
Abstract
To investigate the individual effectiveness of motivational interviewing, tailor-made interventions, social context-related interventions, shared decision making, and monitoring & feedback versus active- and passive control groups on physical activity level among older adults at short-, middle-, and long term. Secondary aim is to compare the effectiveness of interventions using a single motivational strategy versus interventions combining multiple motivational strategies. Literature search of PubMed, EMBASE, CINAHL, and PEDro databases using keywords and subject headings. Randomized controlled trials comparing two or more arms, with one arm focused on motivational strategies influencing physical activity were included. We identified 20,690 titles, of which 51 (comprising 11,596 participants) were included. Methodological quality and quality of evidence was evaluated using PEDro scale and GRADE approach. Outcomes were physical activity levels measured by objective- or subjective instruments at 3-, 6-, and 12 months follow-up. Standardized mean differences between intervention- and control groups were used as the mode of the analyses. For primary outcome, 6 months follow-up, pooled data demonstrated a statistically significant trend for higher effectiveness interventions using multiple motivational strategies compared with an active control intervention, while other singular motivational strategies did not show similar results for this comparison. The quality of the body of evidence was graded as very low for all motivational strategies. In our search, we have used broad in- and exclusion criteria for eligible studies regarding population characteristics resulting in a wide variety of conditions and illnesses included in our review which warrants a better representation of daily clinical practice. However, this led to data being pooled from a wide variety of different study populations and settings, content of interventions and outcome measures, increasing the heterogeneity of study characteristics. Interventions combining multiple motivational strategies show a trend to be more effective than using singular treatment strategies, although the optimal composition remains unclear.
Plain language summary
Purpose: This study aims to evaluate the effectiveness of interventions using motivational interviewing, tailor-made interventions, social context-related interventions, shared decision making, and monitoring & feedback versus active- and passive control groups on physical activity levels of older adults at 3-, 6-, and 12 months. Secondary aim is to compare the effectiveness of interventions using only one motivational strategy versus interventions combining multiple motivational strategies. Methods: Literature search of PubMed, EMBASE, CINAHL, and PEDro databases using keywords and subject headings related to older adults, the motivational strategies and physical activity. Methodological quality and quality of evidence was evaluated using PEDro scale and GRADE approach. Outcomes were physical activity levels measured by objective- or subjective instruments at 3-, 6-, and 12 months follow-up. Conclusions: Interventions combining multiple motivational strategies seem show a trend to be more effective than using singular treatment strategies, although the optimal composition remains unclear. Implications: Evidence is inconsistent, so the optimal combination of strategies remains unclear. Although more research is needed, The outcomes of this review can benefit the effectiveness of interventions by delivered by healthcare professionals in promoting physical activity among older adults. Limitations: Data were pooled from a wide variety of different study populations and settings, different content of interventions and outcome measures, which increased the heterogeneity of study characteristics.
Introduction
Physical activity is considered to have a positive effect on mobility and physical functioning in general, and especially among mobility-limited and/or physically disabled elderly patients (de Vries et al., 2012). However, older adults perceive physical, mental, and social-emotional barriers which represent obstacles to the adoption and maintenance of a physically active lifestyle. Health problems and pain emerge as the most frequently cited barriers to becoming and staying active (Chao et al., 2000). Another barrier of significant importance is the lack of knowledge and understanding of the relationship between physical activity and health. Among older adults with mobility problems and their social environment, physical activities are frequently perceived as unsafe, harmful and malign for their impairments, and therefore undesirable to perform (Burton et al., 1999). Because these perceptions of being physically active are often so ingrained in the older population, adoption and maintenance of a physically more active lifestyle pose serious challenges (Schutzer & Graves, 2004).
As the aging process advances, contact between older adults and healthcare providers intensifies. In general, older adults have great respect for health professionals and are greatly influenced by their advice. Therefore, healthcare providers can be the catalyst for older adults with mobility problems in achieving and maintaining a more physically active lifestyle (Schutzer & Graves, 2004). Addition of motivation enhancing strategies to the delivery of exercise and/or physical activity interventions appear to be promising in promoting and maintaining a physically more active lifestyle (McGrane et al., 2015; Williams et al., 2017).
For the development of an intervention promoting physical activity among older adults in the Netherlands, focus group discussions were held with older adults and experts in the fields of physical therapy, geriatric medicine and health promotion, to identify which motivational strategies are potentially useful in daily practice to promote and increase adherence to a physically active lifestyle (de Vries et al., 2015). The recommended strategies included: (1) motivational interviewing, (2) tailor-made interventions, (3) involvement of the patient’s social context, (4) shared decision making to determine the goals and content of the treatment, and (5) monitoring & feedback to inform the patient on their progress; either as individual- or in combined strategies. To date, systematically reviewed evidence on which of the aforementioned five strategies is optimal for improving physical activity among older adults is lacking. Such evidence, can support healthcare professionals to optimize their programs aimed to promote a physically active lifestyle on the short- and longer duration.
Therefore, the primary aim of this systematic review is to investigate the effectiveness of motivational interviewing, tailor-made interventions, context-related interventions, shared decision making, and monitoring & feedback individually on the physical activity level at the short-, middle-, and long-term. Secondary aim is to compare the effectiveness of interventions using those single individual motivational strategies with interventions combining multiple motivational strategies.
Methods
This systematic review and meta-analysis is conducted for the development of an intervention promoting physical activity among older adults using multiple motivational strategies and is reported according the Preferred Reporting Items for Systematic Reviews and Network Meta-Analyses statement (PRISMA) (Moher David, 2009). An a-priori written study protocol is registered at PROSPERO.
Search Strategy and Selection Criteria
The electronic databases MEDLINE, EMBASE, PEDro, and CINAHL were searched for eligible articles up to March 23rd 2023 to identify all relevant articles. Scientific literature was systematically searched combining key words related to “older adults,”“motivational interviewing,”“tailor-made interventions,”“shared decision making,”“feedback,”“context” and “physical activity.” The complete search strategy including MeSH terms and keywords can be found in Appendix A. The body of the search (population, outcome and Randomized Controlled Trial [RCT] Filter) was used for every search strategy, whereas the motivational strategy was used for the selective searches. Additionally, reference tracking was performed in all full-text included studies.
Articles were eligible for inclusion if (1) the design was an RCT, (2) the study was written in the English or Dutch language, (3) the study included older patients (on average 65 years or older) who were chronically ill and/or suffering from mobility problems, (4) the studied intervention promoted physical activity by use of either motivational interviewing, a tailor-made intervention, context-related interventions utilizing the social context of the patient (e.g., informal caregivers or peers), shared decision making, and/or monitoring & providing feedback on progression in addition to either physical activity or exercise interventions, and (5) the authors reported the quantity of physical activity measured by objective- (e.g., pedometers, accelerometers) and/or subjective instruments (e.g., questionnaires) at periods of either (or close to) 3-, 6-, or 12 months as outcome measure. Articles were excluded if (1) they included patients with a late stage of progressive- or severe neurological disorders and/or are in a palliative phase, (2) the intervention did not aim to alter physical activity levels, or (3) the intervention consisted of only telerehabilitation methods (such as text-messaging or internet) without any face-to-face contact. Two pairs of reviewers independently searched for eligible articles. Initially, articles were screened for eligibility on title and abstract using Rayyan systematic review software (Ouzzani et al., 2016). If titles and abstracts implied an article was potentially eligible for inclusion, a full paper copy of the report was obtained. Disagreements between the reviewers regarding eligibility were resolved in a consensus meeting. Outcome of the study was the effectiveness of the motivational strategies (motivational interviewing, tailored-made interventions, shared decision making, monitoring and feedback, social context related interventions) on short-term (<3 months), middle-term (<6 months), and long-term (±12 months) physical activity behavior of older adults aged 65 and older.
Data Extraction
WH and LS independently extracted data using a standardized extraction form. Data extracted from the included articles were: (1) authors, publication year, and study location, (2) study design, (3) participants and characteristics, (4) intervention characteristics, (5) outcome measures, and (6) study results. For controls, we made a distinction between active- and passive control groups. Interventions were categorized as active control when exercise was promoted without the explicit utilization of any of the treatment strategies, such as regular care or a standardized exercise prescription. Controls were categorized as passive if no physical activity promotion was actively delivered, such as a passive waiting-list or handing out a pamphlet with general information. For our outcome measures, the quantity of physical activity measured by objective- (e.g., pedometers, accelerometers), and/or subjective instruments (e.g., questionnaires), mean scores and standard deviations (SDs) were extracted for both intervention and control groups at the following follow-up points: baseline, short term follow-up around 3 months (up to 14 weeks), middle term follow-up around 6 months (between 15 and 36 weeks), and long term follow-up around 12 months (between 37 and 60 weeks). If a study presented more follow-up points within the predefined timeframe, we extracted the follow-up point closest to 3, 6, or 12 months follow-up. If a study presented physical activity measured with both objective- and subjective instruments, we used the results of the subjective instruments (e.g., questionnaires) in our analyses since many objective instruments tend to underestimate physical activity measurements while walking due to aberrant walking patterns.
