
Abstract
This study investigates the impact of city healthcare resources on immigrants’ employment quality. It has implications for promoting equity in the distribution of healthcare resources, which is critical for immigrants’ survival and settlement. Moreover, the relationship between healthcare resources and employment quality is equally relevant to developing-country urbanization. Using data from the China Migrants Dynamic Survey (CMDS) from 2016 to 2018, we demonstrate the effect of healthcare resources on employment quality. Cities’ healthcare resources are significantly correlated with immigrants’ quality of employment. The more healthcare resources are available, the higher the income from work, the shorter the working hours, and the more stable the employment of immigrants. The quality-enhancing effect of healthcare resources on employment quality is substantial among immigrants with health training and medical files. Urban medical insurance has important differentiating implications for immigrants’ access to healthcare resources. Healthcare resources enhance the employment quality of immigrants by improving their health status and integration into local society. Promoting equalizing healthcare resources and adjusting the differences between urban and rural medical insurance systems increase immigrant employment quality.
Plain language summary
Purpose: Investigate the impact of city health care resources on immigrants’ employment quality. It has implications for promoting equity in the distribution of health-care resources, which is critical for immigrants’ survival and settlement. Moreover, the relationship between healthcare resources and employment quality is equally relevant to developing-country urbanization. Methods: Using data from the China Migrants Dynamic Survey (CMDS) from 2016 to 2018, we demonstrate the effect of healthcare resources on employment quality. The more healthcare resources are available, the higher the income from work, the shorter the working hours, and the more stable the employment of immigrants. Healthcare resources enhance the employment quality of immigrants by improving their health status and integration into local society. Conclusion: Improving immigrants’ employment quality could be achieved by promoting equalization of healthcare services, strengthening immigrants’ awareness of health risk prevention, expanding medical insurance coverage, and increasing participation in basic urban medical insurance. The study highlights the need for policy details to connect rural medical insurance with urban medical insurance and achieve medical reimbursement in different places, given the mobility and job instability of immigrant workers in China.
Introduction
China has the largest migration worldwide, from rural to urban areas and from agriculture to non-agriculture. According to the Migrant Worker Survey Report 2021 from China’s Bureau of Statistics, the total number of migrant workers nationwide in 2021 is 292.51 million, with 130.09 million migrant workers living in cities and towns at the end of the year. The quality of employment of most migrant workers from rural to urban areas is significantly different from that of urban natives. First, the income is low, and the wage satisfaction is low. In 2021, the average monthly income of migrant workers was 4,432 CNY, which is only half of the average monthly wage of urban employed people in the same period. Secondly, employment stability is poor, and a sense of security is lacking. Migrant workers change jobs frequently, and the proportion of non-stably employed migrant workers is about 61%. Third, long working hours and overtime work are the common practice. The average monthly working hours of migrant workers in Guangdong have reached 225 hr from January to March 2021. About 85% of migrant workers have overtime work, about 47.2% are in illegal overtime work, and 21.27% are in illegal severe overtime work. Within the same institutional context, the differentiation of the structure and the informal regulation of the labor market lead to significantly different penalty mechanisms for immigrants and natives (Avola & Piccitto, 2020). Drawing on the inequality perspective, Stainback examines the relationship between hukou (household registration) and job quality—paying particular attention to (1) nonstandard employment and (2) the ownership sector (Stainback & Tang, 2019). Low-skilled immigrants are concentrated in low-wage jobs and have lower incomes than native low-skilled laborers (C. Y. Liu, 2011; Polavieja et al., 2018). Integration of immigrants leads to two occupational outcomes: the probability of being employed and the probability of avoiding the unskilled working class (Panichella, 2018).
Based on the above characteristics of the quality of employment of migrants, it is meaningful to study the factors influencing the quality of employment to promote the integration of migrants into the city. The resources of the city, especially healthcare resources, are among the crucial factors. The focus of this paper is on how healthcare resources affect the employment of immigrants and to analyze what heterogeneity exists.
Literature Review
The quality of employment has been studied since the early 1970s, from the quality of working life to decent work by the International Labour Organisation and, more recently, quality employment. Research concerning the quality of employment has been gradually enriched and improved. Academics have used a variety of indicators to measure migrants’ employment quality, including employment rates, income, wage, adequacy of paid work, employment status, employment flexibility, and stability (Cangiano, 2014; Clibborn & Wright, 2018; Dietz et al., 2015; Riaño, 2021; Wright & Clibborn, 2019). Using longitudinal data, studies have revealed that health shocks affect many labor market outcomes, such as labor and household income, employment status, and hours worked (Lenhart, 2019). The health associations of different employment arrangements in the contemporary European labor market has been verified (Gevaert et al., 2021). The set of variables representing employment is informative for our study of the impact of healthcare resources. The indicators used in this paper to measure the quality of employment include work income, working hours, and employment stability.
Healthcare Resources Affect Productivity and Income
The more healthcare resources a city has, the better the state of the health of its inhabitants. There is a positive effect of health expenditure on health. Many empirical articles have verified that healthcare resource investment positively and significantly impacts health capital and ultimately increases productivity (Audibert & Etard, 2003; Bloom et al., 2020; Combary & Traore, 2021; Croppenstedt & Muller, 2000; Halıcı-Tülüce et al., 2016; Leijten et al., 2014; Rivera & Currais, 2004). Studies have demonstrated that improvements in health lead to a general increase in worker productivity (Grossmeier et al., 2016, 2015; Rudolph & Baltes, 2017); health status and labor productivity positively impact economic growth (Kelani et al., 2019). Studies have verified that the relationship between healthcare access and productivity is the most vigorous in metro areas. A 1% increase in physicians per 100,000 persons could increase earnings per worker by $68.21 to $81.10, depending on the health measure. However, the increase in metro areas is nearly 10 times higher than in nonmetro areas. Health risk, absence, and health shocks lead to productivity losses (García-Gómez et al., 2013; Goetzel et al., 2004; Halla & Zweimüller, 2013). Adverse health shocks negatively affect employment, wages, and income. These effects are vital for males, the less educated, those with lower incomes, those in middle-ranking and professional occupations, and those experiencing the most severe health shocks (Aleksandrova et al., 2021). This paper focuses on the impact of healthcare resources on productivity and income. On the one hand, higher health capital allows employees to have healthy bodies and abundant energy to engage in productive activities (see Figure 1). On the other hand, higher health capital leads to less sickness, less leave, less loss of work time, and a more effective labor supply. A severe illness affects not only one’s working hours but also the working hours of other family members due to the need for care. A healthy body reduces the loss of work time and the economic burden caused by illness.

