
Abstract
This article examines the relationships between workers’ control over their working time and their well-being, looking at how these relationships differ across a set of health care occupations that are stratified by class, gender, and race (physicians, nurses, emergency medical technicians [EMTs], and certified nursing assistants [CNAs]). Across occupations, workers’ ability to control their schedules decreases their job-related stress. The results show that different dimensions of worktime control (WTC) affect workers in different occupations in distinctive ways, offering a corrective to prior work that combines workers who occupy different locations in the system of social stratification. Among nursing assistants—the most socially marginalized group in the study—the relationships between particular aspects of WTC and job stress were distinct from those associations among the other three occupations, reinforcing the importance of examining these relationships in occupationally specific contexts. This kind of comparative perspective illuminates the ways distributions of intangible resources such as WTC both emerge from and reinforce existing patterns of social stratification. The implications of these differences for research and policy are discussed.
Introduction
In the wake of the “Great Recession,” employers’ attempts to cut labor costs have often involved controlling workers’ time. Wal-Mart’s automated system alerts managers when workers approach 40 hours, so those managers can send workers home before they would qualify for either full-time benefits or overtime (Negrey, 2012). At the same time, more and more workers are classified as “exempt” from overtime pay and are pushed to work longer hours without additional compensation (Negrey, 2012). As the American economy becomes increasingly bifurcated into these two kinds of employment, an ever-growing proportion of workers face diminishing control over their work time. This loss of control is of particular concern because control over one’s working environment is associated with both physical and mental health—critical elements of well-functioning economies and societies (Marmot, Bosma, Hemingway, Brunner, & Stansfeld, 1997).
Controlling work hours has long been a point of contention between workers and employers. Economic conditions since the beginning of the “Great Recession” have only made disputes over work time more intense. Although both those who struggle to find sufficient hours and those who contend with long hours and overwork feel economically trapped and socially coerced, the nature of these disputes vary across a segmented labor force (Glenn, 2002; Jacobs & Gerson, 2004; Negrey, 2012; Uttal & Tuominen, 1999). It is these differences in the ways differently situated workers are impacted by different kinds of struggles for worktime control (WTC) that are the focus of this article. I investigate how the lives of workers in a stratified labor market are differently affected by varying distributions and kinds of control over their work time. The simultaneous examination of the effects of different kinds of control on different kinds of workers will contribute to our understanding of how processes related to WTC are implicated in maintaining social inequality.
This study is grounded by Joan Acker’s concept of inequality regimes. Acker (2009) holds that persistent inequalities are created, maintained, and reproduced through “the everyday practices of organization participants” (p. 213). The workers in this study are all from the health care industry, working under conditions of unpredictable demands in a 24-hr cycle of care, where navigating control over working time is a central “everyday practice.” Drawing upon Acker, the driving question underlying this article is as follows: In what ways is the availability and distribution of WTC implicated in the processes of stratification? More concretely, this study was guided by three research questions:
I expect that worker control over work time is an important predictor of worker distress across occupations, net the total number of hours worked. Furthermore, I argue that the character of this relationship between WTC and distress varies across these occupations in ways that reflect the gender, class, and race systems that shape these occupations. Because control over work time, like other social resources, is distributed based on systems of social stratification, its consequences for worker health and well-being arguably perpetuate this societal stratification. The distribution of these material consequences can impact workers’ lives in a way that shapes their paths in the labor market and their life courses, more broadly.
Background: Stratification Within the U.S. Health Care Industry
In the United States, the health care industry provides a particularly appropriate setting in which to study variations in control over work time. It is an industry known for its 24/7 schedule and thus the continuous temporal demands it places on its workers. The industry is also rapidly growing, both in workers and in cost. It was one of the largest industry sectors in 2013, providing more than 15.8 million jobs (Henderson, 2012; Torpey, 2014). Furthermore, the health care and social services sector is projected to have both the largest and the fastest growth between 2012 and 2022, with more than 4 million new jobs expected during that time (Torpey, 2014). Health care spending is projected to comprise more than 25% of the total federal budget in fiscal year 2015 (National Priorities Project, 2015). With this kind of growth, and due to widespread publicity over the recently enacted health care law (the Affordable Care Act), the health care industry is under increasing budgetary scrutiny. This scrutiny, in turn, puts pressure on health care–providing organizations to lower costs—among which worker pay features prominently. Importantly, in addition to being increasingly dominant forces in the landscape of work, these organizations in the health care industry are also places of visible segmentation by gender, race, and class, making them crucial sites for studying the processes that maintain inequality.
This study focuses on four occupations within this industry: physicians, nurses, emergency medical technicians (EMTs), and certified nursing assistants (CNAs)—jobs that are highly stratified by gender, class, and race (Glazer, 1991; Glenn, 1992; Hine, 1989; Scherzer, 2003). Nationally, almost all registered nurses and CNAs are women (about 90% of each), while women make up 36% of physicians and surgeons and 39% of EMTs (Bureau of Labor Statistics, 2013a). The annual median wage nationally for family- and general-practice physicians (who are among the lower paid physicians) was US$176,530 in 2012, more than 2.5 times that of registered nurses (US$66,220), more than 5 times that of EMTs (US$31,270), and 7 times the annual median wage for CNAs (US$24,890; Bureau of Labor Statistics, 2013b). In our data, more than 30% of nurses and EMTs have bachelor’s degrees, compared with fewer than 4% of CNAs. Moreover, all physicians have master’s degrees plus additional graduate-level education, the minimum required by the American Medical Association to practice (American Medical Association, 2012). Thus, in their gender, education, and income profiles, these occupations are quite distinct.
CNAs are particularly distinct from the other three occupations. In addition to being predominantly female and having the lowest incomes and educations, CNAs are the only occupation of the four that is not majority White. Whites make up fewer than half of these workers, nationally, and African Americans about 36%. By contrast, 83% of EMTs are White. Nurses and physicians fall in between with 75% and 68% of these occupations, respectively, represented by Whites (Bureau of Labor Statistics, 2013a). Of the 25% racial minority representation among nurses, African Americans make up about half, whereas among physicians the predominant minority race is Asian (Bureau of Labor Statistics, 2013a). In health care, as in other industries, people of color (especially African Americans and Latina/os) are disproportionately represented in the lowest paid jobs (Slack & Jensen, 2011).
