
Abstract
Given the escalating incidence of sexual and gender based violence events been reported these days in the world, including Namibia where a week hardly passes by without an IPV case being reported in the local media, continual researches into IPV as well as its attributing factors needs to be carried out in order to have a fully developed and functioning strategies in place to combat and reduce IPV incidence in the country, especially among women and mothers. The purpose of this study was to perform an empirical investigation to the extent and determinants of IPV prevalence among women, especially mothers with under-5 children in Namibia, using a cross-sectional quantitative study design of the 2013 NDHS and a multivariable logit model. Results from this study reveals that socio-demographic and behavioral characteristics such as mother’s age, husband/partner drinks alcohol, husband’s/partner’s education level, husband’s/partner’s age, decision maker and earning more than husband/partner had higher odds of IPV prevalence, while characteristics such as mother’s current marital status, afraid of husband/partner, child’s age, region and currently breastfeeding had lower odds. This study highlights the need to implement prevention and intervention programs that aim at encouraging economic empowerment of mothers with under-5 children as a form of protective shield of IPV prevalence by the Namibian government as well as organizations centered on women’s rights, advocacies and development. These preventative measures should begin at an early age, while both prevention and intervention programs should specifically target the high risk ages of 30 to 49 as IPV emerges in dating couples.
Keywords
Introduction
Although violence against women is a major public health issue and can be linked to a variety of negative physical, mental, sexual and reproductive health outcomes, Intimate Partner Violence (IPV) is still one of the most prevalent types of violence against women globally. IPV can be defined as a behavior exhibited by an intimate partner or ex-partner that causes physical, sexual or psychological harm, including physical aggression, sexual coercion and psychological abuse or controlling behavior (Anderson & van Ee, 2018). It can occur among persons aged 16 years or over who are or have been intimate partners. In addition, it comes with adverse effects and is mostly borne by women. Sadly, among women who are mothers, IPV appears in different varieties of forms, with mothers most often not wanting to acknowledge nor discuss the violence in their respective homes once it ends, even though the exposure to it (already) impacted their daily functioning activities (Anderson & van Ee, 2018). Violence against women is usually done by their intimate partner and it is not always in the form of physical violence only, but it can also be emotional, verbal, forceful isolation from family and friends, as well as denial of basic needs such as food and money (Alokan, 2013; World Health Organization [WHO], 2013). In other words, IPV involves physical violence ranging from slapping, striking, kicking, beating, sexual violence, mental abuse, as well as controlling behaviors by an intimate partner (Kebede et al., 2022). According to Joshi and Kharel (2008), IPV is usually inflicted by the perpetrator to gain power and control over their partner, with most reported IPV cases performed by intimate male partners toward their intimate women partners.
Looking at the socio-ecological framework of violence against women, violence is not a result of one single factor. It can occur at individual level, relationship level, community level and society levels as explained by the Heise (1998) framework shown in Figure 1. Individual level includes all the characteristics of an individual woman that makes her vulnerable to violence such as substance abuse, history of violence and low educational attainment, while relationship level focuses on how social relationships with family, peers and intimate partners influences the woman’s behavior and experience toward violence. On the other hand, community level focuses on the social characteristics structures such as neighborhood, workplace and schools that may make the perpetrator or make someone a victim of violence. The society levels focus on the broad societal factors that encourage or influence violence such as norms of male dominance, and the social, economic, educational and health policies that contribute to social and economic inequalities (Heise, 1998). In most countries where the males have been historically and traditionally considered as the main provider of the house and more powerful figure in society, such male superiority and power can be linked to IPV episodes. This in turn makes a woman the most abused object at home in these countries. In the place where they are supposed to feel the greatest safety and security, women often face terror from physical, psychological, sexual and economic abuse, with many having no choice but to stay with the perpetrator (Joshi & Kharel, 2008). Although certain factors can lead partners to become violent against their respective partners such as alcohol use, drug use, stress and insecurities, women who experience IPV do not often talk about it openly. This can be due to fear, family secrecy, cultural norms, shame, and community stigma. According to Joshi and Kharel (2008), domestic violence against women drains their energy, which in turns can affect their physical and mental health, and erodes self-esteem among these women.

Social-ecological model of violence against women (extracted from Heise, 1998).
