
Abstract
The COVID-19 pandemic has brought unique challenges for caregivers. This study examines whether individual resilience accounted for differences in caregiver burden, coping-related resilient behaviors, depression, and stress during the COVID-19 lockdowns. A total of 324 caregivers responded to a survey covering three time points (pre-pandemic (t0, retrospective), first lockdown in April 2020 (t1, retrospective), and second lockdown in winter 2020/2021 (t2, prospective)). Items covered the care situation and caregiver burden (t0 and t1), coping-related resilient behavior (t1), perceived stress (PSS-10) and depression (GDS-15) (t1 and t2) as well as resilience (BRS) (t2). Higher resilience was associated with lower caregiver burden, a higher degree of coping-related resilient behaviors, and with lower perceived stress but higher depression. Stress and depression showed different trajectories over time depending on resilience. Resilience-promoting interventions for caregivers should be used to reduce stress and caregiver burden. Special attention should be paid to depression prevention, with tailored programs to address the needs of resilient caregivers during lockdowns.
Introduction
Informal caregivers represent a particularly vulnerable population (Adelman et al., 2014; Brodaty & Donkin, 2009) that is at increased risk of developing stress-related physical and mental illness (Pinquart & Sörensen, 2003). Nevertheless, caregivers show individual differences in their ability to cope (Adelman et al., 2014; Dias et al., 2015). Originally defined as the ability to return to a previous state of health (Carver, 1998), resilience is currently also described as the ability to “bounce back” in the face of adversity (Smith et al., 2008). Thus, resilience is closely associated with adaptive coping strategies when being confronted with adversities, leading to the idea of resilient coping styles in caregivers (Palacio G et al., 2019). Accordingly, resilience might explain why some caregivers are better able to cope with the stress associated with caregiving than others. The process of resilience consists of the actions that caregivers adopt to access their resources and thus overcome adversity. Research findings in this area predominantly stem from participants’ self-assessments of their ability to draw on their own resources in the context of stressful events (Zhou et al., 2021).
The COVID-19 pandemic has brought unique challenges for caregivers. The associated pandemic control measures and the changes in daily life may have further challenged caregivers’ resilience, leading to a consequent increase in stress (Beach et al., 2021; Fusar-Poli et al., 2022). Studies found resilience to be associated with adaptive coping strategies in older adults that in turn predicted lower stress (Vannini et al., 2021). However, circumstances of the pandemic might challenge what is considered adaptive coping strategies so far, as Fuller and Huseth-Zosel (2020) found emotion-focused coping strategies to be adaptive in older adults during the pandemic, although Galiana et al. (2020) found emotional well-being being negatively influenced by emotional coping in older adults outside the pandemic. The global health crisis linked to the COVID-19 pandemic has repeatedly required (physical) social distancing since March 2020. These measures change and challenge everyday life and daily routines, with numerous consequences for the individual, and particularly for informal caregivers as described in the following paragraph.
Indeed, the impact on caregivers is manifold: The caregiver and the person in need of care have been faced with new adversities, including a reduced number of external resources that are also harder to access (Budnick et al., 2021). In a recent article, we summarized the impact of the COVID-19 pandemic on caregivers of people living with dementia and examined resilience in these caregivers (Geschke et al., 2021).
Internationally, increases in stress-related symptoms such as anxiety, depression, and sleep disorders as well as physical strain due to the pandemic have been reported in up to two thirds of caregivers (Barguilla et al., 2020; Beach et al., 2021; Cagnin et al., 2020; Carcavilla et al., 2021; Masoud et al., 2022; Tsapanou et al., 2021; van Maurik et al., 2020). Many older people stopped receiving medical care and nursing, leading to increased stress and anxiety as well as caregiver burden and a reduction in quality of life in caregivers (Giebel, Lord, et al., 2021; van Maurik et al., 2020). A longitudinal study in the UK revealed that in older people and people living with dementia, the utilization of social support services decreased shortly after the lockdown measures were imposed but increased again in the following 12 weeks. Over this period, anxiety decreased, well-being increased, but cases of depression rose in caregivers and people in need (Giebel, Pulford, et al., 2021). Other studies reported that female caregivers had more anxiety, depression, and sleep problems during the pandemic, but the prevalence of anxiety and depression was lower in caregivers with a higher level of education and those who were married (Carcavilla et al., 2021; Li et al., 2020, 2021; Tsapanou et al., 2021).