The distinct social locations of these occupations within the same industry—and in some cases, within the same organizations—provide a unique opportunity for comparison. The literature about work time suggests that the same societal hierarchies that divide these occupations are also manifested in distinct patterns of work hours and schedules for each of these groups of workers (Clawson & Gerstel, 2014; Clawson, Gerstel, & Crocker, 2008; Jacobs & Gerson, 2004; Negrey, 2012; Presser, 2003). All of these occupations present useful comparisons with one another. CNAs are in a particularly disadvantaged position compared with the other occupations in facing race, class, and gender marginalization, and thus we expect this group might have a unique pattern in the relationship between WTC and worker outcomes.
Using this comparative lens across occupations, this study extends the current literature by looking specifically at how access to control over work hours and schedules impacts differently-situated workers, net the total hours themselves. It also explores the implications for workers of this differential access to WTC—both as a reflection of worker power and as a mechanism reinforcing the processes that maintain occupational stratification.
Literature Review
Control Over Work Time
Control over the conditions of work has long been associated with worker stress and distress outcomes. Theories generally hold that greater control over one’s job reduces worker stress (Collins, Karasek, & Costas, 2005; Hausser, Mojzisch, Niesel, & Schulz-Hardt, 2010; Marmot et al., 1997; Steptoe & Willemsen, 2004). Control over the time one spends working is integral to a sense of control at work and, over the past decade, scholars have begun to separate out, theoretically, workers’ control over working time from control over other work conditions. Employee control over work time or WTC gauges the discretion individual workers feel in determining the amount and scheduling of their working time (Beckers, Kompier, Kecklund, & Härmä, 2012; Berg, Appelbaum, Bailey, & Kalleberg, 2004; Härmä, Kompier, & Vahtera, 2006; Moen, Kelly, & Huang, 2008). Aspects of WTC include control over starting and ending times, break times, vacation or time off, distribution of workdays over the week, quantity of hours, and whether and when to work overtime (Geurts, Beckers, Taris, Kompier, & Smulders, 2008; Moen et al., 2008; Nijp, Beckers, Geurts, Tucker, & Kompier, 2012).
Several long-standing theories tie WTC to worker well-being. Effort-recovery theory suggests that WTC enables workers to balance effort with recovery, whether through the control of break times while at work or recuperation through control of time spent away from work (Meijman & Mulder, 1998). Looking at WTC as a subdimension of general autonomy, self-determination theory (Deci & Ryan, 1985), the job characteristic model (Hackman & Oldham, 1976), and the demands-control model (Karasek, 1979; Karasek & Theorell, 1991), all suggest that increased WTC may stimulate worker motivation, improve health and performance, and prevent stress. These effects of greater WTC are proposed to derive from at least two processes: utilization, where workers actually change their working time, or through perception, where the opportunity to self-determine work hours helps workers, regardless of an actual change in amount of working time (Beckers et al., 2012). Finally, theories of work–home interaction suggest that greater WTC might improve work/nonwork balance (and thus prevent stress) through workers’ ability to adjust working time to meet the needs and obligations of their nonwork lives (Beckers et al., 2012; Geurts et al., 2008; Geurts & Demerouti, 2003).
A broad literature in fields ranging from applied ergonomics to management to public health and sociology offers evidence to support these theories, suggesting a positive relationship between workers’ control over the timing and length of their work hours and their well-being. Outcomes related to increased WTC include reduced physical and psychological distress (Costa, Sartori, & Åkerstedt, 2006; de Jonge, Vegchel, Shimazu, Schaufeli, & Dormann, 2010; D’Souza, Strazdins, Lim, Broom, & Rodgers, 2003; Takahashi et al., 2011), reduced sense of work–family conflict (Fenwick & Tausig, 2004; Geurts et al., 2008; Golden, Wiens-Tuers, Lambert, & Henly, 2011; Hughes & Parkes, 2007; Moen et al., 2008), a greater feeling of income adequacy (Moen et al., 2008), increased job commitment (Halpern, 2005), and reduced rates of sickness-related absence from work (Ala-Mursula et al., 2006; Ala-Mursula, Vahtera, Linna, Pentti, & Kivimäki, 2005).
Despite the myriad ways WTC seems to benefit workers, a recent systematic review of the literature suggests that there are still important gaps in our understanding of the relationship between WTC and worker well-being (Nijp et al., 2012). Indeed, a recent study of hospital employees across European countries found no effect of worktime autonomy on workers’ health (Pisljar, van der Lippe, & den Dulk, 2011). Recent reviews suggest that prior research did not specify the particular subdimensions of WTC and worker well-being nor did it consider the differential benefits to workers in different social positions (Hausser et al., 2010; Nijp et al., 2012). These reviews suggest that teasing apart the different aspects of control over work time would further our attempts to understand the buffering effects of WTC on worker well-being. This study begins to fill this gap in the literature by looking at the effects of different aspects of WTC on workers in different occupations.
Occupational Differences in Worktime Experiences
The effects of various aspects of WTC on well-being likely depend on workers’ different social positions (Nijp et al., 2012). In particular, the social stratification of power across occupations means schedule control is likely more available to workers in some jobs than others (Negrey, 2012). Recently, cross-country comparative studies have begun to explore the impacts of social and institutional context on the relationship between WTC and worker well-being (Berg et al., 2004; Lyness, Gornick, Stone, & Grotto, 2012; Pisljar et al., 2011), but comparison across social contexts within a society is still rare. When they are taken into account, these intrasocietal social contexts, such as occupation, are often added to a model as control variables, rather than a lens through which to look at the relationship between WTC and worker well-being outcomes (see, for example, Pisljar et al., 2011). In one exception the buffering effects of worker job control (including WTC) on worker well-being were examined across different occupational sectors in the Netherlands (de Jonge, Dollard, Dormann, Le Blanc, & Houtman, 2000). They found that the interactive relationship between job demands and job control depended on the occupational sector, suggesting that looking at occupational context might improve our understanding of specific WTC–worker well-being relationships.
Few studies explicitly compare the effects of WTC across occupational contexts differentiated by gender, class, and race. However, some studies do compare the relationship between WTC and worker well-being at an individual level—across individuals with different positions in these social systems. For example, Takahashi et al. (2011) find that most of the effects of WTC (control over daily working hours and days off) on well-being outcomes were the same regardless of an individual’s gender. In the exception, insomnia symptoms decreased with control over daily working hours for men, but not for women. Lyness et al. (2012) find that lack of control over work hours has greater negative consequences for women than for men. However, their analysis of the relationship between schedule control and a particular set of worker consequences (work–family conflict, job satisfaction, and organizational commitment) suggests that this relationship might not vary by workers’ social class (Lyness et al., 2012). Nevertheless, low-wage or lower class workers tend to have less schedule control than workers in higher social class positions, both in the United States and cross-nationally (Clawson & Gerstel, 2014; Lambert, 2008; Lyness et al., 2012; Watson & Swanberg, 2011).
