
Abstract
This study aims to develop a causal map of social isolation among older people that incorporates feedback to inform system-wide interventions. For this study, conducted between September 2019 and November 2019, 19 Senior Activity Centres (SACs) were first contacted, of which 10 responded and 5 agreed to participate. Based on an in-depth qualitative interview with 21 older people (50 years and older) who frequently attended Senior Activity Centres (SACs) in Singapore, a series of causal maps were generated and synthesized to describe the complex dynamic mechanisms of social isolation. Using thematic analysis based on grounded theory, 13 feedback loops (outputs of a system routed back as inputs as part of a chain of cause-and-effect) were elicited and categorized into 4 domains: (a) health and wellbeing, (b) income and unemployment, (c) relationships with family and friends, and (d) behavior and personality. These domains were found to be the most salient factors influencing social isolation. A qualitative mapping approach based on System Dynamics Methodology can provide a comprehensive understanding of the system-level factors of social isolation among older people.
Introduction
As the number of older people increases with an aging population, a higher proportion of older people become more vulnerable to social isolation. Social isolation may be defined as quantitatively and qualitatively diminished social networks—such as reduced contact and poor relationship with family and friends (Berg & Cassells, 1992; Falvey et al., 2021), that can be distinguished from loneliness, which refers to a subjective state of perceived social isolation (Hawkley & Cacioppo, 2009; Hawkley & Capitanio, 2015). The relationship between social isolation and loneliness is complex. Both are related to an individual’s level of disconnectedness (Cornwell & Waite, 2009; Cudjoe, 2020). Having a larger social network, though, possibly reduces the intensity of loneliness that a person may have but does not necessarily denote the absence of loneliness (Davies et al., 2021; de Jong Gierveld et al., 2016; National Academies of Sciences, 2020).
Given that the incidence of social isolation is known to increase with age (Cudjoe, 2020; Dykstra et al., 2005) and that social networks tend to diminish with age (Wrzus et al., 2013), the prevalence of social isolation is estimated to increase with population aging (Cudjoe, 2020; Holt-Lunstad, Robles, & Sbarra, 2017). In the United States, the prevalence of social isolation among older people in 2011 was reported to be 24%, with 4% severely socially isolated (Cudjoe et al., 2020). In Singapore, a longitudinal household survey on the health of the community-dwelling adult population aged 21 and above found 26.3% of the adult population to be socially isolated in 2017 (Ge et al., 2017). In England, the prevalence of social isolation is reported to be 13% among older people, with a higher prevalence of social isolation in younger adults (i.e., 52–59 years of age (37%), 60–69 years of age (38%) and 70–79 years of age (22%)) (Kobayashi & Steptoe, 2018). In Australia, social isolation among older people is reported to be 9.4% among individuals 60 to 64 years of age, while that for individuals 65 to 69, 70 to 74, 75 to 79 years, and 80+ years are 8.2%, 8.9%, 7.9%, and 7.9%, respectively (Australian Institute of Health and Welfare, 2019). The high prevalence of social isolation among older people has health and economic impacts (Victor et al., 2000).
The health impact of social isolation includes, among others, coronary heart diseases and stroke (Valtorta et al., 2016), diabetes (Brinkhues et al., 2017), depression, and increased mortality (Choi et al., 2015; Holt-Lunstad et al., 2015). A systematic review and meta-analysis of longitudinal observational studies by Valtorta et al. (2016) found that poor social relationships were associated with a 29% increase in the risk of incident coronary heart disease and a 32% increase in the risk of stroke. The UK Biobank study (Hakulinen et al., 2018) that followed 479,054 participants over 7 years found that persons reporting social isolation and loneliness had 1.4-fold to 1.5-fold increased risk of incident AMI or Stroke; while social isolation was associated with 1.5-fold increased risk of mortality after AMI or Stroke. On diabetes, the Maastricht study (Brinkhues et al., 2017) found that socially isolated individuals have a higher incidence and prevalence of type 2 Diabetes Mellitus. Lastly, a meta-analysis of 15 studies (Penninkilampi et al., 2018) found that poor social engagement was associated with increased dementia risk. On the cost of social isolation, a study by Shaw et al. (2017) shows that, in general, Medicare spends an estimated $1,643 more annually on objectively isolated beneficiaries than on similar individuals with greater social connections. Another study (Cruwys et al., 2018) has shown that social isolation is associated with a higher frequency of primary care attendance due to poorer health, thus increasing the cost of care. Lastly, being socially isolated was significantly associated with delayed discharge from the hospital, which has a cost of care implications (Landeiro et al., 2016).