Logic of the impact of healthcare resources on income.
Health Status and Immigrants’ Labor Supply and Employment
The effect of health status on working hours is generally negative, and poor health reduces working hours. The population’s health status (measured by life expectancy at birth) is positively related to labor force participation (Novignon et al., 2015). Poor health implies a shorter life expectancy, increasing the incentive to retire, and many may leave the workforce. Leaving the labor market because of persistently low health status levels or new health shocks is a possible response for employees. A lower health status results in fewer working hours, and when they occur, health shocks lead to further reductions in working hours. An empirical study separated the time-persistent effect of health status and the potentially shorter health shocks on working hours (Cai et al., 2014; Jones et al., 2020). There is a substantial decrease in labor market participation, hours, and earnings (Lundborg et al., 2015). Health shocks reduce the labor supply. These impacts are more substantial among women, older workers, and those with more severe impairments. Younger workers display a stronger labor market attachment. There is a significant causal effect of health on the probability of employment: individuals who incur a health shock are significantly more likely to leave (Delattre et al., 2019; García-Gómez, 2011). Suffering a health shock decreases the probability of remaining in employment by 5% and increases the probability of transitioning into inactivity by 3.5%. General health effects on entering and exiting employment, and the effects are higher among men than women (García-Gómez et al., 2010). Health shocks can reduce productivity because people cannot work due to illness or the necessity to care for sick family members. This can reduce income and aggravate pre-existing poverty. Health shocks can also strain public health systems, raising healthcare costs. This can potentially reduce government spending on education, infrastructure, and housing. Third, health shocks can increase public debt by forcing governments to borrow money for health care and other services.
Healthcare Resources Affect the Immigrants’ Stability of Employment
Immigrants’ access to healthcare resources affects their settling intentions (Sangaramoorthy & Guevara, 2017; Serra Mingot & Mazzucato, 2019). A city with many doctors and hospital beds is more attractive. Immigrants with a propensity to settle are more likely to seek stable employment. Settled employees are more likely to have a long-term employment contract with their employer to achieve stable employment. This paper analyses the impact of healthcare resources on employment stability by adopting employees entering into employment contracts as a proxy variable for stability. However, immigrants are not treated the same as locals, reducing their settling propensity. It is difficult for immigrants to access healthcare resources (Castaneda, 2013; Chin et al., 2018; Lattof, 2018; Pandey et al., 2021). Compared to residents, a lack of local insurance is the main barrier to healthcare services among immigrants (Cheng et al., 2015; Douthit et al., 2015; Mandal, 2022). Participating in health training in the community and establishing local health records improve the accessibility of immigrants to urban healthcare resources (Wang et al., 2021). This paper considers these factors when analyzing the impact of healthcare resources on employment stability. The health status and the integration of immigrants are affected by healthcare resources (Bell et al., 2013). Immigrants’ settlement propensity is correlated with their health status (Hu et al., 2008; Lu & Qin, 2014; Xie et al., 2017). Cities with abundant and easily accessible medical resources have residents with better health status and a stronger sense of integration (He et al., 2019). Immigrants’ health status and integration must be included in the analysis mechanism.
In summary, research has focused on the influence of healthcare resources on productivity and employment while ignoring the impact on job quality. Most recent research has focused on health status and shocks impacting immigrants’ income. Other dimensions of employment quality, such as job stability, have received less attention. This paper focuses on employment quality by considering employment quality in terms of income, working hours, and employment stability. Analyzing healthcare resources’ impact on immigrants’ quality of employment is relevant for understanding migration and employment. Cities with more medical resources tend to enable immigrants to achieve high-quality employment. We offer explanations for these findings and suggest directions for future research.
The first part of the paper provides the background of the study and literature review. The data section describes the data sources used and the data cleaning process. We explain the variables and the reasons for their selection. In the Methods section, we outline the innovative methodology we implemented to investigate the complex links between healthcare resources and the quality of employment. After we present and discuss the results, we conclude with some implications and directions for further research.
Methodology
Data
This paper employs survey data from the China Migrants Dynamic Survey (CMDS). CMDS is an annual large-scale national migrant population sample survey conducted by the National Health Commission since 2009. The CMDS covers 31 provinces (autonomous regions and municipalities) with a high concentration of migrant population in the inflow areas. The annual sample size is nearly 200,000 households. The survey covers the basic demographic information of the migrant and family members, the scope and tendency of mobility, employment, and social security, income and expenditure, residence, basic public health services, marriage, and family planning services management, children’s mobility, education, and psychological culture. We focused on the employment quality of the migrating workforce and selected survey data from 2016 to 2018.
When processing the dataset, (1) we limited the sample to females aged 18 to 55 and males 18 to 60 because China’s retirement age is 55 and 60. (2) We merged the mixed multi-wave survey data with macro data to obtain cities’ healthcare resources, control variables, and regional fixed effects. We removed observations with no area administrative codes and observations with missing data. After the data processing, the sample size was 249,495, including 106,630 women and 142,865 men. The gender ratio is roughly balanced. The average age of the respondents was 35.2. In Supplemental Appendix Table S1, we report the sample size of the individual observations and city variables by year.
A selective list of variables used in the regression analysis is shown in Table 1. The independent variable is the city’s healthcare resources, including the number of hospitals, hospital beds, and physicians. Physicians refer to practicing physicians and physician assistants, including those engaged in medical and preventive healthcare work and excluding those involved in management. Hospitals, beds, and physicians are good indicators of a city’s primary healthcare services (Deller, 2022).