Mental health in the general population in Germany at the beginning of the COVID-19 pandemic was marked by a high prevalence of anxiety, depression, loneliness, and psychological distress related to more screen time, more snacking, and less physical activity (Bäuerle et al., 2020; Mata et al., 2021). In another nationwide community sample of adults from Germany, higher restrictions due to lockdown measures, a greater reduction of social contacts, and greater perceived changes in life were associated with higher mental health impairments (Benke et al., 2020). Furthermore, a review about mental health in Germany showed mixed results, which tend to indicate a largely resilient adult population with a proportion of vulnerable individuals (Mauz et al., 2021).
Resilience seems to be linked to changes in caregiver distress due to behavioral and psychological symptoms of people living with dementia, with one study reporting an association between greater resilience and a lower deterioration of distress among caregivers (Carbone et al., 2021). Moreover, resilience appears to exert a strong impact on the severity of depression and anxiety in caregivers of people living with dementia. For instance, caregivers with high resilience reported lower levels of depression and anxiety before the first lockdown but had significantly increased levels of anxiety during the first lockdown compared to those with low baseline resilience (Altieri & Santangelo, 2021). Lower levels of resilience and a higher functional dependence of people living with dementia predicted higher levels of caregiver burden during the lockdown (Altieri & Santangelo, 2021). In another study, resilience was significantly lower in caregivers than in non-caregivers during lockdown, and lower caregiver resilience represented the strongest predictor of individual and family distress (Fusar-Poli et al., 2022).
In sum, there is mounting evidence that resilience has shaped informal caregivers’ coping during the adversity of the COVID-19 pandemic (Altieri & Santangelo, 2021; Carbone et al., 2021; Fusar-Poli et al., 2022; Palacio G et al., 2019). However, most of this evidence is cross-sectional in nature and there is a lack of studies exploring whether resilience is also associated with different trajectories in coping and adaptation over time. In the present study, we therefore examined the influence of individual resilience on (1) the caring situation and caregiver burden during the pandemic in comparison to before the pandemic, (2) individual coping-related resilient behaviors during lockdown, and (3) perceived stress and depression in the first and the second lockdown, and the trajectory of perceived stress and depression from the first to the second lockdown.
Methods
Ethical approval for the study was granted by the ethics committee of the State Medical Association of Rhineland-Palatinate (allowance number: 2020-15286). The survey was registered with the German Clinical Trials Register (identifier DRKS00024621). Concerning ethical aspects, the data was collected and processed anonymously to allow for a maximum of data privacy and minimize social desirability effects. At the beginning of the online survey respectively in the introduction to the printed questionnaire, the purpose of the survey was explained. A study responsible contact was available for all participants in case help and support was needed.
Study Design and Materials
An exploratory, partly retrospectively survey of caregivers regarding their situation during the COVID-19 pandemic in Germany was conducted using printed questionnaires and a respective online version on the SoSci survey platform. The target sample were informal caregivers. Therefore, the questionnaire was sent out to Nursing Counseling Centers. A prepaid return envelope allowed for anonymously sending the questionnaire back. The online link was shared on the website of our institution, in internet forums of caregivers and was sent out by email to institutions that work with caregivers with a request to share the link.
The survey was specifically developed for the purpose of the present study based on validated questionnaires and empirical evidence on caregiver burden and caregiver coping (Adelman et al., 2014; Jones et al., 2019; Palacio G et al., 2019; Wu et al., 2021; Wuttke-Linnemann et al., 2021). It includes questions about the demographic characteristics of the caregiver and the person in need of care, the care situation (caring with professional support [yes/no], average hours of caring per week [<20/20–40/>40], living in the same household [yes/no]) both before and during the COVID-19 pandemic, as well as coping-related resilient behaviors (fixed daily structure, positive activities, exercise, social contacts, utilization of help). Additionally, the following standardized questionnaires on resilience (BRS) (Chmitorz et al., 2018; Smith et al., 2008), stress (PSS-4) (Cohen et al., 1983; Warttig et al., 2013), and depression (GDS-15) (Yesavage & Sheikh, 1986) were employed:
Brief Resilience Scale (BRS): To assess trait resilience, we used the German version of the Brief Resilience Scale (Chmitorz et al., 2018). The scale was created to assess resilience as the ability to bounce back or recover from stress. It consists of six items (three positively worded and three negatively worded) rated on a 5-point Likert scale; total scores are the mean of all item responses and range from 1 to 5, with higher mean scores indicating higher resilience (Smith et al., 2008). Reliability has proven to be good (α = .85) (Chmitorz et al., 2018), as it was in our sample (α = .85).