In case data were missing or further information was required, attempts were made to contact the corresponding author. If unsuccessful, missing data on means and SDs were, if possible, calculated in case adequate data were available (Li et al., 2019). In case data were only presented in figures, we extracted these data using WebPlotDigitizer (Rohatgi, 2019).
Data Analysis
For the primary analysis, conventional meta-analyses were performed based on studies using the same motivational strategy, measuring the same outcome and providing the mean and standard deviation of the outcome variables at either one of the different follow-up points (short-, middle-, and long term follow-up), in order to understand the between-group effects. Between group follow-up scores were included if no between group change scores were reported (da Costa et al., 2013). Intervention- or control groups (≥2 groups) were combined to create a single pair-wise comparison according to the recommendations of the Cochrane Handbook, if appropriate (Higgins et al., 2019). If three or more motivational strategies were combined into a single approach, interventions were defined as using multiple motivational strategies. Some motivational strategies are often delivered in combination with (elements of) another motivational strategy but cannot be considered as multiple strategies combined in one intervention, for example, providing feedback on a tailor-made treatment goal, and are therefore categorized in the main motivational strategy. The results of the meta-analysis are presented by forest plots using RevMan software (Review-Manager & (RevMan), 2020). Continuous outcomes are expressed as standardized mean differences (SMD) with corresponding 95% confidence intervals (95% CI). The I2 index was used to test the heterogeneity of the selected studies (Cumpston et al., 2019).
Network meta-analyses were conducted between types of interventions to study the relative effectiveness between motivational strategies. The different interventions were categorized based on the main motivational strategy described in the content of the intervention. Available direct comparisons between different motivational strategies and control groups were illustrated using network plots (netgraphs) consisting of nodes and lines representing interactions between studies (Chaimani et al., 2013). For the network meta-analysis, we assumed that there were no systematic differences between the available comparisons other than the treatments being compared, and studies were evaluated by comparing similarities of included study populations in terms of age, gender ratio, study location and content of the intervention (Schwingshackl et al., 2019). Potential inconsistency between studies was assessed by splitting effect estimates into direct- and indirect evidence and testing whether they differed. For all outcomes mean differences were calculated. All potential comparisons were calculated via RStudio version 3.6.2 and are presented as SMDs and 95% CI. Network meta-analyses were performed in a contrast-based framework using the R package ‘netmeta’ version 1.1 (Rücker et al., 2021).
Methodological Quality and Quality of Body of Evidence
Methodological quality of the included studies was evaluated using the PEDro scale (Maher et al., 2003). The PEDro scale comprises 11 dichotomous items (i.e., yes/no) measuring the methodological quality of an RCT (e.g., blinding, concealment, random allocation, baseline similarity, dropout). Except for the first item (i.e., specified eligibility criteria), the remaining 10 items sum up to a total score, where higher scores indicate a higher quality level (Moseley et al., 2019). If available, PEDro scores of included articles were obtained from the official PEDro database (Verhagen et al., 1998). If not, the scoring was performed by WH and LS, who resolved disagreements in a consensus meeting. PEDro scores ranged from 3 to 8 points, with a median of 6, see Table 1 and Appendix B. Ten studies scored ≤4. Methodological limitations were related to unclear allocation concealment (40 out of 64 studies), no blinding of subjects (60 out of 64 studies), no blinding of therapists (53 out of 64 studies), no blinding of assessors (32 out of 64 studies), no adequate follow-up (28 out of 64 studies), and no intention-to-treat analysis (27 out of 64 studies).
Methodological Quality of the Included Studies.

Note. One point was awarded when a criterion was clearly satisfied (+ = 1 point was awarded, − = criterion was not satisfied). Item 1 was not used to calculate the PEDro score. Scores range from 0 to 10. The criteria are defined as follows: (1) eligibility criteria were specified; (2) participants were randomly allocated to groups; (3) allocation was concealed; (4) the groups were similar at baseline regarding the most important prognostic indicators; (5) there was blinding of all participants; (6) there was blinding of all therapists who administered the intervention; (7) there was blinding of all assessors who measured at least one key outcome; (8) measures of at least one key outcome were obtained from >85% of the participants initially allocated to groups; (9) all participants from whom outcome measures were available received the treatment of control condition as allocated or, where this was not the case, data for at least one key outcome was analyzed by intention-to-treat analysis; (10) the results of between-group statistical comparisons are reported for at least one key outcome; and (11) the study provides both point measures and measures of variability for at least one key outcome.
aClare 2015 is included in both motivational interviewing and interventions using multiple motivational strategies, because in this study one intervention focuses on motivational interviewing and one intervention focuses on multiple motivational strategies.
Quality of evidence across studies was assessed using the Grading of Recommendations, Assessment, Development and Evaluation (GRADE) approach (Schünemann et al., 2013), which focuses on five domains: limitations of design, inconsistency of results, indirectness, imprecision, and publication bias. Considering these domains, the quality of evidence was assessed for each outcome. For description of GRADE levels see Box 1 (Schünemann et al., 2013). High risk of bias (Guyatt, Oxman, Vist, et al., 2011), inconsistency of results (Guyatt, Oxman, Kunz, Woodcock, Brozek, Helfand, Alonso-Coello, Glasziou, et al., 2011), indirect evidence (Guyatt, Oxman, Kunz, Woodcock, Brozek, Helfand, Alonso-Coello, Falck-Ytter, et al., 2011), imprecise results (Guyatt, Oxman, Kunz, Brozek, et al., 2011), and/or publication bias (Guyatt, Oxman, Montori, et al., 2011) resulted in downgrading the evidence by one or two levels. Grading was performed by LS and verified by WH. For the network meta-analysis, the quality of evidence was assessed using the extension of the GRADE approach (Salanti et al., 2014). In this GRADE extension, the domain transitivity was also assessed. Transitivity requires all competing interventions of a systematic review to be jointly randomizable. Violation of transitivity threatens the validity of both indirect and combined estimates. Therefore, if we lack convincing evidence for the plausibility of the transitivity assumption, we downgraded each pairwise comparison as well as the ranking of the treatments by one level (Salanti et al., 2014).
GRADE Levels Describing the Quality of the Body of Evidence.

Results
The flow of the systematic review and meta-analysis is presented in Figure 1. The electronic database search yielded 23,425 records after duplicates were removed. The screening of titles and abstracts resulted in 346 full-text records. Following full-text review, 64 studies were included in this systematic review. In the meta-analyses, 51 studies were included and in the network meta-analysis 39 studies were included. Of the included studies, four studies reported data about the two same interventions within the same population however they reported their results based on different follow-up points (Arkkukangas et al., 2019; Frändin et al., 2016; Grönstedt et al., 2013; Tuvemo Johnson et al., 2021), therefore the study characteristics were extracted on the basis of one study (Arkkukangas et al., 2019; Grönstedt et al., 2013).