Key Variable Description.

Note. The classification of occupations including: 10 = Legislators, senior officials and managers; 20 = Professional and technicians; 30 = Clerks; 41 = Individual or small businessmen; 42 = Traders; 43 = Restaurant and catering; 44 = Domestic helpers; 45 = Cleaning; 46 = Security; 47 = Renovation; 48 = Couriers; 49 = Other commercial and service; 50 = Agricultural and fishery workers; 61 = Manufacturing; 62 = Transportation; 63 = Construction; 64 = Plant and equipment operators; 70 = No fixed occupation; 80 = Other elementary occupations.
The dependent variable is the quality of employment of immigrants. Currently, scholars are drawing upon the more comprehensive system of indicators of employment quality involving the following six dimensions constructed by Leschke and Watt: wages, nonstandard forms of employment (inverted), working time and work-life balance, working conditions and job security, access to training and career development, and collective interest representation (Leschke & Watt, 2014). Employment quality is currently widely acknowledged to be a multidimensional phenomenon (Cappelli, 2006; Eurofound et al., 2012; Muñoz de Bustillo et al., 2011; Smith et al., 2008). We measure employment quality using wages, hours worked, and employment stability. These variables are proxied using the following three objective indicators: the logarithm of income, working hours per week, and the presence of an employment contract. The choice of variables for inclusion in such an analysis is also driven by data availability. Working hours are a standard indicator of the quality of employment. High-quality employment does not require long hours, high workloads, and strict compliance with China’s labor contract laws. Lower-quality employment requires longer working hours. Employment with a labor contract (yes = 1; no = 0) tends to be more stable and likely to lead to high benefits and long-term development. When a city is more affluent in healthcare resources, laborers are more likely to settle down, sign longer-term employment contracts, and achieve stable employment.
Higher incomes indicate better quality of employment for migrants. We divided all cities into three equal groups according to their healthcare resources by year. A subsample of cities with more, medium, and fewer beds was obtained and classified according to the number of beds per year. The subsample of cities with more beds and those with fewer beds is presented in the upper part of Figure 2. The kernel density distribution of the income of the respondents in cities with more beds is shown in red with the crest to the right and a mean value of 8.19. The kernel density distribution of the income of the respondents in cities with fewer beds is shown in blue with the crest to the left and a mean value of 8.02. Respondents in cities with more beds are higher-income earners. We test the means of the logarithm of income of the two groups of respondents, and they differ significantly at the 1% level. The bottom part of Figure 2 shows the subsample of physicians by city. The income distribution of the respondents in cities with more physicians is shown in green with the crest to the right and a mean value of 8.2. The income distribution of the respondents in cities with fewer physicians is shown in black with the crest to the left and a mean value of 7.97. The difference in mean values between groups was significant at 1%. Respondents in cities with more physicians have higher incomes.

Respondents’ income in cities with more and fewer medical resources.
The control variables include demographics, regional controls, and fixed effect variables as follows: (1) the demographic variables include education, gender, race, marital status, Hukou (household registration), age, the number of children under 18, and the number of family members; (2) a city’s control variables include GDP growth, the logarithm of wages per capital, the logarithm of the population, the logarithm of private sector employment and self-employment in urban areas, and the logarithm of registered unemployment; and (3) the effect of health capital on employment is occupationally heterogeneous. The effects are the strongest among the less educated and those with middle-ranking and professional occupations. (Aleksandrova et al., 2021) Therefore, we not only include regional and year-fixed effects in our analysis but also account for occupational fixed effects. The individual weights of the survey dataset are included in all model estimates.
Methods
In the main regression, the regression models are Ordinary Least Squares (OLS) and Probit models. The measures of employment quality we use include the dimensions of work income, working hours, and employment contract. When the dependent variables are work income and working hours, which are continuous variables, the regression is OLS. The Probit model is appropriate when the dependent variable is employment contract, a binary variable.
In the endogeneity analysis part, instrumental variable models are good choices. As migration patterns evolve, local governments are taking steps to accommodate increased demands for healthcare resources. Notably, the influx of immigrants into local communities has increased the number of individuals employed in healthcare occupations, thereby boosting the overall supply of healthcare resources. There is a significant causal effect of health on the probability of employment: individuals who incur a health shock are significantly more likely to leave and transition into disability (Delattre et al., 2019; García-Gómez, 2011; Schmitz, 2011). However, it is important to recognize that endogeneity issues may be at play when attempting to assess the causal impact of healthcare resources on employment outcomes. OLS regressions, for example, may yield biased results due to the potential for unobserved confounding variables.
To address this issue, we turn to an instrumental variables (IV) approach, using distance from a household’s homestead to the Health and Social Promotion Center (HSPC) as an instrumental variable for healthcare resources. Additionally, we consider various geographical factors, such as a city’s administrative size and built-up area, as additional instrumental variables (Combary & Traore, 2021). Theoretically, the administrative size of a city and the built-up area are suitable instrumental variables. We present in the part of Empirical Results that two instrumental variables do not directly affect the quality of employment of the immigrants. However, they affect the health care resources. The instrumental variable models are two-Step Least Squares (2SLS) and IV Probit.
Next, we analyze the two heterogeneous factors of healthcare resources on the quality of employment: health training and medical files. The accessibility to healthcare resources in a city is an essential determinant of immigrants’ quality of employment and permanent employment. The availability of healthcare resources in a city is the first level of influence, and accessibility is a second level determinant. It is necessary to construct difference-in-difference (DID) models to discern the effects of health resource accessibility. We opt for health training in the community (0 = No, 1 = Yes) and having a medical file in the local area (0 = No, 1 = Yes) as proxy variables for the accessibility of healthcare resources. Health training in the community helps immigrants understand the process of access to healthcare resources. Medical files indicate the ease of access to healthcare resources for immigrants. People who have established medical files locally are generally former health resource users and can quickly provide additional health information to their doctors. The interaction terms of hospitals, beds, and physicians with medical files are added to the models. After integrating the accessibility to healthcare resources and medical insurance, we employ the difference in difference in a different model (DDD) to analyze the effect of healthcare resources on immigrants’ employment quality.
