
Abstract
Indigenous Australians experience a high prevalence of sexual assault, yet a regional sexual assault service found few Indigenous Australians accessed their services. This prompted exploration of how its services might be improved. A resultant systematic search of the literature is reported in this article. Seven electronic databases and seven websites were systematically searched for peer reviewed and gray literature documenting responses to the sexual assault of Indigenous Australians. These publications were then classified by response type and study type. Twenty-three publications met the inclusion criteria. They included studies of legal justice, media, and community-based and mainstream service responses for Indigenous survivors and perpetrators. We located program descriptions, measurement, and descriptive research, but no intervention studies. There is currently insufficient evidence to confidently prescribe what works to effectively respond to Indigenous Australian sexual assault. The study revealed an urgent need for researchers, Indigenous communities, and services to work together to develop the evidence base.
Introduction
Sexual assault is a crime (New South Wales [NSW] Ombudsman, 2012). Sexual assault occurs when any person has sexual intercourse with another person without the consent of the other person and who knows that the other person does not consent to the sexual intercourse (NSW Crimes Act 1900, No. 40; Australasian Legal Information Institute, 2010). It should be noted however that there are variations in the definition of sexual assault between states and territories. Finding reliable data about the nature and extent of Indigenous Australian sexual assault is extremely difficult, as in some cases it is subsumed within Australian federal and state/territory governments’ definitions of, and statistics for, family violence (Keel, 2004). Furthermore, the statistics for family violence are not always available or methodologically reliable. In part, this is because victims and survivors may be reluctant to report experiences of sexual assault to Police or other agencies. Yet anecdotal evidence and submissions to inquiries indicate that sexual violence in Indigenous communities “occurs at rates that far exceed those for non-Indigenous Australians” (Lievore, 2003, p. 56). Indigenous women are particularly at risk of violence, being 12 times more likely to be the victims/survivors of assault than non-Indigenous women; in rural and remote Western Australia women are 45 times more likely to be assaulted by their spouse or partner than non-Indigenous women (Keel, 2004). Female Aboriginal children in NSW were also found to be 2.5 times more likely to be at risk of sexual assault than non-Aboriginal children (Aboriginal Child Sexual Assault Taskforce, 2006).
Many Indigenous Australians experience multiple risk factors for sexual assault. One explanation for the high prevalence of sexual assault is that risk factors occur at disproportionately higher rates, thereby placing Indigenous Australians at significantly higher risk of sexual abuse than the general population (Bodeker, 2008). In addition to being younger and female, risk factors for sexual assault at the societal level have been consistently associated with poverty as well as social norms that reflect male dominance (Rothman, Butchard, & Cerda, 2003). At the individual level, those who physically or sexually assault their female partners are more likely to have a history of witnessing inter-parental violence, and having experienced child abuse and substance misuse (Rothman et al., 2003). Furthermore, the higher levels of disadvantage experienced by Indigenous Australians increases their exposure to stressful life events (Gracey & King, 2009; Keel, 2004).
A seminal paper by Bligh (1983) described Aboriginal women’s personal experiences in seeking responses to sexual assault. In exploring why Aboriginal women were not accessing a Rape Crisis Centre in South Australia, Bligh analyzed data from 100 interviews with individuals and groups, including church, college, and small social groups. She found that women were being raped across ages, from 4 to 58. Aboriginal and non-Aboriginal men were raping Aboriginal women, and often a number of rapists were involved. Women rarely reported rape to Police, the Department of Community Welfare, Aboriginal, or women’s organizations. Women experienced Police to be often indifferent or disbelieving and convictions for rape were rare. Often, to some extent, women blamed themselves, and had taken on a narrative that they were an “easy lay” and particularly deserved this label if they had been drinking alcohol. Many women were not aware of services such as Rape Crisis Centres. However, many said that they would like to have an Aboriginal counselor at the Rape Crisis Centre as a more appropriate choice to meet their needs; while 10% of women reported that the Aboriginality of a counselor was not essential so long as support was available.
