
Abstract
While the positive effects of physical activity (PA) on mental health are well documented, limited research has explored its influence on the positive psychological well-being in elderly individuals. This study examined the effects of a multi-component PA intervention on various facets of psychological well-being among older adults residing in retirement homes. Fifty-eight elderly individuals (mean age = 83.8 years, 76.3% female) residing in retirement homes participated either in either a 12 week multi-component PA intervention program or in an attention control group. Those in the intervention group engaged in supervised group exercise lessons for 45 min, three times per week, and used wearable activity monitors during weekdays over 12 weeks. Assessments were conducted before and after the intervention to measure happiness, life satisfaction, eudaimonic well-being, and depressive symptoms, which are four components of psychological well-being. On average, those in the intervention group attended about 86.9% of group exercise sessions and used the activity trackers for 97.5% of the designated days. Results from linear mixed models indicated that the intervention had a positive effect on happiness in the intervention group, but not in the control group. Nonetheless, no significant differences were found in terms of changes in eudaimonic well-being, life satisfaction, and depressive symptoms between the two groups. This selective impact on different dimensions of psychological well-being implies that subsequent research could explore the integration of more comprehensive components in PA interventions targeting all dimensions of psychological well-being, as each of them is a key aspect of healthy aging and independently related to a range of health outcomes amongst older adults.
Plain language summary
This study aimed to examine the impact of a multi-component physical activity (PA) intervention on psychological well-being in older adults living in retirement communities. Fifty-eight participants (mean age = 83.8 years) were voluntarily assigned to a 12-week multi-component PA intervention program or an attention control group. Participants in the intervention group were asked to take three 45-min supervised group exercise lessons per week and wear wearable activity trackers during the weekdays for 12 weeks. Four components of psychological well-being were assessed at baseline and the end of the intervention including life satisfaction, happiness, eudaimonic well-being, and depressive symptoms. Linear mixed models revealed a significant positive intervention effect on happiness such that happiness improved in the intervention group but decreased in the comparison group. However, there was no significant difference between the two groups in terms of the changes in life satisfaction, eudaimonic well-being, and depressive symptoms.
Introduction
The US population is aging rapidly. The number of Americans aged 65 and older is projected to nearly double from 50 million now to 95 million by 2060, comprising 23% of the total population by that time (U.S. Census Bureau, 2018). As aging is generally associated with a decline in physical and cognitive functioning and an increase in chronic conditions, the increasing number of older adults will lead to the rising cost of medical care (Aranda et al., 2021). In addition to age-related declines in health, the change in the social environment, such as retirement and social isolation, also negatively impacts psychological well-being in older adults (Zhou et al., 2021). Maintaining high levels of psychological well-being is considered a critical part of “successful aging” (Krivanek et al., 2021). For example, there is robust evidence showing that high levels of psychological well-being are associated with a lowered likelihood of functional disability, various chronic diseases, and all-cause mortality (H. Lee & Singh, 2021; Shiba et al., 2021). Therefore, identifying potentially modifiable factors that are associated with psychological well-being in later life has considerable public health importance for the aging society.
Physical activity (PA) has been identified as one of the promising modifiable factors linked to psychological well-being in older adults. For example, considerable epidemiological and experimental research has shown that PA can be used to prevent and treat depression and anxiety in older adults (Dishman et al., 2021). However, previous studies have primarily focused on the relationship between PA and negative aspects of psychological well-being such as mental disorders, whereas been research has explored the relationship between PA and positive aspects of psychological well-being among older adults. Psychological well-being is a comprehensive concept including negative and positive psychological characteristics (Keyes, 2007; Ryan et al., 2008). With respect to the positive dimension of psychological well-being, hedonic well-being, and eudaimonic well-being are two major approaches to operationalizing positive well-being. Hedonic well-being refers to pleasure attainment and focuses on the subjective experience of happiness and life satisfaction (Ryan & Deci, 2001). Eudaimonic well-being refers to the degree to which a person is fully functioning and focuses on meaning, good relationships with others, and self-realization (Ryan & Deci, 2001). Eudaimonic well-being is commonly operationalized as consisting of six psychological domains including autonomy, purpose in life, personal growth, positive relations, self-acceptance, and environmental mastery (Ryff, 1989). Hedonic well-being and eudaimonic well-being are important aspects of healthy aging and both related to a range of health outcomes independent of negative aspects of psychological well-being. For example, a longitudinal study found that happiness was inversely associated with mortality among 1,012 older adults during 15 years of follow-up (Koopmans et al., 2010). Another longitudinal study found that eudaimonic well-being, assessed by autonomy, sense of control, and purpose in life, predicted a lower risk of all-cause mortality among 9,050 older adults with an average follow-up of 8.5 years (Steptoe et al., 2015).
