
Abstract
Immunization is a key element of public health, a pre-requisite to social and economic development, and a crucial element that enables every child to reach his or her full physical and intellectual potential. It is a prevention against various child killer diseases such as tuberculosis (Bacillus Calmette Gurine [BCG]), tetanus, whooping cough, diphtheria, poliomyelitis, hepatitis B, yellow fever, and measles. The main objective of this study is to examine the relationships between household characteristics, social mobilization, and immunization status of under-5 children in Lagos metropolis, Nigeria. To achieve this objective, a non-experimental research design was adopted. The research method utilized in the design is cross-sectional survey. The sampled study location is Ojo local government area of Lagos State. A total of 265 respondents were randomly sampled for the survey using multistage random sampling technique. Generated data were analyzed using univariate, bivariate, and multivariate statistical techniques. The findings of the study reveal significant relationship between women’s level of education and full immunization of their children. Specifically, 38.9% of women without any formal education had fully immunized their children compared with 86.9% of women with secondary education. In addition, 90.9% of women who assessed themselves to be average on wealth assessment compared with 45.3% of the poor had fully immunized their children. On the basis of the study’s findings, there is a need for a holistic approach that will involve all social classes and communities on child immunization to have 100% immunization coverage and minimal child morbidity and mortality in all areas of the city.
Introduction
Child health and, more importantly, the rates of neonatal and under-5 mortality are significant indicators to measure level of development across countries and continents globally. Consequently, reduction of under-5 mortality rate by two thirds, between 1990 and 2015, is Goal Number 4 of the Millennium Development Goals (MDG), which all countries in the world are encouraged to pursue rigorously as the target year draws closer. Recent available statistics reveal that in 2011 alone, about seven million under-5 mortality occurred globally, out of which about 41% occurred in sub-Saharan Africa and vast majority of the deaths are preventable through universal immunization coverage in the region (Rutherford, Mulholland, & Hill, 2010; UNICEF, 2012). In Nigeria, the most populous country in the region, Maduabum (2005) further noted using regional analysis that an estimated 10.8 million children die worldwide each year, of which 41% of these deaths occur in sub-Saharan Africa and 34% in South Asia. Six countries—India, Nigeria, China, Pakistan, the Democratic Republic of Congo, and Ethiopia—account for half of worldwide childhood deaths and Nigeria is ranked 2nd overall and 17th when ranked by under-5 mortality rate. Despite dearth of accurate data in the country, the situation in Nigeria is more precarious to the extent that the former minister of health, Professor Adenike Grange, recently quoting the official hospital records in the country stated that about three million babies die within 1 week of birth in Nigeria including an estimated two million who die on the first day of their lives in the country. She further added that an estimated 5.9 million babies are born in Nigeria yearly and nearly 1 million die before the age of 5 (“One Million Babies Die,” 2011). Regrettably, most of these deaths are from vaccine preventable diseases (VPDs).
In spite of its innumerable potential and overwhelming evidence of the benefits of child immunization, existing data in Nigeria reveal that there have been only small improvements in vaccination coverage in the country. Specifically, the percentage of children fully immunized by age 12 months slightly increased from 14% in the year 2003 to 19% in 2008 (National Population Commission [Nigeria] and ICF Macro, 2009). Empirical evidence has shown that women’s education has a significant relationship with greater health awareness and consequently improved general well-being of their children. It improves gender equality and children’s access to education, and is highly connected to the alleviation of poverty among women. For example, scholars over the years have observed that female education improves their earning potential and the standard of living for their own children, as women invest more of their income in their families than men do. One way in which women’s education reduces child mortality is that better-educated women tend to seek better prenatal care, thus improving the survival rate of their children (Magadi, 2002; Mba, 2006). Oyefara (2011) has found a significant inverse relationship between the education of adolescent mothers and child mortality rate among the Yoruba of Osun State of Nigeria. Indeed so strong was this inverse relationship that it was found to be significant at the more restricted confidence interval (CI) of 1%; this was also the case even among older mothers. Enlarging on the benefits of women’s education, Coleman (2010) has stated that “when women are educated and can earn and control income, a number of good results follow: infant mortality declines, child health and nutrition improve . . . and cycles of poverty are broken” (p. 13). It may therefore not be surprising that women with the highest levels of education are the ones with the healthiest children (UNICEF, 2012). As biologically, socially, and culturally recognized primary caregivers, it is imperative to critically examine the role of mothers’ characteristics on immunization uptake of their children in the country.