In the final part of the empirical analysis, the mechanism of healthcare resources’ impact on employment quality was analyzed using logit and Order Logit (OLOGIT) models. The provision of healthcare resources directly impacts the health status of residents in urban areas, subsequently affecting their quality of employment. Prior studies have found a positive association between the availability of healthcare resources and better health outcomes among city residents (Cai, 2020; Contoyannis & Rice, 2001). Furthermore, evidence suggests that individuals in good health enjoy a higher quality of employment, as indicated by higher wages and increased labor participation rates (Albanesi & Olivetti, 2015; Darkwah, 2019). Empirical research has estimated that the hourly wages of employees in excellent health are 13.2% higher than those in poor health (Kidd et al., 2000). To further understand the mechanisms underlying the relationship between healthcare resources and health status, we analyzed self-assessed health as a proxy variable for health status. Specifically, we employed OLS and OLOGIT models to examine the effects of hospitals, hospital beds, and physicians on the health status of immigrants.
To summarize, the empirical line of this paper is Main regression—Endogeneity analysis—Heterogeneity in access to healthcare resources—Heterogeneity in medical insurance—Mechanism analysis. The flow chart of the research methodology can be summarized in Figure 3.

Flow chart of empirical analysis.
Empirical Results
Main Regressions
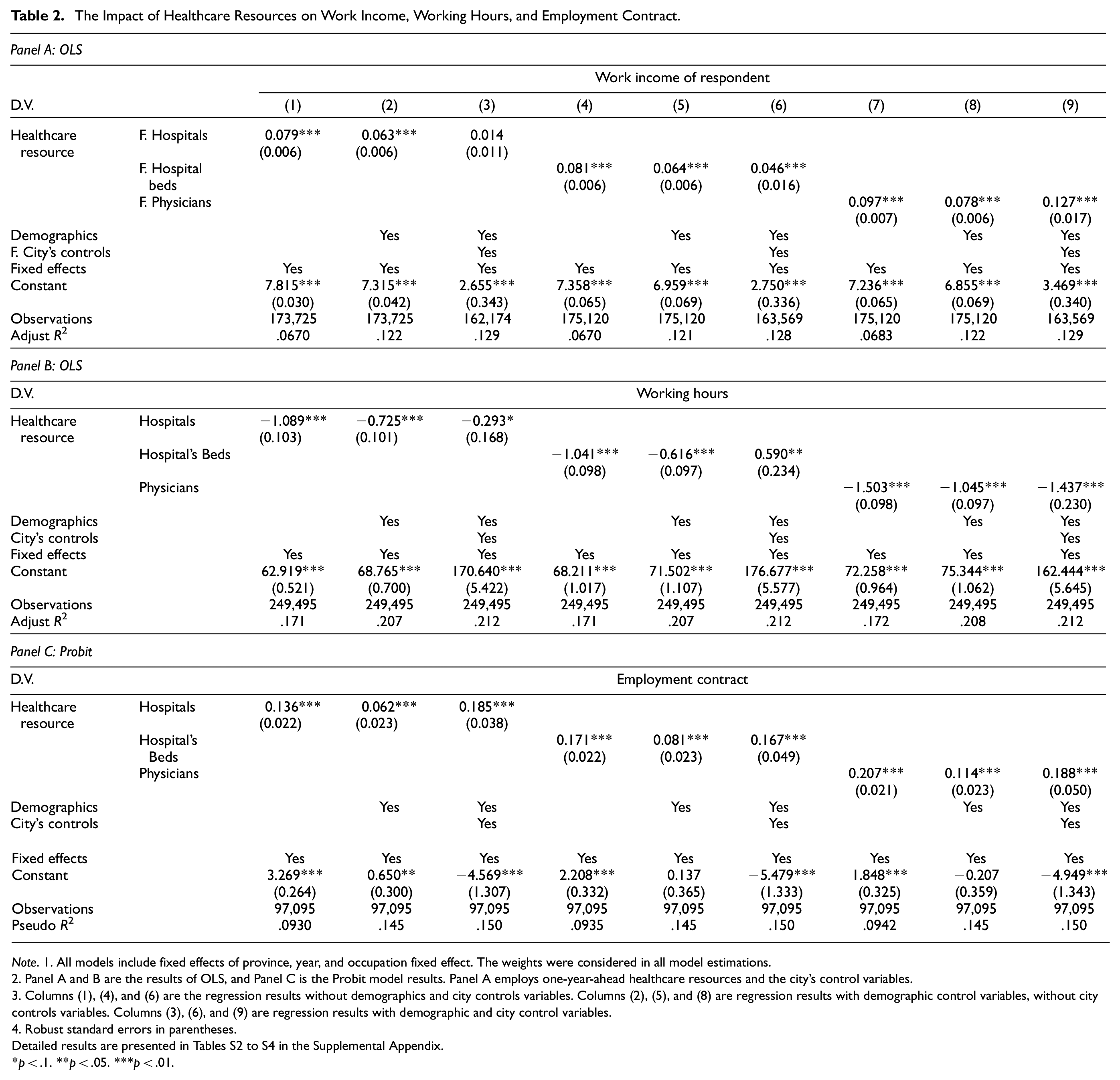
We developed separate regression models with three dimensions of employment quality, namely, work income, working hours, and employment contract, as dependent variables. Concise results are reported in Table 2. Detailed results are presented in Tables S2 to S4 in the Supplemental Appendix. In this case, healthcare resources and city control variables for models with income as the dependent variable use data from one year ahead. For example, the 2015 city variable was used to estimate the income obtained from the 2016 questionnaire. This is because the income of the respondent is from the last year.
The Impact of Healthcare Resources on Work Income, Working Hours, and Employment Contract.
Note. 1. All models include fixed effects of province, year, and occupation fixed effect. The weights were considered in all model estimations.