Previous studies examining the relationship between PA and hedonic well-being and eudaimonic well-being in older adults showed promising findings. For example, Kim et al. (2016) found that higher levels of self-reported leisure-time PA were associated with higher levels of life satisfaction and positive affect in older adults with loneliness. In older adults diagnosed with osteoporosis, leisure-time PA was found to be positively associated with eudaimonic well-being (Gunnell et al., 2011). However, previous studies investigating the relationship between PA and positive psychological well-being in older adults are mainly observational in nature (Zhang & Chen, 2019a). More research on investigating interventions that improve hedonic well-being and eudaimonic well-being is warranted.
Additionally, previous intervention studies examining the effects of PA on psychological well-being, mainly negative aspects, have predominantly adopted supervised, group-based exercise programs such as aerobic or strength training classes and have shown promising results (Netz et al., 2005). While walking has been identified as the favorite type of exercise in older adults (Stathokostas & Jones, 2016), relatively few intervention studies have investigated the impact of walking on psychological well-being in the older population. For example, Fisher and Li (2004) found that a 6 month neighborhood walking program significantly improved life satisfaction in older adults. Recently, emerging research using wearable activity trackers offers significant promise for promoting walking in older adults. For example, Cadmus-Bertram et al. (2015) found that older adults who used Fitbit activity trackers for 16 weeks increased daily steps by 798 on average.
The objective of the current study was to investigate the effect of a 12 week multi-component PA intervention on life satisfaction, happiness, eudaimonic well-being, and depressive symptoms, representing various aspects of psychological well-being, in older adults residing in retirement communities. The intervention components included supervised group exercise classes and using wearable activity trackers combined with providing weekly feedback and setting daily step goals. Unique to our research was the implementation of a multi-component PA intervention and the investigation of its impact on multiple dimensions of psychological well-being in older adults living in retirement communities. As far as we know, no existing study has examined the impact of a combined intervention of supervised exercise lessons and walking on psychological well-being in older adults. The 2018 Physical Activity Guidelines suggest that older adults would gain more health benefits from multi-component PA including aerobic endurance, strength, balance, and flexibility (US Department of Health and Human Services, 2018). Therefore, it is possible that multi-component PA would also have a great impact on psychological well-being in older adults. In addition, the existing literature has largely focused on the negative aspects of psychological well-being, suggesting a need to explore the multifaceted impact of PA on life satisfaction, happiness, eudaimonic well-being, and depressive symptoms, all of which are essential to understanding the full scope of psychological well-being in older adults. It was hypothesized that the multi-component PA intervention would benefit each dimension of psychological well-being in the intervention group compared to the comparison group. The findings of this study would expand the current knowledge on the relationship between PA and psychological well-being by combining supervised exercise programs and wearable activity trackers as intervention components and assessing both positive and negative dimensions of psychological well-being.
Method
Study Design
The current study used a two-arm, quasi-experimental design. We recruited individuals from two retirement communities in southeast Michigan. With the assistance of administrators and staff members in the retirement communities, flyers were distributed, and potential participants were invited to attend an on-site presentation introducing the current study. Eligibility criteria were being aged 65 or older, able to walk for 10 feet without human assistance, able to speak and read English fluently, and scored 3 or greater in the Mini-Cog test, a screening test for cognitive impairment in older adults (Borson et al., 2003). Previous research showed that the recruitment rate to PA intervention research was low in older adults living in retirement communities (Duckham et al., 2018). Therefore, this study employed a non-randomized controlled trial design, in which participants were assigned to the intervention group or comparison group with their preference. participant. The study protocol received endorsement by the University Institutional Review Board (HUM00158279).
Participants
A total of 58 eligible individuals participated in this study. Among these participants, 40 were in the intervention group and 18 were in the comparison group. The mean age of participants was 83.4 ± 6.61 years and more than half (51.7%) of the participants aged 85 years or older. Females counted 76% of the participants and all participants were Caucasian. Thirty-eight percent of the participants were married and near half (48.3%) of the participants were college graduates.