Globally, about 35% of women have experienced violence by an intimate partner in their lifetime (Chilanga et al., 2020), with severe domestic violence particularly experienced in developing countries such as Bangladesh and Sub-Saharan Africa (Hossain et al., 2014). The prevalence of IPV against women still remains high in Sub-Saharan Africa, with approximately 45.6% of women in these Sub-Saharan African countries having experienced at least one form of IPV in their lifetime. Benebo et al. (2018) highlighted that reported IPV cases were more common in southern Africa including Namibia and that although men were also victims of IPV, women mostly bore the overwhelming burden. In Namibia, Bikinesi et al. (2017) estimated the lifetime prevalence of IPV in Windhoek (the capital city of Namibia) to be around 36%. Recently, Pérez-Martínez et al. (2023) estimated that 6% of women in the European Union aged 18 to 29 years who have been in intimate relationships have experienced physical and/or sexual IPV, while as many as 48% have experienced psychological IPV. For non-European Union countries such as countries in South America, Asia and Africa, Pérez-Martínez et al. (2023) estimated a current physical and psychological IPV prevalence of around 30% among women aged 15 to 24 years. Furthermore, IPV is an endemic problem in Namibia, with hardly a week passing by without an IPV case being reported in the local media (Bikinesi et al., 2017). It was further revealed by Bikinesi et al. (2017) that over one-third of women in Namibia have reported physical and/or sexual violence from an intimate partner, with 90% of the cases among pregnant and women with young children perpetrated by the fathers of the children.
Over the years, several factors have been identified to be associated with IPV experience among women, including socio-demographic, socio-economic and behavioral indicators such as length of stay in an intimate relationship, partner’s alcohol and substance abuse, community and societal levels, educational attainment, age difference between couples, women cohabitating with their partners without formally being married, culture/traditional norms and phenomena, decision-making capacity, religion, employment status, occupation, marital status and wealth status (Abramsky et al., 2011; Ahinkorah et al., 2018; Bazargan-Hejazi et al., 2013; Chilanga et al., 2020; Siahaan et al., 2022; Willie et al., 2018). In addition, IPV has been linked to a number of negative health outcomes for abused women and mothers, including bodily harm, death, emotional distress, social isolation, pregnancy and sexual morbidity, depression symptoms, vulnerability to human immunodeficiency virus transmission, still-birth, abortion and premature delivery (Anderson & van Ee, 2018; Chilanga et al., 2020; Siemieniuk et al., 2013; Wagman et al., 2012). However, the long term effects on IPV survivors can never be completely erased, as survivors (who are lucky to be alive) most often end up with long-term poor health outcomes, physical scars and psychological traumas, even long after the abuse has stopped. In the study by Benebo et al. (2018), it was found that the imbalance of power in the patriarchal society tended to contribute to IPV, while IPV also affected those close to the victim including children. In addition, WHO (2013) revealed that there was an association between IPV and child abuse within the same household. In her studies, Alokan (2013) found that wife battering (a common form of IPV) affected the women and their children who witnessed these battering, and concluded that IPV does not only affect the victim but also has negative emotional and social wellbeing consequences on the whole family, especially the children. According to Joshi and Kharel (2008) and WHO (2013), children who witnessed IPV acts on their mothers often suffered from psychological effects and were most likely to become perpetrators themselves. In other words, if there are violence incidents between parents in the family house, these parents will not have time to spend and show love to their children, which can result in these children growing up without love and more likely to become victims or perpetrators of IPV in the future.
Looking at the attitudes toward IPV, including norms and unequal power relations as well as women’s rights, attitudes toward IPV has been known as a predictor of IPV victimization and perpetration, with more women generally believed to justify IPV than men. In their study, Okenwa-Emegwa et al. (2016) revealed that justification of abuse was higher among women who were younger, while less justification was present among women living in the urban areas, those with a higher education attainment and those who were employed. Similarly, Tran et al. (2016) concluded that IPV against women was prevalent in low- and middle-income countries, with women who were less educated and those with primary education attainment and unemployed the most affected by IPV (Oche et al., 2020). Violence against women has long been embedded in most developing countries’ cultural practices and norms, with violence incidences such as wife beatings more acceptable in Africa and South Asia, but least common in East and Central Europe and Latin America (Tran et al., 2016). Joshi and Kharel (2008) and Alokan (2013) further revealed that the historical unequal power relations between men and women was also a key predictor of IPV, with men being the ones exercising their might and vocals, thus their frustration is thrown on their weaker counterpart (women). Alokan (2013) concluded that the historical unequal power relations have led to male dominance and discrimination against women which forces them into subordinate positions when compared to men. However, a reduction in violence against women can be achieved through social change including social norms and cultural practices (ActionAid, 2012), starting with the accomplishment of goal 5 of the United Nations’ Sustainable Development Goals (SDG) that aims to achieve gender equality and empowerment of all women and girls. Furthermore, WHO (2013) outlined that violence against women has great health impacts and violates women rights. The struggle of women’s rights is about making their lives matter at all times and everywhere, which means stopping discrimination and violence against them (Joshi & Kharel, 2008), especially when women are of great importance to the growth and development of the world. They are homemakers and permanent change is usually obtained through them. Therefore, all women deserve better treatment, but sadly the opposite is at its peak (Alokan, 2013).
