
Abstract
This study’s main objective was to determine the factors that led to Turkish women being physically abused by their husbands or partners during pregnancy. The National Research on Domestic Violence against Women in Turkey conducted in 2014 was utilized in our study. We analyzed the survey data using the binary logistic regression method. A pregnant woman who graduated from high school was less likely to encounter physical abuse than an illiterate woman. Those who made more money for the family than their husband or partner were more likely to experience physical abuse. Pregnant women with alcoholic husbands/partners were more likely to experience physical abuse. By supporting the prevention of other potential outcomes for maternal and infant health, implementing screening for partner violence and childbirth phobia in obstetrics and gynecology clinics, and offering comprehensive information about pregnancy labour, we can enhance family and social health.
Plain Language Summary
Intimate partner violence (IPV) against pregnant women has been the subject of research in the scientific world for a long time and has been investigated in various aspects. Understanding the impact of IPV against a pregnant woman can have significant consequences for reproductive health with early diagnosis. It may also help develop future intervention programs. Pregnancy provides an opportunity to screen for domestic violence since pregnant women make routine visits during this period. Physical IPV during pregnancy can directly or indirectly affect pregnancy when there is a blow to the abdomen, have an impact on mental health and behavioral changes, and cause adverse pregnancy outcomes such as fetal death, premature birth, abdominal pain, and hospitalization. In this study, the answers to the questions “What is the exposure of women to physical IPV during pregnancy? Is there a relationship between women’s sociodemographic and economic characteristics and their exposure to physical IPV during pregnancy? Is there a relationship between husband’s/partner’s characteristics and women’s exposure to physical IPV during pregnancy?” have been sought. The findings of this study are significant in terms of providing information for the development of policies and programs aimed at preventing violence against women. In the event that the pregnant woman is exposed to violence, it is crucial for society to take action to protect both the mother and the unborn child’s health. In order to prevent the emergence of violence and develop effective solutions toward this goal, the viewpoint of primary care health workers in our country must be thoroughly evaluated. In addition, health personnel should receive the necessary training, support, and encouragement in these matters.
Keywords
Introduction
One of the most significant human rights problems in the world is violence against women (Babaheidarian et al., 2021). It is also one of the major causes of death worldwide, spreading and affecting an increasing number of couples despite advancements in the humanities (Ozgoli et al., 2016; Razaghi et al., 2013). The social issue of violence against women is exceedingly complex and difficult (Alkan & Ünver, 2020). Violence against women, as defined by the United Nations (UN), is “any type of gender-based violence that results in, or is likely to result in, physical, sexual or mental harm to women, threats of such actions, coercion, or arbitrary deprivation of liberty in public or private life.” (King, 2019).
In the modern world, gender-based violence is one of the most pressing human rights issues. “Intimate partner violence” (IPV) against women is the most prevalent type of gender-based violence (Başkan & Alkan, 2023). According to studies on violence against women, the majority of perpetrators are intimate partners (IP), and IPV during pregnancy (IPV) is one of the most common types of IPV (Yüksel-Kaptanoğlu & Adalı, 2021). A woman’s husband or companion, with whom she engages in sexual activity, or the father of the child she is carrying in her womb, is considered to be her close partner (Lencha et al., 2019). IPV entails physical, emotional and sexual abuse, stalking or psychological harm by a current or former partner (Alkan et al., 2023; WHO, 2018). Slapping, pushing, hitting, kicking, strangling, threatening, or using anything that may physically harm the other person is considered physical abuse (Hoang et al., 2016). According to a study conducted by the World Health Organization (WHO), one out of every three women has already been subjected to physical or sexual abuse, with close partners responsible for 38% of femicide. Women of various ages, races, and educational levels are affected by violence, which is a prevalent problem experienced in the media and society (Steiner et al., 2022).
The condition can be exceedingly problematic in pregnant women, affecting pregnancy, labor, and the initial bond between mother and child. Pregnancy can also evoke sensitivity in women who have been subjected to violence due to it being a period of significant physical, emotional, social, and economic upheaval (Van Parys et al., 2014). Since the repercussions of violence during pregnancy can be significant, immediate, and long-lasting for both the mother and the child, the topic of violence during pregnancy is becoming more and more important as a clinical and public health problem (Chhabra, 2007). Pregnant women who have experienced physical abuse may be more likely to miscarry and have babies that are underweight at birth (Chhabra, 2007; Costa et al., 2017). Physical IPV during pregnancy can directly or indirectly affect pregnancy when there is a blow to the abdomen, have an impact on mental health and behavioral changes, and cause adverse pregnancy outcomes such as fetal death, premature birth, abdominal pain and hospitalization (Abdollahi et al., 2015).
One of Türkiye’s most pressing social challenges is violence against women, which continues to be a global issue (Alkan et al., 2021). Men and women have diverse roles and realms of influence in Turkish society, and Turkish society has a historically patriarchal structure (Gölge et al., 2016). IPV is frequently employed to establish and reinforce a man’s authority in the home or romantic relationship (Adjah & Agbemafle, 2016). The prevalence of violence in Türkiye reveals that it is a social problem fed by patriarchal cultural acceptability, gender disparity, and socioeconomic status (Büyükyilmaz & Demir, 2016). Women’s rights and violence against women are now explicitly addressed in Turkish law. Despite this, most Turkish women are unaware of their rights, which may be due to societal and cultural norms (Alkan & Tekmanlı, 2021). Furthermore, it is widely accepted that disobeying a husband is wrong since Turks uphold Islamic principles that demand women to obey men (Kocacik & Dogan, 2006). Due to customs and religious beliefs, violence, sexuality, and other comparable domestic difficulties are not believed to warrant interference in Türkiye (Alkan & Tekmanlı, 2021).