Intervention
Group Exercise Lessons
The intervention group received three, 45 min group exercise lessons for 12 weeks. The group exercise lessons were taught by two experienced instructors. A typical group exercise lesson consists of 10 min warm-up (i.e., stretching exercises and walking in place), 30 min functional fitness exercises (i.e., muscle strengthening, balance, and coordination), and 5 min cool-down (i.e., stretching and breathing). The design of group exercise lessons was based on the 2018 Physical Activity Guidelines’ recommendation that older adults should participate in multi-component PA that includes aerobic exercises, muscle strengthening exercises, flexibility exercises, and balance training.
Wearable Activity Trackers With Feedback and Goal Setting
Each participant in the intervention group received a Fitbit (Model InspireHR) activity tracker to self-monitor their daily PA, 5 days per week for 12 weeks. The Fitbit activity tracker, a commercially obtainable and noninvasive activity tracker that is worn on the wrist, records multiple PA metrics such as steps taken, distance covered, and floors ascended. These metrics can be visually presented on the device itself, offering immediate feedback to the user. The research team delivered a 1 hr presentation before the intervention to introduce the basic features of the trackers, assist participants to initialize their trackers, and guide them to operate their trackers. Since most of the participants did not use a smartphone, the research team set up a Fitbit account for each participant. Participants were instructed to wear the activity monitors Monday through Friday to track their PA. The research team collected participants’ trackers every weekend and returned the trackers to participants before the next Monday morning. Each participant received a Weekly Individual Report (one-page paper with graphs and numbers) showing their daily steps during the previous week. Collecting trackers every week also allowed us to provide ongoing assistance for participants regarding the use of the activity tracker. In addition, we incorporated a goal-setting strategy as an intervention component. Each participant was given a personalized step-count goal for increasing their daily step counts by 500 to 1,500 every 2 weeks, toward an ultimate goal of 7,500 steps per day (I.-M. Lee et al., 2019). Participants who reached 7,500 steps per day during the intervention were asked to maintain their PA level until the end of the intervention.
The comparison group maintained their regular activities, meanwhile receiving bi-weekly newsletters addressing topics relevant to PA and overall health.
Measures
During the first 2 weeks of September 2019, the research team administered a questionnaire assessing major outcomes including life satisfaction, happiness, eudaimonic well-being, and depressive symptoms, and covariates including sociodemographic information, self-rated health, and PA, as well as a functional mobility test, to each participant in the intervention group and the comparison group. After the 12 week intervention, the research team again administered the same questionnaire for life satisfaction, happiness, eudaimonic well-being, and depressive symptoms to each participant in the two groups.
Life Satisfaction
Life satisfaction, the cognitive component of hedonic well-being, was assessed using the Satisfaction With Life Scale (SWLS) (Diener et al., 1985). The SWLS comprises five items created to measure an individual’s overall assessment of life satisfaction (e.g., “In most ways my life is close to my ideal”). Respondents were prompted to indicate the extent of agreement or disagreement with each item, using a 7-point Likert scale. The sum of all items provides a composite score (from 5 to 35), with higher scores representing higher levels of life satisfaction. Previous research have documented sufficient reliability and validity of SWLS for the use in older adults (Pavot et al., 1991). The internal consistency was satisfactory in the present study (Cronbach’s alpha = .85).
Happiness
Happiness was measured as the affective component of hedonic well-being using the Subjective Happiness Scale (SHS) (Lyubomirsky & Lepper, 1999). The SHS consists of four items, prompting respondents to rate the applicability of each statement (e.g., “In general, I consider myself a very happy person”) on a 7-point Likert scale. A mean score, spanning from 1 to 7, of all items was derived to indicate the level of happiness with higher scores corresponding to greater happiness. The SHS has been demonstrated to be valid and reliable in older adults (Angner et al., 2013). In the present study, Cronbach’s alpha value was .78 for the SHS.