The recognition that social isolation is a risk factor for undesirable health and poor aging outcomes has led to several interventions to reduce social isolation, especially among older adults (Findlay, 2003). Addressing social isolation among older people will require developing a deeper understanding of the causal mechanisms that drive the incidence of social isolation. Achieving that will require active engagement with stakeholders to develop a shared vision for change, including a common understanding of the multiple causes of social isolation and its interrelationships and a joint approach to solving it through agreed-upon interventions. Thus, this study aims to develop a causal map that captures the multiple causal mechanisms that drive the incidence of social isolation among older people. The causal mechanism incorporates feedback perspectives to inform system-wide interventions. Feedback perspectives herein refer to the time-varying behavior of social systems created by a class of causal mechanisms referred to as feedback loops. The qualitative system dynamics model developed herein provides a detailed feedback perspective of the mechanisms that drive social isolation in Singapore from the perspective of older adults who frequently attend Senior Activity Centres (SACs). The purpose of the SACs is to provide a centralized facility where older people can interact with one another through the guidance of trained staff and to provide activity options to those who live alone or may have limited social interactions. The qualitative system dynamics model serves as a boundary object that can be used to engage stakeholders and guide them in identifying leverage points for interventions.
Background: Interventions to Address Ageing and Social Isolation in Singapore
In Singapore, an action plan for successful aging has been implemented. The plan aims to (a) improve older people’s health and wellbeing, (c) decrease social isolation and loneliness and (c) improve older people’s employment and income.
The Ministry of Health’s Healthcare 2020 master plan focuses on increasing the number of community hospitals and geriatric care teams and resources to improve the physical health of older people. At the same time, the Community Resource, Engagement, and Support Teams (CREST) intervention aims to reach out to seniors who may be at risk of dementia or depression to improve the mental health of older people. In addition, MOH’s Senior Mobility and Enabling Fund aim to provide subsidies for assistive walking devices. At the same time, the Land Transport Authority’s new Urban Planning measures include developing and building “Silver Zones,” more rest stops, and wheelchair-friendly buses for older people. Lastly, the Housing Development Board’s Senior Friendly Housing intervention aims to improve mobility by Upgrading lifts in high-rise buildings to allow older people to go out and alleviate social isolation and provide more assisted living Housing and Development Board (HDB) flats for older people.
Employment and income interventions for the elderly include the re-employment act, Skills Future, National Silver Academy, and retirement fund. A new re-employment act that aims to increase the re-employment age to 68 so that older people can work longer if they wish has been implemented. Also, Skills Future and the National Silver Academy have been implemented to create courses and learning spaces for older people to up-skill or re-skill at various polytechnics, universities, and institutes such that they can acquire skills necessary in today’s age for re-employment. In addition to existing policies, subsidies and bursaries are available to offset healthcare and living costs for older people. Finally, the Communities of Care program by the People’s Association and Community Befriending Programmes aims to create an environment that allows older people to interact, make friends, attend health talks, and engage in exercise classes. Many befriending services are run by private volunteers from private and religious organizations, including TOUCH community services and Lions Befrienders.
Methods
For this study, the qualitative system dynamics tool of causal loop diagram (CLD) was used to visualize the complex dynamic mechanism of social isolation among older people in Singapore from the perspective of older people who frequently attended Senior Activity Centres (SAC); to bring feedback perspective to understanding the causal pathways of social isolation. System dynamics modeling is a process of problem identification, causal hypothesis generation, diagramming the proposed causal relationships, translation of qualitative hypothesis into the quantitative simulation, reliability testing, and policy analysis (Ansah et al., 2013; Forrester, 1993; Hovmand, 2014). Qualitative system dynamics uses causal loop diagrams to generate casual hypotheses to visualize and understand dynamics complexity. However, quantitative system dynamics consist of interacting sets of differential and algebraic equations developed from translating the qualitative causal loop diagram to a quantitative stock and flow model from relevant empirical data to capture dynamic interrelationships (Homer & Hirsch, 2006). The system dynamics modeling approach has been used to analyze various issues in healthcare (Abas et al., 2018; Ansah et al., 2015; Ghaffarzadegan et al., 2016), health policy (Sabounchi et al., 2014) and social policy (Homer, 1993; Ng et al., 2011; Townshend & Turner, 2000).