Literature Review
IPV occurs in all countries, regardless of social and economic equality, human rights and health status, and religious and cultural contexts (WHO, 2018). Physical partner violence can occur at any time in a woman’s life, including pregnancy (Orpin et al., 2020). Partner violence during pregnancy may increase due to the presence of gender inequality, lack of social support, cultural structure, physiological effects of pregnancy, and psychological vulnerabilities (Dikmen & Tetikçok, 2023).
The physical abuse against pregnant women has not been adequately examined in Türkiye despite its potential importance. Empirical research on the correlations and consequences of physical abuse towards pregnant women has been limited in Türkiye to date (Arslantaş et al., 2012; Bolu et al., 2014; Giray et al., 2005; Güler, 2010; Karaoglu et al., 2006; Yanikkerem et al., 2006; Yüksel-Kaptanoğlu & Adalı, 2021). IPV is a socio-medical issue that has risen to prominence in recent years (Farquhar et al., 2011). Pregnant women are at higher risk of experiencing IPV (Alhusen et al., 2015). In the literature, there are differing views on whether the prevalence of IPV during pregnancy lowers, remains approximately the same, or increases (Bailey, 2010). According to a study conducted in Italy, 15% of violence cases began during pregnancy, 16.6% escalated throughout pregnancy, and 50.6% remained unchanged during pregnancy (Mauri et al., 2015).
Studies show that the prevalence of physical abuse against pregnant women differs by country (Abdollahi et al., 2015). The lack of a clear definition of violence, variances in study methods, observed parameters, cultural obstacles, and women’s reluctance to talk about physical abuse are all reasons for this disparity, making it difficult to make certain conclusions (Bailey, 2010; Faramarzi et al., 2005; Nasir & Hyder, 2003). In a Portuguese investigation, it was found that 21.9% of pregnant women had experienced physical abuse nationally (Coutinho et al., 2015). In Egypt, China, Nigeria and Brazil, the rates of physical abuse exposure of pregnant women were found to be 30.2% (Elkhateeb et al., 2021), 0.98% (Zheng et al., 2020), 58.6% (Iliyasu et al., 2013), and 6.5% (Audi et al., 2012), respectively. In another study conducted in Sweden, it was found that the prevalence of domestic violence was 1%, and that 0.4% of women were physically abused during pregnancy (Finnbogadóttir et al., 2014). According to a study done in Ethiopia, physical abuse was experienced at a rate of 20.3% among pregnant women who reported any type of IPV (i.e., sexual, economic, or psychological abuse). Another study in Brazil found that the prevalence of physical abuse against pregnant women was 12.4%, and that 66% of these women were physically abused at once (Costa et al., 2017). A study in Tabriz found that more than a third (35.2%) of pregnant women were exposed to close partner violence, and 4.8% of women experience physical abuse (Naghizadeh et al., 2021).
Physical abuse towards pregnant women occurs due to a variety of factors. The level of education is a significant factor impacting women’s exposure to physical abuse (Alkan et al., 2022). It has been discovered that pregnant women with low levels of education are more likely to experience physical abuse (Abdollahi et al., 2015; Arslantaş et al., 2012; Azene et al., 2019; Santos et al., 2017). Education is generally seen as the most important indicator of a person’s socioeconomic level (Alkan & Ünver, 2022). Higher education levels are associated with higher income levels in both public and private institutions, and educated people are also more aware of a variety of other issues, including their health (Ünver, Tekmanli, et al., 2023). As women’s education level decreases, their vulnerability to violence increases (Sen & Bolsoy, 2017). One in two women with lower levels of education is subjected to violence, compared to one in five women with higher levels of education (Flake, 2005). A poor education level undoubtedly increases the chance of being subjected to violence since education level is one of the most significant determinants of the sociocultural position of women in the family. Poorly-educated women may not have a say in decision-making and may have to marry less educated, often low-income men. All of these elements may result in partner miscommunication and susceptibility to domestic violence (Arslantaş et al., 2012). Educated women also appear to be better equipped to recognize abusive relationships and end them (Flake, 2005). In general, women’s financial standing, employability, and personal abilities all have been shown to improve as their education level rises. As a result, it lessens the dangers of being exposed to violence (Boyle et al., 2009; Lee et al., 2015).
The age of pregnant women and their experience of physical abuse are significantly correlated (Ansari et al., 2017; Azene et al., 2019). IPV in pregnant women is also related to the age of the partner (Lencha et al., 2019; Mahenge et al., 2013). According to a study conducted in Ethiopia, male close partners aged 30 and older are twice as likely than other age groups to inflict violence on their pregnant partners (Lencha et al., 2019). In several studies, there was no significant relationship between pregnant women’s age and their exposure to physical abuse (Giray et al., 2005; Yanikkerem et al., 2006; Yüksel-Kaptanoğlu & Adalı, 2021).
