
Abstract
This study aimed to assess the individual, interpersonal, and environmental factors that relate to physical activity (PA) among older adults in rural communities in Wangthong district, Phitsanulok, Thailand. A cross-sectional study was conducted on 545 elders by multi-stage sampling. The data were collected via a validated questionnaire. Multiple logistic regression analysis was performed to identify potential determinants of PA. Factors including youngest-old (adjusted OR 1.55, 95% CI [1.05–2.28]), high level of income (adjusted OR 1.89, 95% CI [1.17–3.19]), being a member of the elders’ club (adjusted OR 1.68, 95% CI [1.15–2.46]), and high level of perceived self-efficacy (adjusted OR 1.79, 95% CI [1.23–2.61]) indicated higher likelihood of PA (p < .05). Interventions to improve PA among older people should include improving physical environmental attributes, creating more inexpensive and less time-consuming alternatives for PA, promoting peer support networks and activities to enhance self-efficacy.
Introduction
The United Nations defined older persons as those at the age of 60 or 65 years or over. This cut-off age acts as an indicator of population aging (United Nations, 2020). For Thailand, the older adults are defined as people at the age over 60. A report by the United Nations (2020) suggested that, in South-Eastern Asia, the number of older persons could double between 2019 and 2050. In 2020, Thailand has become an aging society with 16.73% of the population being over 60 years of age (Department of Older Persons, 2020). The aging society of Thailand is also due to the rise up to 25% by the year 2030, called a “complete-aged society.” According to the Foundation of Thai Gerontology Research and Development Institute (TGRI, 2009), over half of older people in Thailand live in rural areas. The 2015 Survey on Health and Welfare (NSO) found that approximately one out of three older persons were overweight, and half of older persons had a chronic illness or condition (TGRI, 2016).
Regularly physical activity (PA) is recommended to improve physical and mental functions, as well as to prevent many health problems associated with the lack of exercise, such as diabetes and cardiovascular disease. In addition, PA maintains older people mobility and independence (McPhee et al., 2016). The World Health Organization (WHO) classified PA into three groups as follows: (1) activity at work, (2) transportation, and (3) recreational activities. Recognizing the benefits of PA, the WHO recommends older adults to perform at least 150 minutes of moderate-intensity aerobic PA or 75 minutes of vigorous-intensity aerobic PA throughout the week, or a combination of moderate- and vigorous-intensity activity at least 2 days a week (WHO, 2020). Despite the clear benefits of PA, a study carried out on Thai older people in Thailand found that those who were unemployed or had underlying diseases had low levels of PA (28.8%–33.8%) (Liangruenrom et al., 2019). Moreover, the moderate-intensity PA had significantly negative correlation with age (Takagi et al., 2015).
Research studies have shown that several factors might influence the level of PA, such as age (Gopinath et al., 2018), self-reported health (Gaskin & Orellana, 2018), sex, household income, body mass index (BMI), co-morbidity, self-efficacy, perceived benefits and barriers to PA, knowledge about PA, social environment, and physical environment (Doubova et al., 2016; Liangruenrom et al., 2019). Additionally, people who feel encouraged to engage PA in their leisure time (i.e., social support) are more likely to perform PA, especially when the support comes from their family members (Lindsay Smith et al., 2017). The literature showed that the neighborhood environment (Chiang et al., 2019), and a sense of community belonging (Yip et al., 2016) were positively associated with PA. The environmental factors in PA policies, such as access to public exercise parks and exercises equipment for people in the community contribute to equity in health (Hämäläinen et al., 2016). Therefore, engaging in PA appears to be influenced by individual, physical, and socio-environmental factors. However, these factors are presented from different contexts which might not be an inference for the context of older people in rural areas in Thailand. Studies in Thailand reported that male wealthy older people were less likely to participate in physical activity (Ethisan et al., 2017). A systematic review also indicated that the determinants of PA related to individual and interpersonal factors (Liangruenrom et al., 2019) while the neighborhood environment did not. As the neighborhood environment and a sense of community belonging might help promote PA, public health strategies for senior citizens in rural areas should take these two factors into account.
