. The majority (74.75%, 225/301) of them were youth aged 18 to 35. As for the educational level, 85.71% of them having a bachelor degree or higher. For the average monthly income, many participants were below 3,000 RMB. As for the number of children in the family, slightly over half participants (51.16%, 154/301) were from one-child family. Table 3 presents the details.
Demographic Characteristics of Adult Children.

To avoid possible of collinearity of factors, we performed collinearity analysis of all the selected influencing factors together. Some scholars have suggested that the critical value of VIF (variance inflation factor) should be defined as 10 (Montgomery et al., 2012). Through the collinearity diagnostics, we can find that the VIF value among the seven factors is far greater than 10, which indicates that there is strong collinearity among the factors. After several tests, we found that the collinearity of each factor decreased significantly after eliminating the factors of physicians’ professional title (see Table 4).
The Results of Collinearity Test After Excluding Physicians’ Titles.

To ensure model robustness, we used R 4.2.3, and conducted a Goldfeld-Quandt test on the model using the gqtest function. The output reveals GQ = 1.0391, df1 = 1,799, df2 = 1,799, and a p-value of .2078. This suggests that at a significance level of .05, the null hypothesis cannot be rejected. The null hypothesis posits no variance difference in the error term between the two sub-samples, implying the absence of heteroscedasticity. Conversely, the alternative hypothesis considers variance differences between the sub-samples. Thus, it can be concluded that the model does not exhibit heteroscedasticity.
Furthermore, to ascertain the independence of errors, we utilized R 4.2.3 to generate a Residuals versus Fitted plot (as depicted in Figure 1). The residuals are uniformly and evenly dispersed on both sides of the x-axis, thus providing evidence to support the assumption of error independence within the model.

Residuals versus fitted plot.
The result revealed that except for online health insurance reimbursement (p > .05), hospital rank (p = .001, OR = 1.409), hospital accessibility(p < .001, OR = 2.136), waiting duration (p < .001, OR = 1.604), physician attitude(p < .001, OR = 2.740) and treatment effect (p < .001, OR = 5.945) were significant in predicting adult children’s preference for their older parents (See Table 5).
Adult Children’s Preference for Older Parents (Logit Regression Model).
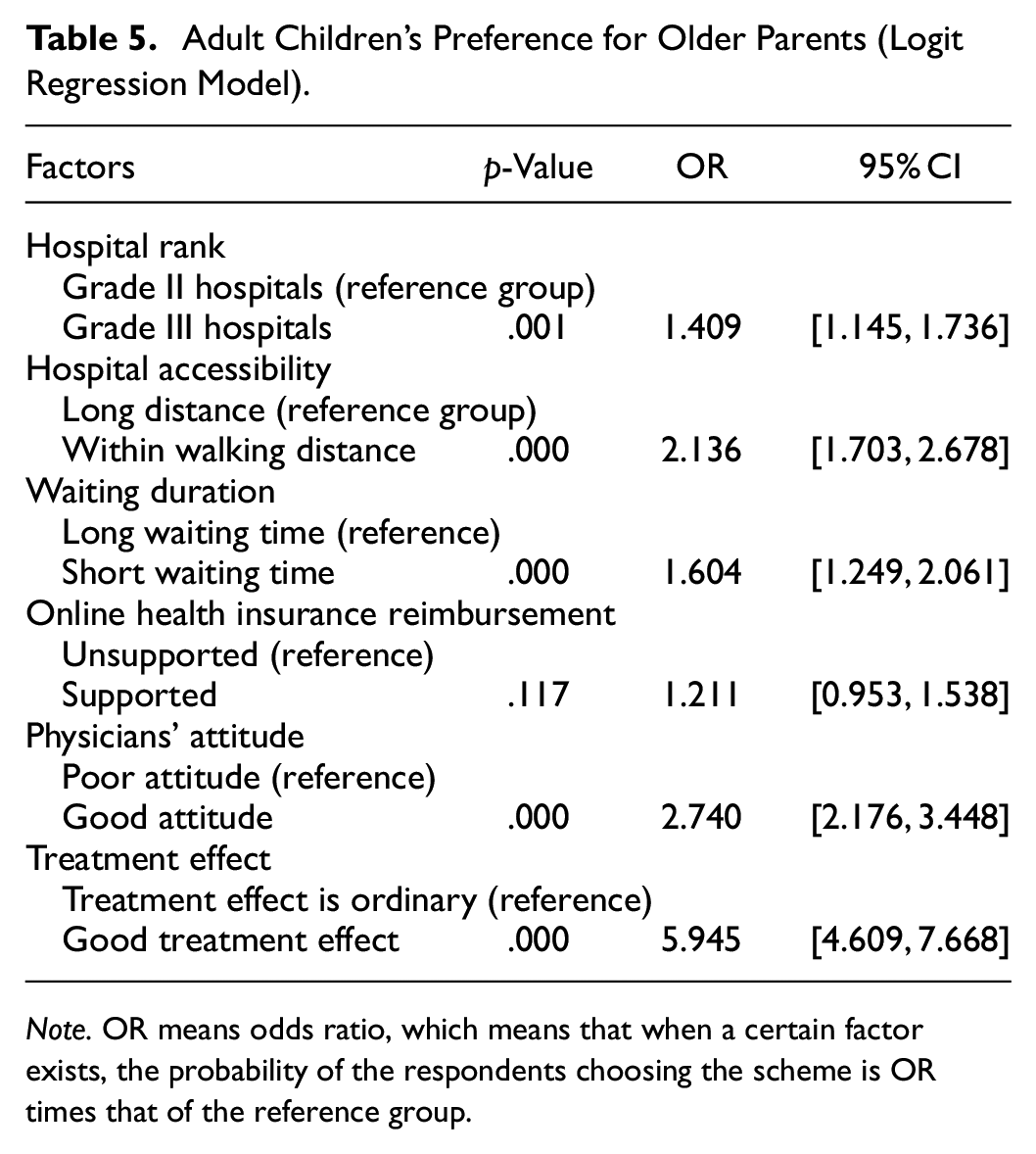