2. Panel A and B are the results of OLS, and Panel C is the Probit model results. Panel A employs one-year-ahead healthcare resources and the city’s control variables.
3. Columns (1), (4), and (6) are the regression results without demographics and city controls variables. Columns (2), (5), and (8) are regression results with demographic control variables, without city controls variables. Columns (3), (6), and (9) are regression results with demographic and city control variables.
4. Robust standard errors in parentheses.
Detailed results are presented in Tables S2 to S4 in the Supplemental Appendix.
p < .1. **p < .05. ***p < .01.
Panel A in Table 2 reports the effect of healthcare resources on the working income of immigrants. Columns (1) to (3) are estimators of the effect of the number of hospitals. In Column(2), the model’s results with demographic variables show that the number of hospitals significantly affects the working income of immigrants. However, once the city’s controls are added, the coefficient shown in Column (3) becomes nonsignificant, implying that further analysis is needed to confirm a robust effect. Columns (4) to (6) report the estimator of the effect of the number of hospital beds on immigrants’ work income. The number of hospital beds has a significant positive effect on the income of immigrants regardless of whether the city control and demographic variables are added. The coefficient is significantly positive at the 1% level. Columns (7) to (9) report the regression results of the effect of the number of physicians on immigrants’ work income. The number of physicians also has a positive effect on income. So, these results suggest that the more affluent the city’s healthcare resources are, the better the quality of employment for immigrants.
Panel B reports the effect of healthcare resources on the working hours of immigrants. Columns (1) to (3) show that the number of hospitals significantly negatively affects the working hours of immigrants at the 1% level. Columns (4) to (6) indicate that the number of hospital beds negatively affects working hours at the 1% significance level. The coefficient is significantly negative. Columns (7) to (9) reveal that the number of physicians significantly negatively affects the working hours of immigrants at the 1% significance level. The healthcare resources of a city significantly adversely affect the working hours of immigrants. Thus, the more healthcare resources available in the region of immigration, the better the quality of employment.
Panel C reports the effect of healthcare resources on the employment contract. We were limited to obtaining data on employment contracts for 2016 to 2017 for estimation. Employment contracts were treated as a binary variable (0 = No, 1 = Yes), and the percentages of those with and without an employment contract were 34.73% and 65.27%, respectively. This metric is a proxy for employment stability, an essential aspect of employment quality. Immigrants with an employment contract are more likely to settle locally and access higher-quality jobs. Columns (1) to (3) show that the higher the number of hospitals in the place of immigration, the immigrants are more likely to enter employment contracts. The results in columns (4) to (6) reveal that the number of hospital beds significantly positively affects the number of immigrants entering employment contracts at the 1% level. Similarly, the results from Columns (7) to (9) indicate that the abundance of physicians promotes employment contracts and increases the employment stability of immigrants. The above regression results suggest that a city’s healthcare resources significantly increase the employment stability of immigrants. Cities with abundant healthcare resources are more attractive and promote stable employment among immigrants.
Endogeneity Analysis
To address the bias due to endogeneity, the instrumental variables used in this paper are the administrative size of a city and the built-up area. On the one hand, the larger the city, the higher the number of hospitals and the higher the total number of healthcare resources. On the other hand, the size of the administrative area and the built-up area have no direct impact on immigrants’ employment quality. Therefore, we test whether these two instrumental variables directly affect the dependent variable (Table 3). Sometimes Administrative size is not an adequate instrumental variable as it can directly and significantly affect employment contracts (Columns (3)). We only use the Built-up area as an instrumental variable for robustness.
Testing the Validity of Instrumental Variables.

Note. 1. All models include demographic variables, city control variables, city fixed effects, year fixed effects, and occupation fixed effects. The weights were considered in all model estimations.
2. Columns (1) and (2) are the regression results of the OLS. Column (3) is the regression results for the Probit model; Column (1) employs one-year-ahead Administrative size of the city, Built-up area, and city’s control variables.
3. Standard errors in parentheses.
p < .1. **p < .05. ***p < .01.
The results of the instrumental variables model estimation are shown in Table 4. Columns (1) to (3) show the effects of hospitals, hospital beds, and physicians on work income. These values are the estimated results of two-step least squares (2SLS). The number of hospitals, hospital beds, and physicians significantly positively affects immigrants’ income and is significant at the 1% level. Columns (4) to (6) present the 2SLS estimates of the effects of hospitals, hospital beds, and physicians on working hours. Healthcare resources have a negative effect on the working hours of immigrants, which is significant at the 1% level. Columns (7) to (9) report the IV PROBIT models’ estimated results on the effect of healthcare resources on employment contracts. The Wald test of exogeneity shows that the built-up area is an exogenous instrumental variable. The results of the instrumental variable model (Table 4) validate the findings of the basic regression (Table 2). Increasing the supply of healthcare resources contributes to higher income, fewer working hours, and stable employment among immigrants.
The Impact of Healthcare Resources on Employment Quality.

Note. 1. Instrument variable is the Built-up area of the city.
2. All models include demographic variables, city control variables, province fixed effects, year fixed effects, and occupation fixed effects. The weights were considered in all model estimations.
3. Columns (1) to (6) are the regression results of the Two-Step Least Squares method. Columns (7) to (9) are the regression results for the IV Probit model. Columns (1) to (3) employs one-year-ahead built-up area, healthcare resource, and city’s control variables.
4. Robust standard errors in parentheses.
p < .1. **p < .05. ***p < .01.
Heterogeneity in Access to Healthcare Resources
A DID analysis was performed separately for the hospital, bed, physician, and health training interaction items and medical files. Concise results are reported in Table 5.
Impact of Health Training and Medical Files on Access to Healthcare Resources.

Note. 1. All models include demographic variables, city control variables, province fixed effects, year fixed effects, and occupation fixed effects. The weights were considered in all model estimations.
2. Columns (1) to (3) employ one-year-ahead healthcare resource and city’s control variables.
3. Robust standard errors in parentheses.
Detailed results are presented in Table S5 and S6 in the Supplemental Appendix.
p < .1. **p < .05. ***p < .01.