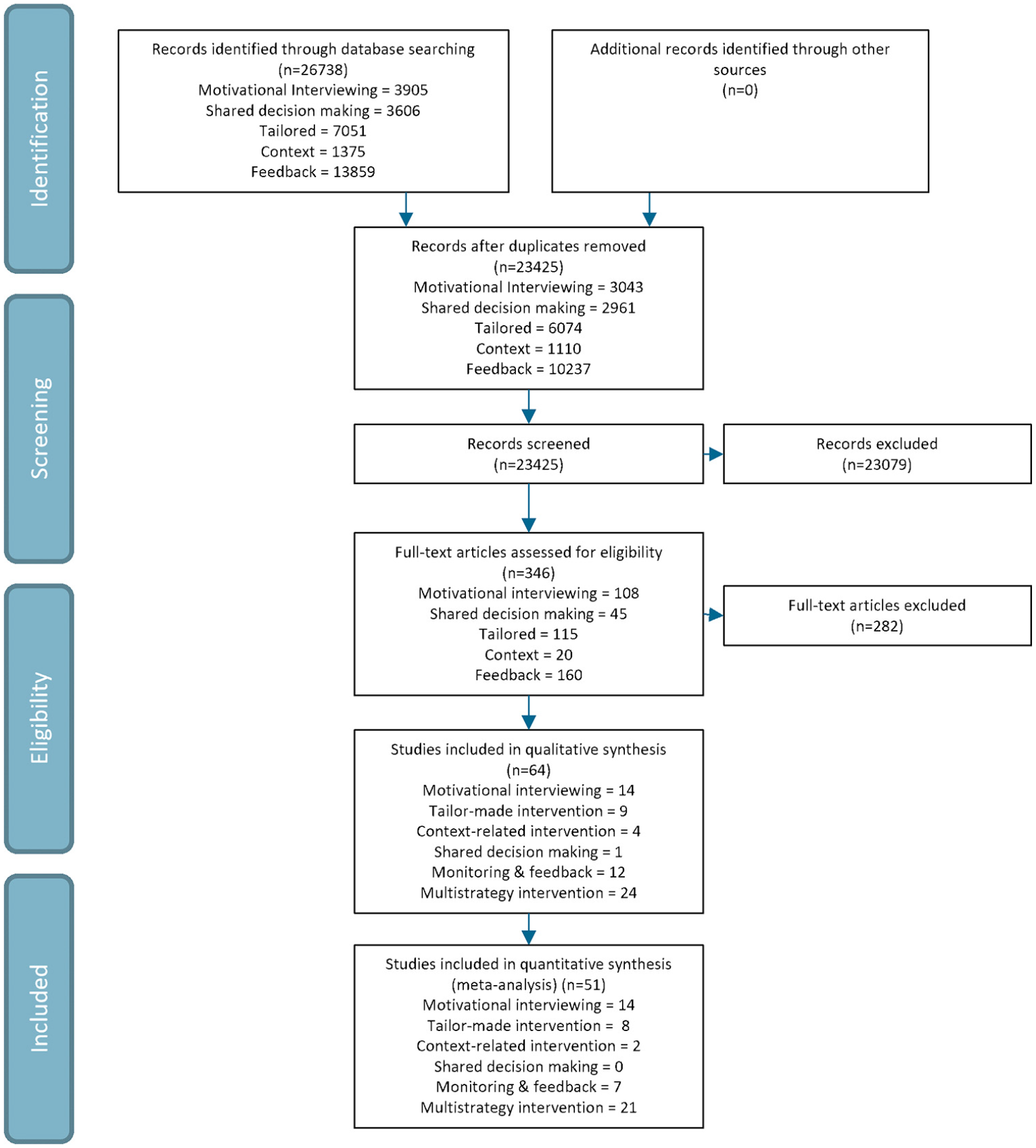
Flow chart. Note that there are duplicates found for different individual motivational strategies. Therefore the sum of for instance all full-text articles differ from the amount which is reported in the flow chart. In the flow chart the sum without duplicates is reported.
Population Characteristics
Sample size of included studies ranged from 15 to 1,734 with a total of 13,619 participants (4,537 men). Study duration ranged from 4 weeks to 12 months. The mean age of all participants was 69 years (SD 6.3) (two studies did not report a mean age (Harris et al., 2015; Siltanen et al., 2020). In 35 studies the range of inclusion was <65 years but the mean age of the people who were actually included was ≥65 years (Bragonzoni et al., 2023; Cabral et al., 2022; Cai et al., 2022; Chang et al., 2023; Cheng et al., 2022; Christiansen et al., 2020; Clare et al., 2015; Cox et al., 2021; Crist et al., 2022; Croteau et al., 2007; de Blok et al., 2006; Gellert et al., 2014; Gillison et al., 2015; Harris et al., 2015; Hornikx et al., 2015; Ismail et al., 2020; Khunti et al., 2021; Lang et al., 2018; Lewis et al., 2020; Lyden et al., 2021; Mackey et al., 2019; Nguyen et al., 2019; Oliveira et al., 2019; Peel et al., 2016; Petrella et al., 2010; Pfeiffer et al., 2020; Piedra et al., 2018; Pinto et al., 2005; Rausch Osthoff et al., 2021; Resnick et al., 2008; Sazlina et al., 2015; Suwanpasu et al., 2014; Turunen et al., 2020; Van Hoecke et al., 2014; Wootton et al., 2019). A detailed description of included studies (n = 65) is presented in Table 2.
Study Characteristics of Included Studies.

Note. NR = not reported.Italic text defines whether the publication is using an active- or passive control group as defined in the methods section.
aUsed timepoints in analyses and narrative results are underlined.
bClare 2015 is included in both motivational interviewing and interventions using multiple motivational strategies, because in this study one intervention focuses on motivational interviewing and one intervention focuses on multiple motivational strategies.
Twenty-four studies included (community-dwelling) older adults (Arkkukangas et al., 2019; Barrows, 2018; Cai et al., 2022; Chang et al., 2023; Clare et al., 2015; Crist et al., 2022; Croteau et al., 2007; De Greef et al., 2011; Gellert et al., 2014; Harris et al., 2015; Herghelegiu et al., 2017; Kerr et al., 2018; Koizumi et al., 2009; Lewis et al., 2020; Mackey et al., 2019; Morey et al., 2009; Oliveira et al., 2019; Peel et al., 2016; Pfeiffer et al., 2020; Piedra et al., 2018; Resnick et al., 2008; Siltanen et al., 2020; Suikkanen et al., 2021; Suwanpasu et al., 2014; Turunen et al., 2020; Tuvemo Johnson et al., 2021), of which seven studies additionally specified their inclusion to older adults with diabetes (De Greef et al., 2011), a musculoskeletal injury or disorder (Turunen et al., 2020), a diagnosis of a polyp or adenoma (Lewis et al., 2020), at risk for cardiovascular disease (Barrows, 2018), admitted to post-acute care (Peel et al., 2016), and hip fractures (Pfeiffer et al., 2020; Suwanpasu et al., 2014), respectively. Fifteen studies specified their inclusion of only inactive (community-dwelling) older adults (Cabral et al., 2022; Cohen-Mansfield & Sommerstein, 2019; Cox et al., 2021; de Vries et al., 2016; Heij et al., 2022; Matz-Costa et al., 2018; McMahon et al., 2017; Petrella et al., 2010; Pinto et al., 2005; Sazlina et al., 2015; Stewart et al., 2001; Sugden et al., 2008; Thompson et al., 2014; Van Hoecke et al., 2014; Warner et al., 2016) of which one study specified the inclusion to inactive older adults with diabetes type 2 (Sazlina et al., 2015). In total sixteen studies focused on patient populations: seven studies included patients with Chronic Obstructive Pulmonary Disease (Cheng et al., 2022; de Blok et al., 2006; Hornikx et al., 2015; Kawagoshi et al., 2015; Nguyen et al., 2019; Rausch Osthoff et al., 2021; Wootton et al., 2019), two studies included patients with a high cardiovascular risk (Gillison et al., 2015; Ismail et al., 2020), one study included patients after unilateral total knee replacement (Christiansen et al., 2020), three studies included patients with heart failure (Brodie & Inoue, 2005; Lang et al., 2018; Witham et al., 2012), one study included patients with intermittent claudication (Cunningham et al., 2012), two articles reported on one study including nursing home residents (Frändin et al., 2016; Grönstedt et al., 2013), one study included patients with stage 2 Chronic Kidney Disease (Lyden et al., 2021) and three studies included patients with a probable Alzheimer’s disease or mild dementia/cognitive impairment (Cabral et al., 2022; Goldberg et al., 2019; Steinberg et al., 2009). In eight studies, the predefined in- and exclusion criteria were not targeted to older adults at all (Babazono et al., 2007; Bragonzoni et al., 2023; Cheng et al., 2022; Cunningham et al., 2012; Khunti et al., 2021; Lang et al., 2018; Lyden et al., 2021; Rausch Osthoff et al., 2021). Of all studies, 28 studies reported additional in- and exclusion criteria regarding functional mobility and/or health parameters (additional to or other than being inactive) (Arkkukangas et al., 2019; Babazono et al., 2007; Bragonzoni et al., 2023; Brodie & Inoue, 2005; Cai et al., 2022; Crist et al., 2022; Croteau et al., 2007; De Greef et al., 2011; Gillison et al., 2015; Harris et al., 2015; Ismail et al., 2020; Kawagoshi et al., 2015; Kerr et al., 2018; Khunti et al., 2021; Koizumi et al., 2009; Lewis et al., 2020; Lyden et al., 2021; McMahon et al., 2017; Morey et al., 2009; Nguyen et al., 2019; Oliveira et al., 2019; Peel et al., 2016; Piedra et al., 2018; Resnick et al., 2008; Siltanen et al., 2020; Steinberg et al., 2009; Suikkanen et al., 2021; Tuvemo Johnson et al., 2021).