Exposure to physical abuse during pregnancy has been linked to lower income (Abdollahi et al., 2015; Bailey, 2010). In a study conducted in the United States, low income and a lack of education were discovered to be the most important predictors of physical abuse throughout pregnancy (Bohn et al., 2004). One of the factors associated with IPV in pregnant women is the habit of substance use (Lencha et al., 2019; Yüksel-Kaptanoğlu & Adalı, 2021). Studies have found that pregnant women whose partners consume alcohol are more likely to be victims of IPV (Gebrezgi et al., 2017; Makayoto et al., 2013). Pregnant women who have alcoholic and cigarette-smoking partners are more likely to experience physical abuse (Alan et al., 2016; Deveci et al., 2007; Karaoglu et al., 2006). It has been noted in various studies that it is important to recognize that alcohol consumption alone cannot account for the occurrence of violent incidents. According to these studies, alcohol consumption appears to be a situational factor that exacerbates couples’ conflicts, rather than the primary factor that leads to violence (de Campos Moreira et al., 2011; Fenton & Rathus, 2010). In another study, it was determined that women whose husbands/partners are occasionally intoxicated are at a higher risk of physical abuse than women whose husbands/partners are frequently intoxicated (Castro et al., 2017).
Physical IPV during pregnancy has been linked to negative health consequences including insufficient prenatal care and weight gain (Khodakarami et al., 2009; Moraes et al., 2006). Additionally, physical IPV during pregnancy has been shown to have significant negative impacts on reproductive health (Abdollahi et al., 2015). Research has also been conducted regarding the link between abortion and violence (Fanslow et al., 2008; Silverman et al., 2010). However, no substantial link between violence and abortion was found in a study conducted in Iran (Abdollahi et al., 2015). According to a study conducted in Tanzania, women who were exposed to violence during pregnancy were 1.9 times more likely to report an induced abortion (Stöckl et al., 2012). IPV is attributed to many causes such as the lack of women’s involvement in decision making in terms of family planning and the previous sex order of the children. These factors lead to various consequences to women’s reproductive health such as sexual disorders, gynecological disarrays, antenatal disruptions, vaginal blood loss, pelvic pains and urinary tract infections (Ehsan et al., 2021). The devastating impact of violence-related mental health problems during pregnancy on adverse birth outcomes was investigated. Depression is the most common mental health consequence of IPV (Flach et al., 2011). In addition, most women who have been exposed to IPV have reported experiencing post-traumatic stress disorder, which is associated with both preterm birth and low birth weight (Cohen et al., 2000; Rosen et al., 2007). It has been found in various studies that physical abuse during pregnancy is usually directed at the abdomen of the woman, resulting in premature birth and even fetal loss (Audi et al., 2012; Khodakarami et al., 2009).
The physical abuse suffered by pregnant women in Türkiye also varies according to region. It was determined that 8.1% of pregnant participants in a study conducted in Malatya (Karaoglu et al., 2006), 18.2% of participants in a study conducted in Kars (Arslantaş et al., 2012), 9.7% of participants in a study conducted in the Aegean region of Türkiye (Yanikkerem et al., 2006), and 10.3% of women in a study conducted in Şanlıurfa were exposed to physical abuse (Bağcıoğlu et al., 2014). It was also found that 20% of pregnant women in a study conducted in İzmir (Giray et al., 2005), 18.1% of pregnant women in a study conducted in Sivas (Güler, 2010), 4.8% of pregnant women in another study conducted in Elazığ were exposed to physical abuse (Deveci et al., 2007). In a study conducted in Düzce University Medical Faculty Research Hospital on pregnant women, 26.5% of the participants (Bolu et al., 2014) and in a study conducted in 30 family health centers in Konya, 11.5% of the participants were found to be exposed to physical abuse (Alan et al., 2016). Men who inflict violence towards their wives while they are pregnant are more likely to inflict violence towards their children (Ayrancı et al., 2002; Bolu et al., 2014). The prevalence of IPV among women in Malatya and Sivas can be attributed to their geographical location in Central Anatolia. The high incidence of IPV in the Kars and Elazığ regions can be ascribed to their geographical location in Eastern Anatolia. On the other hand, while the prevalence rate of IPV in İzmir is 20%, it is 9.7% in the Aegean region. According to a study conducted in Türkiye, a woman’s domicile is one of the factors that influence IPV, and she is more likely to experience violence there than in any other location. The study in question found that women in urban regions were more likely than those in rural regions to experience violence. Therefore, the region in which the women lived also had an impact on the violence. According to the study, women in the western, central, and southern regions are more likely than those in the eastern region to experience violence (Alkan et al., 2021). Earth’s economic and social progress varies over time and space (Tvrdoň & Skokan, 2011). This difference causes favored areas to advance forward while others fall behind. Therefore, spatial inequality paves the way for the occurrence of this problem. Both countries and areas within them may suffer from this issue. Since regional development inequality now affects all nations, developed and developing alike, countries must exert tremendous effort to find a solution (Ünver, Aydemir, et al., 2023).
IPV against pregnant women has been the subject of research in the scientific world for a long time and has been investigated in various aspects. Understanding the impact of IPV against a pregnant woman can have significant consequences for reproductive health with early diagnosis. It may also help develop future intervention programs (Abdollahi et al., 2015). Pregnancy provides an opportunity to screen for domestic violence since pregnant women make routine visits during this period. Physical IPV during pregnancy can directly or indirectly affect pregnancy when there is a blow to the abdomen, have an impact on mental health and behavioral changes, and cause adverse pregnancy outcomes such as fetal death, premature birth, abdominal pain, and hospitalization. However, some studies have not confirmed these associations. A limited number of studies in the literature have identified women’s exposure to physical violence by their husbands/partners during pregnancy as a dependent variable, which is vital for understanding the determinants of this type of IPV. Statistical methods or cross-sectional data sets on physical violence against pregnant women in Türkiye are relatively inadequate. There is also a significant gap in the literature regarding studies focusing on the Turkish example. This study examines physical violence against pregnant women using cross-sectional data sets, demographic variables, and more specific variables (e.g., husband’s/partner’s mother’s exposure to physical violence by her husband, woman’s exposure to violence, husband’s/partner’s physical violence from his own family, wife’s/partner’s social violence). It aimed to fill this gap in the literature by using media (interfering with media use and interfering with spouse/partner’s clothes). For this purpose, the factors affecting physical violence against pregnant women were modeled for Türkiye using a large data set.