Looking at gender and class at an occupational level rather than an individual level is practically and analytically important because those compositions shape organizational policies as well as the practices and responses of both employers and employees (Acker, 2006; Lorber, 2005; Ridgeway, 2011; Wright, 2008). Systems of class, gender, and race do not simply serve as characteristics of individuals but also as operating principles that shape the social ecologies of occupations. Thus, rather than examining either a heterogeneous collection of individuals scattered across a range of occupations or comparing men and women in the same occupation, this study’s design takes as its central point of comparison occupations that are segregated by race, gender, and class.
According to both theory and empirical research, not only is the class location of an occupation associated with varied work conditions, but an occupation where workers are predominantly women tends to have a mode of operation that differs from an overwhelmingly male occupation and differs as well from one that is closer to gender balanced; so, too, an occupation that is racially segregated differs from one that is racially balanced or integrated (Acker, 2006; Glenn, 2009, 2010; Lorber, 2005; Ridgeway, 2011; Ridgeway & Fisk, 2012). This study’s design maximizes the ability to explore differences in workers’ experiences across these occupational ecologies, thereby extending the models that are currently used to understand the relationship between WTC and worker well-being.
This occupational perspective also reflects a focus on the organizational processes shaping workers’ lives. These processes sort jobs into types according to class, gender, and race through everyday management practices that racialize and sexualize definitions of “good” job performance and “skill” (Acker, 2006). Such definitions are then used to justify pay and other job characteristics, such as level of worker control or autonomy (Acker, 2006). Thus, the activities associated with each occupation are bound up with larger social and organizational processes and we look at occupations as ecologies shaped by these processes instead of controlling for job characteristics individually. In other words, by comparing experiences across occupations, rather than individuals, this project focuses on the consequences of these sorting and tracking processes, specifically those related to control over work time.
Health Care Occupations and WTC
This article looks specifically at health care occupations that vary in their gender, class, and racial composition. Health care occupations are similar in that they generally require the physical presence of the worker, which presents a set of unique scheduling demands. However, even among these occupations that require a physical presence, challenges to schedule control differ due to the gendered expectations of the workers, the resources available to workers in different occupations, and the power balance between workers and employers. Comparing occupations in health care can help us understand how workers in different social contexts and locations are affected by WTC.
Gendered expectations of workers can compound differences in material resources among workers and these can translate into different scheduling needs. For example, predominantly male physicians are often able to enact a “breadwinner” paradigm. As salaried workers, they struggle against the constant pressure to work more hours (Jacobs & Gerson, 2004), but they earn high enough wages that they can either pay someone else to take care of their obligations outside of work—such as child care or cleaning—or have spouses who can manage the household because they often do not work for wages or work part-time.
However, predominantly female nurses, despite earning moderate wages and being employed full-time, face gendered expectations to manage their children and household life in addition to working for pay. Because their spouses also typically work full-time, nurses often balance the cost of services and the negotiation of work schedules so that they can take care of home and care obligations themselves. CNAs—who are low-wage, predominantly female, and often women of color—frequently cannot afford to pay someone to take care of their obligations outside of work and also cannot afford the loss of wages that would come with cutting down on work time to take care of those obligations themselves. They are often forced to choose between handling family emergencies—such as picking up a sick child from school—and losing wages or possibly their job. In these ways and others, gender and class forces interact to create not only different levels of schedule control but also different needs for control among different health care workers (Gerstel & Clawson, 2014).
In addition to being caught between the imperatives of family and wages, low-wage care workers, such as CNAs, also continue to have the least access to policies that would give them greater control over their schedules (Bond & Galinsky, 2006; Clawson & Gerstel, 2014; Lambert & Henly, 2009). This lack of access to schedule control is of particular concern for these workers who already have less control over other aspects of their jobs. As well as being paid less, nursing assistants are often marginalized by gendered and racialized occupational segregation into the “dirty work”—bearing the primary responsibility for the “dirtiest” and most physically challenging aspects of caregiving such as bathing, dressing, feeding, and changing briefs and bedpans (Duffy, 2007; Glenn, 1992). Nurses’ work, by contrast, typically involves more managerial and less hands-on work: developing and managing nursing care plans, controlling and delivering medicine, and assisting physicians during treatments and exams. With their physically demanding work, nursing assistants have some of the highest nonfatal injuries and illness rates for all U.S. occupations, the fourth highest in 2012 (Bureau of Labor Statistics, 2013c). These factors all suggest that the relationship between WTC and well-being for CNAs might be unique among the four occupations.
Worker Characteristics Affecting WTC
This study grounds itself in the perspective that workers’ needs for schedule control will differ across occupations that are divided in their gender and class compositions. We suggest that occupations themselves are systems sufficiently stratified by gender, race, and class that workers’ experiences across these occupations will reflect these dominant social divisions, thus obviating the need to measure these as individual worker characteristics. However, the literature also suggests accounting for other worker characteristics that affect access to WTC. A worker’s age and marital and family status are often associated with use of “flexible” worktime policies. Younger workers seem to use flexible scheduling more than older workers (Allen, Herst, Bruck, & Sutton, 2000; Tausig & Fenwick, 2001). Unmarried workers tend to have less control over the timing of their work than married workers, but the causal direction of this relationship is unclear because the effect seems largely attributable to the higher schedule control found among workers with young children at home (especially women with preschool–aged children; Golden, 2001, 2008; Presser, 1989; Sharpe, Hermsen, & Billings, 2002). Single parenthood, as might be expected, leads to much greater competition between work time and family time than partnered parenthood (Kendig & Bianchi, 2008).
Beyond partnership and parental status, some other working conditions seem likely to affect workers’ access to schedule control and the consequences of such control on worker well-being. Unionized workers may have greater access to schedule control because they are likely to have better information about policies regulating such control than nonunionized workers (Budd & Mumford, 2006). Workers whose hours include weekend work may have more stress associated with lack of WTC because weekend hours have been found to be particularly stressful for workers in general (Clawson & Gerstel, 2014). Finally, workers whose paid work hours come from more than one job (more than 60% of the EMTs in this study) might be expected to have a different relationship between WTC and well-being. We account for each of these factors in our analysis.
Research Agenda
As this review argues, an emerging wave of research has focused on the effects that worker control over working hours has on worker quality of life, but this research is just beginning to look comparatively across intrasocietal occupational contexts and to tease apart the effects of particular subdimensions of WTC. The present study contributes a unique perspective to this emerging body of comparative work by looking within the same country and industry at differences in worker experiences across occupational locations that are marked by gender and class stratification. Furthermore, this study differentiates several dimensions of WTC, uniquely creating an opportunity to examine how workers in specific social locations have both different needs and differential access to particular manifestations of WTC.
