
Abstract
There is an emerging view that remittances improve health outcomes in developing countries, though less is known about the conditions under which they may be effective. This study investigates whether and how the impact of remittances on child mortality depends on the level of mortality itself. Using a sample of 134 developing countries over the period 1990 to 2018, we estimate unconditional quantile treatment effects with an endogenous treatment variable, on aggregate child mortality and the three leading cause-specific child mortality rates: mortality from neonatal disorders, lower respiratory infections, and diarrheal diseases. We find that the impact of remittances differs systematically across the mortality distribution and across mortality indicators. Remittances appear less effective at reducing child mortality at the lowest and highest mortality rates than at the average.
Plain language summary
Remittances, money sent by migrant workers to their home countries, amounted to US$605 billion for developing countries in 2021. Recent research finds that remittances, on average, improve overall child health. However, it is theoretically unclear whether such benefits accrue to developing countries that cannot be considered average. In particular, do countries with non-average levels of child health also benefit? The purpose of this paper is to analyze whether and to what extent remittances influence child health at all levels of child health, and not just the average. We do so using novel quantile modeling techniques that enable us to more accurately quantify these differences. Secondly, we investigate whether remittances improve child health from three leading causes of child mortality. We find that remittances reduce child mortality in countries with low and high levels of mortality. However, remittances seem to have the most benefit for child health in countries with an average level of child mortality. Remittances also reduce the rate of the three leading causes of child mortality, but they seem to be more effective in mortality arising from infectious diseases. Our findings imply that countries at different levels of mortality cannot rely on remittances in the same way to improve public health outcomes. Coordinated planning at a national budget level and among donors is indeed required to improve healthcare alongside remittance inflows, even in countries experiencing high remittance inflows. One limitation is that we do not consider the impact of non-monetary migrant transfers which anecdotally may be relatively large.
Introduction
Reducing child mortality is an important component of sustainable development (United Nations, 2015). It is estimated that the under-5 mortality rate (U5MR) fell by 60% worldwide between 1990 and 2020 (UN IGME, 2021). However, there has been a disproportionate reduction in mortality rates across countries, and high mortality rates continue to persist in many developing countries. For instance, while the global U5MR is 36.6 deaths per 1,000 live births, the average rate in low-income countries is 67.6, over twice the average rate in middle-income countries, and over 10 times that of high-income countries (UN IGME, 2021).
The traditional policy approach for reducing child mortality centers on strengthening the healthcare system. Correspondingly, research has focused on whether funding in the form of aid or government expenditure on health has been effective. A more recent literature explores whether remittances, a direct funding to households, may impact child mortality. Apart from the potential of remittances to overcome fungibility challenges associated with aid (OECD, 2012), remittances raise household incomes and may reduce income risk (Balli & Rana, 2015), and migrants may transfer knowledge and better health practices from more developed countries (Hildebrandt & McKenzie, 2005). Importantly, remittances to developing countries amounted to US$605 billion in 2021, three times the size of official development assistance (Ratha et al., 2022). The emerging view is that remittances reduce the aggregate level of child mortality across developing countries (Azizi, 2018; Chauvet et al., 2013; Terrelonge, 2014). While important in empirically linking remittances to health outcomes, these studies, however, use mean regression techniques and implicitly examine the impact of remittances for countries at the 50th percentile of the aggregate child mortality distribution.
The assumption that the impact is the same at different mortality rates, however, is onerous. Why might the effects of remittances differ across mortality rates? The intended purpose and end uses of remittances may differ (Chami et al., 2008). It is possible, for instance, that a country with low mortality, and correspondingly better healthcare system, may see less remittances going to health compared to the average country. On the other hand, a lower-income country with high mortality and poor healthcare may have competing basic needs that inhibit how much remittances can be allocated to healthcare. Secondly, health infrastructure and factors surrounding the socioeconomic and political environment may impact absorptive capacity (Catrinescu et al., 2009; Sobiech, 2019). Where child mortality is high, correlated challenges such as inadequate health infrastructure, lack of access to health services and corruption may influence the effectiveness of remittances. For instance, remittances may be more effective in countries with higher mortality rates to the extent that more remittances are used for health care as a response to health sector deficiencies. Chezum et al. (2018) find that remittances have a greater impact on medical spending in districts with lower human development in Nepal, compared to those with higher human development. Alternatively, remittances may be more effective in countries with lower mortality rates to the extent that a robust health system facilitates the benefits of remittance spending on health care. This argument is based on the theory that a strong infrastructure enhances the benefits of remittances. There is evidence to suggest that a greater level of governance, for instance, may increase the impact of remittances on health outcomes (Borja, 2020). Given the myriad of possible competing channels and effects, the impact of remittances at any part of the child mortality distribution, therefore, requires empirical insight.