A causal loop diagram aids in visualizing how different variables/concepts in a system are interrelated and consists of a set of variables/concepts, connectors (links/arrows), and polarity. The variables depict the concepts used to describe the system. At the same time, a connector indicates the direction of a causal relationship, and the plus (+) and minus (−) on the arrows denote the link polarity of the relationship between the two connected variables. First, older people who frequently attended Senior Activity Centres (SAC) were selected and interviewed to develop the causal map of social isolation. Second, the interview response was transcribed and coded to obtain common variables and concepts with NVIVO software. Third, the causal links/interrelationships between concepts derived from the interview were identified and organized. Fourth, we calculated the frequency of each link/interrelationship between common variables and concepts, and the variables and concepts were categorized into groups and sub-groups. Lastly, the feedback mechanisms were identified.
Selection of Participants for the Study
Qualitative interviews were arranged and conducted between September 2019 and November 2019 with older persons living in public housing estates in Singapore who frequently attend Senior Activity Centres (SAC). The purpose of the SACs is to provide a centralized facility where older people can interact with one another through the guidance of trained staff and to provide activity options to those who live alone or may have limited social interactions. For this study, a total of 19 SACs were first contacted, of which 10 responded and five agreed to participate in the study. A staff member was contacted from each center, with the research purpose explained to the staff member, who then recommended potential participants for researchers to approach and interview.
A semi-structured interview guide was developed to interview participants, with informed consent taken before the interviews. The inclusion criteria for the study are (a) individuals who attend the SACs, (b) are not diagnosed with depression or have depressive symptoms, and (c) are willing to participate in the study. We allowed participants to freely describe their thoughts relating to different aspects of social isolation and loneliness, where they could refer to themselves or others interchangeably. Interviewers paid close attention to the feelings and emotions of participants while asking questions, which may be affected by sensitive events in their own lives that may affect their emotions. Participants interviewed who admitted to having previous depressive symptoms were excluded from the study. Approval was obtained from the National University of Singapore institutional review board before any research activity was conducted.
Analytical Approach
After participants were interviewed, recordings were transcribed, coded, and analyzed thematically using Nvivo (Release No 1.4). Interviews in Chinese were translated and transcribed by two third-party translators and 1 study member and verified by one of the interviewers. To ensure alignment in the coding process, two transcripts were initially coded by two coders, discussed extensively, and cross-verified before half of all remaining interviews were coded by one study member and the other half by another member. Transcribed interviews were analyzed thematically in six steps adapted from Braun and Clarke (2006) guidelines for thematic analysis. During the coding process, codes were categorized into descriptive categories, and broad thematic ideas were further refined as more codes emerged inductively and were populated from the transcripts. The study members came together to discuss ways to iteratively group the codes as new codes emerged. Substantial discussion between the coders occurred throughout the coding process on how the codes should be described and categorized and at what level of detail. As more codes emerged, further adjustments were made to the description and categorization of the codes that provided a thematic structure.
Results
Participant Characteristics
A total of 22 participants were interviewed, and 1 was excluded because of admitting to being diagnosed with depressive symptoms. Of the 21 participants included in the study, 12 were female (57.1%), and 9 were male (42.9%). The age group of the participants is as follows: 4.7% were between ages 50 and 59 years, 42.95% were between ages 60 and 69 years, 28.6% were between ages 70 and 79 years, and 23.8% were aged 80 years and above. The average age was 71 years. For ethnicity, 71.4% were Chinese, 14.3% were Malay, and 14.3% were Indian. Four participants were single (19%), seven were married (33.3%), seven were widowed (33.3%), and three were divorced/separated (14.4%). Ten of the participants interviewed lived alone (47.6%), while six participants lived in a two-person household (28.6%), four lived in a three-person household (19%), and one lived in a four-person and above household (4.8%). A total of 10 interviews were conducted in English (47.6%) and 11 in Chinese (52.4%). Chinese, Malay and Indian respondents who spoke in English had the interview conducted in English, while Chinese participants who spoke only Chinese or Chinese and a dialect had the interview conducted in their native language.