Short Form Perceived Stress Scale (PSS-4): Using this questionnaire, respondents’ rate how often they have experienced stressful situations in the last 4 weeks on a Likert scale from 0 to 4 (0 = never and 4 = very often). Two of the four questions are reverse-coded. Total score is determined by adding together the scores of each of the four items giving a sum score range from 0 to 16. A higher total score on the PSS-4 indicates higher stress (Cohen et al., 1983; Warttig et al., 2013). The PSS-4 was found to be reliable (α = .77) (Warttig et al., 2013) and was acceptable in our sample (αL1 = .75, αL2 = .80).
Geriatric Depression Scale (GDS-15): The GDS-15 consists of 15 questions referring to the previous week that are answered dichotomously (Yes/No). For five of the questions, 1 point is scored if the respondent answers with “No”; for the remaining 10 questions, 1 point is scored if the respondent answers with “Yes.” The sum scores range from 0 to 15; a total of ≥5 points suggests the existence of depression (Yesavage & Sheikh, 1986). Reliability has proven to be acceptable (α = .79) (Jongenelis et al., 2007) and to be good in our sample (αL1 = .86, αL2 = .85).
Procedure
The survey was conducted between October 2020 and January 2021, that is, during the second lockdown in Germany. A total of 295,530 known cases and 9,613 deaths existed in Germany on October 1, 2020, at the beginning of the survey. On January 30/31, 2021, at the end of the survey, there were a total of 2,225,686 known cases and 57,718 deaths in Germany (COVID-19 Coronavirus Pandemic, 2023).
The questions related on the one hand retrospectively to the situation before the pandemic in December 2019 (t0) and the first lockdown starting in April 2020 (t1), and on the other hand to the time of the survey in the second lockdown (t2).
Study Sample
We received a total of 504 questionnaires, 425 online and 79 paper questionnaires. Of these, 180 questionnaires were excluded from the analysis, as fewer than 80% was completed. Of the 324 questionnaires that remained for evaluation, 249 (76.9%) had been filled out online and 75 (23.1%) on paper.
The mean age of the caregivers was 56.4 years (SD 10.6) and 85.8% were female. The mean age of the care recipients was 71.6 years (SD 19.8) and 58.0% were female. Caregivers were most often children providing care for a parent or parent-in-law (50.9%) or spouses providing care for their partner (34.0%). 92.6% of the care recipients were already in need of care before the pandemic. The average duration of care up to the time of the survey was 7.6 years (SD 6.7). 76.0% had a German care level of ≥3, which represents a high need for care (German care levels range from 1 to 5).
Data Analysis
The analyses were carried out using SPSS (version 27). To evaluate (1) differences in caregiver burden, (2) coping-related resilient behaviors, and (3) indicators of stress and depression based on the individual resilience, we performed MANOVAs using the BRS mean score as covariate. Subsequent ANOVAs were conducted to examine the relationships between individual outcomes and resilience. Effect sizes were calculated using partial η2 (0.01 = small effect size; 0.06 = medium effect size, 0.14 or higher = large effect size). Differences in trajectories over time were modeled by means of a delta score. We used the formula Δ = valuelockdown − valuepre-pandemic, such that positive values indicate that the respective value was higher during the lockdown than before the pandemic and negative values indicate that the respective value was lower during the lockdown than before the pandemic. Additionally, we used the formula Δ = valuesecond lockdown − valuefirst lockdown, such that positive values indicate that the respective value was higher during the second lockdown than during the first lockdown and negative values indicate that the respective value was lower during the second lockdown than during the first lockdown. For the graphical illustration of results, we use box plot diagrams and regression lines. Mean values and standard deviations (SD) are reported where appropriate. A significance level of α ≤ .05 was assumed.