In this article, we contribute to two new questions. Firstly, we assess whether the impact of remittances on child mortality depends on the level of mortality. In other words, we examine the impact of remittances on mortality across the entire distribution of mortality. This helps to identify, for instance, the effectiveness of remittances in countries facing more severe child health challenges. Secondly, we ask in what way remittances affect child mortality. Accordingly, we examine the relationship between remittances and the U5MR disaggregated into the three leading causes: U5MR from neonatal disorders, lower respiratory infections and diarrheal diseases. Together, these causes account for three out of every five deaths for children under five (Global Burden of Disease Collaborative Network, 2020). We therefore provide insight into the ways in which remittances affect child mortality, which is relevant to how policymakers may best utilize remittances for public health outcomes alongside other sources of funding. Utilizing a sample of 134 developing countries over the period 1990 to 2018 and estimating unconditional quantile treatment effects, we present two main findings. First, there are differences in both the size of the effect across the mortality distribution, as well as where the effect is significant. Second, there are differences in the size and significance of the estimates across the causes of child mortality.
We contribute to the literature empirically with the use of the Generalized Quantile Regression (GQR) estimator of Powell (2020). This estimator provides the unconditional quantile treatment effect (QTE) of remittances and allows the use of an instrumental variable (IV) to address endogeneity. We go beyond traditional quantile regression approaches which provide conditional effects and where the interpretation of the effect may be confounded by the covariates of the model. To the best of our knowledge, this is the first study to use quantile regression techniques to examine the remittances-mortality relationship. Another contribution to this literature is the approach via which we address endogeneity. Endogeneity bias, through reverse causality, may arise in examining the effect of remittances on health outcomes. Remittances are sent by migrants and the inflows are likely to reflect, to some extent, factors such as child survival rates. We address potential endogeneity bias by constructing a shift-share IV novel to this literature. The concern with previous IVs, based on macroeconomic conditions in the sending country, is whether they are plausibly exogenous to health outcomes. Our IV uses predicted remittance flows and exploits variation from shares of recipient countries in sending-country flows. One advantage of this type of instrument is that it may be able to better identify the effects of a permanent change in the treatment variable (Temple & Van de Sijpe, 2017).
Literature Review
The literature on the link between remittances and health outcomes at the cross-country level is a recent one. The emerging consensus, however, is that remittances improve child health. The empirical evidence shows that a higher level of remittances is associated with higher life expectancy (Amega, 2018; Azizi, 2018; Djeunankan & Tekam, 2022; Zhunio et al., 2012) and lower neonatal, infant and under-five mortality rates (Amega, 2018; Azizi, 2018; Borja, 2020; Chauvet et al., 2013; Djeunankan & Tekam, 2022; Lim & Simmons, 2016; Terrelonge, 2014; Zhunio et al., 2012), often across a wide sample of developing countries. These studies address potential endogeneity bias with the use of instrumental variables. However, these instruments are mostly based on sending-country macroeconomic variables. One general problem is whether these instruments affect recipient-country conditions through remittances alone (Barajas et al., 2009). Some recent evidence from country-specific studies, however, suggest no causality from remittances to infant mortality rates (Musakwa & Odhiambo, 2020, 2021).
It is not clear from the empirical literature, however, through which mechanisms remittances operate to influence child mortality. This is important to address as it provides insight into how best to utilize remittances for health. Further, child mortality may be influenced by many determinants and risk factors. For instance, recent evidence suggests that remittances are reduce child mortality from diarrheal diseases but not from respiratory illness or neonatal disorders (Ramkissoon & Deonanan, 2023). The authors find that this effect may be mediated by sanitation access. From a theoretical perspective, remittances may affect child health in several ways. This is informed by frameworks describing the determinants of child health and nutrition (Mosley & Chen, 1984; UNICEF, 2021) as well as economic models on the demand for health based on household utility maximization (Currie, 2000; Grossman, 1972).