Geographical heterogeneity of urban and rural areas affects PA of the population (Tuangratananon et al., 2018). In addition, kinship ties in the older adults in rural area in Thailand influence their participation in community activities and PA (Ethisan et al., 2017). The healthcare facility provides information related to PA and collaborates with local organizations to promote physical activities in clubs for older adults. However, the research on factors associated with PA for this age group are limited.
To date, there is a need to explore the factors associated with PA among older adults from rural communities. This information is important for designing public health strategies with the aim to promoting PA among older adults. Thus, the main objective of this study is to identify (1) individual factors including socio-demographic factors, perceived health, self-efficacy regarding PA, and perceived external and internal barriers to PA, (2) interpersonal factors comprising perceived social support to PA, and (3) environmental factors consisting of neighborhood environment and sense of community belonging. These factors might associate with PA among older adults from rural communities.
Method
Study Design and Setting
Phitsanulok is a central city in the lower north of Thailand. It was one of the seven provinces participating in a pilot project with the focus on senior citizens in the community by the Ministry of Social Development and Human Security in 2010 (TGRI, 2010). A group of older people in Wangthong district was selected by sampling technique to represent Thailand’s older people who live in rural areas due to its agricultural communities and high proportion of older adults. The proportion of older adults in this district between the years 2017 to 2019 was 13.26%, 14.37%, and 20.77%, respectively (Phitsanulok Provincial Health Office, 2017, 2018, 2019).
A Cross-sectional study was carried out in 2018. Thailand has 7,255 districts on four regions: northern, central, northeastern, and southern. Phitsanulok is a central city in the lower north of Thailand. It was one of the seven provinces that participated in a pilot project with the focus on senior citizens in the community by the Ministry of Social Development and Human Security in 2010 (TGRI, 2010). Wangthong district, which comprises 11 sub-districts, was purposively selected to be a representative of the rural areas as it has the proportion of agricultural communities, and the rise of older adults. The older adult proportion for this district for the years of 2017, 2018, and 2019 was 13.26%, 14.37%, and 20.77%, respectively (Phitsanulok Provincial Health Office, 2017, 2018, 2019).
Study Population, Sample Size and Sampling Method, and Sample Characteristics
The target population was 4,986 older people with no disabilities, living in Wangthong district. The required sample size was calculated using the mean estimation formula:

where n is the necessary sample size, the standard deviation (σ) was 23 from Park et al. (2014), the margin of error (d) was 5%, with 95% confidence interval (Z = 1.96) and the non-response rate was 10%. The necessary sample size (n) was calculated to be at least 520. According to the proportion allocation, the sample size of the older adults from 11 sub-districts was 545. The participants were selected by multi-stage sampling. A total of 4,986 senior citizens lived in 11 sub-districts in Wangthong district, Phitsanulok. Three sub-districts were selected by cluster sampling, resulting in Wangthong, Ban Klang, and Chainam sub-districts. Sampling of village was performed by cluster sampling, yielding three villages. Finally, the sample was sampling by simple random sampling with proportional allocation. The inclusion criteria were older adults with the age of 60 years or over who were able to communicate in Thai, or had a caregiver who could communicate in Thai, and willing to participate in the study. The exclusion criteria were: older adults with severe complications of chronic diseases, such as chronic kidney disease stage five with fatigue and tired, asthma with home oxygen therapy, and older adults with psychotic symptoms with cognitive impairment that were assessed by a doctor and informed by their relatives. A face-to-face structured questionnaire conducted by 10 trained of health professionals (nurses and public health practitioners) at participants’ homes. The training took approximately 4 hours, including informing objective, explaining the items in the questionnaire, and learning the role play while interviewed by the research team.