Results
The caregivers in the current study showed relevant levels of stress and depression during both the first and the second lockdown. The mean PSS-4 score was 9.6 (SD 3.2) during the first lockdown and 8.3 (SD 3.5) during the second lockdown, and the mean GDS-15 score was 7.5 (SD 3.9) during the first lockdown and 8.5 (SD 3.8) during the second lockdown. According to the GDS-15, 67.6% (first lockdown) and 71.0% (second lockdown) of the participants had relevant symptoms of depression (GDS-15 score ≥ 5). Overall, perceived stress decreased over the course of the pandemic (Δ = −1.3), whereas depressive symptoms increased (Δ = 1.0). The mean BRS score lay at 3.2 (SD 0.8).
Hypothesis 1: The caring situation and caregiver burden experienced during the first lockdown differ based on individual differences in resilience.
Using Pillai’s trace, we found a significant effect of the BRS score on the caring situation and caregiver burden during the first lockdown, V = 0.172, F(7,289) = 8.595, p ≤ .001. Separate univariate ANOVAs on the outcome variables revealed significant differences in caregiver burden, insofar as higher resilience was associated with lower caregiver burden. No significant differences emerged regarding the caring situation per se (see Figure 1 and Table 1).

Illustration (box plots) of the relationship between resilience and caregiver burden: higher BRS scores were associated with lower caregiver burden during the first lockdown.
Results of ANOVAs Predicting the Caring Situation and Caregiver Burden Based on Individual Differences in Resilience.
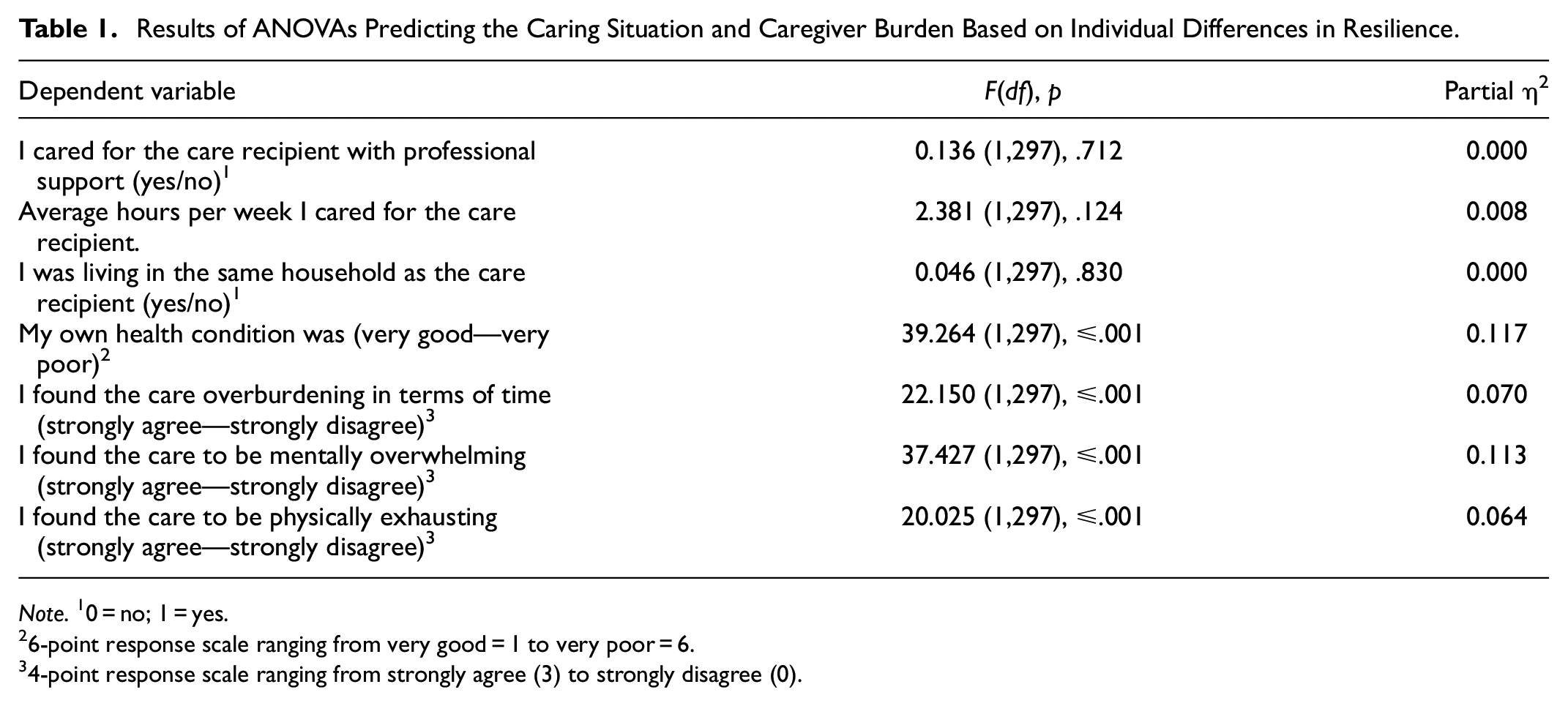
Note. 10 = no; 1 = yes.