Note. OR means odds ratio, which means that when a certain factor exists, the probability of the respondents choosing the scheme is OR times that of the reference group.
Adult Children’s Gender Effect on Preference for Their Older Parents
The hierarchical logit regression models considering the participants’ gender shows that male and female adult child have different preferences for their parents. Male adult children were more likely to value treatment effect (OR = 5.155), physician’s attitude (OR = 2.611), hospital accessibility (OR = 2.157), and hospital rank (OR = 1.665) in descending order. While, female adult children were more likely to value treatment effect (OR = 7.083), physician’s attitude (OR = 2.933), hospital accessibility (OR = 2.183), waiting time (OR = 1.963) in descending order. Table 6 provides the detail.
Adult Children’s Preference for Older Parents (Male vs. Female).

Note. Among the male respondents, the waiting time is not a significant factor, and among the female respondents, the hospital rank was not significant factor. In addition, the online health insurance reimbursement is not a significant in both groups.
Adult Children’s Education Level Effect on Preference for Their Older Parents
The hierarchical logit regression models considering adult children’s educational level showed that adult children with different education levels had different preferences for their parents. Adult children with low education levels were more likely to value treatment effect(OR = 7.645), physician attitude (OR = 4.687), and hospital accessibility (OR = 2.635). While the adult children with higher education levels were more likely to value treatment effect (OR = 5.793), physician’s attitude (OR = 2.540), hospital accessibility (OR = 2.079), waiting time (OR = 1.610) in descending order. See Table 7 for details.
Adult Children’s Preference for Older Parents (High education vs. Low education).

Parents’ Marital Status Effect on Adult Children’s Preference
The hierarchical logit regression models considering the marital status of the older showed that parents’ marital status affect the choice of adult children. If the older parents were singled, the adult children’s concern ranked as treatment effect (OR = 6.236), physician attitude (OR = 2.712), hospital accessibility (OR = 1.859), waiting time (OR = 1.452) and hospital rank (OR = 1.280) . While, If the parents had a spouse, adult children’s concern ranked as treatment effect (OR = 5.360), hospital accessibility (OR = 3.307), physicians’ attitude (OR = 2.912), waiting duration (OR = 2.168) and hospital rank (OR = 1.910). Table 8 provides the detail.