Firstly, remittances are a source of income for recipients and therefore relax budget constraints and may lead to increased spending. This can have effects on health outcomes if remittances affect the demand for medical care, doctor visits and other health services. This may occur if health is considered a normal good for households. Much of the micro-evidence shows that remittances are associated with higher private health expenditure and increased utilization of health care services (Amuedo-Dorantes & Pozo, 2011; Atake, 2018; Berloffa & Giunti, 2019; Chezum et al., 2018; Frank et al., 2009; Kan, 2021; Kapri & Jha, 2020; Petreski et al., 2018; Ponce et al., 2011). Kakhkharov et al. (2021), however, finds that remittances reduce health spending in Uzbekistan, suggesting this supports the view that remittances are channeled to consumer goods. At the macro-level, some studies find that remittances increase access to health care services and private health expenditure (Abraham & Tao, 2021; Azizi, 2018; Drabo & Ebeke, 2011; Yol, 2017). However, Terrelonge (2014) finds that the effect of remittances on household health spending is insignificant, while finding that remittances improve child nutritional status. The spending effect of remittances may therefore affect child health through food consumption and nutrition, without necessarily being seen in increased private health spending. Much of the literature supports the view that remittances affect food expenditure as studies have found that remittances are associated with improvements in food security (Moniruzzaman, 2022; Ogunniyi et al., 2020; Regmi & Paudel, 2017; Sulemana et al., 2023; Thomas-Hope, 2017), dietary diversity (Waidler & Devereux, 2019), calorie consumption (Akçay & Karasoy, 2017), intake of quality nutrients (Isoto & Kraybill, 2017) and nutritional status indicators (Antén, 2010; Azizi, 2018; Frank & Hummer, 2002; Lu, 2013). Waidler and Devereux (2019) and Ponce et al. (2011), however, find no effect on nutritional status, while Antén (2010) finds that remittances improve short- and middle-term nutrition but not long-term status. Mabrouk and Mekni (2018), on the other hand, find that remittances improve some facets of food security but reduce food production.
Secondly, remittances may affect health outcomes indirectly through the socioeconomic and political environment. For instance, higher remittances have been linked to an increase in education (Azizi, 2018), which is considered an important influence for health outcomes and may even mediate the impact of other factors (Charmarbagwala et al., 2004; UNICEF, 2021). Remittances reduce liquidity constraints and allow households to finance educational investments that they may not otherwise make. Remittances have been found to increase educational expenditure (Ambler et al., 2015; Askarov & Doucouliagos, 2020), as well as school attendance (Azizi, 2018; Bansak & Chezum, 2009; Edwards & Ureta, 2003). Remittances have also been linked to a rise in a country’s GDP level (Francois et al., 2022), and a worsening of corruption levels (Ahmed, 2013), which are important socioeconomic and political influences for health outcomes (Charmarbagwala et al., 2004; UNICEF, 2021). Public health spending is also important to a country’s health outcomes. However, some argue that remittances reduce perceived income risk in recipients which may lead to reductions in social spending (Doyle, 2015). This is a crowding-out effect and there is some evidence to suggest this may occur. For instance, Hubert Ebeke (2012) finds that remittances reduce public health spending when governance is bad, while Yol (2017) finds that remittances reduce public health spending despite improving private spending. Remittances may also be linked to improvements in access to sanitation and clean drinking water (Adida & Girod, 2011; Tsafack & Djeunankan, 2021). These are important factors in reducing mortality risk for infectious diseases. Some argue, however, that remittances may only be spent on consumer goods. Even in this context, this may be an optimal situation if recipients are starting from very low consumption levels (Yang, 2013). Increasing household consumption beyond subsistence levels and reducing poverty can have a beneficial effect on child health.
Third, remittances may be linked to health through an insurance mechanism. This refers to remittances being used to prevent or dampen the effects of negative health shocks. For instance, evidence suggests that remittances may increase spending related to preventative issues such as de-worming and vaccination (Ponce et al., 2011). Remittances also increase the household safety net by reducing financial constraints. This is especially relevant to developing countries, as they may have imperfect credit markets. While formal insurance programs and universal health coverage are major components of health policies globally, developing countries still face challenges in implementing such programs (Erlangga et al., 2019). Remittances therefore provide funding which may also cover gaps in formal insurance programs. Amuedo-Dorantes and Pozo (2011) and Frank et al. (2009) find that those with health care coverage provided by employers in Mexico spend less remittances on health, which may imply a certain degree of substitution between remittances and formal insurance coverage. Cuadros-Meñaca (2020) finds that remittances increase contributions to health and pension for informal workers in Colombia. Remittances also provide an income smoothing opportunity, which in turn may dampen the effects of negative health shocks. Ambrosius and Cuecuecha (2013), for instance find that Mexican households with migrants did not increase debt in response to health shocks, despite the average debt burden doubling. Beuermann et al. (2016) find similar evidence in the case of Jamaica.