26-point response scale ranging from very good = 1 to very poor = 6.
34-point response scale ranging from strongly agree (3) to strongly disagree (0).
Additionally, we tested whether there are significant differences, depending on resilience, in changes regarding the caring situation and caregiver burden from pre-pandemic to first lockdown. For each dependent variable, we therefore calculated a delta score (valuelockdown − valuepre-pandemic), which was entered into the analyses. Using Pillai’s trace, we found no significant effect of BRS scores on the differences in the caring situation and caregiver burden, V = 0.041, F(7,286) = 1.744, p = .099. Separate univariate ANOVAs on the outcome variables only revealed differences over time from pre-pandemic to lockdown concerning the items “I found the care overburdening in terms of time” and “I was living in the same household as the care recipient” (see Table 2).
Results of ANOVAs Predicting Changes in the Caring Situation and Caregiver Burden in the Course of the COVID-19 Pandemic Based on Individual Differences in Resilience.
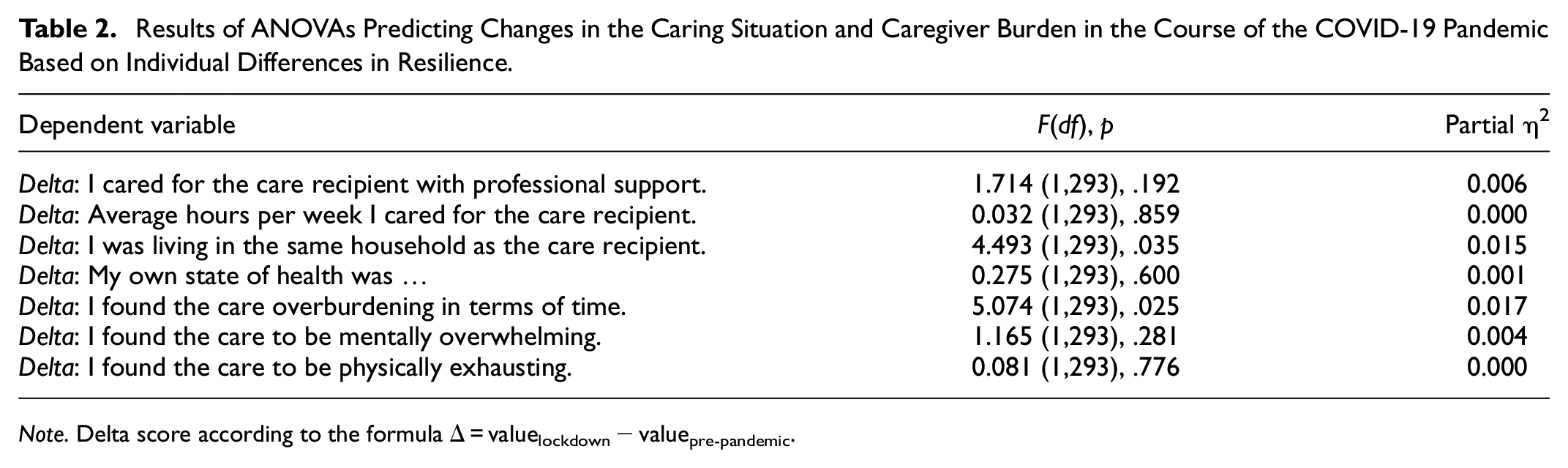
Note. Delta score according to the formula Δ = valuelockdown − valuepre-pandemic.