Studies show that there are some difficulties in addressing and revealing IPV during pregnancy. Gender equality and women’s empowerment are vital to overcoming these obstacles. Identifying the factors affecting physical violence against pregnant women is vital for developing policies that improve the functioning of the legal system and increase cultural awareness in order to promote social change. Evaluating the factors affecting physical violence against pregnant women in terms of demographic variables and the specific variables in question in our current study may assist government officials, policymakers, program designers, and non-profit organizations in designing prevention and control strategies. Additionally, holistic and integrated guidelines need to be developed to improve the quality of emergency and preventive interventions. We hope that our study, which also examines the risk factors that increase violence during pregnancy, will make a significant contribution to the scientific literature.
In this study, the answers to the questions “What is the exposure of women to physical IPV during pregnancy? Is there a relationship between women’s sociodemographic and economic characteristics and their exposure to physical IPV during pregnancy? Is there a relationship between husband’s/partner’s characteristics and women’s exposure to physical IPV during pregnancy?” have been sought. Additionally, by analyzing IPV during pregnancy using nationally representative IPV research in Türkiye, this study aimed to contribute to the literature.
Material and Method
The details of the data used in the study, the dependent and independent variables, and the statistical analysis are all explained in this section.
Data
We used the micro data set obtained from “the National Research on Domestic Violence against Women in Türkiye,” which was conducted by the Institute of Population Studies at Hacettepe University in 2014. The National Research on Domestic Violence against Women in Türkiye was conducted in 2008 and 2014. No current studies were conducted after 2014.
Türkiye was divided into 30 strata for the violence study, with estimates given at the national, urban/rural, 12 regionals, and 5 regional levels. Urban areas are defined as towns with a population of 10,000 or more, whilst rural areas are defined as areas with a population of less than 10,000. Cluster sampling was used to select the study’s sample (DGSW, 2014).
The study’s field application began on April 8, 2014, and ended on July 11, 2014. The surveys were administered by the study team in the National Research on Domestic Violence against Women in Türkiye. At every stage of the study, ethical guidelines established by WHO were followed, and several precautions were taken to protect the safety of both the women being interviewed and the research team (DGSW, 2014).
Seven thousand four hundred sixty-two women between the ages of 15 and 59 who lived in 11,247 sample households were interviewed for the National Research on Domestic Violence against Women in Türkiye, with a refusal rate of 4.4%. Women’s interviews had a response rate of 83.3%. These files now include women’s weight estimates in accordance with the study’s sample design (DGSW, 2014).
In the National Research on Domestic Violence against Women in Türkiye, questionnaires were administered in the form of household question papers (including questions about the number of people living in the household, the number of rooms, and welfare level indicators) and women’s question papers (including questions about the sociodemographic and other traits of the woman and her husband/partner). Data on households and women from two distinct Excel files have been combined into one file. The data of 7,070 women were analyzed after 392 women, whose household information was missing as a result of the merge, were extracted.
Since our analysis focused on the physical abuse experienced during pregnancy by women who had been pregnant at least once as of the survey period, we excluded the data of 1,340 women who had never been in a relationship and who had never been pregnant as of the survey period. As a result, we used the data of 5,730 women who had been pregnant at least once as of the survey period.
Measures and Variables
In the National Research on Domestic Violence against Women in Türkiye, pregnant women were asked two questions regarding their exposure to physical abuse during pregnancy. These questions were: “During your pregnancies, did your partner ever hit you, slap you, beat you, or otherwise physically harm you?” as well as “Did your partner [any of your husbands/partners] punch or kick your stomach during your pregnancies?”. Pregnant women in the study were considered to have been subjected to physical abuse by their husbands/partners if they experienced at least one of the above-mentioned statuses, and they were not exposed to physical abuse if they did not experience either of them. As a result, the study’s dependent variable was whether or not women experiencing pregnancy were subjected to physical abuse, with the value of 1 indicating that they were exposed to physical abuse and 0 indicating that they were not.
An examination of the literature aided in identifying the independent factors in the study. Women’s sociodemographic and economic characteristics, as well as factors related to their husbands/partners are as follows; region (12 regions), education level (illiteracy, primary school, secondary school, high school, university), higher income contribution of women to the household (yes, no), health status (excellent/good, manageable, bad/very poor), having children (aged between 6 and 14) (yes, no), the husband/partner fights with another man in a way that involves physical abuse (yes, no), the woman’s mother’s exposure to physical abuse by her husband (yes, no), the husband/partner’s mother’s exposure to physical abuse by her husband (yes, no), the woman’s exposure to physical abuse by her husband/partner’s own family (yes, no), the husband/partner interferes with the use of social media (yes, no) and her clothes were found to be related to physical abuse during pregnancy (yes, no). In order to observe the impact of the categories of all the variables to be included in binary logistic regression models, ordinal and nominal variables were defined as dummy variables (Alkan & Ünver, 2021).