Fourth, remittances may be linked to health via the effects of migration. Remittances, for instance, may change preferences by affecting health knowledge and the transfer of social norms between migrant and recipients. This is acknowledged as social remittances (Levitt, 1998). There is evidence, for instance, that remittances reduce fertility rates in recipient countries due to a transfer of social preferences (Anwar & Mughal, 2016; Ibrokhimov et al., 2023; Naufal & Vargas-Silva, 2009), while Ponce et al. (2011) finds evidence of a knowledge effect in Ecuador as remittances increase knowledge on AIDS. The migration of household members, however, may be linked to disruptive effects resulting from parental absence. These disruptions may refer to the loss of income, effects on child education and mental health, the role of the parent in child health or increases in child labor. The migration experience may also transmit emotional attributes which can affect family structures in different ways (Katigbak, 2015). There is some evidence to suggest that migration may be linked to disruptive effects which may be offset by remittances (Kanaiaupuni & Donato, 1999). Others find that migration or parental absence may be linked to lower nutritional status (Davis & Brazil, 2016; Gibson et al., 2011; Hildebrandt & McKenzie, 2005). In a study on the link between migration and well-being, Ivlevs et al. (2019) find that the receipt of remittances is linked to an increase in evaluative well-being but having a household member abroad can also be linked to increased stress. Further, there is some evidence to suggest that the disruptive effects may decrease when migration is more common in a country (Ivlevs et al., 2019; Kanaiaupuni & Donato, 1999).
It is not clear which factors may influence or condition the effect of remittances on mortality rates. This is important to understanding how the effectiveness of remittances may be improved. Whether there are such differences in the remittances-health relationship and why, however, has received limited attention. Chauvet et al. (2013) examine the effect of remittances on child mortality and finds that they are more effective in reducing mortality in upper-income classes. Chezum et al. (2018) finds that remittances increase medical spending in Nepal and this result is stronger in districts with a low human development index (HDI). Borja (2020), on the other hand, finds that the effect of remittances on economic development and child health in LAC is stronger when the control of corruption is better. What is not clear, however, is whether and how does the remittances-mortality relationship change for countries facing different mortality rates. Mortality rates, as discussed above, are the product of the simultaneous interaction of a number of underlying country factors. Importantly, can a country facing significant challenges to child health benefit from remittances in the same way that a country with lower mortality rates can?
Data and Methods
Methodology
When considering variation of the impact of a treatment variable across the distribution of the dependent (or outcome) variable, researchers frequently use quantile regression (QR) methods. Traditionally, conditional quantile methods have been used for estimation. It is often necessary to include control variables in a regression, for instance to reduce omitted variable bias. Conditional QR methods, however, do not assume that the relationship between the treatment variable and the dependent variable varies based on other covariates. Thus, the interpretation of the estimates changes as covariates are added (Powell, 2020). The traditional estimators of Koenker and Bassett (1978) also assume the treatment variable to be exogenous.
In this study, we use the GQR estimator to examine the impact of remittances on child mortality. This estimator addresses limitations of the traditionally used QR estimators. The GQR estimator allows us to condition on additional covariates without affecting the interpretation of the quantile effect. It is also developed in an IV framework, which allows for estimating the impact in the presence of an endogenous treatment variable. The specification of interest for the outcome variable can be written as:

where M denotes the child mortality indicator, and R represents remittance inflows. We use the GQR estimator to estimate the structural quantile function (SQF):

The SQF defines the τth quantile of the mortality distribution given the remittances variable. With the GQR approach, additional covariates are used only to provide information about the distribution of the disturbance term before estimation. Thus, β(τ) is evaluated marginally over the distribution of the covariates. It shows how the distribution of child mortality changes at different quantiles in response to changes in remittances, unconditional on the covariates.
To address the potential endogeneity of remittances, we utilize an IV. In the GQR framework, the SQF is estimated under the assumption that U*|Z, X ∼ U*|X, where X denotes the control variables and Z denotes the instrument. To estimate the unconditional QTE with the GQR estimator, there are two moment conditions that differentiate it from conditional estimators:


where τx represents P(M ≤ R’β(τ)|X). Our instrumental variable, Z, is constructed as follows:

where wi,j,t − 1 is the share of remittance inflows to country i sent by country j in the period t − 1. This share component is constructed as follows:

where Ri,j denotes the amount of remittances sent by country j to country i. Rj denotes the total remittances sent by country j. The share therefore represents the portion of remittances received out of aggregate remittances coming from the sending country. R-i j,t is the shift component and denotes the total remittances sent by country j for period t, excluding remittances to country i.