Despite high level government, legal, media, and community concern about the extent of sexual assault experienced by Indigenous Australians (e.g., Gordon, Hallahan, & Henry, 2002; Government of Western Australia, 2002; NSW Ombudsman, 2012; Wild & Anderson, 2007), little is known about service responses implemented nationally to provide counseling, medical, and support services for Indigenous survivors/victims of sexual assault or to manage and treat perpetrators. Published reviews of sexual assault responses targeting Indigenous Australians have been undertaken, but none are systematic (Keel, 2004; Stubbs, 2009). Paul, Sanson-Fisher, Stewart, and Anderson (2010) described the “sorry state” of the Indigenous health evidence base in general and cautioned that before commencing on program/service development or research efforts in an important area such as Indigenous sexual assault, attention needs to be paid to analyzing the existing knowledge output to identify the evidence gaps.
When a mainstream sexual assault service in a regional center with a high Indigenous population was invited to establish a new service in a discrete Indigenous community, staff reflected on the attendance of Indigenous people at the existing service. This, they noted, was relatively low. They subsequently commissioned a research team (the authors of this article) to undertake a systematic search of literature concerning responses to Indigenous Australian sexual assault. The search aimed to scope the number and nature of Indigenous Australian sexual assault publications. To determine proven or promising approaches in the field of Indigenous sexual assault practice, the search focused particularly on what service or program responses to sexual assault had been described or evaluated. The three research questions were as follows:
The findings would inform the design and implementation of a new sexual assault counseling, referral, support, and/or medical services in the nearby Indigenous community, as well as tailoring of the existing regional service to increase accessibility to Indigenous clients.
Method
A written protocol was developed and circulated to the sexual assault service and research team to reach consensus on the purpose and methods for the search, screening, extraction, and analysis of the literature. The protocol described a search strategy incorporating electronic databases and the gray literature. Consistent with methods detailed in the Cochrane Collaboration Handbook on Systematic Reviews of Health Promotion and Public Health Interventions (Jackson, 2007) and with previous systematic searches (Clifford, Doran, & Tsey, 2013; McCalman, Bainbridge, Clifford, & Tsey, 2013; McCalman et al., 2012), the protocol outlined three search steps (Figure 1).

The search strategy.
First, consultation with a qualified librarian identified seven relevant electronic databases to search: Informit, ProQuest, PubMed, Medline via Ovid, Scopus, PsycInfo, Science Direct. The search team was aware of the preference of some Indigenous women and workers to locate sexual assault within the broader concept and language of family violence (Keel, 2004). Discussions about sexual assault have been taboo in some Indigenous communities and the concept of family violence has allowed workers to sensitively broach the subject (Keel, 2004). In this search, however, we chose to limit the scope to the explicit field of sexual assault (or like terms). Two reasons prompted this decision: (a) family violence includes types of violence other than sexual assault and (b) the scope of the study precluded the broader search of the family violence literature. Thus, the following terms were searched in either the title or abstract, article or MESH heading of peer reviewed papers and non-reviewed reports: (Aborigin* or Indigen* or Torres Strait Island* or oceanic ancestry group or australoid*) and (Australia) and (sexual assault or sexual abuse or sexual violence or rape or intimate partner sexual violence). The combined searches of the seven databases (excluding duplicates produced 1,036 references that were imported into Endnote).
Second, to maximize search coverage of the gray literature, the same librarian searched eight websites and clearinghouses related to Indigenous Australian sexual assault. Included were Google Scholar, Australian Centre for the Study of Sexual Assault, Partnerships against Domestic Violence (Australia), National Association of Services Against Sexual Violence, Australian Institute of Criminology, Australian Institute of Family Studies, Australian Indigenous Health InfoNet, and Indigenous Sexual Assault Research and Resources Gateway. 2672 studies not identified in the electronic database search were identified. Third, a researcher (F.B.) hand-searched the reference list of key policy documents identified by the electronic database search for relevant studies not yet identified. The time period for the search was 1993-2012—This 20-year period was considered to provide comprehensive coverage of relevant initiatives.