Instrument and Data Collection
Data were collected through a questionnaire which comprised eight parts as follows:
Part 1 comprised 16 items regarding socio-demographic factors including gender, age, body mass index, marital status, education level (e.g., did not attend school to completed tertiary education), income (the amount of money earned), own current dwelling, number of members in household, living arrangement, being a member of the older adult club, which supported activities by local organization, and duration of living in the community;
Part 2 consisted of eight items regarding participants’ perceived health (e.g., in the past 6 months, you feel healthy; and you have good immune system.). Likert scale ranging from 1 (Mostly disagree) to 5 (Mostly agree). The possible score ranged from 8 to 40 points, with higher scores indicating good health. The score was divided into three levels, with scores ranging between 8–19, 20–30, and 31–40 corresponding to different levels of perceived health: poor health, intermediate health, and good health, respectively;
Part 3 was related to self-efficacy regarding PA (e.g., I will be able to: engage PA as the goal; overcome barriers of PA), and used eight items with Likert scale, adopted from Neupert et al. (2009). The response categories for these items were 1 (Strongly disagree) to 5 (Strongly agree). The scores ranged from 8 to 40, with higher scores indicating greater self-efficacy. They were classified into three levels, with scores ranging between 8–18, 19–29, and 30–40 corresponding to different levels of self-efficacy: low, moderate, and high, respectively.
Part 4 comprised six items related to perceived social support regarding PA (e.g., Is there someone available to: advise in planning of PA; appreciate you when you engage PA). This part employed a Likert scale developed by the research team to measure the impact of participants’ perceived social support on the frequency that the participants were supported in engaging in PA. The response alternatives were “Never,” “Seldom,” “Sometimes,” “Almost always,” and “Always.” The composite scores ranged from 6 to 30, with higher scores indicating greater social support availability. The scores were divided into three levels, ranging between 6–14, 15–23, and 24–30, corresponding to low, moderate, and high social support, respectively.
Part 5 was related to the neighborhood environment and consisted of 22 items adopted from the Neighborhood Environment Scale designed by Cerin et al. (2006). This part contained the following subscales: (1) perceived residential density, (2) street connectivity, (3) infrastructures for walking and cycling, (4) esthetics, (5) safety from crime, and (6) safety from traffic (e.g., non-slippery street, prevention from being hurt by a stranger when being alone outside around the home, slow speed of traffic (30 mph). A five-point Likert scale, ranging from 1 (Strongly disagree) to 5 (Strongly agree), was used. The possible scores ranged from 22 to 110 points, and were divided into three ranges: 22 to 51, 52 to 80, and 81 to 110, corresponding to bad, acceptable, and good neighborhood environment.
Part 6 was related to the perceived external and internal barriers to PA, and adopted the Barriers in Physical Activity and Exercise Participation (BPEP) questionnaire (e.g., time constrain, no money, lack of facility to PA) (Justine et al., 2013). This questionnaire consists of 15 items and uses a five-point Likert scale, ranging from 5 (Strongly agree) to 1 (Strongly disagree). Lower scores indicated more negative belief while higher scores indicated more positive belief. The possible score ranged from 15 to 75 points, and was divided into three categories: 15 to 35, 36 to 56, and 57 to 75, corresponding to low, moderate, and high levels of perceived barriers to PA.
Part 7 comprised 12 items adopted from Young et al. (2004) aiming to assess the sense of community belonging. This part consisted of four subscales. They are: (1) membership, (2) influence, (3) integration and fulfillment of needs, and (4) shared emotional connection (e.g., I feel like community is my home; I familiar with the people in this community). A five-point Likert scale ranging from 1 (Strongly disagree) to 5 (Strongly agree) was used. The possible score ranged from 12 to 60 points. Scores were categorized into <27, 28 to 44, and 45 to 60, corresponding to a low, moderate, and high sense of community belonging, respectively.
Part 8 consisted of 16 items that measure the PA levels of the participants during a week of normal activity. It was adopted from the Global Physical Activity Questionnaire-GPAQ v2 (World Health Organization, 2012), The activity was a value of the metabolic equivalent of task (MET), time spent in performing each activity per week and frequency. The number of MET per week was computed and then classified into high, moderate, and low intensities based on the GPAQ guidelines (WHO, 2012).