Description of Intervention- and Control Conditions
Fourteen studies evaluated interventions with motivational interviewing in adults (on average) 65 year or older (Babazono et al., 2007; Brodie & Inoue, 2005; Clare et al., 2015; Cunningham et al., 2012; de Blok et al., 2006; De Greef et al., 2011; Gellert et al., 2014; Hornikx et al., 2015; Ismail et al., 2020; McMahon et al., 2017; Pinto et al., 2005; Rausch Osthoff et al., 2021; Sugden et al., 2008; Warner et al., 2016). Nine studies provided a tailor-made intervention (Chang et al., 2023; Frändin et al., 2016; Grönstedt et al., 2013; Petrella et al., 2010; Resnick et al., 2008; Suikkanen et al., 2021; Turunen et al., 2020; Van Hoecke et al., 2014; Witham et al., 2012), four studies provided an intervention utilizing the patient’s social context (Barrows, 2018; Cohen-Mansfield & Sommerstein, 2019; Lang et al., 2018; Steinberg et al., 2009), one study was found providing shared decision making (Khunti et al., 2021), and twelve studies provided an intervention based on monitoring & feedback (Bragonzoni et al., 2023; Christiansen et al., 2020; Cox et al., 2021; Herghelegiu et al., 2017; Kawagoshi et al., 2015; Koizumi et al., 2009; Lyden et al., 2021; Nguyen et al., 2019; Peel et al., 2016; Sazlina et al., 2015; Thompson et al., 2014; Wootton et al., 2019). Twenty-four studies provided an intervention using multiple motivational strategies (≥ three motivational strategies) (Arkkukangas et al., 2019; Cabral et al., 2022; Cai et al., 2022; Cheng et al., 2022; Clare et al., 2015; Crist et al., 2022; Croteau et al., 2007; de Vries et al., 2016; Gillison et al., 2015; Goldberg et al., 2019; Harris et al., 2015; Heij et al., 2022; Kerr et al., 2018; Lewis et al., 2020; Mackey et al., 2019; Matz-Costa et al., 2018; Morey et al., 2009; Oliveira et al., 2019; Pfeiffer et al., 2020; Piedra et al., 2018; Siltanen et al., 2020; Stewart et al., 2001; Suwanpasu et al., 2014; Tuvemo Johnson et al., 2021).
Intervention duration ranged from 2.5 weeks to 12 months of which the majority (14 studies) had a duration of 12 weeks (Arkkukangas et al., 2019; Croteau et al., 2007; De Greef et al., 2011; Goldberg et al., 2019; Harris et al., 2015; Koizumi et al., 2009; Lang et al., 2018; Mackey et al., 2019; Morey et al., 2009; Pinto et al., 2005; Rausch Osthoff et al., 2021; Sazlina et al., 2015; Steinberg et al., 2009; Sugden et al., 2008). In four studies the intervention duration varied and depended on the need and physical functioning of the patient (de Vries et al., 2016; Frändin et al., 2016; Grönstedt et al., 2013; Heij et al., 2022). Eight studies did not clearly specify the intervention period (Barrows, 2018; Clare et al., 2015; Cunningham et al., 2012; de Blok et al., 2006; Gellert et al., 2014; Petrella et al., 2010; Resnick et al., 2008; Stewart et al., 2001). The number of sessions ranged from 2 to 104 sessions with a median of six sessions. Duration of sessions ranged from 30 min to 3 hr. Furthermore, sessions were provided individually, in a group, or a combination of individual- and group sessions, and were provided face-to-face or combined with telephone contact. For a detailed description per study, see Table 2.
In twelve studies, a (trained or experienced) physical therapist provided the intervention (Arkkukangas et al., 2019; Cheng et al., 2022; Christiansen et al., 2020; de Blok et al., 2006; de Vries et al., 2016; Heij et al., 2022; Hornikx et al., 2015; Kawagoshi et al., 2015; Lyden et al., 2021; Oliveira et al., 2019; Peel et al., 2016; Pfeiffer et al., 2020; Rausch Osthoff et al., 2021; Suikkanen et al., 2021; Turunen et al., 2020; Tuvemo Johnson et al., 2021; Witham et al., 2012; Wootton et al., 2019). In other studies, interventions were supervised by trained professionals for example, psychologists (Cai et al., 2022; Cunningham et al., 2012; De Greef et al., 2011; Steinberg et al., 2009; Warner et al., 2016), coaches (Gillison et al., 2015; Mackey et al., 2019; Morey et al., 2009; Nguyen et al., 2019; Pinto et al., 2005; Siltanen et al., 2020; Van Hoecke et al., 2014), nurses (Brodie & Inoue, 2005; Chang et al., 2023; Harris et al., 2015; Lang et al., 2018; McMahon et al., 2017; Sugden et al., 2008), nurses in combination with a certified yoga instructor (Barrows, 2018), physical activity teachers (Cohen-Mansfield & Sommerstein, 2019; Resnick et al., 2008), (specialized) physicians (Herghelegiu et al., 2017; Petrella et al., 2010), a multidisciplinary team (Babazono et al., 2007), by a physical- and occupational therapist (Frändin et al., 2016; Grönstedt et al., 2013), and by a physical-, and occupational therapist combined with a rehabilitation support worker (Goldberg et al., 2019). In ten studies the affiliation of the supervisor of the intervention was not clearly specified: “trained staff” (Bragonzoni et al., 2023; Cabral et al., 2022; Crist et al., 2022; Kerr et al., 2018; Stewart et al., 2001), “facilitator” (Cox et al., 2021; Croteau et al., 2007; Ismail et al., 2020; Khunti et al., 2021; Matz-Costa et al., 2018; Piedra et al., 2018), “counselor” (Thompson et al., 2014), “exercise specialist” (Lewis et al., 2020), or not specified at all (Clare et al., 2015; Gellert et al., 2014; Koizumi et al., 2009; Sazlina et al., 2015; Suwanpasu et al., 2014). In one study, the intervention was provided by a physical therapist and unspecified “pulmonary rehabilitation staff” (Kawagoshi et al., 2015). Three studies used peer mentors additionally to the supervision by healthcare professionals (Kerr et al., 2018; Matz-Costa et al., 2018; Sazlina et al., 2015).
In nineteen studies, the control groups consisted of usual care (Brodie & Inoue, 2005; Christiansen et al., 2020; Cunningham et al., 2012; de Blok et al., 2006; De Greef et al., 2011; de Vries et al., 2016; Frändin et al., 2016; Gillison et al., 2015; Grönstedt et al., 2013; Harris et al., 2015; Heij et al., 2022; Kawagoshi et al., 2015; Khunti et al., 2021; Lang et al., 2018; Lewis et al., 2020; Morey et al., 2009; Nguyen et al., 2019; Peel et al., 2016; Pfeiffer et al., 2020; Rausch Osthoff et al., 2021; Resnick et al., 2008; Sazlina et al., 2015; Turunen et al., 2020; Witham et al., 2012). In other studies, control groups consisted of providing information (Arkkukangas et al., 2019; Chang et al., 2023; Hornikx et al., 2015; McMahon et al., 2017; Oliveira et al., 2019; Pinto et al., 2005; Siltanen et al., 2020; Steinberg et al., 2009; Sugden et al., 2008; Suwanpasu et al., 2014; Tuvemo Johnson et al., 2021), an informative session (Cai et al., 2022; Cox et al., 2021; Crist et al., 2022; Van Hoecke et al., 2014), personalized information (Babazono et al., 2007; Clare et al., 2015; Goldberg et al., 2019; Kerr et al., 2018; Lyden et al., 2021; Petrella et al., 2010), instructions to continue normal daily activity pattern (Cabral et al., 2022; Koizumi et al., 2009; Suikkanen et al., 2021), physical activity class (Cohen-Mansfield & Sommerstein, 2019; Ismail et al., 2020; Piedra et al., 2018), yoga sessions (Barrows, 2018), support with determining general activity goal (Gellert et al., 2014), technology-assisted self-monitoring of activity (Matz-Costa et al., 2018), coaching and supervision during group training exercise sessions (Bragonzoni et al., 2023), phone calls to monitor health status (Cheng et al., 2022), no instructions or exercise training at all (Wootton et al., 2019), and waitlist control group (Croteau et al., 2007; Herghelegiu et al., 2017; Mackey et al., 2019; Stewart et al., 2001; Thompson et al., 2014). One study included two control groups; usual care and information (Warner et al., 2016). In meta-analyses the content of the control group was assigned to an active- or passive control group, see Table 2 for this distinction per study.