In total, 3,714 references were identified. Papers were excluded if they (a) were duplicates (n = 474), (b) did not mention responses to sexual assault (or a like term) in the abstract of journal articles or executive summary of reports (n = 1,868), (c) did not mention Indigenous Australians (or like terms) or culturally specific approaches in the abstract or executive summary (n = 1,322), or (d) were published pre-1993 (n = 27). In all, 3,691 papers were excluded, leaving 23 references.
The abstracts or executive summaries of remaining studies (n = 23) were examined to identify studies that were (a) intervention research—which tested the effectiveness of a response to sexual assault or examined the impact of interventions designed to respond to sexual assault or to improve service delivery; (b) program descriptions—which described the methods or processes applied to implement a sexual assault intervention, but in which no data-based evaluation was reported; (c) measurement research—which developed or tested a measure for use in Indigenous populations or concerned with Indigenous sexual assault, for example, the measurement of qualities of a clinical screening or diagnostic tool, and questionnaires assessing variables such as perceptions or attitudes; and (d) descriptive research—defined as epidemiological studies that explored the prevalence or patterns of sexual assault, risk factors, or variables at a community or population level (Sanson-Fisher, Campbell, Perkins, Blunden, & Davis, 2006). The studies were re-classified by another researcher blinded to the results of the initial classification (J.M.), to cross-check classifications performed by the first researcher (F.B.). Agreement was 83% and differenced between analysts were negotiated until consensus was reached.
The data were extracted from studies using a customized on-line data extraction form. The characteristics of intervention and program description studies of sexual assault interventions were categorized by (a) first author and year; (b) publication type; (c) study design; (d) location; (e) intervention issue; (f) main intervention type; (g) intervention components; (h) target age, sample (n); (i) outcomes or effects; (j) study quality (intervention studies only). The data extraction was undertaken by one researcher (F.B.) and categorization of 10% studies validated by a second researcher (J.M.), particularly for any data that required numerical calculations, or was subjective.
Results
Twenty-three studies describing responses to Indigenous Australian sexual assault were identified as meeting the inclusion criteria (Table 1). Six of the publications were peer reviewed while 17 were gray literature. Although there was considerable overlap, the literature documented four main types of response to Indigenous sexual assault: legal justice responses to perpetrators, media responses, community-based responses, and mainstream service responses. The breadth of these response types and associated broad range of stakeholders involved in responding to Indigenous sexual assault suggested that the important task of coordinating service delivery responses to sexual assault was likely to require inter-sectoral partnerships and strategies (Cox, 2008; Cripps & McGlade, 2008; Thomas, 1993; Thorpe, Solomon, & Dimopoulos, 2004; Victorial Indigenous Family Violence Task Force, 2003). Promising responses for combined strategies were tailored to specific communities, and targeted victims/survivors and perpetrators of sexual assault.
The Characteristics of Studies.

Note. FNQ = Far North Queensland; NT = Northern Territory; NSW = New South Wales; QLD = Queensland; VIC = Victoria; FVPLS = Family Violence Prevention and Legal Service; WA = Western Australia; VALS = Victorian Aboriginal Legal Service; WOW = Women Out West.
Intervention research provides vital evidence for practitioners and policy makers about what works in responding to Indigenous sexual assault; however, no intervention studies were found (Table 2). Four studies provided descriptions of programs (Atkinson, Nelson, & Atkinson, 2010; Cripps & McGlade, 2008; Marchetti, 2010; McCallum & Castillon, 1999). One was a measurement study (Willis, 2010). Sixteen studies described problems associated with sexual assault and recommended strategies in response (Aboriginal Child Sexual Assault Taskforce, 2006; Cox, 2008; Cripps & Miller, 2009; Due & Riggs, 2012; Gordon et al., 2002; Government of Western Australia, 2002; Greer, 1997; Langton, 2007; Memmott, 2007; NSW Ombudsman, 2012; Stewart & Jubb, 2005; Thomas, 1993; Thorpe et al., 2004; Victorian Family Violence Prevention and Legal Service, 2010; Wall & Stathopoulos, 2012; Wild & Anderson, 2007). Two publications provided reviews of the Indigenous sexual assault literature (Keel, 2004; Stubbs, 2009). We were not able to assess methodological quality due to the absence of intervention studies.