Content validity was examined by three experts (a policy maker at the provincial health office, a practitioner at Wangthong District Health System, and an academician specialized in health behavior). A pilot test was carried out by 30 older adults who lived in the other sub-districts of the sample with similar environment. The Cronbach’s α coefficients revealed the internal consistency of the scales. The reliability coefficients of questionnaire parts 2 to 7 were .79, .82, .72, .74, .88, and .77, respectively. The GPAQ was translated into Thai, and its psychometric properties were examined. The validity and test-retest reliability of the GPAQ Thai version were in an acceptable level of item-content validity index (I-CVIs): .88 and .99, respectively. The concurrent validity between the GPAQ and the long form International Physical Activity Questionnaire (LF IPAQ) was acceptable (ρ = 0.75). The Criterion validity was relatively low (ρ = 0.33). Test-retest reliability was acceptable (ρ = 0.77) (Visuthipanich, 2016). This instrument was used to assess physical activity in the Thai National Health Examination Survey fifth (Aekplakorn, 2014). The informed consent was obtained from each subject before data collection. All participants were informed the objective of the study. They were voluntarily participated in this study. Confidentiality was undertaken by personal identification number during the process of data collection and analysis.
This study employed structured interview by trained health professionals with 100% response rate. Then the research team checked all questionnaires. The older adults trust health professionals did not reject to participate in this study. Two older adults with home oxygen therapy were excluded.
Data Analysis