Previous Studies
The existing literature reveals some of the crucial factors that may affect child health at global level in general and in developing countries in particular. In recent time, scholars working on child health in Nigeria have started documenting various factors militating against child survival and ethnic differentials in under-5 mortality in the country (Adedini, Odimegwu, Bamiwuye, Fadeyibi, & Wet, 2014). Reports from international level show that efforts at eradicating childhood diseases meet with various levels of success in various parts of the world. A report by the World Health Organization states that Europe was declared polio-free in June 2002. The report explains that this result was “the culmination of a 14-year project to eradicate polio through coordinated national immunization campaigns” (as cited in “Europe Declared Polio Free,” 2003, p. 29). It adds that “the disease has already been eradicated in the Americas and the Western Pacific” (“Europe Declared Polio Free,” 2003, p. 29). In the lesser developed parts of the world, immunization campaigns may face special challenges. Antai (2009) has noted two problems militating against equitable immunization in the Niger Delta region of Nigeria: (a) The region is characterized by extensive mangrove forests, lagoons and swamps stretching over hundreds of kilometers inland, as well as poverty, poor social infrastructure, and conflicts that are exacerbated by environmental degradation from crude oil pollution. Many of the children targeted in the vaccination campaigns in the South-south region generally reside in impoverished and hard-to-reach settlements across the Niger Delta Region; (b) vaccination teams face threats from armed militias who roam the area in search of opportunities to seize control over the local oil resources. These conditions make children in these regions inaccessible to vaccination officers, and it is therefore not surprising that the author found that children in the South-east and South-south regions in Nigeria had significantly lower probabilities of receiving full immunization. Antai highlighted how mothers’ region of residence, community, hospital delivery, and so on could affect a child’s immunization status.
Carr (2004) points out that low government spending on health means that a substantial portion of health care expenditure—up to 80% in some countries—are borne by users through out-of-pocket payments. She adds that “since the poor are less likely to participate in job-based health prepayment or insurance schemes, they are more vulnerable to impoverishment as a result of medical fees” (Carr, 2004, p. 4). In other words, the poor who cannot pay for health care are thus limited in their access to health facilities and services. However, adoption of preventable mechanisms such as child immunization will invariably reduce disease burden through the prevention of child killer diseases most especially among the children of the poor who probably are less likely to avoid cost of medical care for their children. Antai (2009) in his study of immunization uptake in Nigeria has found that there is a significant relationship between mothers’ income level and the likelihood of full immunization status for their children. He noted, for instance, that children of mothers’ from the Igbo ethnic group had more than twice the likelihood of receiving full immunization compared to children of Hausa/Fulani/Kanuri mothers because the Igbos (or Ibos) have high economic power, which is a characteristic that increases their propensity to migrate from areas with poor economic opportunities into areas with higher economic opportunities, more than most other ethnic groups in Nigeria. He concludes that: “Increased socio-economic position increases the likelihood of children being fully immunized.” (Antai, 2009, p. 4)
Immunization of children can most easily be accomplished through the primary health care system. However, Carr (2004) has observed that the primary health care system is not properly integrated into most national health plans. She notes that “in a number of countries, people see primary health programmes as providing ‘primitive’ services exclusively for the poor” (Carr, 2004, p. 3). The result of the distorted view of primary health is that “although the poor have the greatest health needs, the majority of health budgets are directed towards hospitals in urban areas, which are used predominantly by better-off groups” (Carr, 2004, p. 3). This point is most poignantly illustrated by the 2011 N40 billion health budget of the Lagos State Government. While the government distributed N76,800,000 among the five primary health care centers at Onikan, Ebute-Meta, Harvey Road (Yaba), Ketu-Ejinrin, and Ijede, it granted N5 billion to the Lagos State College of Medicine (LASUCOM) and the Lagos State University Teaching Hospital (LASUTH). This was in addition to N5 billion granted for the projects at these tertiary health establishments. Then there was more than N12 billion for the bureaucracy at the ministry of health headquarters (Lagos State Government, 2011). In addition, the health care group Program for Appropriate Technology in Health (PATH; 2009) has pointed to a failing primary health care system as being to blame for the decline of child immunization in Northern Nigeria.
Indeed, recent data at macro level in Lagos State reveal that the proportion of 1-year-old children immunized against measles increased from 30% in the 2004 to 58% in the year 2006 and further up to 68% in the year 2009 and 73% in the year 2011 (Lagos State Ministry of Economic Planning and Budget, 2011). These macro data have rather masked the fundamental dynamics about children immunization uptake in the state since the decision to immunize a child is always taken within a socio-cultural context. Thus, a decision to take a child for immunization may involve more than the availability of and access to the immunization doses because the mere availability of immunization vaccines alone may not translate into higher immunization figures for children. Knowledge and attitude are critical to taking advantage of immunization facilities, and these may be affected by education, socio-economic status, environment, and other pertinent factors. Education, for example, enlightens people as to the availability of health facilities and treatment options, and so places them in positions of making more informed decision on health. However, little is known in Lagos State about the effects of mothers’ characteristics on the immunization status of their children. Thus, this study is designed to fill this lacuna in knowledge by investigating how the socio-economic status of a mother influences her knowledge, attitude, and the immunization uptake of her child.