Eudaimonic Well-being
Eudaimonic well-being was measured using the 18-item Psychological Well-Being Scale (PWBS) (Ryff, 1989). The PWBS comprises six 3-item subscales that measure autonomy, environmental mastery, personal growth, purpose in life, positive relations with others, and self-acceptance. Participants rated their agreement or disagreement with each statement (e.g., “Some people wander aimlessly through life, but I am not one of them”) on a 7-point Likert scale. An index (from 3 to 21) was computed by first summing items in each subscale and then averaging the scores of all subscales. Higher scores indicate higher levels of eudaimonic well-being. Previous studies have provided support for the validity and reliability of the use of PWBS in older adults (Andrew et al., 2012; Clarke et al., 2001). In the current study, Cronbach’s alpha values ranged from .5 to 0.7 for the six subscales while the Cronbach’s alpha value for all of the 18 items was .84, supporting the use of a single index for eudaimonic well-being.
Depressive Symptoms
Depressive symptoms were assessed using the short version of the Centre for Epidemiological Studies Depression Inventory (CESD-R) (Radloff, 1977). The CESD-R consists of ten items pertaining to symptoms of depression, such as “I was bothered by things that usually don’t bother me”. Respondents were asked to rate how often they experience each symptom during the past week on a 4-point Likert scale. The level of depressive symptoms was reflected by summing the responses of the ten items (from 0 to 30), with higher scores indicating greater levels of depressive symptoms and a cutoff score of 10 or higher indicating significant depressive symptoms. Previous studies have demonstrated that the CESD-R is a reliable and valid measure for assessing depressive symptoms in older adults (Andresen et al., 1994; Irwin et al., 1999). The internal consistency in this study was 0.79.
Covariates
Baseline age, gender, race, education (not graduate high school/high school graduate/bachelor degree or higher), marital status (married/not married), body mass index (BMI), self-rated health, functional mobility, and PA were measured to minimize potential self-selection bias. BMI was computed from self-report height and weight (kg/m2). Self-rated health was measured using a single-item question “Would you say in general your health is poor, fair, good, very good, or excellent?” The response options ranged from 1 (poor) to 5 (excellent). This single-item question has been shown to be a valid measure of health status and is related to the mortality and morbidity of a number of diseases (DeSalvo et al., 2006). Functional mobility was evaluated using the Timed Up and Go (TUG) test (Podsiadlo & Richardson, 1991), in which participants are timed as they rise from a chair, walk 3 m, turn, walk back to the chair, and sit down again, with less time indicating higher levels of functional mobility. PA was measured using the validated International Physical Activity Questionnaire—Short Form (IPAQ), which assesses the frequency and duration of vigorous-intensity PA, moderate-intensity PA, and walking during the past week (Craig et al., 2003). The metabolic equivalents (MET) minutes per week were computed according to the standard scoring procedures for the IPAQ, with greater MET-minutes per week indicating higher levels of PA.
Process Evaluation
Adherence to group exercise lessons was assessed by recording and calculating each participant’s attendance as the number of lessons attended divided by the total number of lessons taught. Fitbit tracker compliance was measured by calculating the percentage of days each participant wore the tracker using the Fitabase analytics system (Small Steps Labs, San Diego, CA, USA) which allows investigators to manage the Fitbit data for multiple participants.
Data Analysis
Descriptive statistics including means with standard deviations for numerical variables (i.e., age, self-rated health, BMI, functional mobility, PA, and psychological well-being outcomes) and counts with percentages for categorical variables (i.e., gender, education, marital status) were used to present the baseline characteristics of participants. One participant in the intervention group withdrew from the study in the first week due to dissatisfaction with the accuracy of the Fitbit activity tracker, and thus was excluded from the final analysis. The skewness and kurtosis of all numerical variables were checked for normality, with an absolute skew value greater than two and/or an absolute kurtosis value greater than seven indicating a substantial departure from normality (Curran et al., 1996). Possible transformations, such as logarithmic, squared, or dichotomous, would be applied for non-normally distributed variables. The results showed that all the numerical variables were within the acceptable range of skewness and kurtosis, and thus no transformation was performed. It should be noted that the sample sizes of the intervention and control groups are different due the fact that this study was a non-randomized controlled trial. Therefore, Welch’s t-test, which does not rely on the assumption of equal variance, was used to compare the numerical variables at baseline between the intervention group and the comparison group (Delacre et al., 2017). The differences of categorical variables at baseline between two groups were examined using the Chi-square test.