In the recent remittances-mortality literature, studies use instruments based on sending-country characteristics (Chauvet et al., 2013; Terrelonge, 2014). This is done to address endogeneity bias which may arise as health outcomes may influence remittances (Azizi, 2018; Musakwa & Odhiambo, 2021). Worsening health outcomes may encourage migrants to increase remittances. The decision to migrate and remit may also depend on the health of family members (Azizi, 2018). The potential problem with instruments based on sending-country conditions, however, is that they are likely to have an impact on health outside of the impact that they have through remittances. Our IV is based on predicted remittance flows. By using total sending-country outflows we can capture the effects of changes in the microeconomic determinants of remittances (Barajas et al., 2009). It is unlikely that changes in total sending-country outflows are related to recipient-country conditions. We also avoid direct links with other domestic variables by excluding own-country remittances for each recipient. We also capture differences in the exposure of recipients with lagged shares of recipient-country remittances in those outflows. These are likely to be good predictors for remittances due to migration networks and are plausibly exogenous since recipient-country factors are unlikely to be correlated with the lagged remittance shares.
Data
For the outcome variables in this study, we collected data on aggregate child mortality as well as cause-specific mortality. Data on the aggregate U5MR is collected from the World Development Indicators (WDI) database (World Bank, 2022). Data on the three leading causes of child mortality is obtained from the Global Burden of Disease 2019 Study (Global Burden of Disease Collaborative Network, 2020). This study, led by the Institute for Health Metrics and Evaluation (IHME), estimates the global burden of 369 diseases and injuries across 204 countries and territories for the period 1990 to 2019 (Vos et al., 2020). We use the three leading causes since, together, these causes account for three out of every five deaths in children under age five. Remittances may also have theoretical linkages to the risk factors associated with these causes (Ramkissoon & Deonanan, 2023). These causes are the U5MR from neonatal disorders (U5MR-N), lower respiratory infections (U5MR-R), and diarrheal diseases (U5MR-D). We use these variables as mortality rates by expressing them as the number of deaths per 1,000 live births. Data on remittances is collected from the WDI database. To account for the relative size of remittances across countries and the effects of changes in price levels, we express remittances in per capita terms and in constant 2015 US dollars.
The control variables used are common covariates from the child mortality literature (Hanmer et al., 2003; Houweling & Kunst, 2010). We use gross domestic product (GDP) per capita (constant US$2015) as this may influence the resources spent on health, as well as other socioeconomic factors (Hanmer et al., 2003). We also include demographic variable such as population and the total fertility rate. Fertility is an important control as birth intervals tend to be correlated with mortality rates as well as malnutrition (Charmarbagwala et al., 2004; Finlay et al., 2011). Disbursements of development assistance for health (DAH) per capita (constant US$2015) is included as a control, as aid targeted to health may be important to developing countries by providing additional funding for health programs and interventions (Mishra & Newhouse, 2009). We also control for average years of schooling (adults aged 25 year and over), as higher education levels may be associated with healthier children (Cutler et al., 2006). Data on schooling is obtained from the Human Development Reports database (UNDP, 2022). DAH is obtained from the IHME’s DAH database (IHME, 2021), while data for the other control variables are obtained from the WDI.