Data and Method
Research Design and Study Setting
The study used a non-experimental research design that consists of cross-sectional survey to generate quantitative data that are reliable and valid. The adoption of this research design was to document the role of mothers’ characteristics on the immunization status of their children in a rapidly urbanized area in Nigeria. Ojo local government area (LGA) of Lagos State was selected for the study considering the heterogeneity of the residents and its geographical location. It is imperative to note that Ojo LGA is 1 of the 20 major LGAs in Lagos State, Nigeria. It was created in May 1989. Today, two local council development areas (LCDAs) have been carved out of it by Lagos State Government, namely, Iba LCDA and Oto-Awori LCDA. With this development, there were boundary adjustments. As of today, Ojo LGA shares boundaries with Oto-Awori LCDA on its Southwest; it is bounded in the East by Alimosho LGA, in the North by Iba LCDA, and in the South by the Lagoon. It also shares boundary with Amuwo Odofin LGA between military barracks and the trade fair complex. The local government had a total land mass of 180 sq. km with about 30% of it constituting the riverine area. Like other parts of the Lagos metropolis, it is made up of a complex mix of people from various parts of Nigeria. Prominent in Ojo LGA are the international trade fair complex, the Lagos State University (LASU), and the Alaba international market. While most of Ojo LGA is part of Lagos metropolis, there are certain remote areas comprised of about 15 major indigenous communities such as Tedi, Sibiri, and Ajangbadi inhabited mainly by the Aworis who are Yoruba peasant farmers and fishermen. Many women in the LGA are engaged in petty trading, while a majority of the men are either self-employed artisans or in paid employment.
Study Population and Sample Size Determination
The study population comprised mothers with children of 1 to 5 years as at the time of the study. In the case of a mother with more than one child within the age range, the last birth was recruited into the study as this gave a better reflection of the current practice of the mother. To have a representative sample size for the cross-sectional survey, a statistical formula for the estimation of representative sample size designed by Israel (1992) and re-adjusted in 2009 (Israel, 2009) was used. The formula is denoted as follows:

where N = estimated representative sample size for the survey; P = prevalence rate of immunization coverage in 2011 among under-5 children in Lagos State, which was 81.0%; Z = the standard normal distribution set at 1.96; D = the degree of accuracy set at 0.05; Z α2 = (1.96)2 = 3.8416; D2 = (0.05)2 = 0.0025; P = 81.0% = 0.810.

Therefore, N = approximately 237.
Thus, 237 respondents came out to be a representative sample of the estimated population. However, a total of 280 questionnaires were administered considering expected cases of invalid questionnaires due to incomplete response, inconsistency in the responses, or a total no response from the respondents. At the end of the questionnaire administration, a total of 265 questionnaires were found usable for the study. Thus, the non-responses and incomplete responses constitute about 5% of the total questionnaires administered.
Sampling Method
The selection of respondents for the cross-sectional survey was done using a multistage random sampling method. This sampling method was adopted due to unavailability of a sampling frame to facilitate adoption of other random samplings. Using the multistage random sampling, the LGA was first divided into wards, and from wards, communities were selected on the second stage. The third stage involves the selection of the street, while in the fourth stage buildings were selected from the street. In the fifth stage, households in the building were identified and an eligible respondent was picked from the household. To satisfy the inclusion criterion of motherhood of children of 1 to 5 years, the women were asked whether they had children who were still receiving immunization shots. On responding in the affirmative, the women were included in the study population in the selected household. In case of plural eligibility in a household, simple random method was used to select one for the study.
Research Instrument, Data Collection, and Variables Measurement
One research instrument was developed to elicit data from the respondents in the study that is questionnaire. The instrument used during the study was designed in such a way that adequate information was collected on the research questions with a view to actualizing the purpose and objectives of the study. Specifically, the questionnaire consists of 73 questions that were sub-divided into three sub-sections. Section 1 consists of questions on socio-demographic background of the participants. In Section 2, there were questions on mother’s health care utilization, and in the third section, questions on knowledge and behavior of mothers on their children’s vaccinations were asked. The fieldwork activities of the study were carried out between March and April in the year 2013. Six research assistants were recruited and trained in addition to the principal researcher to conduct the study.
Outcome Variable
The outcome variable of this study was the full immunization status of a child. This was assessed by vaccination cards and maternal history. A child was said to be fully immunized if he or she had received all of the following vaccines: a dose of Bacille Calmette Guerin (BCG); three doses of oral polio (OPV); three doses of diphtheria, pertussis, and tetanus (DPT); three doses of hepatitis B (HB); and a dose of measles by the time his or her mother was enrolled in the study.