Method
Data
The data for this project come from a mail survey of CNAs, nurses, physicians, and EMTs conducted in 2004 (for methodological discussion, see Clawson & Gerstel, 2014; Gerstel, Clawson, & Huyser, 2007). Since the survey was conducted, time and money pressure on the health care industry and on workers have only become more intense, and thus the findings from these data likely represent a conservative estimate of the relationships we explore. The sample was drawn from Massachusetts, chosen to be demographically representative of the national population but also within easy driving distance of the investigators’ location (for the interview portion of the larger project of which this survey is a part). Because the state requires workers in these occupations to register to maintain legal certification, the sample frame was a current list of all those legally certified for each occupation, allowing the selection of a true random sample. Three waves of the survey were sent out. Of the 800 surveys, only 9.6% were returned as not having accurate addresses, indicating that the lists were current and well maintained. Of the delivered surveys, the overall response rate was an excellent 64.5% (464 out of 719); for every group, the response rate was greater than 50%; for CNAs, it was 53.9% (n = 89), for physicians 57.6% (n = 102), for EMTs 64.7% (n = 119), and for nurses 78.2% (n = 154).
Descriptive statistics are in Table 1. In their income, education, and gender, participants’ characteristics generally reflected the national populations of these workers. Racially, a higher proportion of all the occupations among the survey participants were White than nationally, but this is representative of the New England region. EMTs in this sample also had slightly higher annual incomes than nationally. This may be due to the high rate of second-job holding among EMTs, for whom we report total income from all jobs.
Descriptive Statistics (N = 420).

Note. EMTs = emergency medical technicians; CNAs = certified nursing assistants.
Having a second job meant significantly higher total work hours among CNAs and EMTs, but not for physicians and nurses. CNAs who had second jobs worked an average of 19 hr more per week than those who did not. EMTs with second jobs worked an average of 14 hr more per week than those without. CNAs with second jobs averaged 35 hr per week at their main jobs and 23 hr per week at their second jobs. EMTs with second jobs averaged 43 hr per week at their main jobs and 18 hr per week at their second jobs.
As discussed, this study uses occupations as the lens of comparison, treating them as organizational ecologies, shaped by the gender, class, and race of the workers who predominate in that occupation. To illustrate this stratification to the reader, indicators of gender, race, and income are included in the descriptive statistics. However, because of the study’s design, the regression models do not contain indicators of individual respondents’ class, gender, or race status. Instead, models were run either within each occupation or including an occupation variable as indicator of a particular social location.
Dependent Variable: Worker Job-Related Stress
Following the WTC literature, reduced job stress is used to indicate increased worker well-being. Job stress was operationalized as the response to the statement, “My job really wears me out.” Responses were captured on a 5-point Likert-type scale (from strongly disagree to strongly agree).
Independent Variables
WTC variables
Control over work time
Informed by the major theories tying WTC to worker well-being, four survey items measure different subdimensions of the central explanatory concept: perceived control over work time. The first three measures are responses to various statements about work hours and schedules. On the survey, the following instructions introduced these items: Some people can choose their work hours and schedules and some can’t. Please rate the following statements on the following scale from Strongly Agree to Strongly Disagree based on your main job as a [occupation].
To measure workers’ perceived ability to alter their work schedules, the analysis includes responses to the statement, “I can change my schedule when I need to, even on short notice.” A second item measures workers’ ability to adjust working time to meet the needs and obligations of their nonwork lives, using responses to “I can always work extra hours when I want to,” which touches on both time and monetary needs. To measure workers’ sense of their ability to self-determine their schedules, responses to “My supervisor pressures me to work additional hours” are included. Each of these measures is coded such that higher numbers indicate increased agreement with the statement, so a higher number on the “I can change my schedule” variable indicates greater control, whereas a higher number on the “my supervisor pressures me” indicates less control. These items were standardized (M = 0, SD = 1) for easier comparison.
To measure control over the amount of time spent away from work (a dimension of WTC associated with Effort-Recovery theory) and ability to balance work/ nonwork time, a fourth measure compares workers’ preferred quantity of hours with their actual reported work hours. This concept is sometimes called “hours mismatch” (Golden, 1996; Reynolds, 2003). Unlike the other three measures of WTC, which asked somewhat explicitly for workers’ perceptions of their own control over their work hours and schedules, this variable attempts to capture workers’ control over the quantity of hours they work in a more implicit way, based on the differences between their realities and their preferences. The variable was constructed by combining two separate self-reports of work hours. First, respondents reported the number of hours of paid employment they would prefer to work each week. Several pages later, they reported the number of hours they worked last week (or usually). Using these two responses, we constructed a dichotomous dummy variable to differentiate those respondents who want to work fewer hours than they currently work (coded 1) from those who want to work the same or more hours than they currently work (coded 0).
Each of these items captures different manifestations of WTC, which may have different relationships to distress. Factor analysis confirmed that these items tapped different concepts, as they did not form a single scale. Thus, each is included in the model individually.
Worktime variables
Total work hours
This measures self-reported total hours worked either in the previous week or in a typical week (including second jobs).
Number of weekends worked
This measures number of weekends worked in the past month to capture the timing of work. .
Demographic variables
The analysis includes items measuring respondents’ age, union status, whether or not the respondent has a second job, and their partnership and parental status. Based on previous research indicating the intertwined effects of partnership and parental status, I have combined these two factors into a single measure with four values. Thus, single parents of young children (<6 years old) are compared with married or partnered parents of young children, married or partnered individuals who do not have young children, and single individuals who do not have young children.
Interaction variables
Interaction terms
To examine the different relationships between WTC and worker stress in different occupations, I created a set of multiplicative interaction terms, crossing each of the four occupations with each of the four main time control variables.
Statistical Methods
The baseline model for each occupation predicts worker job stress based on weekly work hours, controlling for some worker personal characteristics (Table2). This allows for an evaluation of the main effects of work hours on worker job stress. To this model for each occupation, I added WTC variables to evaluate their effects on job stress and on the main effect of work hours.