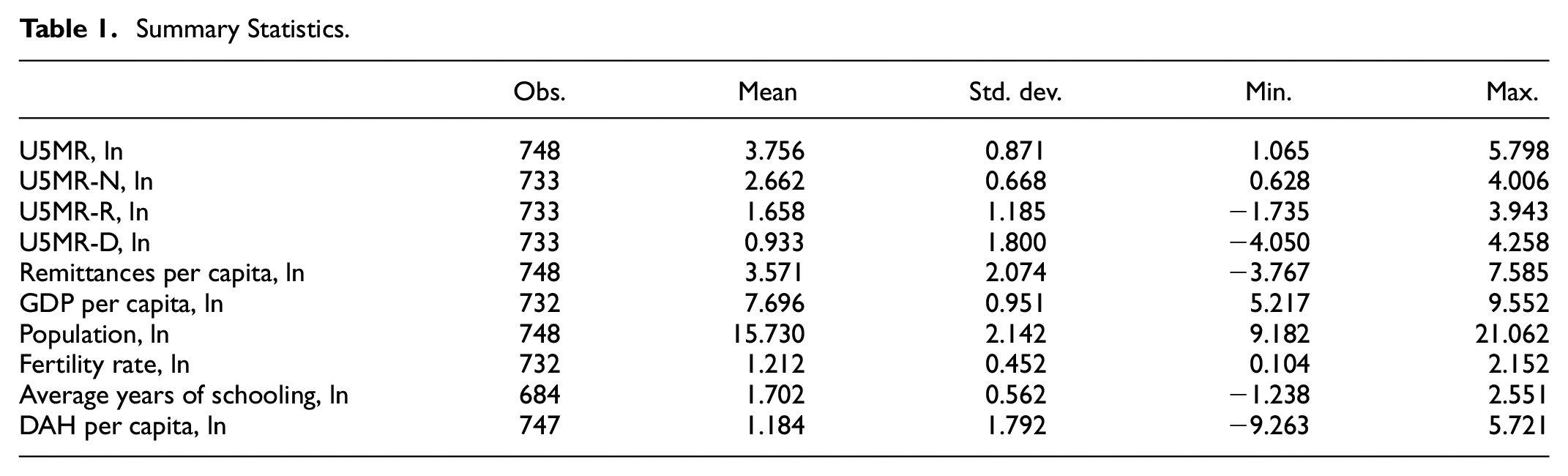
For the construction of the instrument, we estimate bilateral remittances using the method of Ratha and Shaw (2007) using weights based on migrant stocks and per capita income in both destination and source countries. Bilateral migrant stock data is collected from Özden et al. (2011) and World Bank staff estimates available from World Bank (2017). All data used in this study is publicly available country-level data, obtained from international sources. Our sample consists of an unbalanced panel of 134 countries over the period 1990 to 2018, using five-year non-overlapping periods with values taken every fifth year. The sample is constructed to include all low- and middle-income countries for which data is available. We express all variables in logarithmic form. Table 1 displays summary statistics for the variables, including the covariates. As mentioned previously, however, the additional covariates are used only to provide information about the distribution of the disturbance term. Table A1 in the Appendix lists the countries in the sample. The quantile regressions are carried out in Stata, version 17.0, using the genqreg package (Baker et al., 2016). Numerical optimization is done using Markov Chain Monte Carlo methods.
Summary Statistics.
Results and Discussion
Empirical Results
Table 2 reports quantile regression estimates, while Figure 1 presents the graphical illustration of the results. The solid lines in Figure 1 represent the QTEs and the shaded region represents the 95% confidence interval. Looking at the overall U5MR, we find the effect of remittances to be negative and significant at the 50th percentile. A negative and significant effect indicates that remittances lower mortality. While this is consistent with the previous literature (Azizi, 2018; Chauvet et al., 2013; Terrelonge, 2014), our first novel finding, however, is that there are differences in both the size of the effect across countries facing different mortality levels, as well as where the effect is significant. Remittances are not only significant at the middle of the distribution but also from the 25th percentile onward (τ ≥ 0.25). We find that the mortality-reducing effect is largest at the 40th percentile. However, we also find that the size of the significant effects ranges from −0.154 to −0.028, with the mortality-reducing effect decreasing along the mortality distribution above the median.
The Effect of Remittances on Four Indicators of U5MR Across Quantiles.

Note. Standard errors are denoted in parentheses.
p < .01. **p < .05. *p < .1.

Unconditional quantile treatment effects. Dependent variables are: (a) U5MR, (b) U5MR-R, (c) U5MR-N, and (d) U5MR-D.
When we disaggregate by cause of death, we find that the results are also not generalizable across the mortality spectrum, nor across causes. Our second novel finding is that there are differences in the size and significance of the impact of remittances across different causes of child mortality. At the 50th percentile, the effect of remittances is negative and significant across all indicators. However, it is also significant at other points in the distribution for each cause. The effect remains significant from the 30th percentile onward for U5MR-R, between the 25th and 60th percentiles and from the 85th percentile onward for U5MR-N, and between the 10th and 60th percentiles and from the 90th percentile onward for U5MR-D. For the U5MR-R, the magnitude of the impact is largest at the 45th percentile. The decline in the coefficient estimates at higher quantiles, however, is smaller than that for the overall U5MR.
Although the effect is strongest near the average mortality rate, the impact of remittances on U5MR-R is similar at high mortality rates. For the U5MR-N, the size of the impact for the mortality-reducing effects is smaller when compared to the other causes. For the U5MR-D, the magnitude of the impact is largest at the 45th percentile. The size of the effect is also the largest among all the mortality rates. Remittances lose effectiveness above the median for both U5MR-N and U5MR-D but become effective again at the highest mortality rates. Unlike the other causes, remittances are effective for U5MR-D below the 25th percentile. We also find that the size of the impact differs across the distribution for each cause. Looking at the significant coefficients, the magnitude ranges from −0.172 to −0.089 for U5MR-R, −0.080 to 0.052 for U5MR-N, and −0.290 to −0.053 for U5MR-D. For each cause-specific rate, the mortality-reducing effect of remittances appears to decline along the distribution above the median. However, this decline is less pronounced for the U5MR-R. In the case of the U5MR-N, the effect becomes positive and significant for τ ≥ 0.85.