Given the escalating incidence of sexual and gender based violence events been reported these days in the world, including Namibia where a week hardly passes by without an IPV case being reported in the local media, continual researches into IPV as well as its attributing factors needs to be carried out in order to have a fully developed and functioning strategies in place to combat and reduce IPV incidence in the country, especially among women and mothers. When women, in particular mothers, are subjected to IPV, they are more likely to develop post-traumatic stress disorder, anxiety, despair, suicidal behavior, sleeping and eating disorders, social dysfunction, substance abuse, as well as unintended pregnancies (Memiah et al., 2020). Most often mothers tend to stay in abusive relationships for a variety of reasons, including their financial condition, the circumstances around their children, low self-esteem and self-worth, peer and societal pressure, and other factors that make leaving difficult for them. Although, quite a number of studies have been carried out to examine the prevalence of domestic violence and its associated factors on women in Namibia, no empirical investigation has been conducted to investigate the extent and determinants of IPV prevalence among mothers with under-5 children in the country, despite the increased prevalence of IPV reported in the media among the women population in Namibia. Hence, this gap in IPV research in the country merits attention. For this reason, this study was aimed at identifying the determinants of IPV prevalence among mothers with under-5 children in Namibia. Identifying these determinants can ensure effective awareness and intervention programs to reduce the IPV prevalence among mothers with under-5 children. In addition, resonating one of the recommendations made by Joshi and Kharel (2008) that prevalence data are often needed to convince policy makers of both the pervasiveness of violence and its serious implications for women’s health and development, studying violence against women, including IPV, is of paramount importance. Thus, findings from this study can provide useful insights for evidence-based IPV awareness campaigns as well as fill the above mentioned missing gap in IPV research in the country, thereby advancing the SDG of gender equality and empowering mothers with under-5 children in the country.
Material and Methods
The data used in this study was obtained from the 2013 Namibia Demographic and Health Survey (NDHS) funded by the United States Agency for International Development, in collaboration with Namibia’s Ministry of Health and Social Services, as part of their global Demographic and Health Survey (DHS) programs. The 2013 NDHS is the fourth & latest comprehensive, national-level population and health survey conducted in Namibia that provides demographic, socioeconomic and health data information for the country, with the study initiated in April 2012 and the data collection aspect carried out from May to September 2013 across all then 13 administrative regions in Namibia (Ministry of Health and Social Services & ICF International, 2014). As of 2014, Namibia now has 14 administrative regions.
The sampling design used in the 2013 NDHS was a two-stage stratified sampling design, with stratification achieved by separating each of the 13 administrative regions into urban and rural areas, resulting in 26 sampling strata (13 rural strata and 13 urban strata). Stage one entailed the selection of primary sampling units from the urban areas (269) and rural areas (285) while stage two entailed the selection of a fixed number of households (20) from both the urban and rural clusters according to equal probability systematic sampling (Ministry of Health and Social Services & ICF International, 2014). More detailed information about the sampling design and methods as well as the entire survey can be found in the 2013/14 NDHS report, freely available online on the DHS website, while the 2013 NDHS data can be obtained from the website after the user’s agreement of the DHS program has been completed. The inclusion criteria for this study were all women aged 15 to 49 years who were mothers of children under the age of 5 years who participated and provided information in the 2013 NDHS. Mothers with incomplete, non-response or missing information were excluded from this study. The individual mothers considered in this study were identified from the NDHS as per the inclusion criteria for this study.
Descriptive Analysis
The socio-demographic and behavioral characteristics of the mothers with under-5 children considered in this study were husband/partner drinks alcohol, afraid of husband/partner, child’s age (in months), mother’s age (in years), region, highest educational level, sex of household head, age of household head (in years), currently breastfeeding, current marital status, cohabitation duration, husband’s/partner’s education level, husband’s/partner’s occupation, husband’s/partner’s age (in years), decision maker and earns more than husband/partner as captured in the 2013 NDHS data. The individual mothers considered in this study were identified from the NDHS as per the inclusion criteria for this study.