Data were transferred and analyzed using SPSS Statistics 17.0 for Windows. Both descriptive and inferential statistics are presented in this paper. The independent variables were socio-demographic factors, perceived health, self-efficacy, social support, perceived barriers, neighborhood environment, sense of community belonging. PA was dependent variable. Categorical variables were described using frequency and percentage whereas quantitative variables were presented with mean, standard deviation, median (minimum, maximum), or median (interquartile range [IQR]). Adequate PA was classified according to PA level, with high and moderate intensity being adequate PA, and low intensity being inadequate PA. Type and duration of exercise were presented using the descriptive statistics. Factors associated with PA were assessed using multivariable logistic regression analysis. First, univariate analysis by Chi-square test was employed to select the candidate factors. The candidate factors with p-value <.25 were included in the multiple logistic regression analysis by backward elimination method (Wald test). Then, the Hosmer-Lemeshow goodness of fit test was used in the final model. Factors associated with PA were those with a p-value <.05 in the final model.
Results
Socioeconomic Characteristics, Living Conditions and Participation in the Community
A total of 545 older adults, aged 60 to 88 completed the questionnaires. The majority of participants were women (61.3%), and between the age of 60 to 69 years (62.9%). More than one-third (38.7%) of the sample had a normal BMI, married (68.8%), and had completed primary school education (72.5%). The most of them earning less than 50,000 Baht per year (see Table 1).
Socioeconomic Characteristics of the Study Sample (n = 545).
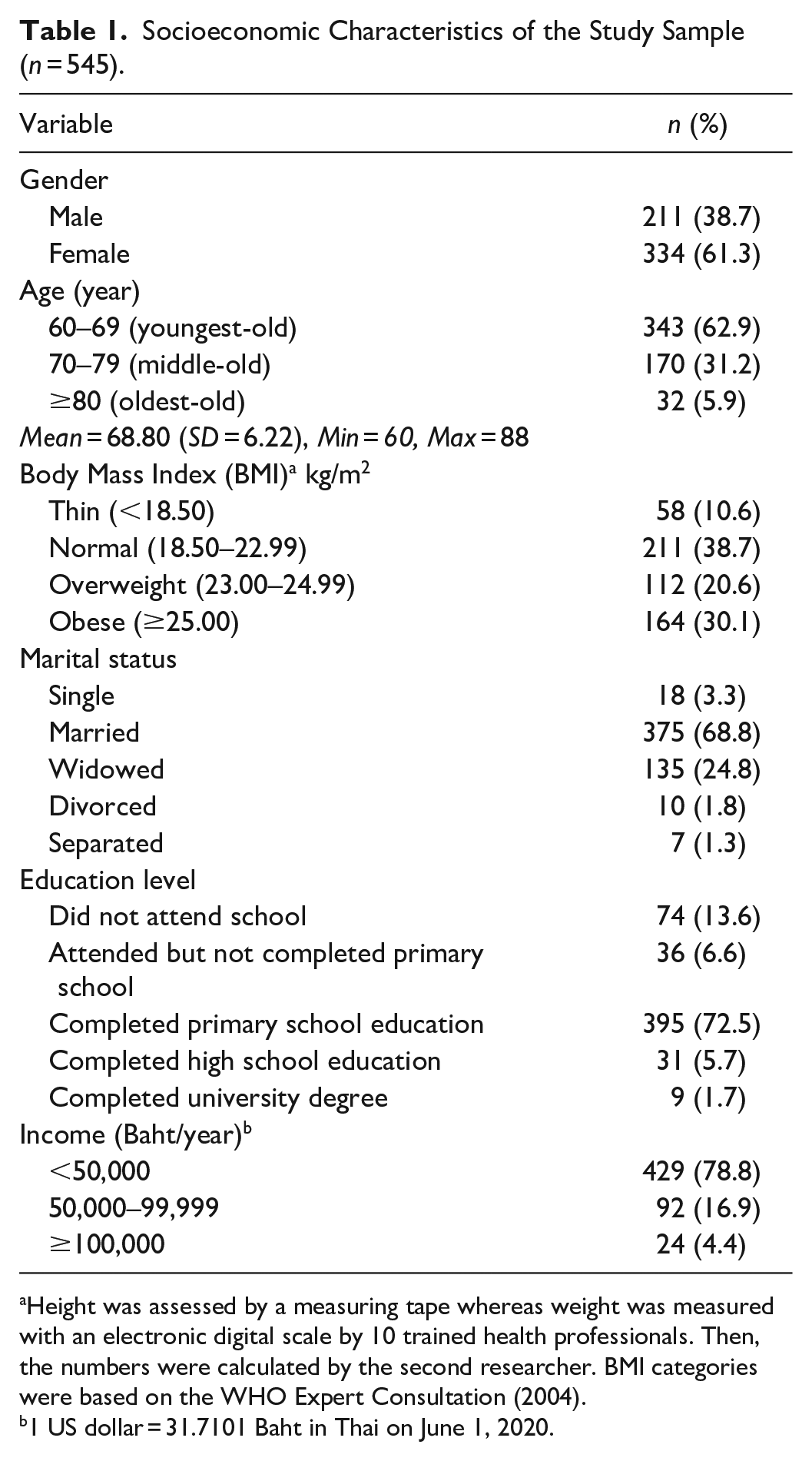
Height was assessed by a measuring tape whereas weight was measured with an electronic digital scale by 10 trained health professionals. Then, the numbers were calculated by the second researcher. BMI categories were based on the WHO Expert Consultation (2004).