The Classification of Studies.

Perhaps reflecting the challenges of conducting studies in the sensitive area of sexual assault and the absence of intervention research, 12/23 (52%) of the studies relied on secondary data rather than primary data. Only two of the program descriptions (both relating to offenders) utilized primary data—one from interviews with court practitioners and Elders and observations of intimate partner violence sentencing hearings in the courts, and the other from participatory research within a group-based program for sex offenders (Marchetti, 2010; McCallum & Castillon, 1999). The other two program description studies (both relating to survivors of sexual assault) used secondary data: A critique of literature and a description and author’s experience of a program (Atkinson et al., 2010; Cripps & McGlade, 2008). The measurement study utilized primary data; it described the development of a questionnaire designed to capture perceptions of community safety in Indigenous communities, and the piloting of the questionnaire with service providers (Willis, 2010). Nine of the 16 descriptive studies utilized primary data through consulting with Indigenous community members and/or sexual assault workers and other relevant professionals (Aboriginal Child Sexual Assault Taskforce, 2006; Gordon et al., 2002; Greer, 1997; Memmott, 2007; NSW Ombudsman, 2012; Thorpe et al., 2004; Victorian Family Violence Prevention and Legal Service, 2010; Wall & Stathopoulos, 2012; Wild & Anderson, 2007). The other seven descriptive studies and the two reviews accessed secondary data, some augmenting reviews of literature, the media, and government policies and reports with the authors’ expert opinions.
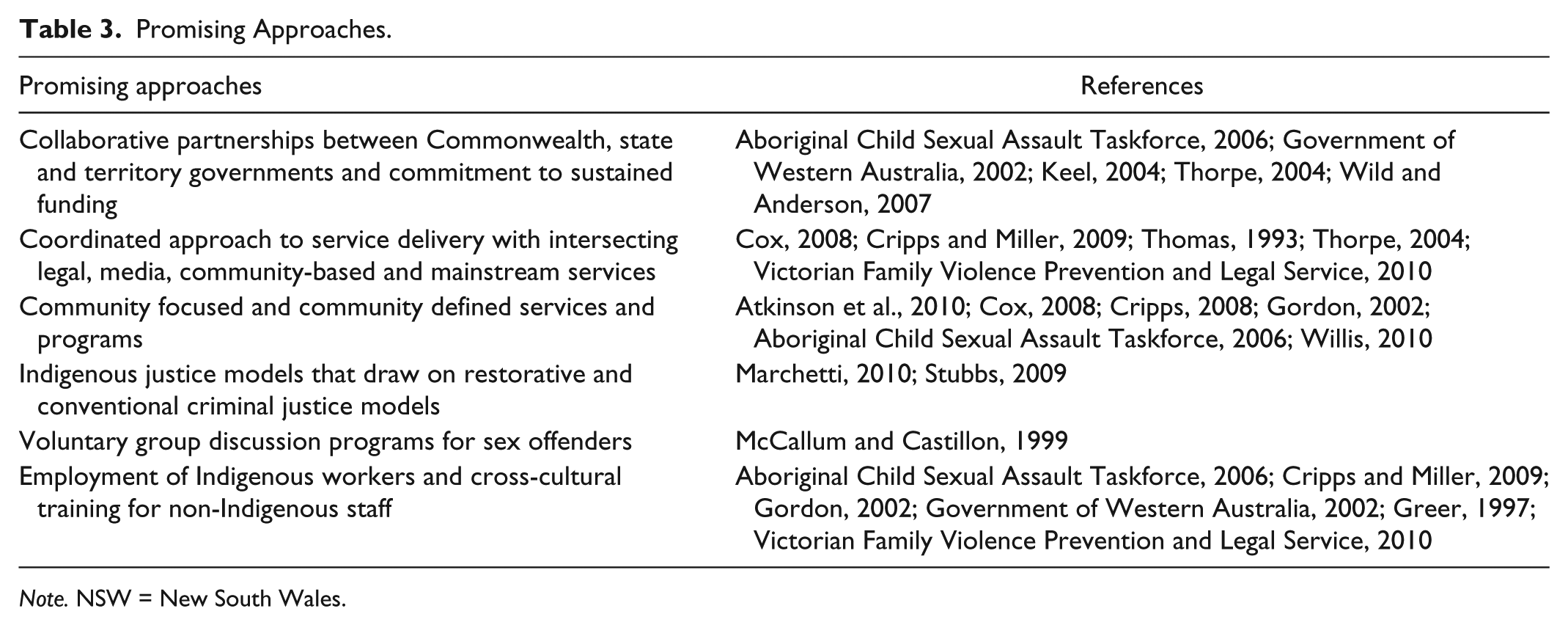
Only two of the studies focused on programs delivered at a local level (Due & Riggs, 2012; McCallum & Castillon, 1999). Most described macro state-wide, cross-state, or national strategic plans and approaches. Yet one of the principles expounded by studies was the need for community development approaches within local communities (Cox, 2008; Gordon et al., 2002; Willis, 2010). Studies suggested six promising responses and/or recommendations (outlined in Table 3). However, without evidence for what works at local levels, there was no guidance on which services can make decisions about particular responses to sexual assault.
Promising Approaches.
Note. NSW = New South Wales.