To examine the intervention effect on psychological well-being, several linear mixed models were conducted due to the repeated nature of the study design and the unbalanced sample size between the two groups. The psychological well-being outcomes, life satisfaction, happiness, eudemonic well-being, and depressive symptoms, were treated as the dependent variables of these models, respectively. The independent variables of each model included the main effect of time (baseline vs. posttest), the main effect of group (intervention vs. comparison, dummy coded), and the interaction term between time and group. In addition, the covariates that were significant at baseline between two groups were controlled for in each model. Statistically significant level for all analyses is set at p < .05. All of the quantitative data analyses were performed using R version 3.5 via RStudio (Posit Software, USA).
Results
Table 1 presents the baseline characteristics and their differences between the two groups. Based on Welch’s t-tests and Chi-square tests, no significant differences were found between the two groups, except for age and life satisfaction. Specifically, participants in the intervention group were older (85.4 vs. 80.3 years, p = .025) and had a higher level of life satisfaction (29.86 vs. 23.81, p = .001) than the comparison group. In addition, there was a marginally significant difference (p = .059) in the self-rated health between the intervention group (
Baseline Characteristics of Participants.

p < .05. **p < .01.
Table 2 shows psychological well-being outcomes at baseline and post-test between the intervention group and the comparison group. Table 3 presents the results of linear mixed models of intervention effects on the psychological well-being outcomes. Regarding happiness, the linear mixed model showed that there was no main effect of group (β = .17, p = .29) but a significant main effect of time (β = −.31, p = .03). In addition, this main effect was overshadowed by a significant interaction between group and time (β = .42, p = .02), suggesting that the change of happiness from baseline to posttest was different between the two groups. Specifically, the average happiness score of the intervention group increased from 5.65 to 5.76, while the average happiness score of the comparison group decreased from 5.21 to 4.90. These results indicate a positive impact on happiness due to the intervention.
Means and Standard Deviations of Psychological Well-being Outcomes at Baseline and Posttest.

Standardized Coefficients (Standard Error) of Linear Mixed Models (Fixed Effects Only).
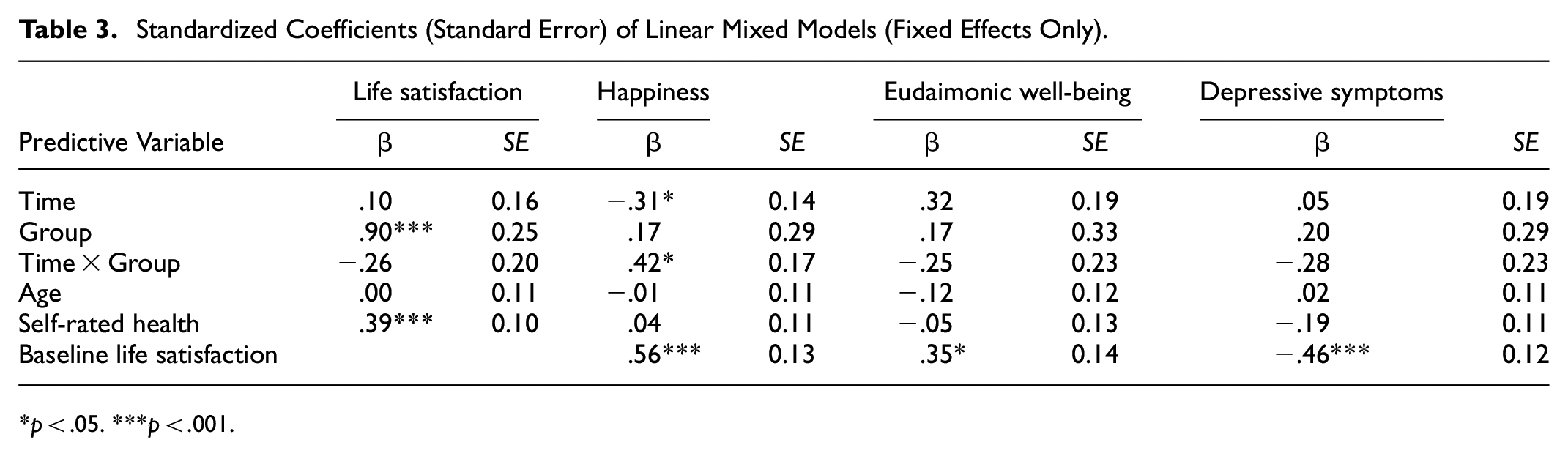
p < .05. ***p < .001.