Panel A in Table 5 reports the effect of the interactions between healthcare resources and health training on immigrants’ employment quality. All models incorporate city control and demographic variables. Columns (1) to (3) suggest that healthcare resources have a greater income-raising effect on immigrants who participated in health training. Columns (4) to (6) show that healthcare resources’ working hours reduction effect is more profound in the group of immigrants who participated in health training. Columns (7) to (9) reveal that the employment-stabilizing effect of healthcare resources is more substantial in the group of trained immigrants. Participating in healthcare training implies that access to healthcare resources is favorable. The results of the DID analysis suggest that availability significantly increases the impact of healthcare resources on employment quality.
Panel B in Table 5 reports the impact of the interactions between healthcare resources and medical files on immigrants’ employment quality. Immigrants with medical files use healthcare resources more, which can significantly improve employment quality. In conclusion, health training and medical files enhance the impact of healthcare resources and improve immigrants’ employment quality to a greater extent.
Heterogeneity in Medical Insurance
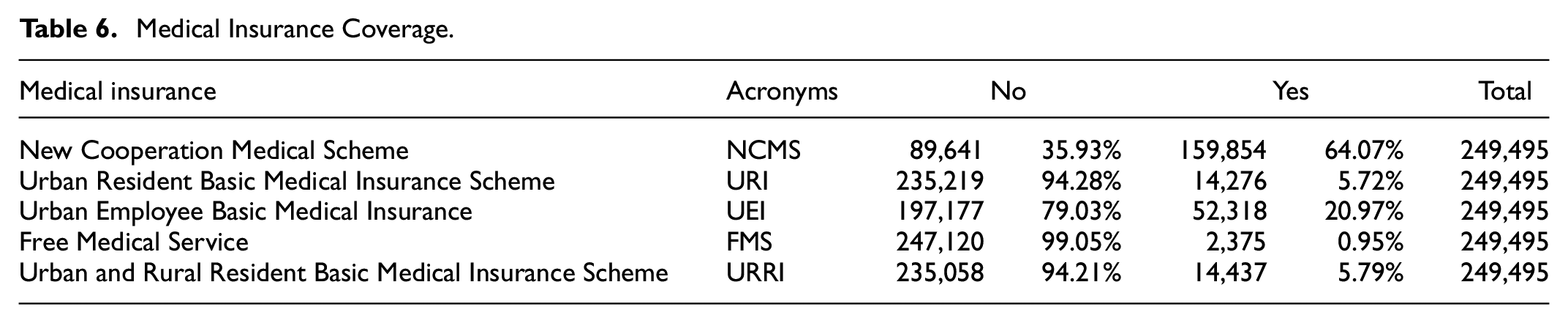
Participation in local medical insurance is crucial for immigrants, and immigrants without local medical insurance have difficulty accessing local healthcare resources. The direction of population migration in China is from rural to urban areas. China currently has five parallel public health insurance systems. The New Cooperation Medical Scheme (NCMS) mainly focuses on pooling serious diseases to provide medical assistance to the rural poor. Urban medical insurance includes the Urban Resident Basic Medical Insurance Scheme (URI), Urban Employee Basic Medical Insurance (UEI), and Free Medical Service (FMS). NCMS is for rural residents. URI is for urban residents. UEI is for employees in nonagricultural employment. Most respondents were enrolled in NCMS (64.1%), URI (5.79%), and UEI (20.91%) coverage. The Urban and Rural Resident Basic Medical Insurance Scheme (URRI) is a merger of NCMS and URI proposed in 2016. A few participants purchased coverage from the merged URRI (5.79%). FMS is mainly for civil servants and people in nonprofit organizations. The percentage of those enrolled in FMS (0.95%) is low because it is mainly for civil servants. The number of participants in the five types of insurance is shown in Table 6.
Medical Insurance Coverage.
Medical insurance is an essential determinant of immigrants’ access to local healthcare resources. We divide medical insurance into rural medical insurance (insurance = 0) and urban medical insurance (insurance = 1). Rural medical insurance is NCMS. Urban medical insurance includes URI, UEI, FMS, and URRI. Rural medical insurance is more advantageous in rural areas but is reimbursed at a lower rate in urban areas. Urban medical insurance has better benefits for access to healthcare in a city. Having urban medical insurance has an influential impact on immigrants’ access to city healthcare resources. The interactions between healthcare resources and medical insurance were included in the DID model. The results are shown in Table 7. In Columns (1) to (3), the interactions between hospitals and medical insurance (hospital beds and medical insurance or physicians and medical insurance) significantly affect immigrants’ income at the 1% level. Given the same supply of healthcare resources, immigrants with urban medical insurance have higher incomes. Urban medical insurance helps promote a more significant effect on healthcare resources. In Columns (4) to (6), the interactions between healthcare resources and medical insurance significantly negatively affect the working hours of immigrants at the 1% level. The shorter working hours’ effect on healthcare resources is stronger among those with basic urban medical insurance. In Columns (7) to (9), the coefficient of the interactions between healthcare resources and medical insurance on employment contracts is significantly positive. The stabilizing employment function of healthcare resources is more pronounced among the urban medical insurance population.
The Impact of Medical Insurance on Access to Healthcare Resources.

Note. 1. All models include demographic variables, city control variables, province-fixed effects, year-fixed effects, and occupation-fixed effects. The weights were considered in all model estimations.
2. Columns (1) to (3) employ one-year-ahead healthcare resource and city’s control variables.
3. Robust standard errors in parentheses.
Detailed results are presented in Table S7 in the Supplemental Appendix.
p < .1. **p < .05. ***p < .01.
Immigrants covered by urban medical insurance generally have more stable employment in cities. Participation in urban medical insurance is more conducive to immigrants’ continued easy access to healthcare resources, further improving the quality of their employment. Those with basic urban medical insurance and who know how to access healthcare resources quickly benefit the most from a city’s healthcare resources. The first difference is the city’s healthcare resources available, which affects immigrants’ employment quality. The second difference is the accessibility to healthcare resources. Immigrants with health training and medical files are more likely to have access to healthcare resources, which influences healthcare resources’ effect. The third difference is the category of medical insurance. Urban medical insurance facilitates access to a city’s healthcare resources and influences the final effect of healthcare resources.