Moreover, in order to determine their experience levels to physical, emotional and sexual violence during the 2013 NDHS period, each interviewed woman was asked questions such as did your husband/partner/ex-partner: “Push you, shake you, or throw something at you?,”“Slap you?,”“Twist your arm or pull your hair?,”“Punch you with his fist or with something that could hurt you?,”“Kick you, drag you, or beat you up?,”“Try to choke you or burn you on purpose?,”“Threaten or attack you with a knife, gun, or any other weapon?,”“Say or do something to humiliate you in front of others?,”“Threaten to hurt or harm you or someone close to you?,”“Insult you or make you feel bad about yourself?,”“Physically forced (you) to have sexual intercourse with him when (you) did not want to?,”“Physically forced (you) to perform any other sexual acts (you) did not want to?” and “Forced (you) with threats or in any other way to perform sexual acts (you) did not want to?.” Their obtained responses to these questions were later tabulated under the “Experienced any emotional violence (D103A-D103C),”“Experienced any severe violence (D105D-D105F) by husband/partner” and “Experienced any sexual violence (D105H-D105I, D105K) by husband/partner” variables in the NDHS data, with response options of “Yes” or “No.” For this current study, under each of these variables, a score of 1 was given to the “Yes” responses (indicating an experience), while a 0 was given to the “No” responses (indicating a no experience) and these were later used to determine the IPV experience status of the mothers with under-5 children. The IPV score per mother was calculated by summing up their scores across the three variables (experienced any emotional violence, experienced any severe violence and experienced any sexual violence), after which their respective IPV experience status was determined using the IPV score as follows:

Similarly, the wealth index status of a household interviewed in the 2013 NDHS was a composite measure of the household’s cumulative living standard, calculated using the household’s ownership of selected assets such as televisions, bicycles/vehicles, materials used for housing construction, as well as dwelling characteristics such as source of drinking water, sanitation facilities, type of flooring materials, types of water access and sanitation facilities. More detailed information about the construction of the wealth index and the remaining socio-demographic and behavioral characteristics considered in this study can be found in the 2013/14 NDHS report, freely available online on the DHS website.
Statistical Analysis
R software (version 4.2.2) was used for the data cleaning, variables re-coding and data analysis. Pearson’s chi-square test was performed to examine the association between the mothers’ IPV experience status and their socio-demographic and behavioral characteristics, while the effect of the socio-demographic and behavioral characteristics on the mothers’ IPV experience status was determined using a multivariable logit model, considering the binary nature of the mothers’ IPV experience levels. This model, with a general format of:

where

In this study,
Results
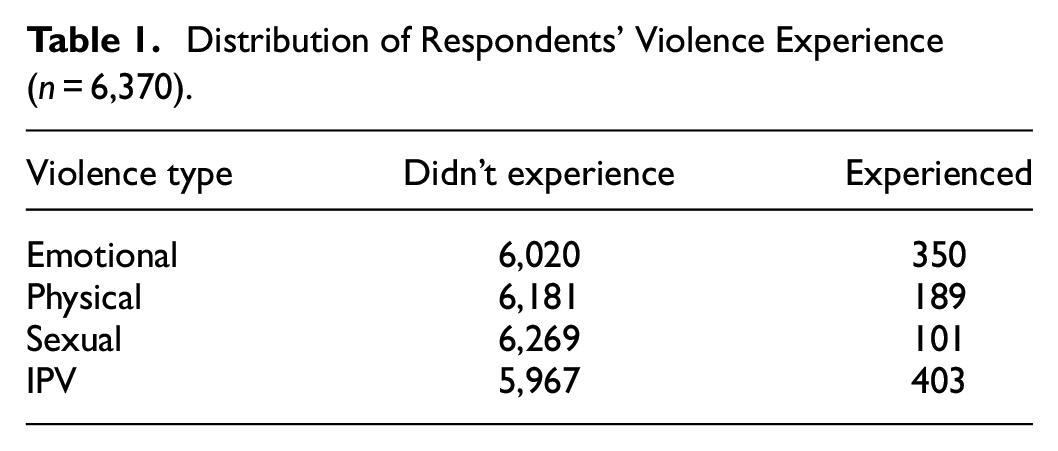
Out of the 9,176 women aged 15 to 49 years interviewed in the 2013 NDHS, a total of 6,370 were mothers with under-5 children and were considered in this study as per the inclusion criteria of this study. Of the 6,370 mothers with under-5 children, 350 experienced emotional violence, 189 experienced physical violence and 101 experienced sexual violence as shown in Table 1, making emotional violence more prevalent among the three main types of violence constituting IPV among these mothers. Out of the 6,370 mothers with under-5 children considered, 403 (6.33%) experienced IPV, while 5967 (93.67%) did not as shown in Table 2.
Distribution of Respondents’ Violence Experience (n = 6,370).
Weighted Summary Statistics of the Respondents’ Socio-Demographic and Behavioral Characteristics and IPV Experience.