Explanatory Variables
The main explanatory variables of this study were mothers’ characteristics. In all, a total of eight variables were used to determine the mothers characteristics in the study, and these variables were categorized into two groups for multivariate analysis. Group “A” “socio-wealth characteristics” consists of the following four variables: education, religion, ethnic background, and wealth assessment. Group “B” “nuptial-occupational characteristics” also has four variables as follows: age of the mother, occupation, marital status, and form of marriage.
Study Limitations and Ethical Issues
The major constraint of the study was the fact that many women were not ready to be interviewed due to their claims that they were very busy with their economic activities. In addition, the women had poor record keeping mechanism, most especially, with the use of immunization card where all immunization taken by a child should have been recorded. This has made the researcher to also rely on mother’s history to ascertain whether the child was fully immunized or not. It is imperative to note that human history is prone to certain level of error. In spite of these constraints and limitations, efforts were made to generate both reliable and valid data for the study. Considering the medical and social implications of the topic of the study on the respondents, some ethical factors were considered and implemented during the period of data collection. The first ethical issue is the fact that all respondents were promised total confidentiality of the information provided. In addition, there was an “informed consent” form which each of the respondents read through to understand the purpose and objectives of the study and finally signed before the commencement of each interview. Furthermore, respondents were completely anonymous in relation to their responses. In-depth interview respondents were identified in the report by their age, employment status, or pseudo names to hide their real identities.
Data Processing and Analysis
The adopted research design and method produced mainly quantitative data for the study. Consequently, quantitative methods of data analysis were used in the study. The procedures and specific methods utilized for the two data were briefly discussed below after a detailed description of the outcome and explanatory variables of the study. It is imperative to note that quantitative research method seeks to statistically appraise observable behavior with a view to providing a coherent explanation to its findings. Thus, the analysis of the collected data was done at three levels: (a) univariate analysis, (b) bivariate analysis, and (c) multivariate analysis. The univariate analysis consists of frequency distributions, percentages, and modes; bivariate analysis involves the use of chi-square (χ 2 ) to examine relationships between outcome variable and various explanatory variables; and multivariate analysis consists of one logistic regression model on outcome and explanatory variables.
Findings
This section has been sub-divided into five sub-sections, namely, “Socio-Demographic Profile of Respondents”; “Child Immunization Schedule and Records”; Child Immunization Shots: Types of Immunization Received”; “Child Immunization Status” (full or partial); and “Mothers’ Characteristics and Full Immunization Status of Their Children,” bivariate and multivariate analyses. These sub-sections are presented below accordingly:
Socio-Demographic Profile of Respondents
Data on socio-demographic profile of the respondents can be seen in Table 1 below. As presented in the table, about 4% of the sampled women were of age less than 20 years as at the time of the study. The rest were at least 20 years old. Data on educational level reveal that about 1 in every 15 (6.8%) women had not attended school at all. However, almost one third (32.8%) had attended primary school, whereas 46% had secondary education. A little over a fifth (21.1%) of the women had received higher education. The distribution of respondents by religious affiliation shows that majority (57.7%) of the sampled respondents were Christians, whereas 42.3% reported practicing Islam. The information on ethnic background shows that although the majority (46.8%) of the women were Yoruba, the Igbo were not few in comparison (41.5%). The sizable Igbo contingent may be explained by the commercial prospects of Lagos as a city, especially that part of Lagos where Alaba international market is located. The Igbo have traditionally been known as enterprising people and highly engaged in trading. In fact, it has been recognized long in Nigeria’s history that “any market without an Igbo contingent would not be successful” (Dioka, 1997, p. 87). The women of Hausa/Fulani extraction make up just 11.7% of the study population.
Percentage Distribution of Respondents by Socio-Demographic Characteristics.

Table 1 further indicates that the majority (37.4%) of the women were involved in trading and crafts, which dominate the informal economy, and 26.8% reported not working at all. Those women that reported that they were not working at all may be regarded as “full time housewives” with different forms of domestic work which can be categorized largely as unpaid labor. Even with improvements in certain respects, housework still takes a significant portion of women’s time (Henslin, 2010). It is noteworthy that only 7.2% of the women are professionals. Unemployment may have caused some of the academically qualified women to settle for non-professional careers. Also, very few women (17%) are engaged in the civil service. Despite the fact that not many of the women had higher education and that many of them were gainfully employed, a significant majority of the women (61.8%), classified themselves to be average on the scale of wealth assessment. Indeed, less than one in four respondents (24.2%) reported themselves as poor. Data on current marital status of the respondents show that 227 (85.7%) were currently married, 9 (3.4%) were separated, 2 (0.8%) were divorced, 12 (4.5%) were widows, and 15 (5.7%) were single. It is instructive to note that most of the ever-married women (87.2%) were in a monogamous marriage, whereas 47 (12.8%) were in a polygamous marriage with one or more co-wives in their matrimonial homes.