To illustrate the significant effect concerning the relationship between resilience and changes in time burden, Figure 2 shows that higher BRS scores were associated with a decreased time burden during the first lockdown compared to the pre-pandemic situation (see Figure 2). Concerning the relationship between resilience and changes in relocation, 94.8% of caregivers stayed in the same living arrangement with their care recipient, during the first lockdown 4.0% changed into the same household and 0.9% separated from a common household with their care recipient. Resilience was highest in the subsample that changed to the same household (mean BRS 3.50 ± 0.89), followed by the subsample that remained in the same housing arrangement (mean BRS 3.15 ± 0.84). In the subsample that changed to separate households during the first lockdown resilience was lowest (mean BRS 2.22 ± 0.10).
Hypothesis 2: Coping-related resilient behavior during the lockdowns differs based on individual resilience.
Using Pillai’s trace, we found a significant effect of the BRS score on coping-related resilient behavior during the lockdowns, V = 0.110, F(5,292) = 7.211, p ≤ .001. Separate univariate ANOVAs on the outcome variables revealed significant differences in all of the surveyed resilient behaviors during the lockdown based on individual resilience (see Table 3).

Illustration (box plots) of the relationship between resilience and changes in time burden: higher BRS scores were associated with a decrease in time burden during the first lockdown compared to before the pandemic.
Results of ANOVAs Predicting Different Coping-Related Resilient Behavior During the Lockdown Based on Individual Resilience.

Note. Response options for each statement ranging from strongly agree (3) to strongly disagree (0) on a 4-point scale.
The visual illustrations show that higher BRS scores were associated with more frequent coping-related resilient behaviors (fixed daily structure, positive activities, exercise, social contacts, utilization of help) during the lockdowns (see Figure 3).
Hypothesis 3: Perceived stress and depression differ between the first and second lockdown and in the trajectory from the first to the second lockdown based on individual resilience.
To test for differences in stress and depression in the first lockdown, the second lockdown, and in the trajectory from the first to the second lockdown based on individual resilience, we calculated a delta score (valuesecond lockdown − valuefirst lockdown), which was entered into the analyses. Using Pillai’s trace, we found a significant effect of BRS scores on the respective outcomes, V = 0.332, F(4,276) = 34.346, p ≤ .001. Separate univariate ANOVAs on the outcome variables revealed differences in stress and depression in both the first and second lockdown. In both lockdowns, higher resilience was associated with lower stress but with higher depression (see Figure 4).

Illustrations (box plots) of the relationship between resilience and coping-related resilient behaviors: higher BRS scores were associated with more frequent coping-related resilient behaviors during the lockdowns.

Illustrations of the cross-sectional and longitudinal relationship between resilience, perceived stress, and depression: results of regression analyses are presented: (a) higher BRS scores were associated with lower PSS-4 scores during both lockdowns and a decrease in stress over the course of the pandemic and (b) higher BRS scores were associated with higher GDS-15 scores during both lockdowns but not with differences in trajectories over time.
Concerning trajectories over time, resilience was associated with changes in stress (but not in depression) from the first lockdown to the second lockdown (see Table 4). Higher BRS scores were associated with lower PSS-4 scores during both lockdowns and a decrease in stress in the course of the pandemic. By contrast, resilience was associated with higher GDS-15 scores during both lockdowns but not with differences in trajectories of depressive symptoms over time (see Figure 4).
Results of ANOVAs Predicting Perceived Stress, Depression, and Changes Therein During the Course of the COVID-19 Pandemic.

Note. PSS-4 = perceived stress scale; GDS-15 = geriatric depression scale; delta score according to the formula Δ = valuesecond lockdown − valuefirst lockdown.