Causal Map of Social Isolation
Based on the qualitative responses and thematic analysis, we identified 13 feedback loops, of which 12 are reinforcing feedback loops and 1 is a balancing feedback loop (see Table 1 for the notation of the causal map and definition of feedback loops). The 13 feedback loops were further categorized into four domains: (a) health and well-being, (b) income and unemployment, (c) relationships with family and friends, and (d) behavior and personality.
Shows the Overview of Notations for the Qualitative System Dynamics Model.

Social Isolation
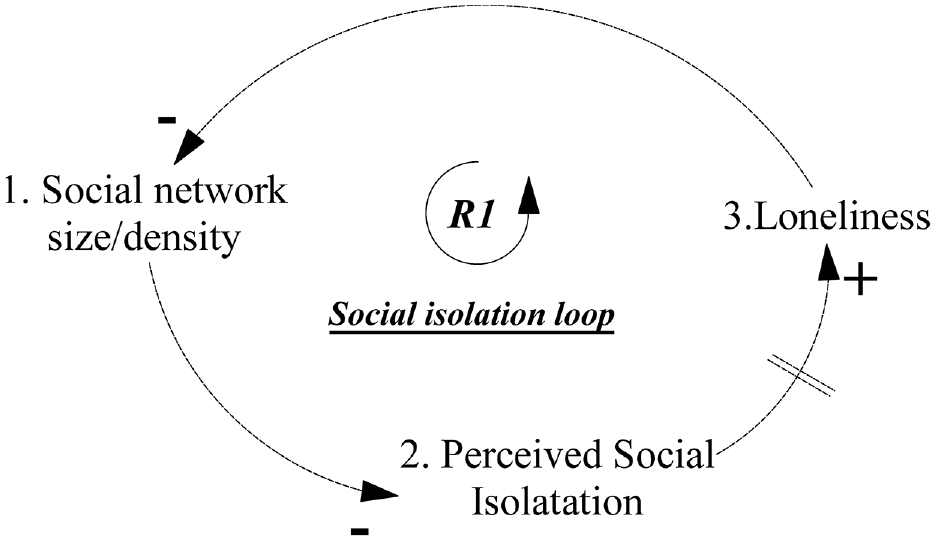
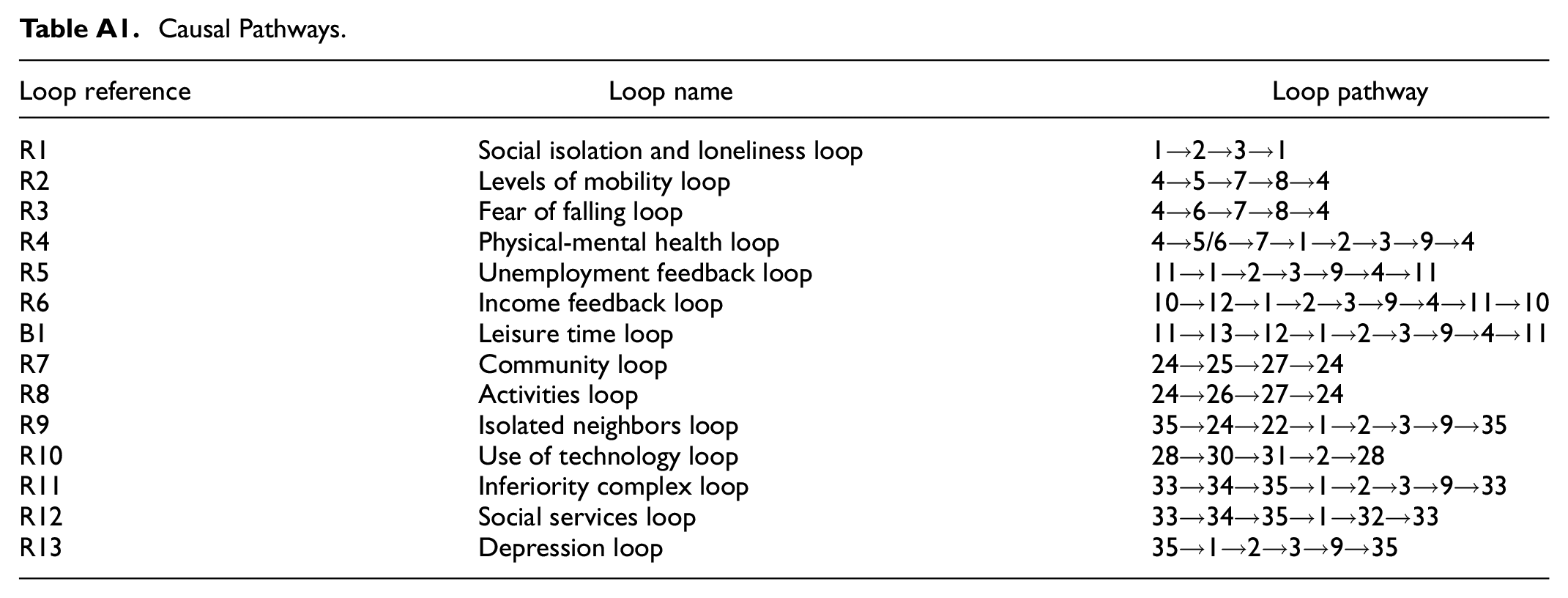
Figure 1 shows the social isolation feedback loop, which is the foundational feedback loop, and Table A1 in the Appendix shows the causal pathway. The reinforcing feedback loop R1 suggests that as the social network size/density of older adults decreases, perceived social isolation is hypothesized to rise, increasing the feeling of loneliness over time. As loneliness increases due to limited social contact, older people tend to inward-looking behavior that restricts their engagement with others, resulting in limited social network size/density. During the interviews, participants often mentioned how having few relatives, friends, or a lack of social contact creates an environment that isolates them from other people leading to a feeling of loneliness. The observation captured in reinforcing feedback loop R1 is supported by literature as cited (Cacioppo & Patrick, 2008).
Social isolation structure.
Health and Wellbeing
Figure 2 shows the generic causal structure of health and wellbeing and its impact on social isolation among older people in Singapore; Table A1 in the Appendix shows the causal pathways of reinforcing feedback loops R2, R3, and R4. The reinforcing feedback loop R2 stipulates that as frail and cognitively impaired older people increase (i.e., due to depression/poor health from loneliness and aging), physical mobility is expected to decrease, which may increase the number of homebound older people. As homebound older people increase, physical activity is expected