Evidence Synthesis
Interventions with Motivational Interviewing
For short-, middle-, and long term follow-up (on average 3, 6, and 12 months), respectively six (de Blok et al., 2006; De Greef et al., 2011; McMahon et al., 2017; Rausch Osthoff et al., 2021; Sugden et al., 2008; Warner et al., 2016), five (Brodie & Inoue, 2005; Cunningham et al., 2012; Gellert et al., 2014; McMahon et al., 2017; Rausch Osthoff et al., 2021), and five studies (Babazono et al., 2007; Clare et al., 2015; Gellert et al., 2014; Ismail et al., 2020; Warner et al., 2016) compared interventions with motivational interviewing to active control groups. All studies were pooled, while intervention groups were combined for five studies (Brodie & Inoue, 2005; De Greef et al., 2011; Ismail et al., 2020; McMahon et al., 2017; Warner et al., 2016). In one study we included one intervention group out of two (goal setting group, see Table 2) in the meta-analyses for motivational interviewing interventions (Clare et al., 2015). A comparison versus passive control groups at short-, middle-, and long term follow-up was done in three (Hornikx et al., 2015; Pinto et al., 2005; Warner et al., 2016), one (Pinto et al., 2005), and one study (Warner et al., 2016), respectively, while only results of the three studies for short term follow-up were pooled. Therefore, change scores were included for one study (Hornikx et al., 2015). For one study, we included the usual care group as active control group, and the information group as passive control group in meta-analyses for motivational interviewing as intervention (Warner et al., 2016).
Analysis of the pooled effect of motivational interviewing versus active control at short term follow-up in terms of physical activity resulted in a SMD of −0.07 (95% CI [−0.27, 0.12]), for middle- and long term follow-up SMDs of 0.06 [−0.16, 0.28] and 0.19 [−0.05, 0.43] were found, respectively (Figure 2). For motivational interviewing versus passive control group a SMD of −0.10 [−0.44, 0.25] (Figure 3) at short term follow-up was found, while for middle- and long term follow-up no significant difference were found (Pinto et al., 2005; Warner et al., 2016).

Motivational interviewing versus active control group at short-, middle-, and long term follow-up.
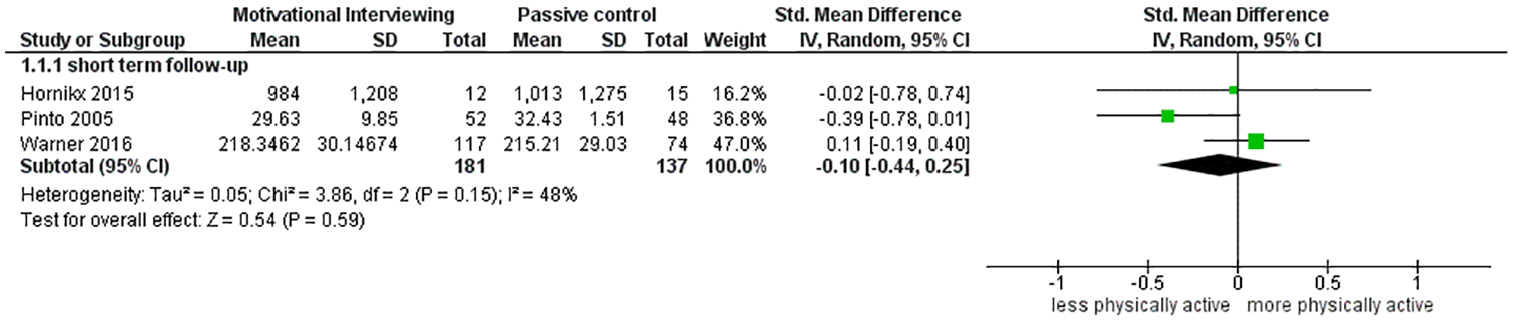
Motivational interviewing versus passive control group at short term follow-up.
Due to very low quality of evidence at all follow-up points of both comparisons with active- (short term: very serious risk of bias, very serious inconsistency, serious indirectness; middle term: very serious risk of bias, very serious inconsistency, very serious indirectness; and long term: very serious risk of bias, serious inconsistency, serious indirectness) and passive control groups (short term: very serious risk of bias, serious inconsistency, serious indirectness, serious imprecision; middle term: serious risk of bias, very serious imprecision; and long term: very serious risk of bias, very serious imprecision), we are uncertain whether interventions with motivational interviewing can improve level of physical activity. See Table 3 and Appendix C.
GRADE Overview Table for the Outcome Physical Activity at Time Points 3, 6, and 12 months Follow-Up, Ordered Per Research Question and Group Comparison. Reasons for Downgrading can be Found in Appendix D.

Tailor-Made Interventions
For short-, middle-, and long term follow-up, five (Grönstedt et al., 2013; Suikkanen et al., 2021; Turunen et al., 2020; Van Hoecke et al., 2014; Witham et al., 2012), four (Frändin et al., 2016; Suikkanen et al., 2021; Turunen et al., 2020; Witham et al., 2012), and three studies (Petrella et al., 2010; Suikkanen et al., 2021; Van Hoecke et al., 2014) reported tailor-made interventions versus active control group, respectively. For short-, middle, and long term follow-up four, three, and three studies were pooled, respectively. We included change scores of four studies (Frändin et al., 2016; Grönstedt et al., 2013; Petrella et al., 2010; Van Hoecke et al., 2014). Intervention groups were combined for one study (Van Hoecke et al., 2014). For tailor-made intervention versus passive control group, two studies (Chang et al., 2023; Resnick et al., 2008) were found for short term follow-up.
Analysis of the pooled effect of a tailor-made intervention versus active control at short term follow-up in terms of physical activity resulted in a SMD of 0.27 (95% CI [−0.14, 0.67]), for middle-, and long term follow-up a SMDs of 0.38 [−0.35, 1.12] and 0.45 [0.18, 0.73] were found, respectively (Figure 4). Three studies were not included in meta-analyses. The authors of one study were no longer able to provide the requested data for the meta-analyses (Witham et al., 2012). Data for short- and middle term follow-up were in line with pooled data (Witham et al., 2012). One study reported no significant difference in physical activity between intervention and active control group in mean change from baseline to middle term follow-up (Frändin et al., 2016). Another study reported no significant difference in overall physical activity between the intervention and passive control group at short term follow-up (Resnick et al., 2008). For a tailor-made intervention versus passive control a SMD of 0.22 [−0.08, 0.52] (Figure 5) at short term follow-up was found. Due to very low quality of evidence at all measurement points of both comparisons with active- (short term: very serious risk of bias, very serious inconsistency, very serious indirectness; middle term: very serious risk of bias, serious inconsistency, very serious indirectness, serious imprecision; and long term: very serious risk of bias, serious indirectness) and passive control groups (short term: very serious risk of bias, serious inconsistency, serious indirectness, and very serious imprecision), we are uncertain whether tailor-made interventions can improve level of physical activity. See Table 3 and Appendix C.

Tailor-made intervention versus active control group at short-, middle-, and long term follow-up.

Tailor-made intervention versus passive control group at short term follow-up.
Interventions Involving the Social Context of the Patient
For short-, and middle term follow up, three studies (Barrows, 2018; Cohen-Mansfield & Sommerstein, 2019; Steinberg et al., 2009), and one study (Lang et al., 2018) reported a context-related intervention versus active control group, respectively. For short term follow-up two studies were pooled. Change scores were included for one study (Barrows, 2018). For the long term follow-up and the comparison to a passive control group, no studies were found.
Analysis of the pooled effect of an intervention based on a context-related intervention versus active control at short term follow-up in terms of physical activity resulted in a SMD of 0.20 (95% CI [−0.61, 1.00]) (Figure 6).