The findings of the literature search were presented to key stakeholders at a meeting of service providers in the discrete Indigenous community within which the new sexual assault service was being established. Stakeholders included representatives from the mainstream sexual health service, other regional and local health and welfare service providers, advocacy organizations, and community members. Despite the lack of evidence from this review, service providers within the community were keen to pursue long-term strategies to better respond to sexual assault. They agreed to support and promote a weekly visiting service from the mainstream service provider, with a counselor to be available across different services (to protect confidentiality and reduce the potential stigma associated with seeking help for sexual assault-related issues). In addition, community members were encouraged to attend the regional service’s headquarters. Community stakeholders committed to seeking further funding to further develop and evaluate a tailored community-based approach, with university research partners. Funding submissions to date have been unsuccessful.
Limitations
There were methodological limitations within the design of this study. Although the protocol guided the rigorous and thorough search strategy, potential limitations include the possibility that the search did not locate all the relevant studies. For example, our omission of the broader family violence literature may have meant that we missed relevant sexual assault studies that had been framed within the broader family violence concept and terminology. Similarly, our omission of the literature of mainstream sexual assault health responses meant that we are likely to have missed studies of interventions that included Indigenous Australians but did not specifically identify the interventions as Indigenous. Relevant intervention evaluations may have been misclassified; however, the research protocol was adhered to minimize bias and a high level of agreement between blinded coders suggests not. The researchers perceived no potential conflicts of interest inherent in the context of the study.
Discussion
This article identified a complete lack of evidence from the published peer review or gray literatures on what works in responding to Indigenous sexual assault. Furthermore, there was a paucity of program descriptions. We found only two studies that described responses for victims/survivors of sexual abuse (the Indigenous Australian developed We-Ali and Family Well-Being Programs (Atkinson et al., 2010), and an analysis of the feasibility and acceptability of adapting a Canadian Indigenous program (Cripps & McGlade, 2008). Hence, there is currently insufficient evidence from peer review or gray literature studies of sexual assault responses targeting Indigenous Australians to confidently direct practice or policies regarding what strategies are likely to be effective in responding to sexual assault.