Statistical Analysis
Survey statistics in Stata 15 (Stata Corporation) were used to account for the results due to the complex sampling design and weights. There was a weighted analysis (Güney et al., 2023). Firstly, the frequency and percentages of pregnant women who took part in the study were determined based on their exposure to physical abuse by their husbands/partners during pregnancy. Secondly, the relationship between physical abuse and independent factors was investigated using the chi-square independence test. Then, using binary logistic regression analysis, the risk factors that affect pregnant women’s exposure to physical abuse were determined. When the outcome (dependent variable) contains two options (binary or dichotomous), this analysis is used to examine the relationship between the dependent variable and the independent variable(s). Binary logistic regression offers the chance to compute the odds ratio in addition to the chance to assess the statistical significance of each independent variable as a risk factor. In the binary logit model, the cumulative logistic distribution function is utilized (Alkan & Ünver, 2020).
Results
Descriptive Statistics
The information in Table 1 reveals the elements that may help reduce the physical abuse of pregnant women in Türkiye. 8.39% of the women in this study experienced physical abuse from their husbands or boyfriends when they were pregnant.
Findings on the Factors Affecting Physical Abuse Against Women During Pregnancy.
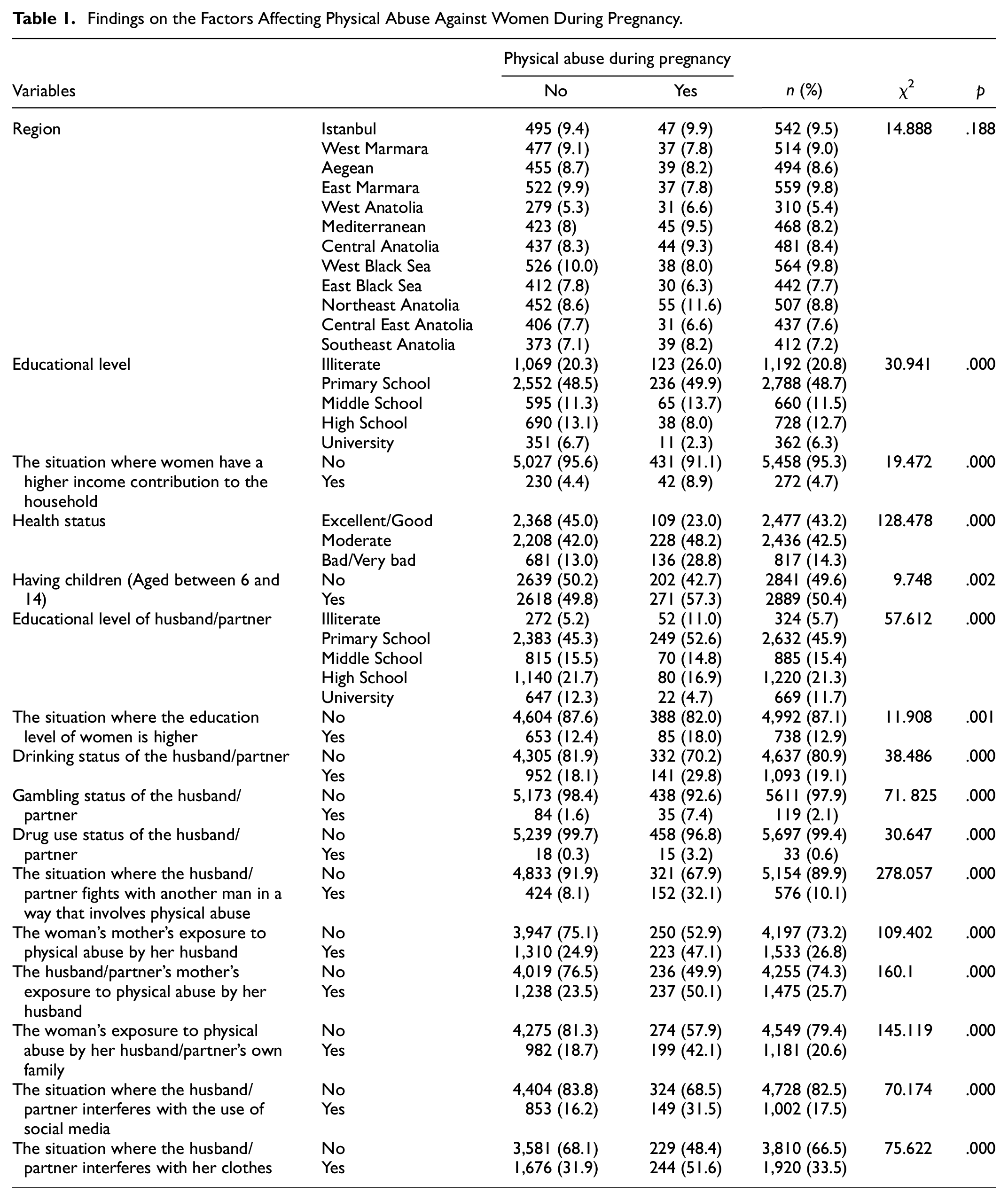
The results of the chi-square independence test are shown in Table 1, and it was demonstrated that there is a substantial correlation between physical abuse against pregnant women and sociodemographic (with the exception of the region) and economic factors.
Model Estimation
The estimated results of the binary logistic regression model are displayed in Table 2. In the study, it was tested whether a multicollinearity existed between the independent variables to be included in the binary logistic regression model. VIF values of 5 and higher are thought to cause moderate multicollinearity, whereas VIF values of 10 or more are thought to generate significant multicollinearity (Coskun et al., 2023). In this study, there isn’t a variable that contributes to the problem of multicollinearity among the variables.