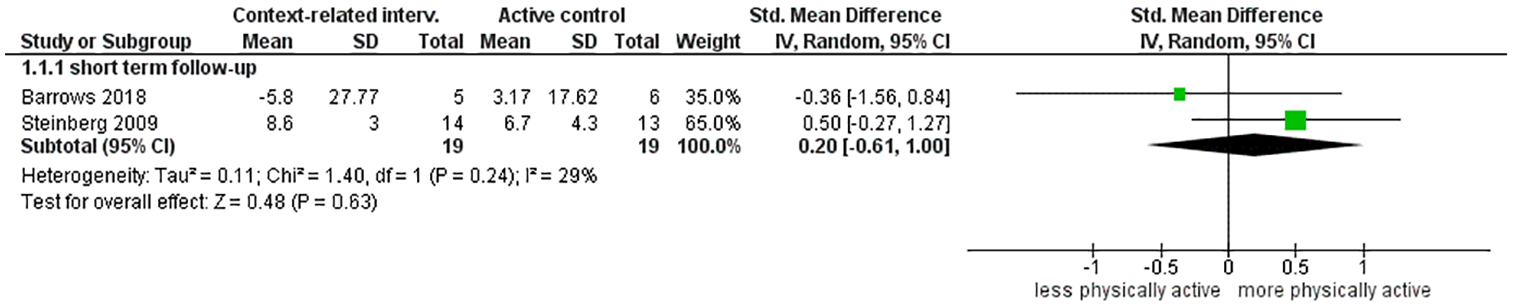
Intervention related to involving the social context of the patient versus active control group at short term follow-up.
One study was not added to the pooled analyses since no standard deviations were available (Cohen-Mansfield & Sommerstein, 2019). This study reported a similar magnitude of effect compared to the pooled results but this study reported a significant difference between context-related intervention and active control group at short term follow-up (Cohen-Mansfield & Sommerstein, 2019). For middle term follow-up versus active control group no significant between group difference in accelerometry data was found (Lang et al., 2018).
Due to very low quality of evidence at all measurement points of comparisons with active control groups (short term: very serious risk of bias, serious inconsistency, very serious indirectness, very serious imprecision; and middle term: serious risk of bias, very serious imprecision), we are uncertain whether a context-related intervention can improve level of physical activity. See Table 3 and Appendix C.
Shared Decision Making
For middle- and long term follow-up, one study reported an intervention based on shared decision making versus active control group (Khunti et al., 2021). No between-group differences in overall daily physical activity were found at middle- and long term follow-up. Due to very low quality at all measurement points of comparisons with active control groups (middle term: very serious risk of bias and very serious imprecision; and long term: very serious risk of bias and very serious imprecision), we are uncertain whether an intervention based on shared decision making can improve level of physical activity. See Table 3 and Appendix C.
Intervention Based on Monitoring & Feedback
For short-, middle-, and long term follow-up, two (Peel et al., 2016; Sazlina et al., 2015), five (Bragonzoni et al., 2023; Christiansen et al., 2020; Cox et al., 2021; Lyden et al., 2021; Sazlina et al., 2015), and four (Bragonzoni et al., 2023; Christiansen et al., 2020; Cox et al., 2021; Kawagoshi et al., 2015) studies reported an intervention based on monitoring & feedback versus active control group, respectively. For long term follow-up, all studies were pooled. We included change scores for one study (Kawagoshi et al., 2015). Other results were not pooled since two studies did not report a standard deviation (Peel et al., 2016; Sazlina et al., 2015). For the comparison to a passive control group, two (Koizumi et al., 2009; Wootton et al., 2019), three (Herghelegiu et al., 2017; Nguyen et al., 2019; Thompson et al., 2014), and three studies (Nguyen et al., 2019; Thompson et al., 2014; Wootton et al., 2019) were found for short-, middle-, and long term follow-up, respectively. For short term follow-up, all studies were pooled. Other results were not pooled since three studies did not report the level of physical activity at all outcome levels adequately (Herghelegiu et al., 2017; Nguyen et al., 2019; Thompson et al., 2014).
For short term follow-up, both studies which compared an intervention based on monitoring & feedback to active control groups reported significantly higher levels of physical activity in the intervention groups (Peel et al., 2016; Sazlina et al., 2015). A SMD of 0.15 (95% CI [−0.22, 0.52]) (Figure 7) for middle term follow-up was found. Conflicting results were found for other studies reporting results at middle term follow-up; one study reported significantly higher levels of physical activity in the intervention group (Sazlina et al., 2015), whereas the other study found no significant difference (Christiansen et al., 2020). For an intervention based on monitoring & feedback versus active control a SMD of 0.26 [−0.43, 0.95] (Figure 7) at long term follow-up was found. For an intervention based on monitoring & feedback versus passive control group a SMD of 0.36 [−0.36, 1.07] (Figure 8) at short term follow-up was found. For middle term follow-up, conflicting results were found; one study reported significantly higher levels of physical activity in the intervention group compared to the passive control group (Herghelegiu et al., 2017), one study reported no significant difference between intervention- and control group (Nguyen et al., 2019), whereas the other study reported the experimental group to be less physically active, however this was not significantly different compared to baseline (Thompson et al., 2014). For long term follow-up, the authors reported no differences within either group or between groups from 6 to 12 months of level of physical activity (Thompson et al., 2014), and two other studies reported no significant differences between groups (Nguyen et al., 2019; Wootton et al., 2019).
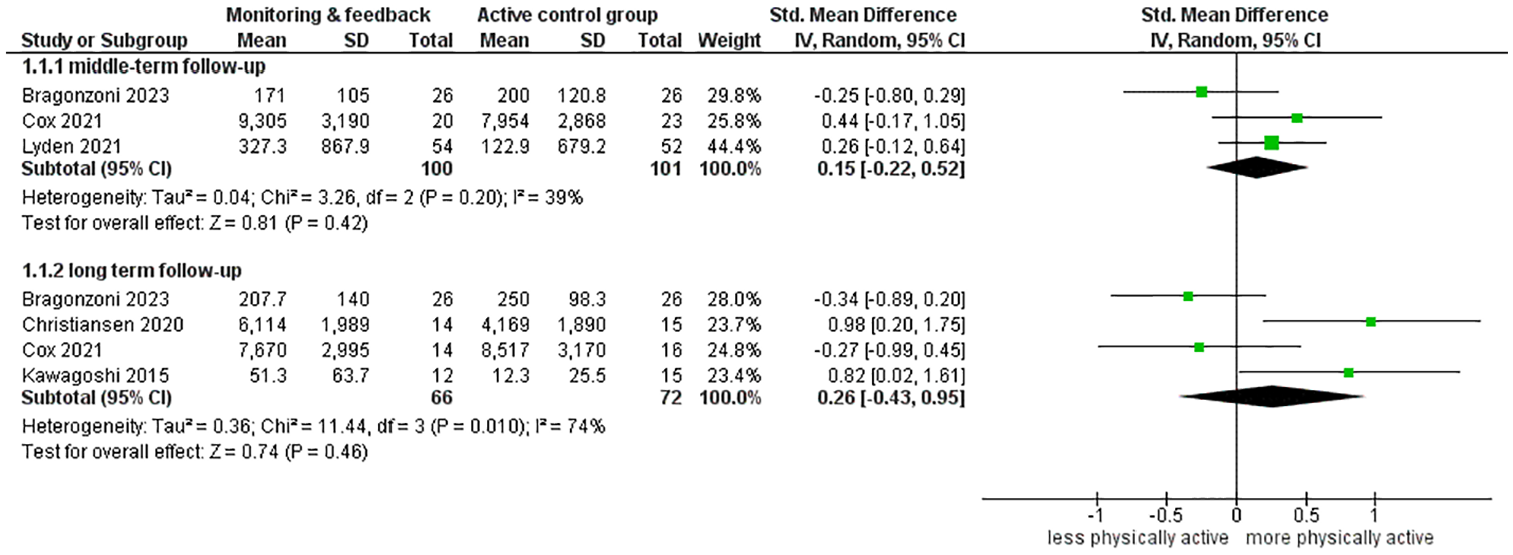
Intervention using monitoring & feedback versus active control group at long term follow-up.

Intervention using monitoring & feedback versus passive control group at short term follow-up.