Discussion of Findings
Importantly, we find that the impact of remittances on child mortality is not generalizable across the mortality spectrum. This finding is important as the recent literature suggests that remittances reduce child mortality rates (Azizi, 2018; Chauvet et al., 2013; Terrelonge, 2014; Zhunio et al., 2012). While we find the same result at the average, these studies use mean-regression approaches which makes it difficult to draw conclusions about how the impact varies across countries with different mortality rates. We find that countries with the lowest U5MR do not appear to benefit from remittances via a reduction in child mortality. One explanation for this is that countries with lower mortality rates have more robust health systems and may not be as underfunded in health resources. We check the robustness of our findings to including physician density as an additional covariate. These findings are similar to our main results and are available upon request. To the extent that this occurs, significant improvements in healthcare and health infrastructure may dampen the effect of remittances on child survival. Recalling the findings of Chezum et al. (2018), the impact of remittances on medical spending in Nepal were found to be stronger in districts with low HDI. Another explanation, however, may be that developing countries with the lowest mortality rates face a lower proportion of preventable and communicable diseases. The results at the fifth percentile show an insignificant effect for remittances across all causes. We do find, however, that remittances reduce child mortality at mortality rates below the average. Remittances reduce the U5MR-D even at the 10th percentile. This shows that even for countries with less health challenges, remittances can affect child survival rates from diarrheal diseases. The U5MR-D may be more sensitive to household income increases stemming from the influx of remittances, as many treatment options are fairly simple (Fontaine et al., 2007), and detection is relatively easy. This is important for understanding the mechanisms through which remittances affect child mortality. This supports recent findings that remittances reduce child mortality from diarrheal diseases (Ramkissoon & Deonanan, 2023).
For countries facing more moderate child mortality rates and countries near the median, the mortality-reducing effect of remittances tends to be largest. These appear to benefit most from remittances for child health. The impact of remittances on the U5MR-R and U5MR-D is over twice and three times, respectively, larger than the impact on the U5MR-N. This provides further insight into the mechanisms through which remittances operate. For instance, reducing the U5MR-N may depend not only on factors related to maternal health but also on health infrastructure and hospital care, where remittances may have less of an impact. On the other hand, risk factors for U5MR-R and U5MR-D include undernutrition and poor sanitation, where remittances may have a greater impact. Recent studies find that remittances may improve food security and nutritional outcomes in children (Antén, 2010; Ogunniyi et al., 2020) One implication is that remittances may be more effective for health through improvements in nutrition and living conditions than through medical spending. While this may support the view of Terrelonge (2014), our results do not suggest that the impact of remittances through private health spending is insignificant. We do find that remittances reduce mortality rates from all three causes.
As mortality rates increase, there may be correlated challenges such as a larger gap in funding needs and public health resources, or worsening health infrastructure. Remittances may be better poised to promote child health when such constraints exist. This, however, is not the complete story. The mortality-reducing effect of remittances declines as mortality rates increase past the average. This effect may even be lost at moderately higher mortality rates. For instance, the impact of remittances on U5MR-N and U5MR-D is insignificant between the 60th and 80th percentiles. However, we note that remittances have a negative and significant impact at the highest mortality rates for all but the U5MR-N, where it is positive. Countries facing higher mortality rates, and thus greater challenges to child health, benefit from remittances but to a lesser extent as countries at the average U5MR. One explanation for such a finding is that as constraints in the health sector increase, other sources of health financing may have a greater role and therefore sideline the effect of remittances to some extent. Other factors that are correlated with higher mortality rates may also be important, such as the challenges from overcoming weaker institutional quality. This, however, requires further evaluation. Borja (2020), for instance, finds that the effect of remittances on human development is greater when the control of corruption is better. Our finding, however, does not suggest substitutability between remittances and other funding sources. Remittances still reduce child mortality for countries with the highest mortality rates. This is in contrast to some quantile regression estimates for health aid, which suggest that aid may be ineffective in countries with higher mortality rates (Kizhakethalackal et al., 2013). We also note that remittances may increase the U5MR-N at the highest mortality rates. As the U5MR-N may have less risk factors affected by remittances, compared to the other causes of death, then in countries with the greatest health challenges, the disruptive effects of migration may outweigh the benefits of remittances.