Discussion
Summary
This study provides insight into differences in how caregivers coped with the adversity of the COVID-19 pandemic-related lockdowns based on their individual resilience. In general, the caregivers in our sample showed relevant levels of stress and depression during both lockdowns. The mean scores on the PSS-4 and the GDS-15 were substantially higher than in other studies of caregivers outside of the COVID-19 pandemic (Bianchi et al., 2016; Potier et al., 2018; Warttig et al., 2013). The present findings support previous results related to the pandemic (Barguilla et al., 2020; Beach et al., 2021; Cagnin et al., 2020; Carcavilla et al., 2021; Masoud et al., 2022; Tsapanou et al., 2021; van Maurik et al., 2020). Importantly, resilience had a strong impact on the outcomes in the present study. While the caregiving situation per se did not differ based on resilience, higher resilience was associated with lower caregiver burden, higher frequency of coping-related resilient behaviors, and lower stress, but higher depression. The interesting finding that stress decreased while depressive symptoms increased during the course of the pandemic from the first lockdown in April 2020 to the second lockdown between October 2020 and January 2021, seems counterintuitive at first glance. However, these findings might be explained by the unique circumstances of the lockdowns and might inform depression prevention measures in this vulnerable population.
Differences in Caregiver Burden Based on Resilience
Higher resilience was associated with lower caregiver burden during the first lockdown but had no significant effect on changes in the caring situation and caregiver burden, except for a decreased time burden during the first lockdown compared to before the outbreak of the pandemic. The finding that the situation per se did not differ based on resilience, while the associated perceived time burden did differ depending on resilience fits well with the notion that in the face of adversity, resilience explains differences in appraisal and coping. Furthermore, it alludes to the idea that under special circumstances flexibility in appraisal and coping is necessary to successfully adapt. This finding has clear implications for the development of interventions to support informal caregivers and to prevent adverse health effects. Thus, strengthening resilience is worthwhile, particularly in situations where the context (e.g., a lockdown) cannot be changed. Suitable targets for interventions would be to strengthen adaptive appraisals and develop helpful coping-related resilient behaviors.
Differences in Coping-Related Resilient Behaviors Based on Resilience
Although the caring situation did not differ based on resilience, higher resilience was associated with more frequent coping-related resilient behaviors (fixed daily structure, positive activities, exercise, social contacts, and use of help) during the lockdowns. This finding supports the idea that higher resilience is associated with more adaptive coping strategies in the face of the specific adversities brought by the pandemic. The largest effect sizes were found for the maintenance of social contacts, followed by the scheduling of pleasant activities. In particular, social support and social contacts are thought to be crucial contributors to building resilience in caregivers (Palacio G et al., 2019), and it is precisely this dimension that is constantly challenged by measures to contain the pandemic. Thus, for interventions that aim to build resilience in caregivers, it is essential to find robust ways to allow for social contacts and social support. As older people might be unfamiliar with using digital innovations to maintain social contacts, low-threshold assistance and guidance must be provided to guarantee social participation despite physical distancing. Furthermore, the planning of pleasant events is an adaptive coping strategy that also has been challenged by lockdown policies. Vannini et al. (2021) found resilience as an important moderator in understanding the beneficial effect of planning, as it was associated with higher stress in people with lower resilience during the pandemic. This stresses again the importance to strengthen resilience to allow for more adaptive coping. Interestingly, Tomás et al. (2012) found that resilient coping as latent variable accounts for well-being irrespective of single coping strategies demonstrating that resilience and coping are intermingled in their positive effect on health.