The results of the DDD are shown in Table 8. Panel A reports the effect of the interactions among healthcare resources, health training, and medical insurance on immigrants’ employment quality. The coefficients of the interactions shown in Columns (1) to (3) are significantly positive, those shown in Columns (4) to (6) are significantly negative, and those shown in Columns (7) to (9) are significantly positive. All coefficients are significant at the 1% level. Immigrants with health training and urban medical insurance are more likely to have better access to healthcare resources. Healthcare resources can have larger effects on improving the quality of their employment. Panel B in Table 8 presents the effect of the interactions among healthcare resources, medical files, and medical insurance on immigrants’ employment quality. Healthcare resources are more influential among immigrants with medical files and urban medical insurance.
Impact of Health Training, Medical Files, and Insurance on Access to Healthcare Resources.

Note. 1. All models include demographic variables, city control variables, province-fixed effects, year-fixed effects, and occupation-fixed effects. The weights were considered in all model estimations.
2. Columns (1) to (3) employ one-year-ahead healthcare resource and city’s control variables.
3. Robust standard errors in parentheses.
Detailed results are presented in Tables S8 to S9 in the Supplemental Appendix.
p < .1. **p < .05. ***p < .01.
Mechanism Analysis
Healthcare Resources Directly Affect the Health Status of Immigrants
The findings of mechanisms of healthcare resources on employment quality presented in Table 9, suggest that the number of hospital beds has a significant positive effect on the health status of immigrants (Columns (3)–(4)), while the number of hospitals and physicians does not show a significant impact (Columns (1)–(2), Columns (5)–(6)). Healthcare resources play a role in promoting better health outcomes and higher quality employment opportunities among city residents. As such, policymakers and healthcare providers should prioritize increasing the availability of hospital beds and other relevant resources to improve the health status of populations, particularly migrants.
The Impact of Healthcare Resources on Health Status.

Note. 1. Observations for the self-reported health status are only available for 2017 and 2018, so data are estimated for two periods only.
2. All models include demographic variables, city control variables, province-fixed effects, year-fixed effects, and occupation-fixed effects. The weights were considered in all model estimations.
3. Robust standard errors in parentheses.
Detailed results are presented in Table S10 in the Supplemental Appendix.
p < .1. **p < .05. ***p < .01.
Healthcare Resources Affect Immigrants’ Propensity to Settle and Integrate
Promoting local integration among immigrants is crucial in enhancing their overall well-being and facilitating their economic and social success. Access to healthcare resources plays a significant role by providing essential medical care, enabling immigrants to view themselves as integral community members, and accessing basic public services. Moreover, increased healthcare resources enhance the attractiveness of a city, bolstering the health and safety of immigrant families and increasing their desire to settle permanently. Immigrants who are firmly integrated locally are less likely to return home. In contrast, immigrants are likelier to return home, leading to precarious employment (Gherghina et al., 2020). Once immigrants have decided to settle and integrate locally, there is little difference between them and the native residents. These immigrants are more inclined to enter long-term contracts for permanent employment (Z. Liu et al., 2019; Toruńczyk-Ruiz & Brunarska, 2018). We employ a binary variable of settling propensity (0 = no, 1 = yes) and local integration (progressively increasing integration from 1–4) as dependent variables.
Table 10 reports the effect of healthcare resources on settling propensity and integration. Columns (1) to (3) show the coefficients of the effect of the numbers of hospitals, hospital beds, and physicians on settling propensity. The LOGIT model was adopted. The number of hospital beds and physicians has significant positive effects on the intention to settle, while hospitals do not have a significant effect. Columns (4) to (6) show the LOGIT regression results. Hospitals, beds, and physicians significantly positively affect the local integration of immigrants at the 1% level. The presence of abundant healthcare resources in a city facilitates local integration.
The Impact of Healthcare Resources on Settling Propensity and Local Integration in 2017.

Note. 1. Observations for the integration are only available for 2017, so data are estimated for 2017.
2.All models include demographic variables, city control variables, province-fixed effects, year-fixed effects, and occupation-fixed effects. The weights were considered in all model estimations.
3.Robust standard errors in parentheses.
Detailed results are presented in Table S11 in the Supplemental Appendix.
p < .1. **p < .05. ***p < .01.
Discussion
The Mechanisms by Which City Healthcare Resources Affect the Quality of Employment
In both the baseline regression and the instrumental variables model, we validate the effect of cities’ healthcare resources on immigrants’ employment quality. The main pathways of influence are health status, the propensity to settle, and integration. The results of the mechanism analysis show that a city’s healthcare resources influence the health status of its residents, which is consistent with existing research (Bell et al., 2013). A healthy status increases the labor force’s income, productivity, and employment stability. Health as human capital affects employment through productivity, leisure preferences, life expectancy, unemployment benefits, health expenditure, and health insurance (Britton & French, 2020; Delattre et al., 2019).
First, health affects the productivity of the workforce. Employees in good health are more productive (Ullah & Malik, 2019). Higher productivity is associated with higher incomes and shorter working hours (Baharin et al., 2020; Bevan & Cooper, 2021). Employees in good health are likely to spend less time on medical appointments to increase their productivity. Employees in poor health have lower productivity, leading to lower incomes (Iseghohi, 2021). Lower incomes reduce the labor supply and employment stability. Second, health status affects employment participation rates. Poor health raises the marginal utility of leisure relative to work. Increasing an individual’s leisure time reduces the time available for work, which leads to withdrawal from the labor market and affects employment stability. Poor health lowers life expectancy, increases individuals’ thoughts of early retirement, and reduces the labor supply (Ilmakunnas & Ilmakunnas, 2018).