Estimated Binary Logit Model Results Regarding the Factors Affecting Women’s Exposure to Physical Abuse During Pregnancy.

Note. CI = confidence interval.
p < .01; **p < .05; ***p < .10.
The odds of experiencing physical abuse were 2.31 times greater for women in Central Anatolia compared to Central East Anatolia, according to the binary logistic regression model shown in Table 2. When compared to other women, those who contributed more to the household’s income than their husbands or partners were 1.81 more likely to experience physical violence. The study predicts that women with poor/very poor health would have 3.25 times greater odds of experiencing physical abuse than women in the reference group (perfect/good health). The odds of experiencing physical abuse increased by 1.27 times for pregnant women with kids between the ages of 6 and 14 compared to non-pregnant women.
A pregnant woman whose husband or partner was illiterate had 1.54 times higher odds of exposure to physical abuse compared to a woman whose husband/partner was a primary school graduate. A pregnant woman whose husband or partner used alcohol had 1.32 times higher odds of exposure to physical abuse than others. A pregnant woman whose husband or partner was gambling had 1.78 times higher odds of exposure to physical abuse than others. A pregnant woman whose husband or partner used drug had 3.83 times higher odds of exposure to physical abuse than others.
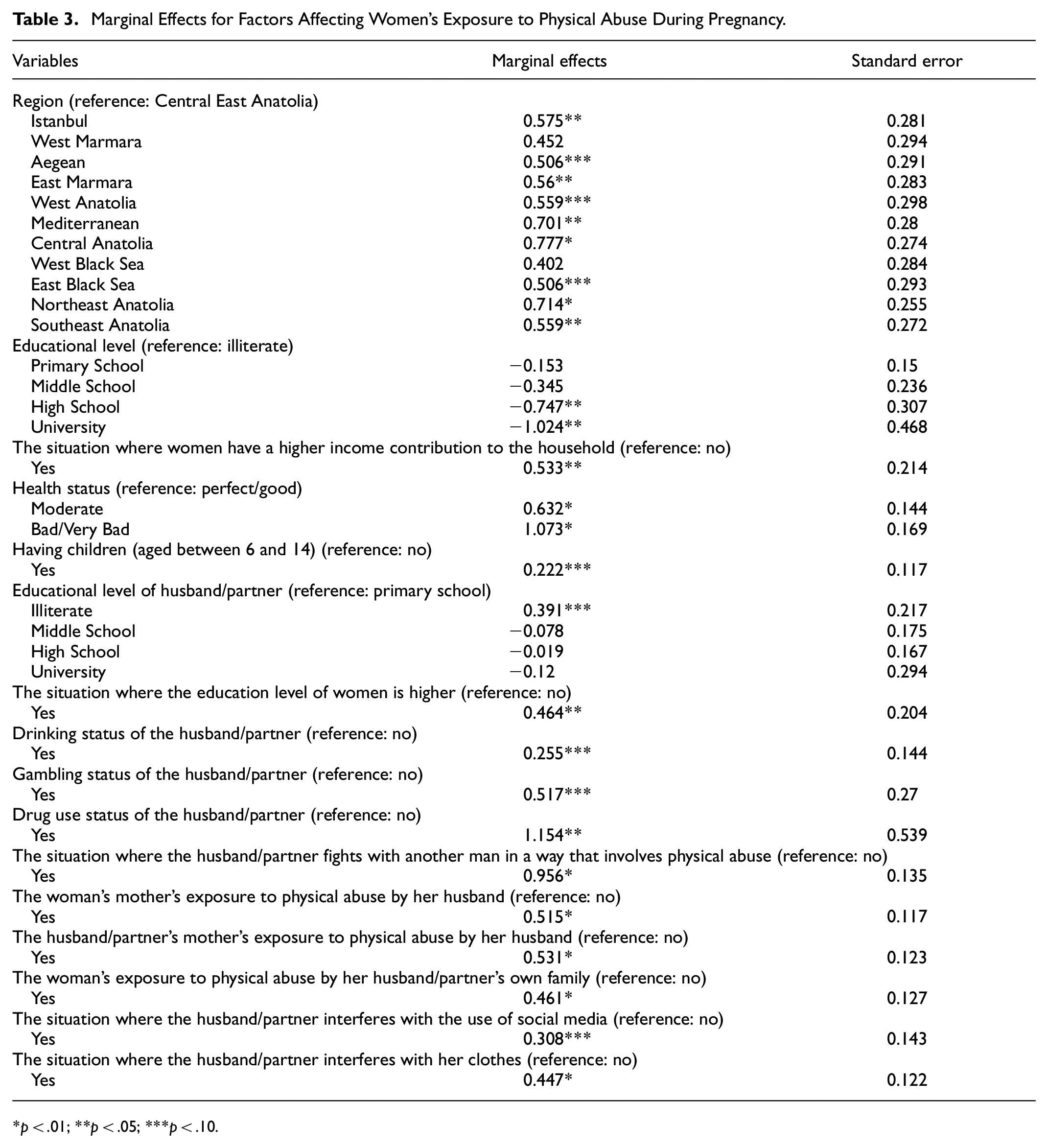
Table 3 lists the marginal impacts of the variables influencing pregnant women’s exposure to physical abuse.
Marginal Effects for Factors Affecting Women’s Exposure to Physical Abuse During Pregnancy.
p < .01; **p < .05; ***p < .10.