What the review did confirm was that a starting point for any new service is to engage with local community members. Taking this principle on board, the regional service that commissioned this literature search interviewed 47 members from a discrete Aboriginal community, asking four simple questions about their knowledge of the community’s current response to sexual assault, knowledge of past strategies, perceptions of barriers to people coming forward about sexual assault, and suggestions for future strategies. Like Bligh’s (1983) study 30 years earlier, the consultation found that community members knew about the availability of generic health, Police, and school services, but highlighted that in general, sexual assault was not being adequately responded to. Instead, the victims of sexual assault responded personally with shame, fear of family retaliation, family and community pressure, and unwanted attention. Perceptions of barriers for people coming forward about sexual assault included personal barriers of shame, fear, denial, and lack of knowledge of what process might ensue once sexual assault was disclosed. Family barriers included family members not being willing to listen or believe, blaming, denial to protect other family members and bullying, retaliation, and family fights. As well, community members noted service barriers such as a historical distrust of government organizations and fear of breaches of confidentiality particularly given that workers were often family members and many lacked the requisite understanding or training in issues of confidentiality. As well, community members perceived a decline in the availability of women’s resource center services over time. Community barriers included what members perceived as a culture of male dominance, with women and children being ignored or silenced, and a cycle of violence. Community members identified seven strategies for responding to sexual assault. These were: sustained awareness-raising and service promotion through local resource development branded with a language name for sexual assault and providing contact details for who to call and where to report; education at community events and in schools; training for health practitioners to respond culturally and appropriately including for assessments; safe houses with dedicated workers who could respond over a 24-hr period and a 1800 free-call number; prevention rather than just intervention; a youth drop in service; and increased parent involvement.
The urgent need to reduce the disproportionately high rates of sexual assault experienced by Indigenous Australians and to improve responses to sexual assault has been widely acknowledged. For this to occur, there is an urgent need to develop evidence-based programs and evaluate extant programs and policies. Collaboration and partnerships between service providers, community groups, funding bodies, and researchers are critical for systematically building the evidence as to what works and under what conditions. However, most of the descriptive literature described macro state-wide, cross-state, or national strategic plans and approaches rather than locally based initiatives. Without evidence for what works at local levels, there was no guidance on which services, such as the regional service that commissioned this search, could make decisions about situated responses to Indigenous sexual assault.
Systematic literature searches such as this are important for determining the state of evidence about the issue of concern, but cannot determine why there has been so little evaluation research in Indigenous sexual assault. Possibly, Indigenous communities have struggled with how to respond to family violence and the sensitivities associated with sexual assault have not garnered the same attention. Sexual assault service providers may have been concerned about the under-utilization of their services by Indigenous people but lacked the resources to respond, or to document their responses. Similar to our experience, community stakeholders may have been frustrated in their attempts to obtain funding for collaborative research with university research partners. The reflections of the project worker from the regional sexual assault service are telling. On completion of the project, she said, Opportunities for the follow on from this project are endless! My feelings with my role in this project are that I could easily have been involved with [community name] for another year, if not longer . . . It takes time for one individual to spend time looking at sexual assault and what this means to them, let alone a whole community . . .
In this case, the trust developed through engagement with community members in this project, provided solid grounding for informing the establishment of a part-time sexual assault counseling service at the local community-controlled health service. Nevertheless, the complexities and sensitivities of responding appropriately to Indigenous sexual assault clearly outweigh this level of minimal resourcing.
This review makes it apparent that despite public outcry, the evaluation of public health and other responses to Indigenous sexual assault is heavily under-resourced and requires investment. There is a need for a long-term commitment to consistent community responses to sexual assault and rigorous evaluation methods. While evaluations of sexual assault interventions using non-experimental designs may be easier and cheaper to implement, they are unlikely to provide strong evidence applicable to other Indigenous communities. Instead, methodologically rigorous mixed method studies such as multiple baseline designs can be applied to test the effectiveness of those promising interventions identified in the literature across geographically and culturally diverse Indigenous population groups. Such evaluation will provide evidence to inform the implementation of future interventions with a greater likelihood of more effectively responding to Indigenous sexual assault.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The author received financial support from the regional sexual assault service for the literature search, but the authorship of this article was not funded.