1 US dollar = 31.7101 Baht in Thai on June 1, 2020.
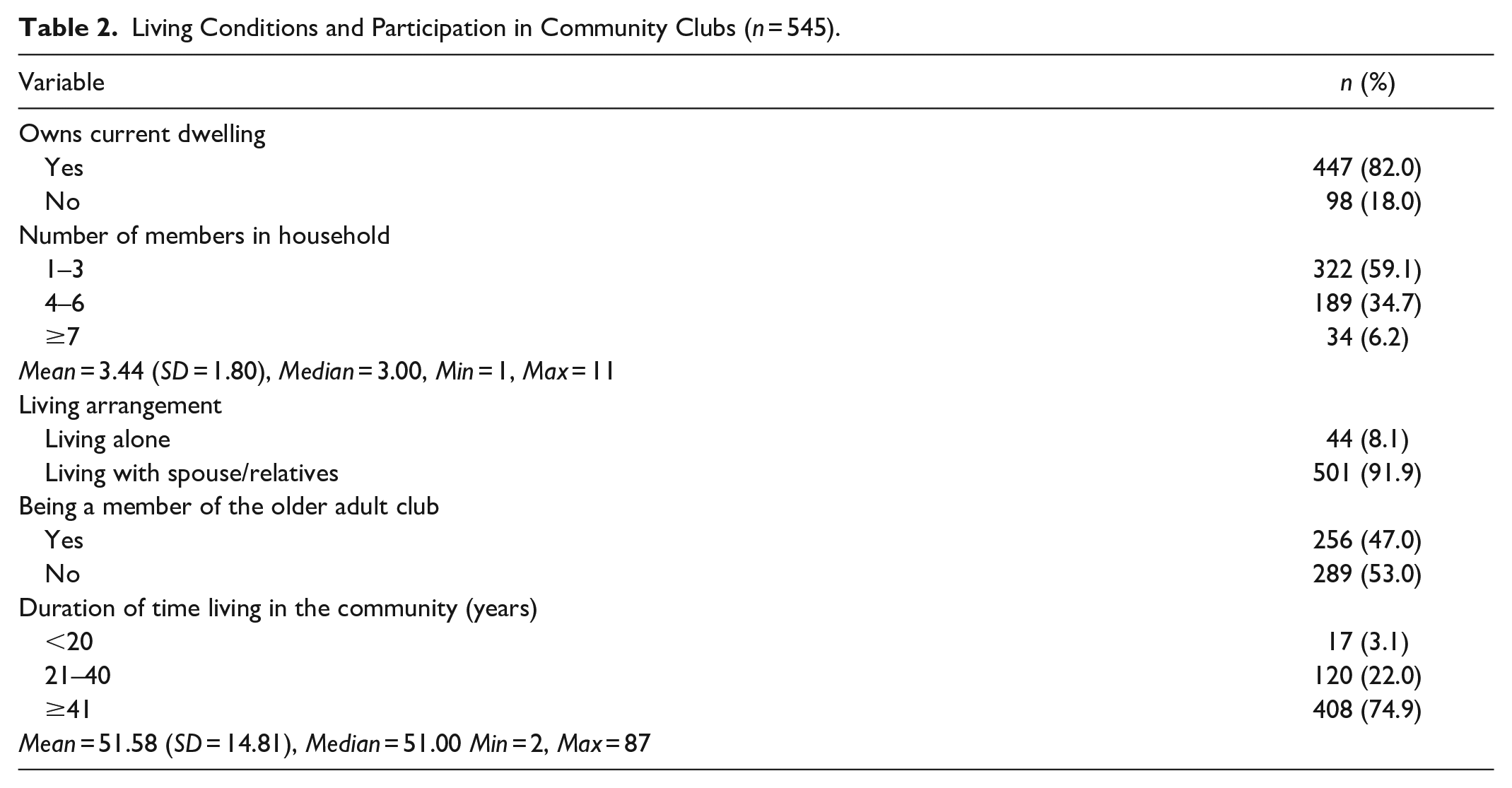
Table 2 shows the living conditions and participation in community clubs. The majority (82.0%) of older adults had their own current dwelling, with one-to-three household members (59.1%), followed by four-to-six members (34.7%). A small number of older people (8.1%) lived by themselves in their own homes. Regarding participation in the community, 47.0% of the participants engaged in a community club. The median parity of the duration of living in the community was 51 years (2–87), with the majority of participants (74.9%) reporting having lived in the community over 40 years.
Living Conditions and Participation in Community Clubs (n = 545).
Physical Activity
Table 3 shows the type and duration of exercise of older adults. The majority (44.0%) of older adults had high intensity. The duration of exercise in minutes per week is expressed as the mean and median of each activity.
Type and Duration of Exercise (n = 545).

Factors Associated With Physical Activity
The univariate analysis in Table 4 shows that seven characteristics were significantly related to adequate PA. These factors included the young-old, high level of income, being a member of a community club, high level of perceived self-efficacy, no education, high level of social support, and low level of perceived barriers to physical activity (p < .05).
Relationships Between Physical Activity Level and Participants’ Characteristics (n = 545).

Significant at alpha = .05 from chi square test.
The multivariate analysis with multiple logistic regression showed five statistically significant factors, including young-old, high level of income, being a member of a community club, not living in the community since birth, and high level of perceived self-efficacy (Table 5).
Crude and Adjusted Odds Ratio (OR) for Total Adequate Physical Activity According to the Independent Variables (n = 545).