Adult Children’s Preference for Older Parents (Single aged vs. Aged With a spouse).

Note. The online health insurance reimbursement is not a significant in both groups.
Discussion
Our study shows that treatment effect and physician attitude are the two most important factors, and hospital rank is not that important factors (the fifth important one) when adult children choose doctors for their older parents. These suggest that adult children are logical when facing medical decision for their older parents, and they are likely to choose primary healthcare centers and Grade II hospitals over tertiary hospitals if evidence demonstrates their capability in good therapeutic effect and physician-doctor communication. For the promotion of hierarchical medical system, it is worthwhile to invest greatly in primary healthcare centers and Grade II hospitals for the improvement of their therapeutic effect and attitude of service delivery, and thus divert patients and relieve overcrowding in Grade III hospitals.
Firstly, in addition to treatment effect and physician attitude, hospital accessibility and waiting duration are also significant factors in predicting adult children’s choice. However, our research findings diverge from previous studies concerning the roles of hospital accessibility and waiting duration. For example, in a discretion choice experiment for Iranian patients’ medical service preference presented that physical examination was the most crucial factor (Bahrampour et al., 2018). This may attribute to the self-other choice difference since adult children easily fail to discover the medical service problems encountered by their older parents, and the different scenario designs and cultural variations may also be another explanation. Similarly, many research into patients’ choice of physician online suggest that hospitals and physician reputation positively affect patients’ choice, while hospital distance and waiting duration were not important factors (Deng et al., 2019; Liu et al., 2016). In these studies, although hospital rank and physician professional title were frequently used for the measurement of hospital and physician reputation respectively, this is not necessarily mean they are important at all occasions. Particularly in the realm of online medicial platforms, patients have the convenience of conducting medical consultations remotely through internet-based processes, obviating the importance of factors such as distance and waiting time. Moreover, tertiary hospitals, being more attuned to social media publicity (Zhang, Deng, Evans, et al., 2018), facilitate patients’ access to information about these institutions through online platforms. Consequently, patients may exhibit a stronger inclination toward choosing the familiar tertiary hospitals for engaging in online medical consultations. As for the insignificance of hospital accessibility and waiting duration, the possibility of online health consultation may have reduced their impact. Meanwhile, our study focus on making decision for older parents exclusively, while these studies focused on general patients used online health services, and these two factors are likely to be underreported patients who have already chosen a specific physician online.
Secondly, our study observed older people’s utilization of healthcare service from the perspective of their adult children. It is highly possible that their own preference differs with their children’s preference. Previous studies revealed that for patients over 45 years old, the two factors affecting their preference for medical treatment are the time of arrival at the hospital and hospital reputation (Burge et al., 2004). Drawing from the perspective of self-other decision differences, people are likely to consider more on the loss and risk when making decision for themselves (Von Gunten & Scherer, 2019). In the context of making decision themselves, the older parents might pay much attention on the avoidance of bad consequence of multiple factors, such as too long distance, high charge, and just-so-so hospital reputation. While in the context of making decision for their older parents, adult children’s concern is usually relatively one dimension (J. Z. Xu & Xie, 2012). When an option meets the psychological needs of them, they are likely to choose it because they attribute much attention to the benefits that the decision can bring (Kray & Gonzalez, 1999). In this sense, when adult children make decisions for their older parents, their first intuition is whether their parents could receive better treatment, namely treatment effect.
Finally, our study has distinguished the variations in decision-making when adult children and their older parents under different condition. From the perspective of adult children, The gender effect is that male children attach more attention to the hospital’s rank than female children do. Generally, female children have no obvious preference for Grade III hospitals than their counterparts. This could be explained by the altruism and sensitiveness toward environment changes in females, they turn to have more considerations on their parents’ physical efforts and experience of visiting specific physician (Andreoni & Vesterlund, 2001; Rubin et al., 2006). From the perspective of older parents, adult children are prone to attach greater attention to physician attitude if their parents were divorced or widowed compared to those who has a spouse. This may attribute to the mental status of the older parents. Usually, the physical condition of singled older are worse than their counterparts, and their emotion is more vulnerable than that of the elderly with a complete family (Ha, 2010). It is no wonder that their children cared more on the dimension of physician attitude. In addition, adult children’s variations in educational background leads to different medical preferences for their older parents. Specifically, adult children with higher education are likely to have more considerations compared to more those with lower education. This may pertain to the different understandings of medical and health service between the two groups, and higher educated children always have higher health literacy, which enables them to obtain more information on alternative options and much harder to find a solution for their older parents. However, this requires further qualitative explorations on why adult children make specific choice.