Regarding the life satisfaction, the linear mixed model revealed a significant main effect of group (β = .90, p < .001), but no main effect of time (β = .10, p = .56). In addition, there was no interaction between group and time (β = −.26, p = .20). The results indicated that the intervention group had overall a higher level of life satisfaction compared with the comparison group.
As shown in Table 3, the linear mixed models showed similar results for eudaimonic well-being and depressive symptoms. There was no significant main effect of time and group, and no significant interaction between time and group for eudaimonic well-being and depressive symptoms (p’s > .05). Regarding the covariates controlled in each model, self-rated health was positively associated with life satisfaction (β = .39, p < .001). Life satisfaction at baseline was a significant covariate of happiness (β = .56, p < .001), eudaimonic well-being (β = .35, p = .02), and depressive symptoms (β = −.28, p < .001), indicating higher levels of life satisfaction associated with higher levels of happiness and eudaimonic well-being and lower levels of depressive symptoms. In addition, age was not a significant covariate in any model, indicating that the difference of age in two groups did not affect the research results.
Discussion
In the current study, we investigated the effects of a 12 week multi-component PA intervention on both positive and negative dimensions of psychological well-being among older adults residing in retirement communities. The results revealed that the intervention did not have consistent effects on different components of psychological well-being. Specifically, while it had a positive impact on happiness, it did not affect life satisfaction, eudaimonic well-being, and depressive symptoms. Happiness, life satisfaction, eudaimonic well-being, and depressive symptoms are indicators of different aspects of psychological well-being. The selective impact of PA on these indicators further substantiates that psychological well-being is a complex and multifaceted construct and highlights the importance of considering various dimensions in understanding the role of PA in enhancing mental health.
Supporting our findings, a recent systematic review has shown a positive relationship between PA and happiness in older adults (Zhang & Chen, 2019b). Tse et al. (2014) reported that an 8-week exercise intervention consisting of stretching and balance exercises, lasting 60 min per session and conducted once per week, significantly enhanced happiness in the intervention group, but not in the control group receiving usual care, among elderly persons residing in nursing homes. In another study, McAuley et al. (2000) found that both aerobic exercises and stretching exercises, lasting 40 min per session and conducted three times per week, resulted in a significant improvement in happiness after 6 months. Furthermore, they found there was no substantial difference in the impact on happiness between the two forms of PA. Compared with life satisfaction, happiness is commonly considered as the affective component of subjective well-being. There is considerable evidence that PA is associated with positive affect (Liao et al., 2015). Therefore, happiness may be improved by frequent experiences of enjoyment and pleasure induced by participation in PA (Diener et al., 2009; Salmon et al., 2003). However, it should be noted that the magnitude of improvement in happiness in the intervention group was relatively small (5.65 vs. 5.76). Therefore, the results should be interpreted with caution as the positive effect of the PA intervention on happiness was reflected in maintaining high levels of happiness rather than substantially improving happiness.
The current study did not show a positive intervention effect on life satisfaction. This finding is consistent with a recent randomized controlled trial, in which Yu et al. (2020) found that a 12 week exercise intervention, including two, 60 min group exercise lessons per week consisting of aerobic exercises and resistance training, which were similar to our study, had no impact on life satisfaction in older adults. However, the mean age of the participants was 62.2 years in their study (Yu et al., 2020), which was lower than that in the current study. Although the Physical Activity Guidelines suggest that older adults would gain more health benefits from multi-component PA (US Department of Health and Human Services, 2018), based on the findings of our study and existing literature, multi-component PA might not have a significant impact on life satisfaction. The lack of consistent evidence showing the positive relationship between PA and life satisfaction in older adults may be explained by two reasons. First, compared with happiness, life satisfaction is a more stable component of psychological well-being reflecting evaluations across the life-course and thus is less subject to change (Schimmack et al., 2002). Second, interventions targeting PA alone may not be sufficient to alter the level of life satisfaction in older adults. Previous studies have identified a range of determinants of life satisfaction in older adults such as social support and cognitive functions (St. John & Montgomery, 2010; Yeung & Fung, 2007). A recent study found that an active aging program targeting social engagement, PA, and cognitive functions significantly improved life satisfaction in institutionalized older adults (Buedo Guirado et al., 2020). Therefore, it might be promising for future research to examine the effect of more comprehensive interventions on life satisfaction in older adults.