According to the binary logistic regression models in Table 3, a woman living in the Mediterranean region is 70.1% more likely to encounter physical abuse compared to a woman living in the Central East Anatolia region. Similarly, a woman living in the Central Anatolia region is 77.7% more likely to encounter physical abuse compared to a woman living in the Central East Anatolia region. A woman living in Northeast Anatolia and Southeast Anatolia is 71.4% and 55.9% more likely to encounter physical abuse compared to a woman living in the Central East Anatolia region, respectively.
A woman with a high school diploma is 74.7% less likely to encounter physical abuse than an illiterate woman. Furthermore, a woman with an undergraduate degree is 102.4% less likely to encounter physical abuse than an illiterate woman. A woman with a higher income contribution to the household from her husband/partner is 53.3% more likely to encounter physical abuse compared to others. A woman with moderate health is 63.2% more likely to encounter physical abuse compared to a woman with excellent/good health. Similarly, a woman with poor/very poor health is 107.3% more likely to encounter physical abuse from her husband/partner compared to a woman with excellent/good health conditions. A woman whose child is between 6 and 14 is 22.2% more likely to encounter physical abuse compared to other women.
A woman with an illiterate husband/partner is 39.1% more likely to encounter physical abuse than a woman with a primary school graduate husband/partner. Physical abuse is 46.4% more likely to occur when a woman has a higher education level than her husband/partner. A woman who drinks with her partner is 25.5% more likely to encounter physical abuse than other women. A woman who has a gambling husband/partner is 51.7% more likely to encounter physical abuse than other women. A woman who has a drug-using husband/partner is 115.4% more likely to encounter physical abuse than other women. A woman who has a quarrelsome husband/partner is 95.6% more likely to encounter physical abuse than other women. Table 3 shows that a woman whose husband/partner interferes with her social media usage and clothing is 30.8% and 44.7% more likely to experience physical abuse than other women, respectively.
Discussion
It is also essential from a social perspective that if a pregnant woman is exposed to violence by her physically intimate partner, the health of both the pregnant woman and her unborn baby will be affected. In this study, binary logistic regression analysis was used to examine the variables influencing physical abuse against pregnant women in Türkiye. The variables of region, education level, health status, having children (6–14 years old), education level of the husband/partner, drinking status of the husband/partner, gambling status of the husband/partner, drug use status of the husband/partner, the situation in which the husband/partner fights with another man in a way that involves physical abuse, the woman’s mother’s exposure to physical abuse by her husband, the husband/partner’s mother’s exposure to physical abuse by her husband, the woman’s exposure to physical abuse by her husband/partner’s own family, the interference of the husband/partner with the usage of social media and her clothes were found to be statistically significant.
The study discovered that pregnant women’s educational status was associated with their exposure to physical abuse. According to the findings, the likelihood of experiencing physical abuse reduces as one’s degree of education rises. According to a study conducted in Campinas (São Paulo), pregnant women with low education are more vulnerable to physical and sexual abuse (Audi et al., 2008). In a study conducted in Türkiye, it was stated that illiteracy or low education level, unemployment, poverty, unwanted pregnancies, unhealthy behaviors like smoking, urban lifestyle and violence during pregnancy were all identified as part of a vicious circle (Karaoglu et al., 2006). Other studies conducted in Türkiye concluded that as the level of education increases, the probability of experiencing physical abuse decreases (Altınay & Arat, 2009; Arslantaş et al., 2012; Kocacik & Dogan, 2006; Mayda & Akkuş, 2005; Yanikkerem et al., 2006). Studies have shown that women with higher degrees of education feel more secure and confident than women with lower levels of education. Furthermore, educated women are more likely to be economically self-sufficient because they have formal jobs or the ability to engage in income-generating activities (Vyas et al., 2015). According to a study, Malawian women with higher levels of education had higher access to resources and were therefore less tolerant of an abusive relationship (Bazargan-Hejazi et al., 2013).
In the study, the level of education of the husband/partner was found to be linked to physical abuse against pregnant women. According to the findings, the likelihood of experiencing physical abuse reduces as the education level of women’s husbands/partners rises. In a study conducted in Ghana, it is stated that the high education level of husbands/partners has a protective effect against violence (Adjah & Agbemafle, 2016). The education level of the partner was found to be effective in preventing physical abuse against pregnant women in a study conducted in Konya (Karaoglu et al., 2006). There are studies with similar findings (Akar et al., 2010; Bağcıoğlu et al., 2014; Tokuç et al., 2010). The health status of pregnant women is one of the factors linked to their exposure to physical abuse. It was concluded that as women’s health improves, the likelihood of being subjected to physical abuse reduces. Furthermore, the study found that there is a correlation between the region in which pregnant women live and their exposure to physical abuse.
In the study, it was determined that pregnant women whose spouses drink alcohol are exposed to more physical abuse. The frequency of consuming two or more drinks per week by the spouse increases the possibility of psychological, physical and sexual abuse against pregnant women (Santos et al., 2017). As intoxication frequency increases, the aggression levels of individuals, causes misunderstanding of verbal or non-verbal cues and increases risk-taking behavior. Therefore, alcohol consumption plays a role in triggering acts of violence in individuals (Stöckl et al., 2012). In the study, it was determined that pregnant women whose spouses/partners gamble were exposed to more physical abuse. In the study, it was determined that pregnant women whose spouses/partners use drugs are also exposed to more physical abuse. One study found that partner drug use more than doubled the likelihood of perpetrating physical and sexual abuse against pregnant women (Santos et al., 2017). Studies conducted in Türkiye have also determined that women whose husbands/partners consume alcohol are more exposed to physical abuse (Akar et al., 2010; Bağcıoğlu et al., 2014; Tokuç et al., 2010).