In contrast, healthy workers are more active in the labor market to improve the quality of employment. Finally, health affects migrants’ propensity to settle or stay permanently. Healthy migrants are more likely to stay or settle in the area and stabilize their employment (Huang et al., 2020). In contrast, migrants with poor health do not have equal access to healthcare resources due to various factors, including household registration restrictions, causing them to feel discriminated against and unequal and return to their hometown. City healthcare resources significantly increase the propensity to settle and facilitate the local integration of immigrants. A solid settling propensity and high social integration positively affect immigrants’ employment quality. Cities provide abundant healthcare resources and promote equalizing public services, effectively enhancing immigrants’ social integration and citizenship. In turn, they are willing to devote more time to planning a long-term career and finding long-term stable jobs to improve their family’s financial status. Furthermore, more socially integrated immigrants are generally more active in social activities and accumulate social capital. Immigrants with a vast social network have access to more labor market information, further enhancing the quality of employment.
The Importance of Accessibility to Healthcare Resources
Accessibility to healthcare resources determines their performance. The effect of healthcare resources on employment quality is influenced by accessibility. Immigrants with health training and medical files have a higher quality of employment than those without. Health training and medical files improve the ability of immigrants to access, understand and use information regarding health and health services. More excellent health knowledge and wider access facilitate immigrants’ use of a city’s healthcare resources. Increased access to healthcare resources strengthens the impact of healthcare resources on employment. The impact of healthcare resources on population migration is reflected in voting with one’s feet. People are more likely to settle in areas that best match their resource needs and preferences.
China has established the world’s most extensive public healthcare system, with a comprehensive four-tier health service network and a three-tier integrated primary healthcare network. Health resources for basic healthcare services include human resources and hardware facilities, such as community health service centers, county people’s hospitals, and maternal and child health centers. The government provides these services to guarantee people’s needs for basic healthcare services. The state is primarily responsible for basic healthcare input, and the people only pay a portion of the cost to access basic healthcare services with quality assurance. Basic healthcare resources are concentrated in cities, and newly arriving immigrants are unaware of the local healthcare and referral policies, resulting in low utilization of resources. Health training and health records accelerate the process of familiarizing immigrants with healthcare resources and strengthen the impact of healthcare resources on immigrants.
The Importance of Medical Insurance for Immigrants
The rand health insurance experiment (HIE) shows that different medical insurance schemes affect the demand for and use of health services. In this paper, immigration for urban medical insurance is more influenced by healthcare resources. Healthcare resources are mainly concentrated in cities, and the type of insurance is urban medical insurance. Urban medical insurance is reimbursed at a higher rate in a city’s healthcare system and is more advantageous for using healthcare resources. Due to financial constraints and the fact that they often do not have local urban medical insurance, many immigrants have relatively low affordability of healthcare services, resulting in low demand and underutilization of their healthcare services. Consolidating and harmonizing medical insurance have important implications for migrants’ access to local resources.
Conclusion
This empirical study aims to investigate the effects and mechanisms of city healthcare resources on the employment quality of immigrants using data from the 2016 to 2018 China Migrants Dynamic Survey (CMDS). Our findings suggest that city healthcare resources significantly positively affect immigrants’ work income, reduced working hours, and stable employment. Access and accessibility to healthcare resources are critical in influencing resource use. Urban medical insurance is more advantageous than rural medical insurance regarding the effect of healthcare resources. The study also shows that healthcare resources influence immigrants’ health status, propensity to settle, and integration, all directly affecting employment quality.
The present study adds to the existing literature on the impact of healthcare resources on the labor market, and our findings have significant implications for policymakers. Improving immigrants’ employment quality could be achieved by promoting equalization of healthcare services, strengthening immigrants’ awareness of health risk prevention, expanding medical insurance coverage, and increasing participation in basic urban medical insurance. The study highlights the need for policy details to connect rural medical insurance with urban medical insurance and achieve medical reimbursement in different places, given the mobility and job instability of immigrant workers in China.
However, there are some limitations to our study. Firstly, our analysis did not consider the equity of healthcare resources. The equitable allocation of healthcare resources does not necessarily imply absolute equity in healthcare resources in any local area, and the hierarchy of needs also needs to be considered. Secondly, the self-rated health status used as a proxy variable for health is subjective and may have influenced our results somewhat. Therefore, using objective health indicators in future studies may enhance the persuasiveness of the findings.
In conclusion, this study contributes to our understanding of the impact of healthcare resources on immigrants’ employment quality and provides valuable insights for policymakers. Further research is needed to address the present study’s limitations and examine the impact of healthcare resources on different groups of immigrants with varying needs and characteristics.
Supplemental Material
sj-docx-1-sgo-10.1177_21582440241268520 – Supplemental material for The Impact of a City’s Healthcare Resources on Immigrants’ Employment Quality
Supplemental material, sj-docx-1-sgo-10.1177_21582440241268520 for The Impact of a City’s Healthcare Resources on Immigrants’ Employment Quality by Ping Li, Ziqi Wang and Liting Zhao in SAGE Open
Footnotes
Authors’ Contributions
P.L. contributed to the data source and designed the methodology, provided modification ideas. Z.W. made major and minor revisions to address all the suggested changes, empirical analysis, modify the manuscript. L.Z. analyzed the data, wrote the manuscript. All authors have seen the manuscript and approved to submit to your journal.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: National Office for Philosophy and Social Sciences. Grant ID: 21BJY094.
Ethical Approval and Consent to Participate
All procedures of this research were conducted in accordance with the 1964 Declaration of Helsinki and its later amendments or comparable ethical standards. South China Normal University Academic Committee has proved the study protocols. Approved Number: SCNU-SEM-2021-005. This is a secondary data analysis. The data from China Migrants Dynamic Survey (CMDS) are provided by Chinese National Health Commission Department. No human being and animals were involved. The secondary data used was de-identified data. The dataset has been stripped of all identifying information and there is no way that it could be linked back to the subjects from whom it was originally collected.
Consent for Publication
All authors read and approved the final manuscript.
Data Availability Statement
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.