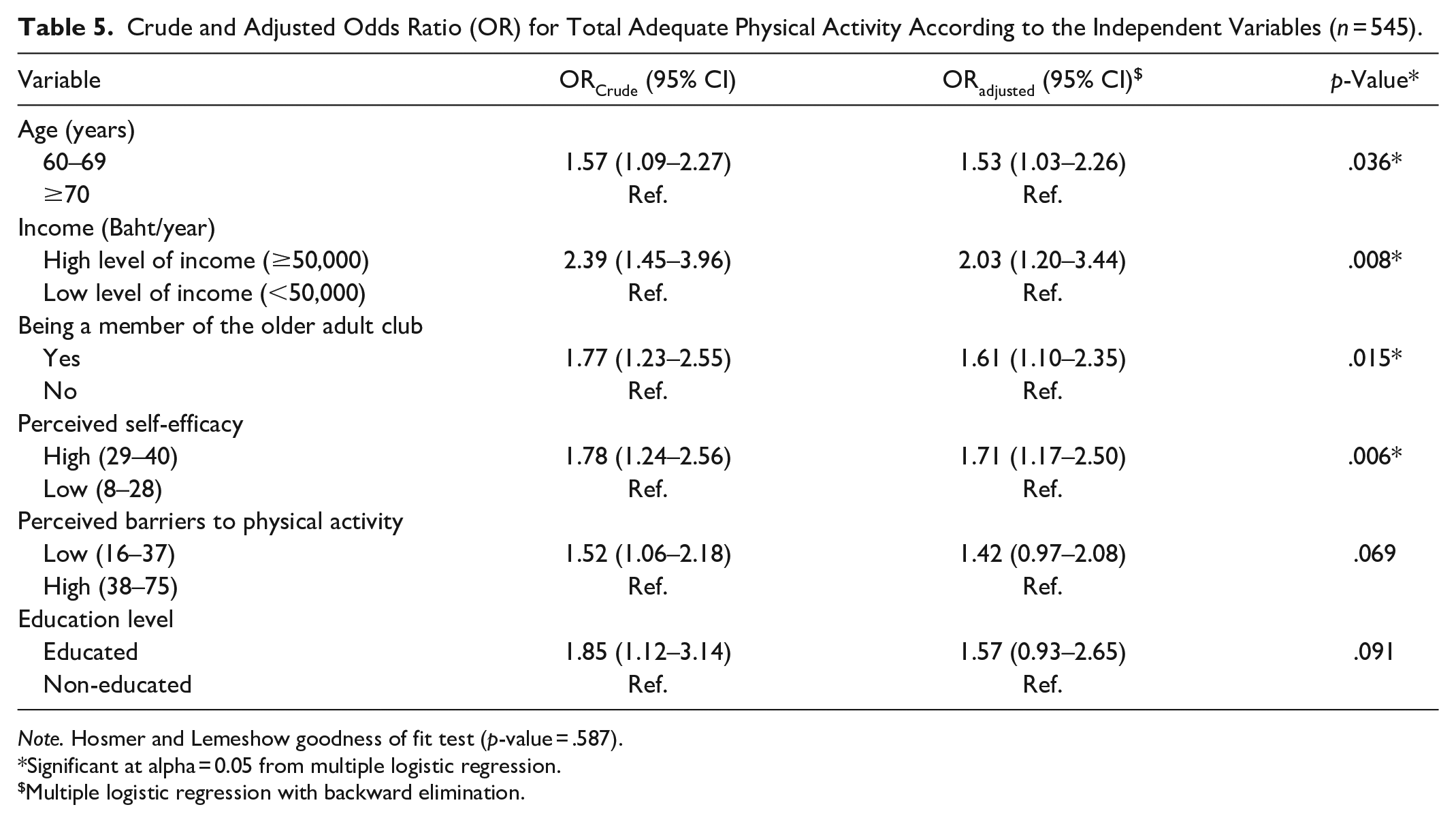
Note. Hosmer and Lemeshow goodness of fit test (p-value = .587).
Significant at alpha = 0.05 from multiple logistic regression.
Multiple logistic regression with backward elimination.
Discussion
The results suggest that 44% of older adults had high intensity PA. This finding can be explained with the availabilities of public exercise parks, and exercise equipment for people in the community of rural area by local organizations. This widens the access for older adults’ to work out in the community. This finding is consistent with a study by Olanrewaju et al. (2016) indicating that access and convenient scheduling are the key facilitators of PA. It suggests that local organizations in rural area should coordinate with the heath sector and invest budget for public exercise parks and exercise equipment related to social prescribing concept. This concept is an important way to expand the options available for health sector to provide individualized care for people’s physical and mental health through social interventions (Husk et al., 2019) As rural area is spacious and has equipment to PA, this tackles the health inequalities, especially for the poor to access PA.