Conclusion
Our study is one of the early efforts, which looks into the medical preference of adult children for their older parents under the online medical environment. We used a discrete choice experiment design to explore the adult children’s rank of seven potential factors influencing older people’s medical decision. This study reveals that, adult children are more likely to choose physician with good treatment effect, good attitude, and hospitals with short distance, short waiting duration and high hospital rank. Among then, the treatment effect is the most concerned factor. In additional, compared to male adult children, female seems more rational on the hospital rank although both gender rank treatment effect, physicians’ attitude, and hospital accessibility as the three most critical factors when making medical decision for their older parents.
Practice Implications
This study explored the utilization of healthcare service of the older from the perspective of their adult children, which broadens the research perspective of healthcare service adoption among the older. In addition, this research enriches the relevant theories of self-other difference in decision making, which investigated the decision-making differences of different roles in the medical context. In this paper, we investigated the influencing factors of adult children’s decision making for their older parents through a discrete choice experiment. Understanding the preference of adult children in healthcare utilization of their older parents contributes to a more comprehensive picture on the formation of healthcare utilization of the elderly under emerging online medical environment. In addition, considering the limitations of Internet usability, the older group are more likely to go offline for medical treatment than that of their younger counterparts. Their actual healthcare needs are easily buried among increasing younger patients in the online medical community. Our study highlights the role of their proxies (i.e., adult children) of decision making, which is quite common in many Chinese families, and provides new directions for optimizing the allocation of medical resources.
Our study also has some implication for online health service for the older generation. For example, since variations in module access order is positively correlates with healthcare service utilization (Y. Xu & Armony, 2016), understanding the preference of the adult children helps the online health platform to optimize their module order for the attraction of adult children’s attention. Another possible improvement is increasing the visibility of primary healthcare centers and Grade-II hospitals. Currently, few primary healthcare centers and Grade-II hospitals and physicians from these healthcare institutions offer their service online compared to Grade-III hospitals. However, our study concludes that physician’s professional title and hospital rank has little impact on the healthcare decision for the adult children. Meanwhile, the accessibility of these two healthcare institutions are higher than that of Grade-III hospitals. It is necessary to encourage physicians’ in primary healthcare centers and Grade-II hospitals to provide highly desired online health service for the older, for example online consultation. For physicians, improvement of their online profiles, expertise, and communication skills can help to build their reputation in the older and their adult children.
Our study is not flawless. First, although our targets are adult children with older parents, most of our participants were below 35 years old with a higher educational background. Adult children in their 20-early 30s are still in the starting stage of their career, and they are more likely to suffer great pressure from soaring housing prices and daily work/life, which will restrict their capability and attention for their older parents. In this sense, our conclusion may not well apply to other adult children’s groups, for example, adult children with affluent income and capability to address their parents’ health needs. Future studies can enlarge the size and heterogeneity of the participants to improve their reliability. Second, limited by the scenario plotted with a focus on a parental inquiry under uncertain conditions, the conclusion may not necessarily apply to the known deadly or chronic diseases. Future research may investigate more choice-making scenarios to explore the dynamic of adult children’s medical decisions for their older parents. The deployment of AI in medicine has also created affluent decision-making scenarios, and future studies can extend to AI-based health service adoption( Zhang et al., 2024). In addition, culture could also be an important factor affecting adult children’s decisions. For example, in non-Asian countries, the culture of Xiao may not be that fundamental in their preferences, and their medical choice for their older parents could be more rational.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by National Natural Science Foundation of China(72104087).
Ethical Statement
We confirm that we have obtained the review committee permission (Refence Number is U201612721).
Data Availability Statement
The datasets generated during and/or analysed during the current study are available from the corresponding author on reasonable request.