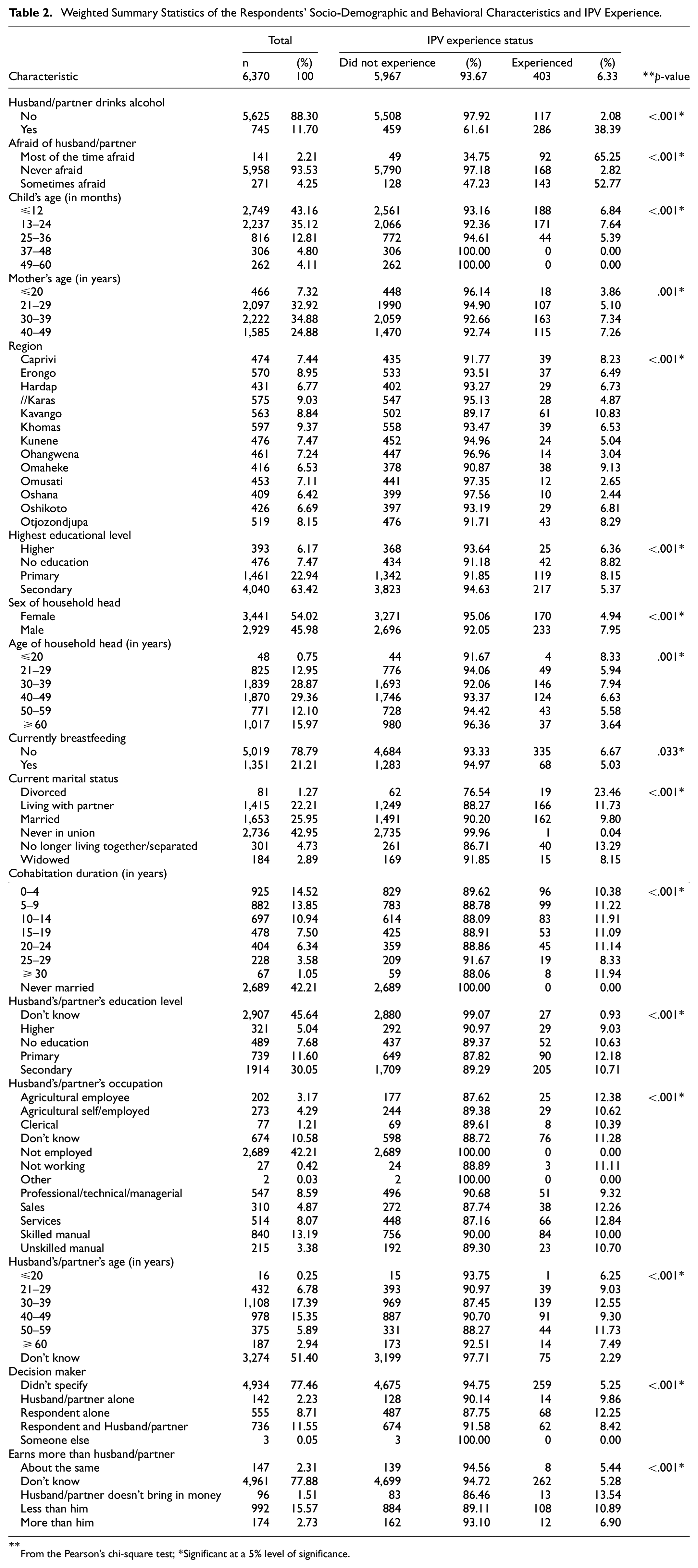
From the Pearson’s chi-square test; *Significant at a 5% level of significance.
With respect to the socio-demographic and behavioral characteristics, out of the 403 mothers with under-5 children who experienced IPV, a high number had 30 to 39 years old husbands/partners (n = 139) who drank alcohol (n = 286) and lived in the Kavango region (n = 61) as shown in Table 2. In addition, a high number of these women were aged 30 to 39 years old (n = 163), had secondary education (n = 217) as their highest educational attainment and caring for at most 12 months old children (n = 188). A high number were not currently breastfeeding (n = 335), with their husbands/partners having secondary education (n = 205) as their highest educational attainment and worked as skilled manual workers (n = 84).
Association Examinations
From Table 2, at a 5% level of significance, the mother’s age (p = .001), region (p < .001), highest educational level (p < .001), sex of household head (p < .001), age of household head (p = .001), currently breastfeeding (p = .033), current marital status (p < .001), cohabitation duration (p < .001), husband’s/partner’s education level (p < .001), husband’s/partner’s occupation (p < .001), husband’s/partner’s age (p < .001), decision maker (p < .001), husband/partner drinks alcohol (p < .001), afraid of husband/partner (p < .001), child’s age (p < .001) and earning more than husband/partner (p < .001) can be concluded to be significantly associated with the IPV experience status. All these characteristics with significant associations were included in the fitted multivariable logit model and the subsequent results shown in Table 3.