In addition, I ran an interactive model for each of the subdimensions of WTC (Table 3). These models include all four occupations, with dummy variables for each occupation and interaction variables between each occupation and each WTC variable, to allow me to explore the differentiated effects of WTC on worker stress for different occupations. In this kind of multiplicative interaction analysis, an “omitted” or base category forms the basis for comparison (CNAs in Models 9-11 and physicians in Model 12). Thus, the coefficient for the WTC variable that is included in the interaction term (e.g., supervisor pressure in Model 9) reflects the effect of this variable on job stress only for the base occupation (e.g., in Model 9, the coefficient of 0.227 reflects the relationship between supervisor pressure and job stress only among CNAs). The coefficients for the interaction terms (e.g., “Supervisor pressure × EMT”) reflect the difference in coefficient between the base occupation and the occupation in the interaction term. A positive and significant interaction term indicates a significantly stronger relationship between that WTC variable and job stress for the occupation in that interaction term than for the base occupation (e.g., in Model 9, nurses have a significantly stronger relationship between supervisor pressure and job stress than do CNAs).
Worker job stress is an ordered categorical variable without a fixed distance between categories. Thus, following Long (2004), I used ordinal logistic regression, the recommended model for this kind of variable (similar results were found when the models were run as ordinary least squares [OLS] regressions). To maintain sample size and statistical power, I used multiple imputation (via chained equations; the ICE command in Stata 12) to impute values for those that were missing on several variables. To confirm that ordinal logistic regression would be appropriate for the dependent variable, I verified that the data do not violate the proportional odds assumption using a likelihood ratio test (omodel in Stata), which was nonsignificant (Institute for Digital Research and Education, n.d.).
Results
These results show that WTC does have a significant impact on worker well-being. Importantly, the findings also show that different dimensions of WTC affect the four occupations in distinctive ways, offering a corrective to prior work that does not distinguish between workers who occupy different locations in the system of social stratification.
Two WTC measures significantly affected all groups except the CNAs: Feeling supervisor pressure to work more hours significantly increased stress, whereas workers’ perceived ability to change their work schedules significantly decreased stress among physicians, nurses, and EMTs (Table 2). Some dimensions, however, affected only one occupational group: Wanting to work fewer hours significantly increased job-related stress only among CNAs, whereas feeling able to “always” work extra hours significantly increased job-related stress only among physicians. When tested with an interaction model, this variation by occupation was statistically significant only in the cases of the relationships between work-related stress and either supervisor pressure or wanting fewer hours (see next section).
Ordinal Logistic Regression Predicting Increased Job Wear-Out (N = 420).

Note. CNAs = certified nursing assistants; EMTs = emergency medical technicians.
p< .10. *p< .05. **p< .01. ***p< .001.
In the base model without WTC variables, partnership and parental status was significantly associated with job stress among CNAs and physicians. For CNAs, being a single parent of young children was associated with the most job stress of any of the partnership/parental status combinations. CNA single parents’ level of job stress was significantly higher than that of CNAs who were single and had no children or had older children. Among physicians, those who were married or partnered with young children reported significantly less job stress than single physicians with either no children or older children. Interestingly, when WTC variables are added to the model, the significant effect of partnership and parental status disappears for CNAs but intensifies for physicians.
Occupation-Specific Relationships
The two significant results in Table 3 (Models 9 and 10) reveal the unique circumstances of CNAs. One shows no relationship for CNAs between one aspect of WTC (supervisor pressure) and job stress where the other occupations did, and another result shows a significant relationship for CNAs between job stress and a different aspect of WTC (hours mismatch) where other occupations did not. Table 3 contains four models with interaction terms—one for each WTC variable. Only the first two (Models 9 and 10) show statistically significant differences between occupations in the WTC–job stress relationship.
Ordinal Logistic Regression Predicting Increased Job Wear-Out With Occupation × WTC Interactions (N = 420).

Note. CNA = certified nursing assistant; EMT = emergency medical technician.
p< .10. *p< .05. **p< .01. ***p< .001.
Supervisor pressure (Model 9)
CNAs are the only occupational group for whom there is not a significant relationship between increasing supervisor pressure to work more hours and job stress (Table 2, Model 2; Table 3, Model 9). The positive and significant interaction term for nurses in Model 9 indicates that, for them, supervisor pressure has a significantly stronger relationship to job stress than for CNAs. Figure 1 illustrates these different relationships using predicted probabilities of a worker agreeing that their job causes them stress for varying levels of supervisor pressure. As supervisor pressure to work more hours increases, so does the probability of workers agreeing that their job wears them out for all occupations except for CNAs. The difference between CNAs and the other occupations in the relationship between supervisor pressure and job stress can be seen in the relative flatness of the slope of the CNA line compared with those of the three other occupations.
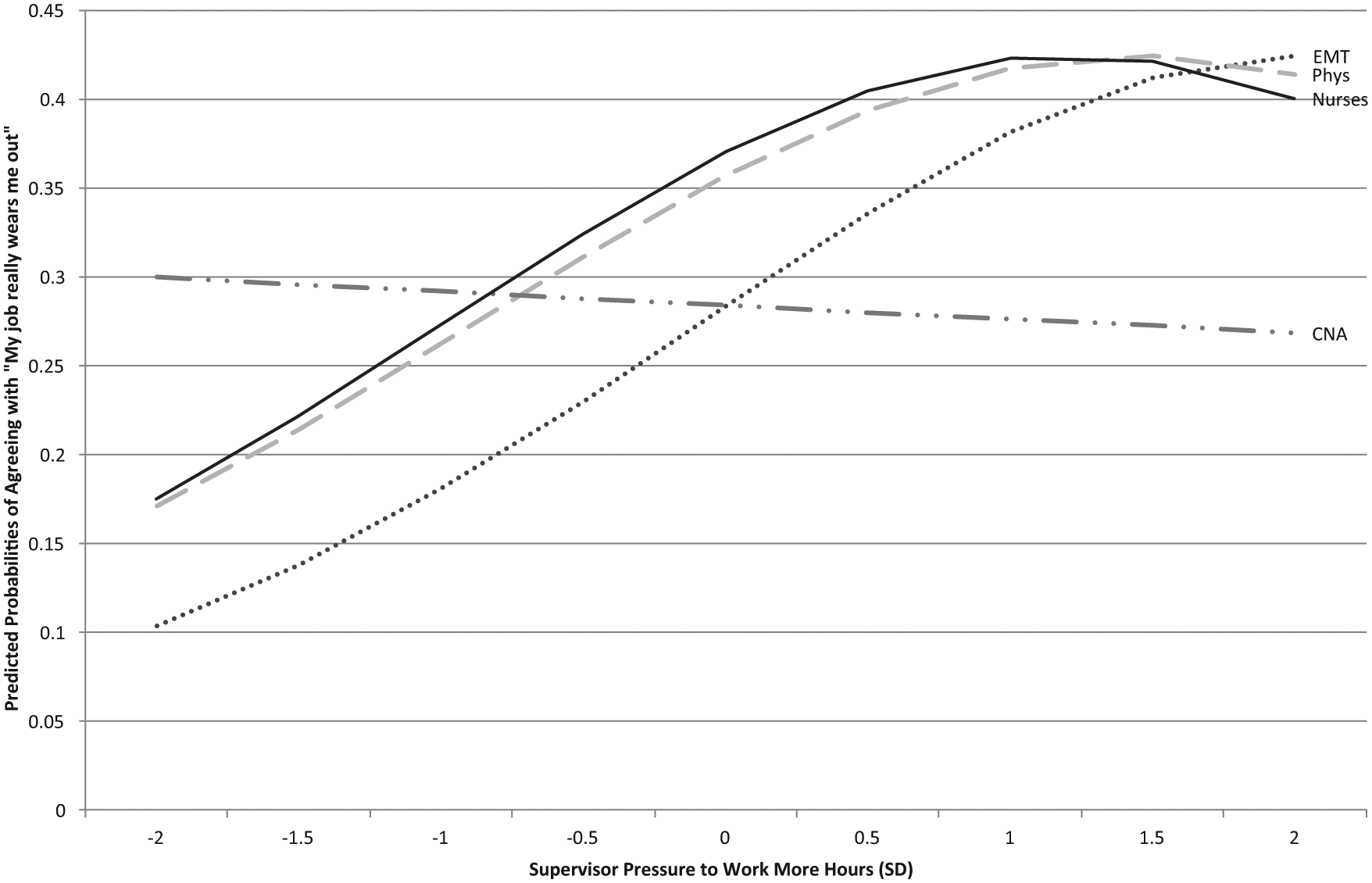
Worker job stress by supervisor pressure to work more hours (moderated by occupation).