Due to very low quality of evidence at all measurement points of both comparisons with active- (short term: very serious risk of bias, very serious indirectness, very serious imprecision; middle term: very serious risk of bias, very serious inconsistency, very serious indirectness, very serious imprecision; and long term: very serious risk of bias, very serious inconsistency, serious indirectness, very serious imprecision) and passive control groups (short term: very serious risk of bias, serious inconsistency, serious indirectness, very serious imprecision; middle term: very serious risk of bias, serious inconsistency, very serious indirectness, very serious imprecision; and long term: very serious risk of bias, serious inconsistency, very serious indirectness, very serious imprecision), we are uncertain whether interventions based on monitoring & feedback can improve level of physical activity. See Table 3 and Appendix C.
Interventions Using Multiple Motivational Strategies
Interventions were defined as using multiple motivational strategies when three or more motivational strategies were combined into a single approach.
For short-, middle-, and long term follow-up, respectively eight (de Vries et al., 2016; Harris et al., 2015; Heij et al., 2022; Kerr et al., 2018; Morey et al., 2009; Pfeiffer et al., 2020; Piedra et al., 2018; Suwanpasu et al., 2014), five (de Vries et al., 2016; Gillison et al., 2015; Heij et al., 2022; Kerr et al., 2018; Morey et al., 2009), and eight studies (Clare et al., 2015; Gillison et al., 2015; Goldberg et al., 2019; Harris et al., 2015; Heij et al., 2022; Kerr et al., 2018; Morey et al., 2009; Piedra et al., 2018) reported interventions with multiple motivational strategies versus active control groups and all studies were pooled. For the comparison to passive control groups, seven (Arkkukangas et al., 2019; Cabral et al., 2022; Cai et al., 2022; Cheng et al., 2022; Croteau et al., 2007; Mackey et al., 2019; Matz-Costa et al., 2018), three (Crist et al., 2022; Lewis et al., 2020; Oliveira et al., 2019), and six studies (Crist et al., 2022; Lewis et al., 2020; Oliveira et al., 2019; Siltanen et al., 2020; Stewart et al., 2001; Tuvemo Johnson et al., 2021) were found for short-, middle-, and long term follow-up, respectively and all studies for short term follow-up were pooled. In the pooled results, for one study we included the goal-setting with mentoring intervention group versus active control group (Clare et al., 2015). For another study, we included the supervised Otago exercise program supplemented with motivational interviewing versus the supervised Otago exercise program without the addition of motivational interviewing as passive control group (Arkkukangas et al., 2019). And for one study we included the moderate intensity group as multiple motivational strategies intervention (Goldberg et al., 2019).
Analysis of the pooled effect in terms of physical activity of interventions with multiple motivational strategies versus active control at short term follow-up resulted in a SMD of 0.27 (95% CI [0.04, 0.50]), for middle term follow-up a SMD of 0.25 [−0.02, 0.46], and for long term follow up a SMD of 0.26 [0.07, 0.45], see Figure 9. Pooled results for short-, middle-, and long term follow-up for interventions with multiple motivational strategies versus passive control groups resulted in a SMD of 0.66 [−0.45, 1.77], −0.09 [−0.37, 0.19], and 0.17 [0.00, 0.33], respectively (Figure 10).

Intervention using multiple motivational strategies (multistrategy) versus active control group at short-, middle-, and long term follow-up.

Intervention using multiple motivational strategies (multistrategy) versus passive control group at short-, middle-, and long term follow-up.
For long term follow-up of an intervention with multiple motivational strategies versus passive control group, one study reported a significant increase between the intervention with multiple motivational strategy and passive control group (Stewart et al., 2001). Another study reported no significant difference for this comparison (Tuvemo Johnson et al., 2021).
Due to very low quality of evidence at all measurement points of both comparisons with active- (short term: very serious risk of bias, very serious inconsistency, very serious indirectness; middle term: very serious risk of bias, very serious inconsistency, very serious indirectness; and long term: very serious risk of bias, very serious inconsistency, very serious indirectness) and passive control groups (short term: very serious risk of bias, very serious inconsistency, very serious indirectness; middle term: serious risk of bias, very serious inconsistency, very serious indirectness; and long term: very serious risk of bias, serious inconsistency, very serious imprecision), we are uncertain whether interventions with multiple strategies can improve level of physical activity. See Table 3 and Appendix C.
Individual Strategies Versus Interventions Using Multiple Motivational Strategies
To study the effect of individual strategies versus interventions using multiple motivational strategies, network meta-analyses were conducted for each of the follow-up points. Pooled studies in meta-analyses comparing interventions versus active control groups were included in network meta-analyses for short-, middle-, and long term follow-up, while studies comparing intervention with passive control groups were excluded since a passive control group is not applicable in daily clinical practice and provided distortion in the analyses.
For short term follow-up, respectively twenty-two (Arkkukangas et al., 2019; Barrows, 2018; de Blok et al., 2006; De Greef et al., 2011; de Vries et al., 2016; Grönstedt et al., 2013; Harris et al., 2015; Heij et al., 2022; Kerr et al., 2018; Lyden et al., 2021; McMahon et al., 2017; Morey et al., 2009; Pfeiffer et al., 2020; Piedra et al., 2018; Rausch Osthoff et al., 2021; Steinberg et al., 2009; Sugden et al., 2008; Suikkanen et al., 2021; Suwanpasu et al., 2014; Turunen et al., 2020; Van Hoecke et al., 2014; Warner et al., 2016), for middle term follow-up twenty (Bragonzoni et al., 2023; Brodie & Inoue, 2005; Christiansen et al., 2020; Cox et al., 2021; Cunningham et al., 2012; de Vries et al., 2016; Frändin et al., 2016; Gellert et al., 2014; Gillison et al., 2015; Heij et al., 2022; Kerr et al., 2018; Khunti et al., 2021; Lang et al., 2018; Lyden et al., 2021; McMahon et al., 2017; Morey et al., 2009; Rausch Osthoff et al., 2021; Suikkanen et al., 2021; Thompson et al., 2014; Turunen et al., 2020) and for long term follow-up twenty (Babazono et al., 2007; Bragonzoni et al., 2023; Christiansen et al., 2020; Clare et al., 2015; Cox et al., 2021; Gellert et al., 2014; Gillison et al., 2015; Harris et al., 2015; Heij et al., 2022; Ismail et al., 2020; Kawagoshi et al., 2015; Kerr et al., 2018; Khunti et al., 2021; Morey et al., 2009; Petrella et al., 2010; Piedra et al., 2018; Suikkanen et al., 2021; Van Hoecke et al., 2014; Warner et al., 2016) studies were included. For short term follow-up, interventions using multiple motivational strategies showed higher effects on increasing physical activity compared with motivational interviewing and interventions using the patient’s context, but these differences were not statistically significant, see Figure 11. The smallest effect (SMD of 0.07 [95% CI [−0.24, 0.39]) was found for interventions using multiple motivational strategies versus a tailor-made intervention and the greatest effect (SMD of −0.30 [−0.69, 0.009]) was found for interventions using multiple motivational strategies versus a interventions using the patient’s context. For middle- and long term follow-up, no statistical differences were found between interventions using multiple motivational strategies and interventions using singular strategies. For netgraphs and forest plots per timepoint, see Figure 11.

Netgraphs of the network meta-analysis analyzing individual strategies versus interventions using multiple motivational strategies (multistrategy) at the short-, middle- and long-term follow-up. The size of the nodes are proportional to the sample size of each intervention and the thickness of the lines are proportional to the number of studies available. Comparisons of the different strategies show combined results of direct- and indirect evidence. A negative SMD indicates superior effectiveness of interventions using multiple motivational strategies in comparison with individual strategies.
Due to very low quality of evidence at all measurement points of both direct- and indirect comparisons (very serious risk of bias, serious inconsistency, very serious indirectness and very serious imprecision), we are uncertain which strategies are the most effective in the promotion of physical activity at short- middle and long term follow-up. See Appendix C.
Discussion
Summary of Key Findings
This review provides an overview of the effectiveness of addition of motivational strategies in promoting and maintaining physical activity levels. Although higher effects on physical activity were observed for singular motivational strategies versus active control interventions, these results were not statistically significant. However, statistical significant differences in favor of interventions using multiple motivational strategies compared with an active control group were found at the short and long term. In addition, tailor-made interventions showed statistical significant higher effects versus an active control group on the long term. Direct- and indirect results of the network meta-analyses show no statistical differences between interventions using multiple motivational strategies than utilizing separate treatment strategies on their own. On middle- and long duration follow-up points, studies using monitoring & feedback, tailored interventions and interventions using the social context of the patient suggest higher effectiveness compared with interventions using multiple motivational strategies. At long term follow-up, tailor-made interventions suggest to be more effective in increasing physical activity as interventions using multiple motivational strategies. However, it is unclear how these differences translate in daily clinical practice. The quality of body of evidence has been assessed using GRADE and is of very low quality due to serious risk of bias, indirect evidence, and inconsistent effectiveness of strategies across studies. Small- to medium effect sizes and possible clinically important differences were identified based on evidence of very low quality, and therefore it is uncertain what the effectiveness of these strategies is in improving physical activity in daily clinical practice. Future research with higher quality evidence is recommended.