Impact of Respondents’ Socio-Demographic and Behavioral Characteristics on IPV Experience.

Significant at a 5% level of significance; (ref)=reference category.
Effects on IPV Experience
From Table 3, with a significant p-value at a 5% level of significance, the odds of experiencing IPV for mothers with under-5 children who were never afraid (AOR = 0.015; p < .001; 95% CI [0.011, 0.022]) and sometimes afraid (AOR = 0.595; p < .001; 95% CI [0.389, 0.903]) of their husbands/partners were 0.02 and 0.60 times lower compared to the odds for those who were most of the time afraid of their husbands/partners. Likewise, the odds of experiencing IPV for mothers with under-5 children whose children were 49 to 60 months old (AOR = 0.526; p = .035; 95% CI [0.285, 0.945]) were 0.53 times lower compared to the odds for those whose children were at most 12 months old, while the odds of experiencing IPV for mothers with under-5 children who did not know their husbands/partners’ age (AOR = 0.236; p < .001; 95% CI [0.159, 0.356]) were 0.24 times lower compared to the odds for those whose husbands/partners were aged 21 to 29 years old. The odds of experiencing IPV for mothers with under-5 children living in the Oshana (AOR = 0.280; p < .001; 95% CI [0.130, 0.546]), Omusati (AOR = 0.304; p < .001; 95% CI [0.150, 0.570]), Ohangwena (AOR = 0.349; p = .001; 95% CI [0.181, 0.637]), //Karas (AOR = 0.571; p = .029; 95% CI [0.343, 0.939]) and Kunene (AOR = 0.592; p = .050; 95% CI [0.346, 0.994]) regions were 0.28 and 0.59 times lower compared to the odds for those living in the Caprivi region, while the odds of experiencing IPV for mothers with under-5 children who were currently breastfeeding (AOR = 0.741; p = .028; 95% CI [0.563, 0.962]) were 0.74 times lower compared to the odds for those not currently breastfeeding. Moreover, the odds of experiencing IPV for mothers with under-5 children who were never in a union (AOR = 0.02; p < .001; 95% CI [0.010, 0.063]), widowed (AOR = 0.290; p = .001; 95% CI [0.137, 0.603]), married (AOR = 0.355; p < .001; 95% CI [0.211, 0.623]), living with their partners (AOR = 0.434; p = .002; 95% CI [0.258, 0.761]) and no longer living together/separated (AOR = 0.500; p = .027; 95% CI [0.274, 0.937]) were 0.02 and 0.50 times lower compared to the odds for those who were divorced.
On the other hand, the odds of experiencing IPV for mothers with under-5 children whose husbands/partners drank alcohol (AOR = 29.333; p < .001; 95% CI [23.249, 37.227]) were 29.33 times higher compared to the odds for those whose husbands/partners did not drink alcohol, while the odds of experiencing IPV for mothers with under-5 children whose husbands/partners were aged 30 to 39 years old (AOR = 1.446; p = .050; 95% CI [1.004, 2.126]) were 1.45 times higher compared to the odds for those whose husbands/partners were aged 21 to 29 years as shown in Table 3. Similarly, the odds of experiencing IPV for mothers with under-5 children who were aged 40 to 49 (AOR = 1.947; p = .010; 95% CI [1.202, 3.341]) and 30 to 39 (AOR = 1.970; p = .008; 95% CI [1.232, 3.350]) years old were 1.95 and 1.97 times higher compared to the odds for those who were aged 20 years or less, while the odds of experiencing IPV for mothers with under-5 children living in a male-headed households (AOR = 1.663; p < .001; 95% CI [1.357, 2.042]) were 1.66 times higher compared to the odds for those living in a female-headed households. The odds of experiencing IPV for mothers with under-5 children whose husbands/partners had higher (AOR = 10.594; p < .001; 95% CI [6.180, 18.220]), no education (AOR = 12.693; p < .001; 95% CI [7.959, 20.693]), secondary (AOR = 12.795; p < .001; 95% CI [8.688, 19.621]) and primary (AOR = 14.792; p < .001; 95% CI [9.679, 23.344]) education as their highest educational attainment were 10.59 and 14.79 times higher compared to the odds for those who did not know the highest educational attainment of their husbands/partners.