Worker expectations for autonomy might be one possible explanation for this finding. This variable captured workers’ perceived ability to self-determine their schedules. As the least powerful occupation out of the four studied, CNAs may have lower expectations than the other three occupations for their level of discretion at their workplace and thus not experience greater stress when pressured by a supervisor. Alternatively, the chronic underemployment of CNAs—who are often seeking additional hours to have the income to pay their bills—might make supervisor pressure to work more hours a lesser source of job stress than, say, supervisor pressure to cut hours (Kahn, 2006).
Hours mismatch (Model 10)
Among CNAs, there was a uniquely significant relationship between wanting to work fewer hours and job stress, different from all the other three occupations. CNAs who want to work fewer hours than they currently work reported significantly more job stress than those CNAs who wanted the same or more hours than they were working. This association was small and nonsignificant for the other three occupations (Table 2). The negative and significant interaction terms in Model 10 (Table 3) show that the relationship between wanting fewer hours and increased job stress was significantly weaker among the other three occupations than for CNAs. Figure 2 presents a visual illustration of these differences. The line marking the drop in stress between workers who want to work fewer hours and those who want the same or more hours is markedly steeper for CNAs than for any of the other occupations.
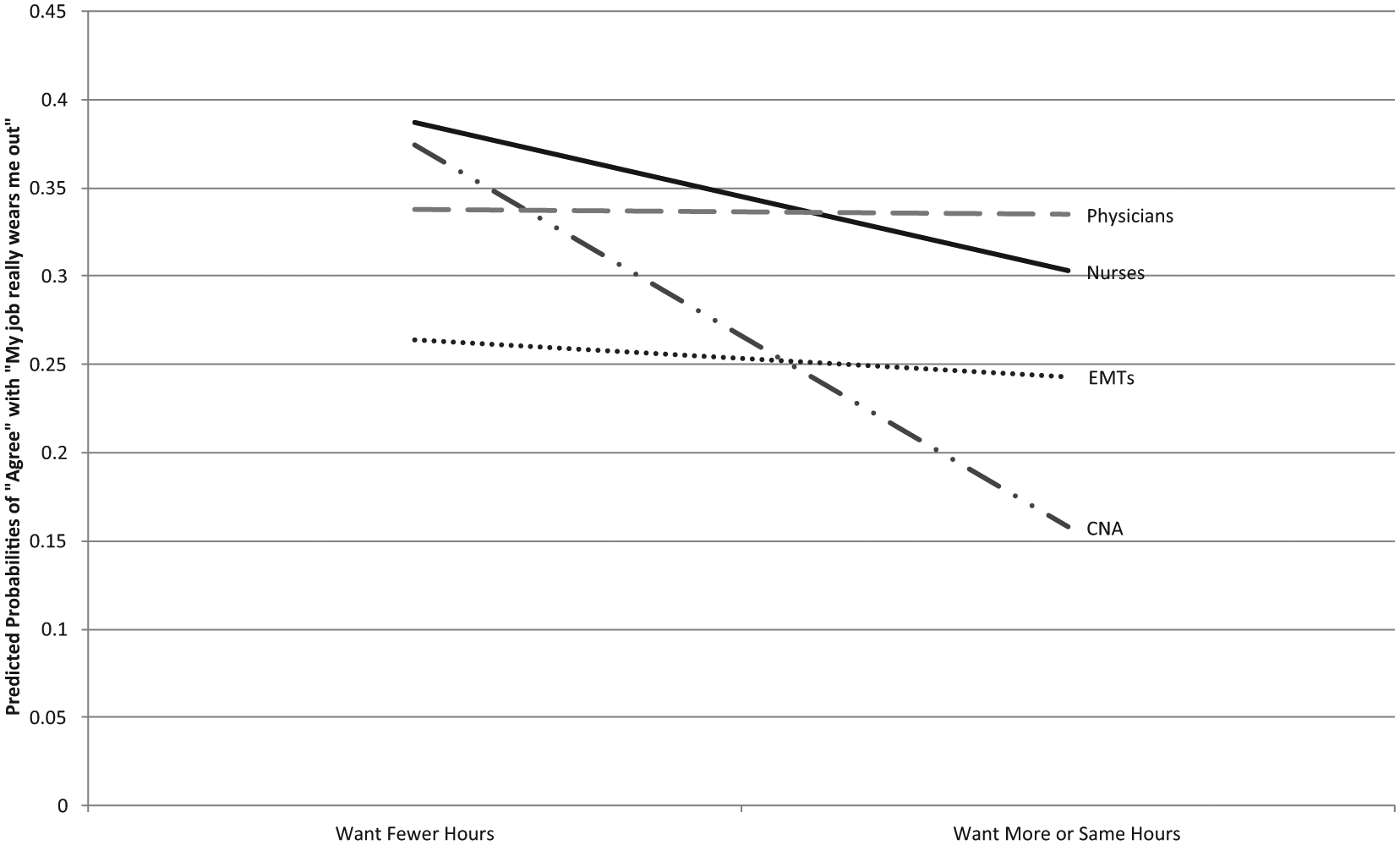
Worker job stress by hours preference (moderated by occupation).