Differences in Indicators of Mental Health Based on Resilience
Higher resilience was associated with lower perceived stress during both lockdowns and with a decrease in stress over the course of the pandemic. At the same time, however, higher resilience was associated with higher depression during both lockdowns. While this seems counterintuitive at first glance, it is in line with other studies in caregivers conducted before the pandemic and during lockdown (Altieri & Santangelo, 2021; Carbone et al., 2021; Dias et al., 2015; Fusar-Poli et al., 2022; Mulud & McCarthy, 2017). One previous study also reported an effect of time (before and during lockdown) on depression scores in the whole group, as well as a significant interaction between time and resilience on anxiety scores, revealing that caregivers with high resilience showed a more significant increase in anxiety levels during lockdown than caregivers with low resilience (Altieri & Santangelo, 2021). This contradiction might be explained by the fact that while high resilience in caregivers is seen as a protective factor against depression and anxiety, resilience may not exert a protective effect on caregivers’ mental state during extraordinary global events such as a pandemic, and such events may nullify the advantages of high resilience (i.e., showing lower levels of anxiety symptoms). In addition, it is likely that coping strategies that are considered adaptive outside the pandemic are not adaptive under challenging circumstances of a pandemic. Indeed, the pandemic made it more difficult to access the factors that are known to promote resilience and mental health. Moreover, the unpredictable length of the pandemic and of the related pandemic control measures might explain the increase in depression, and on the other hand, an adaptation to the situation and the development of automatic behaviors might have led to the decrease in stress. Thus, on a short-term basis, daily life functioning might be maintained, but on a long-term basis, the limitation of social structures might increase the risk of developing depressive symptoms. A further explanation might be methodological in nature, as the GDS-15 asks about depressive behaviors such as a lack of social contacts and pleasant activities, behaviors that were limited per se during the lockdowns, and especially in caregivers. Thus, the higher GDS-15 scores may be attributable to the lockdown restrictions themselves. Future studies are necessary to examine the validity of assessing depressive symptoms under lockdown circumstances.
Implications
The findings once again support the necessity to particularly focus on the needs of informal caregivers who are considered Germany’s largest unpaid care service. Our findings indicate to specifically target their psychological well-being by increasing resilience. So known “Pflegekurse” paid by health insurances for caregivers in Germany should specifically be extended by psychological interventions for caregivers (apart from the physical support caregivers need).
Limitations
While the present study provides insights into the role of resilience in caregivers’ situation considering different time points during the COVID-19 pandemic, certain limitations deserve critical consideration: First, it must be mentioned that the survey was partly retrospective, and there are indications that retrospective measures are potentially biased by personal tendencies and thus cannot be assessed objectively (Carnevali et al., 2018; O’Dwyer et al., 2017; Zhao et al., 2020). However, given the unanticipated and abrupt start of the COVID-19 pandemic, it was not possible to design a genuinely longitudinal study with different assessment waves prior to and during the pandemic. Second, the study population predominantly consisted of female caregivers. Although this reflects the unequal gender distribution among caregivers, the findings might not be generalizable to male caregivers. Furthermore, there might be a self-selection bias within the sample, as caregivers with higher stress might not have found the time to complete the survey. Future studies should also address explicitly vulnerable caregivers to analyze more heterogeneous samples.
Conclusions
This study is one of the first providing insight into the role of resilience in caregivers’ situation considering different time points during the COVID-19 pandemic. Higher resilience was associated with lower caregiver burden, a higher degree of coping-related resilient behaviors, and with lower perceived stress but also higher depression. Furthermore, stress decreased while depressive symptoms increased during the course of the pandemic depending on resilience.
Further research should investigate the needs of informal caregivers facing challenges to help building resilience and adaptive coping strategies. Resilience-promoting interventions for caregivers should be used to reduce caregiver stress and burden. Particular attention should be paid to depression prevention through tailored programs to address the needs of resilient caregivers during lockdowns. In this regard it is of utmost importance to consider the mental health of caregivers more pronounced and to acknowledge that informal caregivers not only provide physical services but also, and above all, bring emotional and psychological resources to bear on caregiving that make them particularly vulnerable.
Footnotes
Acknowledgements
The authors gratefully acknowledge Teresa Weber’s skilled work in the preparation of the study and Theresa Schmitt’s diligent work in data acquisition and data management.
Author Contributions
KG, AF, and AW-L contributed to the conception and design of the study. KG and AS organized data acquisition and the database. AS and KG performed the statistical analyses. KG wrote the first draft of the manuscript. KG, AS, and AW-L wrote sections of the manuscript. All authors contributed to manuscript revision and read and approved the submitted version.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
The study was approved by the Ethics Committee of the State Chamber of Physicians of Rhineland-Palatinate (Landesärztekammer RLP, approval number 2020-15286). Written informed consent for participation in this anonymous survey study was not required in accordance with the national legislation and the institutional requirements.
Data Availability Statement
The dataset will be made available upon reasonable request.