Furthermore, the odds of experiencing IPV for mothers with under-5 children whose husbands/partners and themselves (AOR = 1.660; p = .001; 95% CI [1.235, 2.201]), husbands/partners alone (AOR = 1.974; p = .018; 95% CI [1.074, 3.358]) and themselves alone (AOR = 2.520; p < .001; 95% CI [1.887, 3.326]) were decision makers in their households were 1.66 and 2.52 times higher compared to the odds for those who did not specify who the decision maker was in their households. Likewise, the odds of experiencing IPV for mothers with under-5 children who earned less than their husbands/partners (AOR = 2.123; p = .046; 95% CI [1.076, 4.822]) and those whose husbands/partners do not bring in money (AOR = 2.721; p = .033; 95% CI [1.100, 7.134]) were 2.12 and 2.72 times higher compared to the odds for those who earned the same amount as their husbands/partners.
Discussion
In this study, a multivariable logit model was used to examine the determinants of IPV prevalence against mothers with under-5 children. A high number of the mothers with under-5 children who experienced IPV were aged 30 to 39 years old, had secondary education as their highest educational attainment, were never afraid of their husbands/partners, had 30 to 39 years old husbands/partners who drank alcohol, lived in the Kavango region in male-headed households whose head was aged 30 to 39 years, and lived with their partners and married for a duration of 0 to 9 years, with their husbands/partners having secondary education as their highest educational attainment.
IPV prevalence was more likely to occur for mothers with under-5 children who were aged 30 to 49 years old, whose husbands/partners drank alcohol and living in a male-headed household. Likewise, IPV prevalence was more likely to occur for mothers with under-5 children who earned less than their husbands/partners, those whose husbands/partners do not bring in money, as well as those whose husbands/partners alone were the decision makers in their households. These findings are not surprising and can be attributed to the long-held tradition of male dominance and patriarchal ideology which has allowed men to freely dominate their women, thereby making IPV an acceptable cultural norm in most societies. Husbands/partners, most especially those who are heads and decision makers in their households, often believe that they have the right to govern and physically correct their spouses/female partners as they deem fit since women in general are still being seen as inferior beings in most societies, while some believe that it is justifiable for husbands/partners to beat their wives/female partners as a means of corrections and disciplines. These findings also concur with those made by Hindin (2003) and Bazargan-Hejazi et al. (2013), with Bazargan-Hejazi et al. (2013) concluding that in families where the husbands/partners had traditional gender-role beliefs, numerous incidences of assaults against their women will be prominent, while Hindin (2003) concluded that in as much as women can imagine equality in marriage/relationship, they are unable to break with the social and gender norms, and expectations that dictate men’s powerful position in marriage/relationship, particularly in terms of decision-making and financial dependence.
Similarly, mothers who earned less than their husbands/partners vastly depend on their husbands/partners financially, thereby rendering these mothers unable to make financial decisions in the relationship. Thus, such mothers do not have economic empowerment which can be a protective factor against IPV. This finding also agrees with Osuorah et al. (2012) whose findings showed that the employment status of mothers which reflects the socio-economic class of their empowerment played a significant role in their IPV experience. Moreover, it is common knowledge that husbands/partners that are alcohol drinkers are more likely to be violent because of the effect of alcohol which reduces their self-control as well as influences their decisions and exaggerates underlining suppressed issues in their relationships. This finding is similar to those made by Chilanga et al. (2020) where it was concluded that having a husband/partner that drinks alcohol increases the likelihood of IPV for women who are in relationship with these types of husbands/partners.
However, IPV prevalence was less likely to occur for mothers with under-5 children who were never afraid and sometimes afraid of their husbands/partners, whose children were 49 to 60 months old and living in the Oshana, Omusati, Ohangwena, //Karas and Kunene regions. Likewise, IPV prevalence was less likely to occur for mothers with under-5 children who were currently breastfeeding, never in a union, widowed, married, living with their partners and no longer living together with their partners. These findings are not surprising as the older the children get, the lesser the amount of time needed by the mothers to indulge them, thus, creating more time for the mothers to spend with their husbands/partners. Likewise, it is believed that husbands/partners of mothers that are currently breastfeeding tend to be more sympathetic and supportive toward their wives/partners especially when they are still breastfeeding their children. With Oshana, Omusati, Ohangwena, //Karas and Kunene regions being some of the underdeveloped regions in Namibia with limited employment opportunities, most husbands/partners of mothers with under-5 children are more likely to be away from their households for a longer period of time seeking full employment opportunities in more developed regions with business hubs and employment opportunities to provide food and basic essential needs for their respective households and themselves. As a result, such couples will not fully be living in the same households under the same roof most of the time, thus, reducing the chances of IPV episodes.