Child Immunization Schedule and Records
Elicited data on Table 2 show that 245 (92.5%) women report that their children had received some vaccination shots either during the regular schedules or during a national immunization campaign, whereas only 20 (7.5%) women reported that their children had never received any vaccination. This indicates a high level of child immunization uptake in the study area. In addition, the data in Table 2 reveal that only 15.1% of the women had a card in which the vaccination schedule dates were written. Although 205 women (77.4%) claimed that they had the card, they could not produce evidence by presenting the card. Furthermore, the table shows that out of 40 women with the vaccination cards of their children, 13 (32.5%) reported that their children have received some vaccination shots that were not recorded on the vaccination card.
Percentage Distribution of Mothers by Immunization History of Their Children.

Child Immunization Shots: Types of Immunization Received
Mothers were asked the specific immunization shots that their children had received, and their responses can be seen in Table 3 below. The table shows that the children of 239 (89.1%) women had received BCG vaccination against tuberculosis. The children of about 1 in 10 (10.9%) of sampled women had not received BCG vaccination. The BCG immunization uptake for this area is appreciable given that it is higher than the 76% figure for Nigeria (UNICEF, 2012). Furthermore, the table shows high level of polio immunization intake among the children of the women in the study location as 243 (91.7%) women had their children immunized against polio, whereas children of 22 (8.3%) women had not had the polio vaccination. The vaccination uptake against DPT was also high as 237 (89.4%) of the sampled mothers had immunized their children against tetanus, whereas 28 (10.6%) had not. The vaccination against measles had the second highest uptake after polio in the study area. Specifically, about 9 in 10 women had taken their children for vaccination against measles. The national average for Nigeria, according to UNICEF (2012), was 71%. In addition, it is important to note in the table that 220 (83.0%) women had taken their children for HB vaccination, while 45 (17.0%) had not done so.
Percentage Distribution of Mothers by Types of Immunization Ever Received by Their Children.
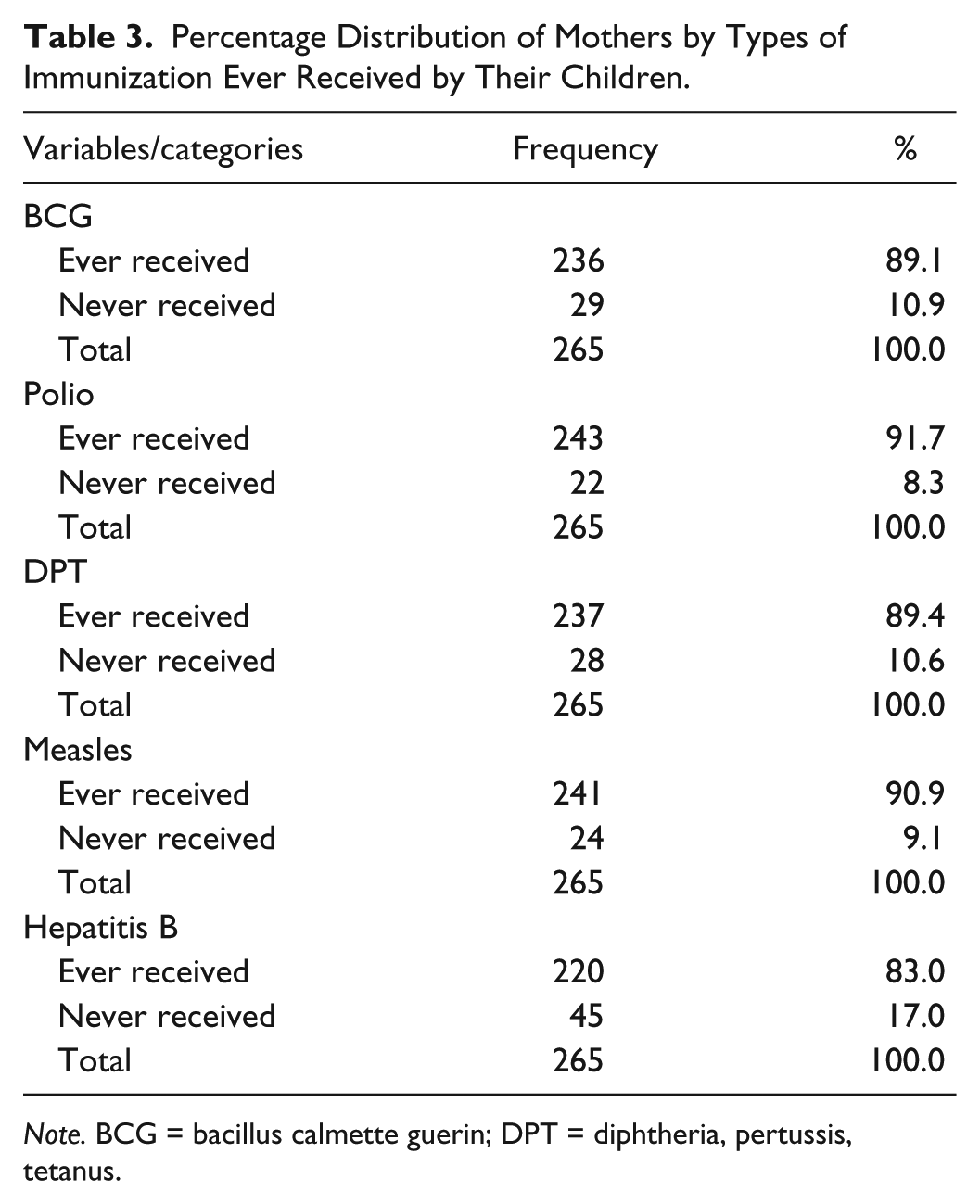
Note. BCG = bacillus calmette guerin; DPT = diphtheria, pertussis, tetanus.