Hours mismatch captures an aspect of WTC related to workers’ ability to recover from work through time away from work and their ability to balance work and nonwork obligations—related to both time and money. Workers across class social locations report hours mismatches in the literature, but higher status and lower status workers tend to lack control over this aspect of scheduling in opposite ways. Middle- and upper-class workers tend to report excessive hours whereas lower-class workers tend to report deficient hours (Lyness et al., 2012). Thus, for higher wage workers, a sense of control is often more closely tied to being able to limit one’s hours, whereas for lower wage workers, a sense of control might emerge instead from being able to acquire enough hours to meet financial needs.
The unique salience of hours mismatches for CNAs may be due to their unique position of marginalization compared with the other occupations. Physicians and EMTs who want to cut back on their hours might be buffered from the stress of overwork by other mechanisms, such as the satisfaction of fitting in with the social norm of breadwinning. Nurses—who face similarly gendered time demands as CNAs—may also have greater material resources (because of their own wages and those of their partners) with which to deal with excessive work hours. Although more research is needed to investigate this unique relationship among CNAs, the findings here suggest that these workers’ exceptionally draining work experience results from a combination of an inability to cut back on hours of strenuous, low-paid work and having little social or financial buffer with which to cope with this lack of control.
Discussion and Conclusion
This study analyzes the relationship between WTC and worker well-being in the context of specific occupations that are shaped by class, gender, and race. It teases apart both the different relationships between control and distress across occupational ecologies and the different aspects of WTC that might be relevant in each of those settings. The results suggest that the buffering effects of WTC depend on a match between the specific aspect of control and the kinds of demands workers face, both of which depend on occupational context. Importantly, this project’s results also corroborate previous work that finds beneficial effects for worker well-being of worker-controlled scheduling flexibility (e.g., the ability to leave work early to pick up a sick child), rather than the kind of employer-controlled flexibility (e.g., calling people in or sending them home on short notice) that often creates unpredictability in workers’ schedules (e.g., see Clawson & Gerstel, 2014; Henly, Shaefer, & Waxman, 2006; Lambert, 2008; Lambert, Haley-Lock, & Henly, 2012; Negrey, 2012).
This study’s findings of the unique time control needs among CNAs illustrate why attention to particular aspects of WTC in specific occupational contexts is important. CNAs are the most socially marginal group of workers examined in this study. They are the lowest paid, are predominantly female, and have an overrepresentation of women of color. At this intersection of race and gender, workers are disproportionately likely to be employed in low-wage work (Jensen & Slack, 2003) and thus more likely than those in higher wage occupations to seek additional work hours to meet basic family financial needs (Geiger-Brown, Muntaner, Lipscomb, & Trinkoff, 2004; Jacobs & Gerson, 2004). These financial pressures may be especially acute for CNAs, many of whom are single parents or the sole or primary earners in their households (Kahn, 2006; Rakovski & Price-Glynn, 2009). Attention to occupational context is critical to illuminating how the struggles of socially marginalized workers, such as CNAs, are compounded by the limited control this article elucidates.
The financial exigencies that go into work hours calculations for CNAs are emphasized by our finding that (a) for these workers alone, the desire to cut back on hours was a significant predictor of stress but (b) supervisor pressure to work additional hours had no relationship with job stress. In other words, something other than supervisor pressure keeps CNAs who are overworked in that situation. In interviews from the larger study of which this article is a part, CNAs were torn between the trade-off between time and money embedded in this kind of hours mismatch. They simultaneously worried about not working enough to support their families financiallyand also about not spending enough time with their families. Unlike nurses, their wages were not sufficient to make them comfortable choosing family time over additional income. Although many workers struggle with overwork, it seems that CNA’s experience is exacerbated by this sense of ambivalence and the limited resources they might use to buffer themselves.
From this angle, looking at the case of CNAs suggests some relatively straightforward—albeit politically charged—solutions to improve conditions for these workers. Their fundamental bind is that their wages are too low to meet their families’ needs, but the very insufficiency of those wages increases those needs, by requiring CNAs to maintain longer paid work hours instead of having the time to, for example, provide their own child care. When combined with employer-controlled scheduling, these low wages leave CNAs in a particularly vulnerable position. CNAs report being regularly assigned fewer weekly hours than they would prefer, leaving them in a constant search for extra hours to add to their schedules (Clawson & Gerstel, 2014). Employers save money through this kind of lean staffing. Furthermore, by keeping weekly hours low, employers create a pool of workers eager for more hours—workers they can call in whenever they need extra labor, but who will not earn overtime wages when they pick up these extra shifts (Henly et al., 2006).
Raising wages, providing subsidized child care, and giving workers paid sick leave are solutions that would benefit not only these health care workers but also those for whom these workers are providing care (Gornick & Meyers, 2008). Kahn (2006) reports that strict attendance requirements at nursing homes lead some CNAs to “report to work when they themselves are ill, sometimes with contagious illnesses, in order to conserve possible discipline-incurring absences for the occasions when they have sick children” (p. 105). In the larger study, we found the same patterns (Clawson & Gerstel, 2014). Despite the danger to patients, management not only permitted this practice of showing up to work sick but even indirectly encouraged it because it might save money (Kahn, 2006). Thus, giving workers more control over their time in the form of paid leave for “routine and non-routine caregiving” (Gornick & Meyers, 2008) is not only the right thing to do for low-wage workers, it also benefits the people for whom these workers care.
In addition to paid family leave, free or subsidized child care and preschool would help all workers, especially those who are forced to choose between time to earn money (often used to pay for child care) and time to spend with their children. Because these workers are often women, such policies would particularly help to address gender- and class-based inequalities in terms of work time (Gornick & Meyers, 2008; Williams, 2010). The United States, we should note, is shockingly behind in this regard; ranking below most other developed nations in the provision of subsidized child care and pay for care workers(Heymann, 2001; Kelly &Kalev, 2006). Ultimately, worktime scheduling is a way that workers balance many competing demands in their lives. Thus, policy can and should address not only workers’ control over work time itself but also the pulls of those competing demands such as child care that are experienced by all workers.