Moreover, mothers who are always afraid of their husbands/partners will always experience high prevalence of IPV as they are always fearful of being hurt or killed by their partners whenever they have a disagreement or misunderstanding. This finding concurs with those made by Hardesty and Ganong (2006) who found that mothers who feared their husbands/partners never want to engage in long combative talks with their husbands/partners even if these talks have to do with their children, behaviors and/or wellbeing.
Limitations
Majority of the questions in the 2013 NDHS questionnaire relied heavily on memory recalling of the participating mothers which could have led to the possibilities of systematic under-reporting of some family socio-demographic and behavioral characteristics as well as general information. In addition, since violence in general within families and households as well as IPV are some of the most sensitive information to share with non-household and non-family members and still strongly seeing as taboo topics to openly discuss in some communities, there is a possibility that interviewed mothers did not give their true emotional, sexual and physical violence experience during the 2013 NDHS survey. Also, with IPV considered internal household problems, it is likely that the IPV cases reported in the 2013 NDHS survey were under-reported, especially when some women were reluctant and/or afraid to report or acknowledge its occurrence in their lives, while some communities might have had reservations about reporting IPV cases in general. This in turn might have had an implication on the prevalence of IPV cases in the country. Moreover, the cross-sectional nature of the DHS does not allow for the establishment of causal inferences. While the most recent nationally representative dataset from Namibia (2013 NDHS) was used for this study, the time between 2013 and 2023 might have brought about significant changes, thus, the findings about the geographical differences may have changed and interpretations were made with caution.
Conclusion
With socio-demographic and behavioral characteristics such as mother’s age, husband/partner drinks alcohol, sex of household head, husband’s/partner’s education level, husband’s/partner’s age, decision maker and earning more than husband/partner creating more likelihoods of IPV prevalence, while characteristics such as mother’s current marital status, afraid of husband/partner, child’s age, region and currently breastfeeding had fewer likelihoods, it is therefore recommended that programs that aim at encouraging women economic empowerment should be implemented by the Namibian government as a form of protective factor of IPV. The implementation of these programs can contribute to the achievement of the United Nations’ SDG (goal 5) that aims at promoting gender equality and empowering women. Furthermore, community awareness gatherings should be implemented at the societal level to create awareness of the effects that some cultural norms and practices have toward the contribution of IPV episodes. Likewise, regular education programs centered at advocating and raising awareness that can help with educating girls and women on how to (i) make domestic decision, (ii) recognize what their rights are, (iii) recognize when their rights are being violated, and (iv) recognize injustice treatment in their intimate relationships should be implemented by the Namibian government as well as organizations centered on women’s rights, advocacies and development. Besides, if women in general were provided with alternate options to living with an (IPV-) abusive husbands/partners as well as shown means to gain financial and emotional independence from an abusive husbands/partners, then perhaps IPV prevalence against women, including mothers, will significantly reduce and become a thing of the past.
Moreover, seeing as the prevalence of IPV has remained high worldwide and in Namibia, regular intervention programs such as men’s conference that aims at (i) educating men and boys on the importance of women in the society, (ii) promoting equal decision-making behavior, (iii) discussing IPV issues and means of overcoming them, as well as (iv) discussing how alcohol intakes can lead to increased IPV prevalence should be implemented and made mandatory especially for young men and those in intimate relationships with mothers of under-5 children. This can easily be achieved through constant engagements and collaborations with community-based organizations such as churches, traditional authorities, community leaders, local authorities and regional councils. However, preventative measures should begin at an early age, while both prevention and intervention programs should specifically target the high risk ages of 30 to 49 as IPV emerges in dating couples. In addition, further research on the IPV experience of mothers on children’s wellbeing as well as the effect of maternal exposure to IPV on children aged 0 to 4 year old should be precipitously conducted in Namibia since no comprehensive investigations of these types of studies have been carried out in the country to the knowledge of the authors. Likewise, a longitudinal study that will examine the same specific population group of women to detect any changes that might (have) occur over a (specified) longer period of time is recommended, given the causality limitations that comes with cross-sectional study designs.
Footnotes
Acknowledgements
The United States Agency for International Development is thanked for availing the 2013 NDHS data.
Author Contributions
OO and NS conceived and designed the review. OO conducted the analysis of data, interpretation of findings and prepared the first draft of the manuscript. Final version of the manuscript was read and approved by both the authors.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
All methods were carried out in accordance with the University of Namibia’s Research Ethics Policy and Guidelines. Ethical approval was not sought for this study since the 2013 NDHS data used in this study is freely available on a public domain and downloadable from the DHS website. No separate permission is required for data usage and publication. Additionally, this study followed all ethical standards for research without direct contact with human or animal subjects as there were no names of persons or household addresses recorded in the DHS data.
Data Availability Statement
Data sharing not applicable to this article as no datasets were generated or analyzed during the current study.