Child Immunization Status
The study probed further to ask for full immunization status of the children among mothers who had ever immunized their children. Table 4 shows that the children of about 4 in 5 (85.7%) women have been fully immunized. Only 36 (14.3%) women had not fully immunized their children. Some of the reasons given for partial immunizations by the mothers are that the immunization post was too far (37.2%), lack of information on the exercise (20.0%), fear of side effects (17.1%), and the fact that the child was absent during immunization (17.1%).
Percentage Distribution of Mothers by Number of Time Their Children Received Some Immunization Shots and Reasons for Partial Immunization.

Note. DPT = diphtheria, pertussis, tetanus; HB = Hepatitis B.
Mothers’ Characteristics and Full Immunization Status of Their Children
Significant reduction to a barest minimum or total eradication of deaths and morbidities from VPDs among infants and under-5 children is the utmost desire of state and non-state actors working in the areas of child health and immunization programs in the country. This section examines the nexus between mothers’ characteristics and full immunization status of their children in the study location. To have deeper understanding of the relationships, the analysis has been sub-divided into two sections using both bivariate and multivariate statistical analytical techniques. At the bivariate level, chi-square statistical method was used to examine the initial relationships between eight socio-economic characteristics (level of education, religious affiliation, ethnic background, wealth assessment, age group, occupational status, marital status, and form of marriage) of the mothers and the full immunization status of their children. At the multivariate level, two logistic regression models were developed from the bivariate analysis. The rationale behind the two-level analysis was to determine whether those characteristics that were significant at the bivariate level will also be statistically significant at multivariate level after controlling for other explanatory variables. The two levels of analysis are presented below respectively.
Bivariate Analysis
The results of the bivariate chi-square analysis can be seen in Table 5. The first analysis examines whether there is a significant relationship between mothers’ level of education and full immunization of their children. The relationship is statistically significant with χ2 = 23.632, df = 3, p < .001, with a contingency coefficient of .286. Specifically, 38.9% of women without any formal education had fully immunized their children compared with 86.9% of women with secondary education.
Percentage Distribution by Mothers’ Characteristics and Children’s Full Immunization Status.
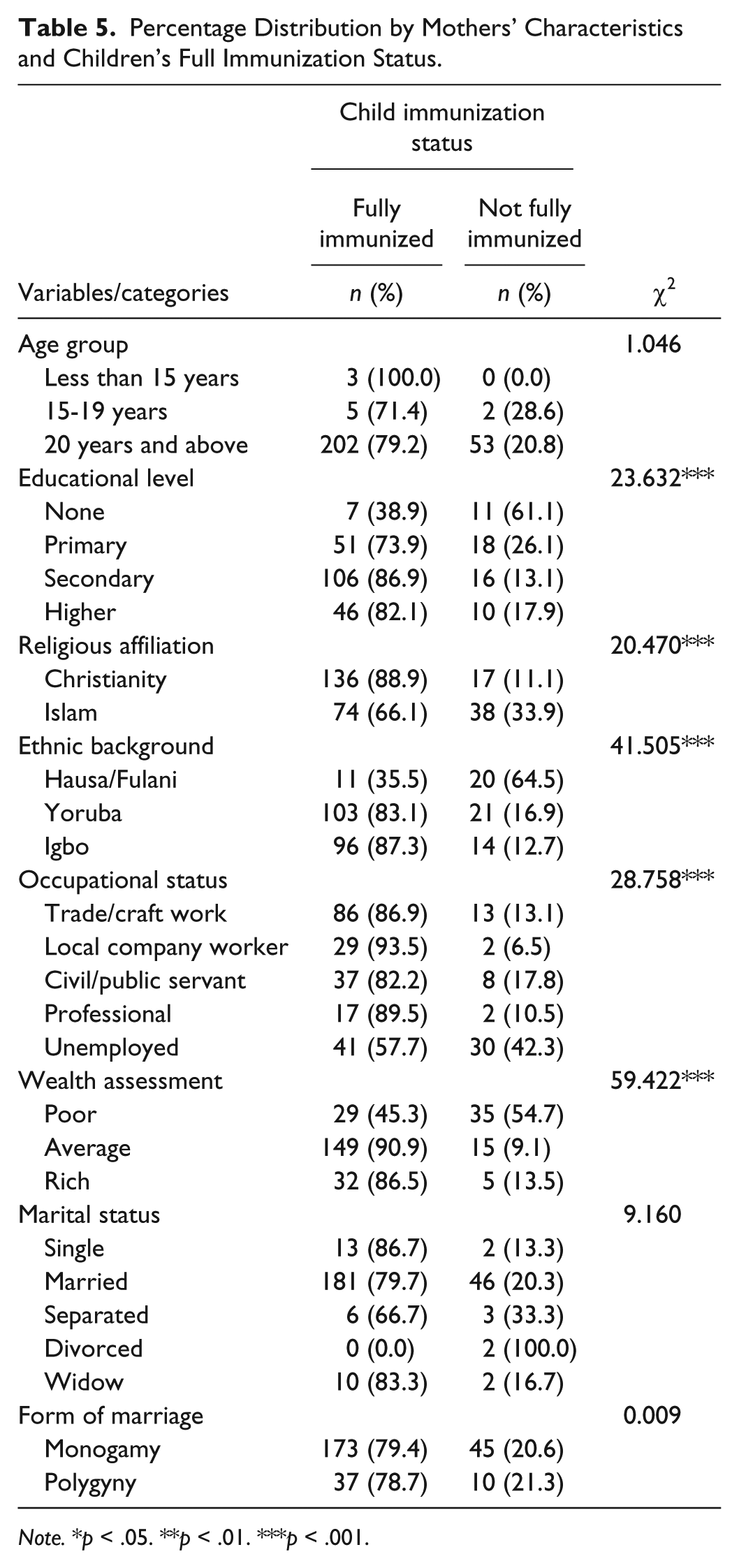
Note. *p < .05. **p < .01. ***p < .001.