In the study, it was determined that pregnant women whose husbands/partners are prone to violence are more exposed to physical abuse compared to others. There are studies with similar findings (Lencha et al., 2019; Makayoto et al., 2013; Shamu et al., 2011).
It has been determined that pregnant women who witnessed violence during their childhood are more likely to be subjected to physical abuse from their spouses/partners than other women. Individuals who were exposed to or witnessed violence as a youngster appear to be more likely to inflict violence towards their partners later in life (Benson et al., 2003). Domestic violence by family members is perceived as typical in future life or marriage by those who have been exposed to it as a child (Alan et al., 2016). The existence and recurrence of violence, as well as its approval by those who experienced or witnessed it, plays a significant role in the formation of personality, attitudes, and behaviors in general. If violence committed by fathers is regarded as normal behavior, it affects the development of children’s personalities. This can result in highly dangerous consequences, such as a tendency toward violence, low self-esteem, loss of self-confidence, depressive symptoms, or “submissive” behavior (Arslantaş et al., 2012). It has been determined that the number of children is also linked to the exposure of pregnant women to physical abuse. Mothers who have children between the ages of 6 and 14 are more likely to be subjected to violence than other women.
The study found that pregnant women whose social media usage and clothing were interfered with by their husbands/partners were more likely to be subjected to physical abuse than other women. According to the study, husbands/partners are more likely to engage in aggressive behavior, particularly when jealously or suspicion of cheating is present during pregnancy (Chan et al., 2011; Graham-Kevan & Archer, 2011). Stress was found to be significantly connected with moderate physical aggressive victimization in pregnant women in one study, whereas partner jealousy and suspicion of cheating were found to be significantly associated with serious physical victimization in pregnant women in another study (Hellmuth et al., 2013).
According to the findings of the study, women with a higher income contribution to the household than their husbands/partners were exposed to physical abuse more than others. According to the male-backlash model developed by sociologists and anthropologists, when women’s income contribution to the household is higher than their husbands, their susceptibility to violence increases. Men see women’s economic power as a challenge to traditional masculine standards at home, and they use violence to reclaim their dominance (Dildar, 2021).
Conclusion
IPV against women is a universal problem that transcends borders in social, cultural, religious and geographical terms. Despite national and international policies and practices on intimate partner violence against women, women are exposed to intimate partner violence all over the world. The findings of this study are significant in terms of providing information for the development of policies and programs aimed at preventing violence against women. In the event that the pregnant woman is exposed to violence, it is crucial for society to take action to protect both the mother and the unborn child’s health. In order to prevent the emergence of violence and develop effective solutions toward this goal, the viewpoint of primary care health workers in our country must be thoroughly evaluated. In addition, health personnel should receive the necessary training, support, and encouragement in these matters. In light of these findings, it is suggested that healthcare professionals should be more cautious when evaluating women with significant pregnancy-related symptoms for IPV, and that the healthcare team should be equipped with the necessary knowledge and tools. Early identification of the presence of IPV during pregnancy and the planning of interventions for cases of IPV have positive short- and long-term effects on the health of mothers and infants. It is crucial that antenatal clinics are properly set up, have screening forms available, and have protocols created to specify which interventions should be administered to IPV victims.
Considering the widespread condemnation of violence against women as a violation of fundamental human rights and an affront to human dignity, it is critical that women be made aware of the types of violence they are exposed to, what they should do when they are exposed to violence, and legal regulations. Furthermore, promoting social awareness about violence, educating children about the fact that nothing should be addressed with violence, and broadcasting in the media and other forms of mass media with the goal of preventing violence against women can all have positive outcomes. It should also be recognized that offering psychological assistance to individuals will aid in the development of family communication, the development of anger management skills, and comprehension of problem-solving process.
Despite the fact that laws exist to prohibit all forms of violence against women, the current regulations are inadequate. It is critical that institutions and organizations working in this field collaborate in order to avoid husband/partner physical abuse against women, which is a multifaceted and complicated phenomenon. State institutions, local governments, law enforcement agencies, and the media should all assume responsibility for preventing violence against women and take the required actions to achieve this. It is not enough that such organizations are simply designed to eradicate violence. The actions they take to reduce violence against women must be more stable and based on sound decisions. Otherwise, it is evident that years of diligent effort to prevent violence against women will have no purpose.
Strengths and Limitations of This Study
Data from a nationally representative sample in Türkiye were used in this investigation. Binary logistic regression was used to identify the risk factors for pregnant women in Türkiye experiencing physical violence from their partners or husbands. There are a few limitations to this study. First, the study’s data are secondary data. The variables necessary for statistical analysis are those found in the data set. Second, since the data are cross-sectional, a conclusive causal association cannot be established regarding physical abuse against women cannot be established. Thirdly, the study’s data is based on the women’s own responses. Due to the lack of official data, the results obtained by the data collection method may be biased. Fourth, in the study, women who had been pregnant at least once were asked two questions about their exposure to physical abuse. However, the times when during which these previously pregnant women were exposed to violence were not specified. The data are outdated because the most recent data on the topic was collected in 2014.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Data Availability Statement
The data underlying this study is subject to third-party restrictions by the Turkish Statistical Institute. Data are available from the Turkish Statistical Institute (