To date, relatively few studies have examined the relationship between PA and eudaimonic well-being in older adults. Although a handful of cross-sectional studies showed a positive relationship between PA and eudaimonic well-being (Gunnell et al., 2011; Ju, 2017; Kim et al., 2017), the findings from the current study do not support this positive relationship. Only one previous experimental study (Conradsson et al., 2010) has examined the effects of exercises on eudaimonic well-being in older adults and the findings were consistent with the findings of the current study. In their study, Conradsson et al. (2010) conducted a 13 week high-intensity weight-bearing exercise intervention and found there was no difference in the change of eudaimonic well-being between the intervention group and the control group. It is possible that the positive relationship between PA and eudaimonic well-being in older adults observed in cross-sectional studies is caused by the reverse causality. As supported in a recent longitudinal study, Rector et al. (2019) found that the odds of maintaining high levels of PA were significantly higher for those with higher eudaimonic well-being. Another possible explanation is that treating eudaimonic well-being as a single construct might prevent our ability to reveal the impact of PA on specific dimensions of eudaimonic well-being.
Inconsistent with previous studies showing that exercises have a robust effect on reducing depressive symptoms in older adults (Chodzko-Zajko et al., 2009), the current study found no intervention effect on depressive symptoms. The lack of intervention effect on depressive symptoms in the current study may be explained by the ceiling effect, because the average score of depressive symptoms was low at baseline for participants in the intervention group. Future research is suggested to exclusively include older individuals with major depression or subsyndromal symptomatic depression.
Psychological well-being is a broad concept covering multiple distinct components. Each component of psychological well-being itself is associated with a range of factors. Based on our findings, PA alone may not be sufficient to substantially change psychological well-being in older adults. Future research is suggested to develop interventions combining PA and other potential factors such as social participation, cognition-enhancing activities, and psychological therapy, and examine their effects on different components of psychological well-being.
There are several limitations associated with this study. First, a non-randomized sampling was used in the group assignment, which may lead to the self-selection bias, even though we have controlled for covariates at baseline that were significantly different between the two groups. Second, the sample in the current study consisted of all white, non-Latino older adults, which limits the generalizability of the results to older adults of other race/ethnicities. Third, the effect of each component of the intervention (group exercise lessons, wearable activity trackers with self-regulatory techniques) was not independently examined and thus no conclusion can be made as to which component is more or less effective than the other. Last but not least, since psychological well-being is a broad term, dimensions of psychological well-being were not totally covered. Despite these limitations, the current study has strengths in measuring different dimensions of psychological well-being, adopting the multi-component PA intervention, and targeting older adults living in retirement communities, which contributes to the theoretical and empirical literature of PA and health promotion in older adults.
Conclusion
The current study expanded the understanding of the complex relationship between PA and psychological well-being by implementing a multi-component PA intervention and examining its impact on various dimensions of psychological well-being. The findings indicate that the 12 week multi-component PA intervention comprising group exercise classes and wearable activity monitors with self-regulation strategies is effective in improving happiness but has no impact on life satisfaction, eudaimonic well-being, and depressive symptoms among older adults residing in retirement communities. This selective impact on different aspects of psychological well-being suggests that future studies may consider incorporating more inclusive intervention components addressing all dimensions of psychological well-being, as each of them is a key aspect of healthy aging and independently related to a range of health outcomes in older adults.
Footnotes
Acknowledgements
The authors would like to thank Tony Maino, Kristy Collins, and Jun Chen for their help during the data collection.
Author Contributions
ZZ: Conceptualization, formal analysis, investigation, and writing. BG: Conceptualization and editing. WC: Conceptualization and supervision. All authors have read and approved the manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was partially supported by the University of Michigan School of Kinesiology Innovative Donor Award and the Rackham Graduate Student Research Grant. The funders have not played a role in the design, conduct, or analysis of the study.
Ethical Approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards. Written informed consent was obtained from all participants. The study protocol was approved by the University of Michigan Institutional Review Board (HUM00158279).
Trial registration
Registered on Clinicaltrials.gov # NCT05233813.
Data Availability Statement
The datasets generated and/or analyzed during the current study are not publicly available but are available from the corresponding author on reasonable request.