The pattern of the relationship is positive in nature showing that the higher the level of education, the higher the proportion of the children who were fully immunized. The second variable is religious affiliation of the mothers. The chi-square analysis in the table also shows a significant relationship between women’s religious affiliation and full immunization of children with χ2 = 20.470, df = 1, p < .001, with a contingency coefficient of .268. In particular, about 88.9% of Christian women had fully immunized their children compared with 66.1% of Muslim women. There is also a significant relationship between ethnic background of women and full immunization of the children at p < .001. Data in the table show that 87.3% of Igbo women as against 83.1% of Yoruba women and 35.5% of Hausa/Fulani women had fully immunized their children in the study location. Personal wealth assessment of the respondents has significant relationship with full immunization of children at p < .001. Specifically, about 90.9% of women who assessed themselves to be average compared with 45.3% of those who assessed themselves to be poor and 86.5% of those who assessed themselves to be rich had fully immunized their children.
Further analysis at bivariate level shows a significant relationship between mothers’ occupational status and full immunization status of their children. The relationship is statistically significant with χ2 = 28.758, df = 4, p < .001, with a contingency coefficient of .313. Specifically, women working in the private sector (i.e., local company workers) are more likely to have fully received immunization for their children compared with other occupational status. It is imperative to note that at the bivariate level of analysis, mothers’ age group, marital status, and form of marriage were not statistically significant with full immunization status of their children even at the 95% confidence level. In all, out of the eight socio-economic characteristics examined, only five were statistically significant at the bivariate level of analysis.
Multivariate Analysis
The eight explanatory variables (education, religion, ethnic background, wealth assessment, age of the mother, occupation, marital status, and form of marriage) used at bivariate level were entered for multivariate analysis. The results of the multivariate logistic regression analysis of the model can be seen in Table 6. The findings show a significant relationship between women’s level of education and full immunization status of their children at primary and secondary levels compared with higher education at ps < .01 and .05 respectively. Specifically, the odds ratio from the model shows that women with primary education were about 0.350 times (CI = [0.063, 1.931]) as likely as women with higher education to have fully immunized their children, whereas women with secondary education were about 0.796 times (CI = [0.220, 2.878]) as likely as women with higher education to have fully immunized their children. The variation between women with no education and higher education was not statistically significant even at 0.05 level of significance. Personal wealth assessment of the women is also statistically significant with full immunization status of their children. The odds ratio from the model shows that women who assessed themselves to be rich were about 16.198 times (CI = [2.910, 90.158]) as likely as women who assessed themselves to be poor to have fully immunized their child with p < .001. Worthy to note is that religious affiliation, marital status, form of marriage, age group, and ethnic background of the women were not statistically significant at multivariate level as presented in the table. However, occupational status of the mothers was also statistically significant with the full immunization status of their children.