Reviews studying the effect of behavioral change strategies added to exercise interventions among older adults have been conducted before, although using different outcome measures and focused on different treatment strategies, limiting the comparability with our findings. One of the reviews confirmed that booster sessions by physical therapists utilizing motivational strategies have small to medium effect in increasing the adherence to exercise at short- and middle term follow-up in patient suffering from chronic low back pain or hip and/or knee osteoarthritis (Nicolson et al., 2017). Besides the targeted population, the construct of therapeutic exercise adherence differs from the construct of our primary outcome which is becoming or staying physically active. Physical activity can be defined as any bodily movement produced by skeletal muscles that require energy expenditure, which is not specifically connected to doing therapeutic exercises. Therapeutic exercise is considered as predefined, structured and repetitively doing physical exercises aimed at improving or maintaining musculoskeletal functions and/or physical condition (Caspersen et al., 1985). Although therapeutic exercise can be considered as physical activity, physical activity is not limited to exercise and can contain more ways of being physically active. The construct of adherence is seems to be more connected to doing exercises which are prescribed, while becoming or being more physically active is connected to behavior in daily living.
Another systematic review indicates motivational interventions (like motivational interviewing) are successful in the increase of adherence to exercise among individuals with a variety of conditions referring to behavioral change theories like the self-determination theory and social cognitive theory (McGrane et al., 2015). Another review has found moderate increase in physical activity in comparison to control groups when activity monitors are used among older adults at the short- and middle term follow-up (Larsen et al., 2019). Although the utilization of physical activity trackers is not considered as a motivational strategy in our review, it does provide a potential key element in the strategy monitoring & feedback. A systematic review of reviews on promotion of physical activity in community-dwelling older adults concluded moderate effect sizes of interventions using multiple motivational strategies at the short term, and small at middle term follow-up (Zubala et al., 2017). These interventions also incorporated elements of motivational interviewing, tailor-made interventions and shared decision making. Authors concluded that, although reviews included heterogenous studies and incorporated a variety of motivational strategies, providing feedback on performance led to significant, but inconsistent results. However, positive effects of tailor-made interventions focused on both environmental and psychosocial mediators, are suggested to be important for enhanced benefit of physical activity promotion. The impact of goal setting by either health practitioner or patient was assessed and made no statistical difference in effect sizes of interventions employing these strategies. Social support was not associated with any particular effects on physical activity, but it is suggested to be an effective component of successful walking interventions.
Taken together, based on the outcomes of our review and previous conducted reviews in this area, it can be concluded that older adults could experience the most beneficial effects from interventions combining multiple motivational strategies with effects maintained over a longer period than interventions utilizing one of the single strategies. The effects of such combined motivational strategies have been studied among patients with a variety of illnesses and diseases, which affect various aspects of daily functioning and cause different impairments. Each individual patient is unique and therefore it is recommended to provide a personalized intervention taken into account wishes, needs, and disabilities) of the patient instead of a standardized one-size-fits-all intervention.
This review has identified certain combinations of treatment strategies which are more common than others. Every intervention using multiple motivational strategies we identified, utilized motivational interviewing as basis for a tailored intervention and shared decision making sometimes complemented with monitoring & feedback. Shared decision making was identified in the description of all interventions using multiple motivational strategies but only once explicitly mentioned as an individual motivational strategy (Khunti et al., 2021). Consequently it could be possible this strategy was utilized in other studies as well, but not explicitly described and therefore not identified.
Using the GRADE criteria, the quality of body of evidence of this review shows large uncertainty. Future research should explore how the quality of the studies can be increased corresponding with the GRADE criteria. To optimize generalizability, we recommend future studies to explore the effect of one or more treatment strategies within an individual over a longer period of time over multiple timepoints, and compare these outcomes with other individuals among a heterogenous population. This allows to detect different pathways over time. The promotion of embedding physical activity in daily life is an important topic among older adults, especially in case of mobility problems and comorbidities, since it has many beneficial effects (de Vries et al., 2012). Therefore it is important which motivational strategies are capable of achieving and maintaining physical activity over a longer period of time. Further research is needed to understand if there is an optimal combination of treatment strategies and how to implement this in an individualized approach based on the wishes, needs and personal preferences of each patient. However, such an approach is challenging to study in larger samples, since the content could vary depending on the individual patients, and might therefore need other study designs which allows analysis of individual differences in interventions. In addition, implementation processes taking barriers and facilitators into account at patient-, professional-, and institutional level have to be identified to increase the fidelity of the delivered strategies in studies and to replicate effectiveness of successful interventions in daily clinical practice. This helps understanding what actions must be accomplished to successfully translate promising scientific initiatives into daily clinical practice.
Strengths and Limitations
This is one of the most extensive systematic reviews and meta-analyses analyzing the effect of motivational strategies added to exercise or physical activity interventions on physical activity among older adults. Strengths of this study were the data extraction and assessment of methodological quality which were carried out by two researchers, contributing to a higher accuracy of the review. The distinction between the several motivational strategies over the different time points during the meta-analyses and the network meta-analyses can be of added value to earlier reviews studying this topic. In our search, we have used broad in- and exclusion criteria for eligible studies regarding population characteristics resulting in a wide variety of conditions and illnesses included in our review which warrants a better representation of daily clinical practice.
However, this review has limitations that must be addressed. First, despite a thorough search with broad in- and exclusion criteria, we have used strict criteria for eligibility and might have excluded studies which were potentially appropriate for the review due to inadequate description of the content of the intervention in the abstract or full-text. Secondly, studies included in this review have measured physical activity through objective- (e.g., pedometers, accelerometers) and/or subjective instruments (e.g., questionnaires), which makes one-on-one comparisons more difficult to interpret (Skender et al., 2016). When both were used within a single study, we choose the subjective instrument due to an underestimation of physical activity levels among older adults with divergent gait patterns (Siebeling et al., 2012). Third, included studies were heterogenous in terms of content of the intervention and patient characteristics. Although interventions were clustered based on main treatment strategy, frequency, intensity, and involved practitioners differed between studies which could impact the comparability in the meta-analyses, but moreover could have serious consequences for the network meta-analyses. Although we downgraded for indirectness by GRADE and we evaluated transitivity of the study while assessing the quality of the evidence, evidence between strategies is predominantly indirect. While it is stated that indirect evidence is not necessarily of lesser importance than direct evidence, it is argumentative that indirect evidence of heterogenous interventions is debatable concerning generalizability of findings. This raised questions among the authors regarding the usability of network meta-analyses in the analyses of behavioral change interventions (Molloy et al., 2018). In contrast with studies concerning pharmaceutical interventions, where the active ingredient normally is fixed, whereas the dose and frequency may be subject to change, behavioral change interventions might not be as fixed. Therefore the results of our network meta-analyses must be interpreted with care.
Conclusion
This systematic review shows that interventions can increase physical activity in older adults by using different motivational strategies in physical activity. Interventions combining multiple motivational strategies seem to be more effective compared with active control groups, such as usual care treatment. Interventions using motivational interviewing, tailor-made interventions, interventions using the social context of the patient, interventions using shared decision making and interventions based on monitoring & feedback did not show statistical differences between the singular strategies and an active control intervention. The network meta-analysis did not show statistical significant differences between interventions using multiple motivational strategies in comparison with singular motivational strategies. Evidence is inconsistent, so an optimal combination of strategies remains unclear. Although more research is needed, outcomes of this review can benefit the effectiveness of interventions by healthcare professionals in promoting physical activity among older adults.
Footnotes
Acknowledgements
The authors acknowledge the contribution of Alice Tillema for her advice and help in creating the search strategies for the different databases.
Author’s Note
This research was conducted while Ward Heij was at Radboud university medical center. He is now at c and may be contacted at
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Data Availability Statement
The data used in this study are available upon reasonable request from the corresponding author. Requests should include a brief description of the intended use of the data.