Participants aged 60 to 69 years were 1.53 times (95% CI [1.03–2.26]) more likely to engage in PA than those aged 70 years and above. This might be explained by the physical nature of the aging process, that is, the reduction of muscle mass and muscle strength in both upper and lower limbs, change of fat-free mass, flexibility, agility, and endurance (Westerterp, 2018). This finding is in line with the previous literature (Maniragaba et al., 2019; Milanović et al., 2013; Ng et al., 2020; Takagi et al., 2015; Watson et al., 2016) which highlighted age-related decline in PA. Our finding supports the design of an appropriate program for PA, and the development of infrastructures and resources that promote exercise and active behaviors in aging adults, such as street accessibility, green areas, parks, and public transportation stations (Koohsari et al., 2018).
Regarding income, the findings indicated that a high level of income was 2.03 times (95% CI [1.20–3.44]) more associated with PA than a low level. Older adults with higher incomes had sufficient amount of money which could facilitate their time management and inclusion of PA. Those with lower levels of income needed to work to support their families which could hinder their availability of time to access to PA. In this study, it was confirmed that high level of income (≥50,000) was associated with adequate PA (81.0%). This finding aligns with the previous literature of Manz et al. (2018), and the Government of Canada (2018) which showed that those who had a higher socioeconomic status were more likely to engage in PA. However, this result is inconsistent with a previous study carried out in Thailand which found that older adults with high incomes tended to engage in sedentary behavior (Ethisan et al., 2017). Moreover, the meta-ethnographic analysis of qualitative studies found that financial constraints on affordability of exercise equipment, commitment of individuals in participating in sports, and perceived stigma for being below the poverty line were barriers that caused a low participation in PA (Rawal et al., 2020). As a result, more economical alternatives for PA as well as less time-consuming ones should be taken into consideration.
Participants who were members of the older adult club had 1.61 times (95% CI [1.10–2.35)]) more PA than those who did not belong to the older adult club. The reason for this finding might be that those older adults who are part of this club, communicate more actively and frequently with their peers (i.e., group members), which might result in a positive impact on the level of PA. This finding is in agreement with previous studies (Broderick et al., 2015; Geffen et al., 2019) showing that peer support is a social determinant of health, and may increase PA.
Finally, a high level of perceived self-efficacy was 1.71 times (95% CI [(1.17–2.50)]) more associated with PA than a low level of the same attribute. The older adults’ belief about their capabilities to perform PA seems to have association with their perception of what activities and situational demands can be classified as PA. As shown in our study, participants perceived that PA had benefits, and was not necessarily difficult. They also realized that moderate-intensity PA could include daily tasks like crop production, walking, cycling, folk dancing while vigorous-intensity activities could include jogging, Tai chi, and running. In agreement with the study of Notthoff et al. (2017), the perception of individual self-efficacy is positively correlated to PA levels in older adults.
Limitations of the Study
The strength of this study is the use of a cross-cultural translation and adaptation in Thai of the GPAQ (Notthoff et al., 2017; Visuthipanich, 2016; Visuthipanich et al., 2009). Nevertheless, there are some limitations to this study. The subjective nature of PA self-reports, instead of having more objective measures, such as pedometers, may have under-estimated the magnitude of the activity status of older adults (Ng et al., 2020). With the increase of smartphones among older adults in rural area (84.6%) (Pewnil, 2016), the measure of PA could be assessed more objectively in future study. The other limitation is that as this study was conducted in rural a community, the results can only be generalized to a similar geographic context. Further studies should aim to investigate barriers of PA, and design interventions to facilitate it, together with investigating its outcomes and maintaining adequate levels of PA for older adults.
Conclusion
In overall, the odds of engagement in PA could be predicted by certain factors, such as age between 60 and 69 years old, high level of income, being a member of the older adult club, and a high level of perceived self-efficacy. These findings have implications on the encouragement to provide PA among older people, including improving the physical attributes of the environment to increase accessibility, such as the development of exercise parks with equipments, and safety areas for senior cycling, and less time-consuming alternatives for PA, peer support networks and enhancing perceived self-efficacy.
Footnotes
Data Availability
The dataset supporting this article are available upon request from the corresponding author.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Considerations
This study was approved by the Naresuan University Ethical (COA No. 522/2018), and written informed consent was obtained from each subject before data collection.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Naresuan University [grant number NUAS 62-5].