Multivariate Logistic Regression Model of the Effects of Mothers’ Characteristics on Full Immunization Status of Their Children in Ojo LGA, Lagos State, Nigeria.

Note. LGA = Local Government Area; OR = odds ratio; CI = confidence interval; RC = reference category.
p < .05. **p < .01. ***p < .001.
Particularly, the odds ratio shows that professional women were about 1.722 times (CI = [0.389, 7.624]) as likely as women working with local companies (private organizations) to have fully immunized their children at p < .05. Women working in the informal sector of the economy (trade and craft work) were about 0.321 times (CI = [0.090, 1.146]) as likely as women working with local companies (private organizations) to have fully immunized their children at p < .001. In addition, unemployed women were about 0.571 times (CI = [0.073, 4.451]) as likely as women working with local companies (private organizations) to have fully immunized their children at p < .05.
Discussion of Findings
Five out of the eight personal characteristics of the mothers (educational status, religious affiliation, ethnic background, occupational status, and wealth assessment) were found to be statistically related to full immunization status of their children at bivariate level. However, only three of the explanatory variables (educational status, wealth assessment, and occupational status) remain statistically significant after a rigorous multivariate logistics regression analysis. The findings of this study have showed significant positive relationship between a mother’s education and full immunization status of their children. These three variables are central and very important in the assessment of women’s autonomy and employment in the contemporary society. For instance, women with higher education were more likely to have fully immunized their children compared with women without any formal education. A very close examination of the interplay between mothers’ educational status and full immunization status of their children depicts the significant importance of women education concerning the health status and general well-being of their children. Women with exposure to little education (primary and secondary education) do have a positive attitude concerning full immunization of their children. The relationship was significant at both bivariate and multivariate levels of analysis. Conscious efforts and great commitment of educated mothers to fully immunize their children are one of those factors why scholars argued in the literature that women’s education reduces child mortality because better-educated women tend to seek better prenatal and postnatal care, thus improving the survival rate of their children (Magadi, 2002; Mba, 2006; Oyefara, 2011).
In addition, personal wealth assessment of the mothers was found to be an important factor that influenced full immunization status of their children as mothers who assessed themselves to be rich were more likely to have fully immunized their children compared with women who assessed themselves to be either poor or average. Financial autonomy of a woman gives her a greater opportunity to fund and do all necessary things that are required to get best health care services for her children as a primary caregiver. Mothers’ occupational status has been found to have significant influence on full immunization status of their children. Women who work with local companies (private organizations) and professionals are more likely than any other occupational categories to have fully immunized their children. This emerging set of women seems to be distinct considering the nature of their working environment. The working environment of these women (i.e., those working with local companies [private organizations] and professionals) is being driven by high competition; thus, they need to be proactive, visionary, and dynamic to retain their jobs in the organizations they are working with and to survive in a keen competitive environment unlike women working with the government and other informal sectors. It may be inferred that the proactiveness of their working environment will invariably make them to be abreast with modern technology and the need to maximize any existing potentiality. This unique attribute may also be deployed into the utilization and uptake of any useful available health services such as immunization for the survival of their children. Consequently, it can be inferred from this study that women who are socially and economically relatively independent and empowered are more likely to use their knowledge and available resources to procure good health services for their children such as full immunization of their children, thus maximize their survival potentiality than the ones who are less empowered.
Summary of Findings and Recommendations
This study has been able to demonstrate the significant role of mothers’ characteristics in the full immunization status of their children in the study location. Proceeding from the findings of the study, the following recommendations become pertinent: (a) governments (federal, state, and local government) need to intensify those factors that will increase women’s autonomy in the study location. Their autonomy will positively influence their decision making regarding the health of their children, most importantly, in the areas of adoption of immunization to prevent VPDs and deaths among under-5 children in the study location. Such programs should focus strongly on giving women necessary education, making environment conducive for them to be fully engaged occupationally in the formal sector of the economy, and provision of enabling environment for them to be financially independent. This will go a long way to assist them to be functional in their health seeking behavior concerning their children; (b) it is also important to educate women on the need and usefulness of keeping their children’s immunization cards especially for tracking the shots their children had collected and the outstanding/remaining ones; (c) government immunization campaigns in the study location should involve all the stakeholders (religious leaders, community leaders, associations leaders, and various community development associations) more than their current involvement. This will go a long way to educate and sensitize other mothers who may have nonchalant attitude toward the immunization of their children.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research and/or authorship of this article.