Conclusion
Do remittances reduce child mortality in the same way across countries with differing mortality rates? Do these effects change across different causes of mortality? This study examines these questions and seeks to address how remittances fit into the public health discussion. Our first novel finding is that the effect of remittances on child mortality varies across the mortality distribution. Our results suggest that remittances generally do not appear to have an effect in reducing child mortality where mortality rates are lowest. Remittances reduce child mortality and have the largest effects near the average, though this effect is reduced at higher mortality rates. Our second major finding is that there are differences in the size and significance of remittances across different causes of child mortality. Remittances appear to be more effective in reducing mortality rates from diarrheal diseases and respiratory infections than from neonatal disorders.
Our findings highlight that while remittances are likely to reduce child mortality in many developing countries, this effect is not the same for each one. One implication of this is that cutting back on funding such as health aid due to high remittance inflows may not be effective in countries with the highest mortality rates. In countries with the lowest and highest child mortality rates, remittances may still be important to other outcomes, but policymakers should focus on addressing other aspects of the health system. Policymakers in countries with child mortality rates at average levels may want to increase the focus of remittances in health policies as the effects appear to be largest here. This focus should also extend to facilitating easier transfers of remittances and lowering transaction fees to allow greater inflows. Our results also imply that remittances may have a stronger link to child mortality through infectious diseases and their risk factors. This suggests an important relationship between remittances and nutrition as well as environmental factors. Remittances may be viewed as a complement to other sources of health financing, that may address health outcomes through demand-side interventions. Health policy discussions in developing countries with high rates of communicable diseases may increase the focus of remittances. We also highlight that the assumption of uniformity may not always hold when examining the effects of remittances. It is important for future research to consider whether and how these effects may be heterogeneous.
Footnotes
Appendix A
List of Countries in Sample.

| Afghanistan | Ecuador | Madagascar | Serbia |
| Albania | Egypt, Arab Rep. | Malawi | Sierra Leone |
| Algeria | El Salvador | Malaysia | Solomon Islands |
| Angola | Equatorial Guinea | Maldives | Somalia |
| Argentina | Eritrea | Mali | South Africa |
| Armenia | Eswatini | Marshall Islands | South Sudan |
| Azerbaijan | Ethiopia | Mauritania | Sri Lanka |
| Bangladesh | Fiji | Mauritius | St. Lucia |
| Belarus | Gabon | Mexico | St. Vincent and the Grenadines |
| Belize | Gambia, The | Micronesia, Fed. Sts. | Sudan |
| Benin | Georgia | Moldova | Suriname |
| Bhutan | Ghana | Mongolia | Syrian Arab Republic |
| Bolivia | Grenada | Montenegro | Tajikistan |
| Bosnia and Herzegovina | Guatemala | Morocco | Tanzania |
| Botswana | Guinea | Mozambique | Thailand |
| Brazil | Guinea-Bissau | Myanmar | Timor-Leste |
| Bulgaria | Guyana | Namibia | Togo |
| Burkina Faso | Haiti | Nauru | Tonga |
| Burundi | Honduras | Nepal | Tunisia |
| Cabo Verde | India | Nicaragua | Turkey |
| Cambodia | Indonesia | Niger | Turkmenistan |
| Cameroon | Iran, Islamic Rep. | Nigeria | Tuvalu |
| Central African Republic | Iraq | North Macedonia | Uganda |
| Chad | Jamaica | Pakistan | Ukraine |
| China | Jordan | Papua New Guinea | Uzbekistan |
| Colombia | Kazakhstan | Paraguay | Vanuatu |
| Comoros | Kenya | Peru | Venezuela, RB |
| Congo, Dem. Rep. | Kiribati | Philippines | Vietnam |
| Congo, Rep. | Kyrgyz Republic | Romania | West Bank and Gaza |
| Costa Rica | Lao PDR | Russian Federation | Yemen, Rep. |
| Cote d’Ivoire | Lebanon | Rwanda | Zambia |
| Djibouti | Lesotho | Samoa | Zimbabwe |
| Dominica | Liberia | Sao Tome and Principe | |
| Dominican Republic | Libya | Senegal |
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by The University of the West Indies Campus Research and Publication Fund under Grant number CRP.3.MAR19.1.
Ethics Statement
Not applicable to this study.
Data Availability Statement
Data sharing not applicable to this article as no datasets were generated or analyzed during the current study.