Despite a political and economic climate that might seem hostile to these worker-friendly policies, recent evidence suggests cautious optimism. For example, although national legislation on paid sick leave has proved elusive, states and cities have recently begun to take action on the issue. In 2014, California and Massachusetts passed statewide paid sick days laws, joining Connecticut (which passed the only other statewide measure in 2011) and more than a dozen cities with such legislation (Ness, 2014). Movements toward a higher minimum wage have also received widespread attention in recent years. In 2014, President Obama supported a US$10.10 national minimum wage. In 2013 and 2014, 13 states increased their minimum wages, as did 10 city and county governments. Seattle voted to raise its citywide minimum to US$15 an hour by 2018 and the mayors of New York, Los Angeles, and Chicago have all backed a US$13 wage floor. These actions are relevant to CNAs, whose national median wage was US$11.73/hr in 2012 (Bureau of Labor Statistics, 2014).
Many forms of worker organizinghave played a critical role in advancing these demands for wages and benefits, and such organizing might be the most promising route to implementing the kinds of changes in worktime policy outlined here. Unions—such as Service Employees International Union (SEIU) United Healthcare Workers—continue to organize CNAs despite the obstacles created by employer resistance to collective bargaining and a climate of relatively high unemployment in the United States. Unionized CNAs earn higher wages than their nonunionized counterparts (Wicks-Lim, 2009). The faster-than-average job growth for nursing assistants and the consequent shortage of skilled long-term care workers (Bureau of Labor Statistics, 2014; Stone & Harahan, 2010) would seem to put CNAs in a stronger position to collectively organize; however, CNAs who are members of a union remain a minority—only about 14% of nursing assistants, nationally (Wicks-Lim, 2009).
Nevertheless, collective actions by low-wage workers both inside and outside of union models have intensified and gained national attention in recent years—most famously among fast-food workers. Home health care workers (who have roles similar to that of CNAs, but do not have the formal training) have begun to join fast-food workers in these widespread strikes and the only-slightly-less-marginal CNAs might find inspiration in these kinds of actions. The case for better working conditions for CNAs is bolstered by evidence that nursing home resident well-being is greater where CNA job satisfaction is higher (Bishop et al., 2008).
An alternative form of worker organization—worker-owned businesses—also offers promise in terms of improving working conditions for workers such as CNAs by creating structures that give workers control over the institutions that affect their lives (Majee & Hoyt, 2010). The intimate nature of their jobs leads care workers to feel a strong emotional attachment to the work they do (Dodson & Zincavage, 2007; Rakovski & Price-Glynn, 2009). Rather than allowing employers to exploit this attachment as a means to motivate an undercompensated workforce (Dodson & Zincavage, 2007), worker-owned care businesses can transform this attachment into mutually-beneficial, patient-worker, business models. Indeed, the worker-owner model for home health care has been found to benefit both workers and clients (Majee & Hoyt, 2010). Further evidence of the potential of worker-owned home health care cooperatives comes from Bologna, Italy, where as much as 60% of home health care services are provided by employee cooperatives (Logue, 2006). A handful of successful examples exist in the United States (including Bronx-Based Cooperative Home Care Associates, Home Care Associates in Philadelphia, and Partners in Personal Assistance in Ann Arbor) and this promising model would benefit from additional research and policy that supports funding and incubation.
Researchers concerned with the consequences of workers’ control over their work time must acknowledge long-standing patterns of occupational segregation that leave workers in different social locations with very different needs and also very different resources on which to draw to meet those needs. The variation found in this study in the relationships between specific elements of WTC in specific occupational contexts remind us that bringing an awareness of stratification patterns into our research designs can create opportunities to better understand workers’ experiences. Research has already begun to move in the direction of disentangling subdimensions of WTC but could pay more attention to the ways these aspects have different valences across occupational ecologies.
Policymakers, too, should account for the ways work-scheduling policies can have different implications for differently situated workers. The contrasting pulls of overwork felt by salaried workers and underemployment by hourly workers suggest that maintaining such a system benefits employers at the expense of all workers. Nevertheless, choices between income and time are much more constrained for some. Recently, a prominent worktime scholar (Schor, 2010) argued for distributing time in the labor market more evenly—reducing labor market time for high-hours workers to increase income for low-hours workers. Demands to redistribute work time as a way of countering unemployment and sharing the available wages arose during the Great Depression, but such solutions have yet to be broached in the current economic recovery (Negrey, 2012).
The negative impact that a lack of WTC can have on workers’ health and well-being should give us new impetus to consider alternative and innovative solutions to worktime regulation. Control, like other resources in society, is not distributed evenly across social locations. For the least powerful workers, challenges to health and well-being due to a lack of WTC promise to compound the disadvantages of their social location and reinforce, even bolster, existing inequalities.
Limitations
Although this study makes important contributions to the study of WTC and its consequences, it also has several limitations. The cross-sectional, nonexperimental design does not allow for causal conclusions. Reverse causality is a possibility—that feeling control over work time is a result of feeling less job-related stress. In their review, Hausser et al. (2010) find that longitudinal studies showed weaker support for the job-demand control model predicting job-related well-being than did cross-sectional studies. Incorporating an occupationally comparative model into future longitudinal and experimental research designs might be a fruitful avenue of research. A small sample size within each occupation also limited statistical power in making comparisons. In addition, although some might consider using single-item measures as a limitation, it also leads to useful insights regarding the different aspects of WTC that would otherwise be concealed by combining these items into a scale.
Another limitation is that class and race are clearly entangled in this study, as they are in American society. Without a low-wage, predominantly female, and predominantly White comparison group, I can only speculate about the ways CNAs’ racial composition contributes to the distinct outcomes for that group. Also, as noted, Massachusetts has a higher proportion of Whites in the workplace than the national average. The results might have been different if the study was based in a state with a higher population of people of color.
EMTs and CNAs held second jobs at much higher rates than physicians and nurses and worked significantly more hours in those jobs than the other two occupations. Stress levels in these second jobs are likely tied to stress levels in primary jobs, and lacking a measure of “second job stress” is a limitation of this study. However, holding a second job was not a significant predictor of worker stress in our models.
The self-report nature of the data could also be seen as problematic. But, as I was interested in workers’ perceptions of their own control and their own well-being, I felt that a self-report measure was appropriate, especially because the same measure was used across occupations. However, the self-report nature of these measures raises some questions for future research. For example, to what degree do worker expectations of control differentially impact their self-assessment of stress? Also, how does attitude about one’s work affect that self-assessment? In other words, does a sense of “doing good” buffer workers from feeling stressed about a lack of control over their work time?
Footnotes
Acknowledgements
I would like to thank Naomi Gerstel, Dan Clawson, and Anna Branch for their support and guidance with this project. I would also like to thank Matt Atwood, Joel Rudin, and two anonymous reviewers for their helpful comments.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research and/or authorship of this article.