to decrease, which may increase the incidence of frailty and cognitive impairment among older people. The reinforcing feedback loop R2 shows how physical mobility due to frailty is interconnected with social isolation. Many participants mentioned that limited mobility due to poor physical health could impede participation in movement and social activity. Participants talked about how poor physical health can make “walking very inconvenient and walking too far impossible even with a walking stick” [participant 12, male, 62 years, and participant 13, male, 79 years]. It was frequently mentioned that inactivity at home worsened physical health, as stepping outside to “breathe fresh air … [participant 11, female, 60 years] and exercise” was necessary for health maintenance and allows one’s “mind also to be clear” [participant 18, female, 83 years].

Health and wellbeing structure.
The reinforcing feedback loop R3 indicates that as frailty and cognitive impairment among older people increase, the fear of falling among frail older people is expected to increase, which may increase the tendency for older people to stay at home with little movement. As the number of older adults homebound increases, physical activity among older people is expected to decrease, possibly increasing the incidence of frailty. The reinforcing feedback loop R3 reflects how previous experiences of earlier falls, visual impairment, and hearing about an acquaintance or neighbor’s fall can generate a deep-seated fear of going out. As reported by the participants, there are many older people who “did not dare to walk” as they “worry about falling” and were “afraid of a fall” [participant 14, female, 84 years]. To these older people, leaving the house may be “very dangerous” [participant 02, female, 77 years] as it increases the chances of a person falling and causing injuries. One participant indicated that “if they fall, that is it,” so they will “go out very rarely” [participant 13, male, 79 years].
The reinforcing feedback loop R4 observed that as frail and cognitively impaired older people increase physical mobility and fear falling causes older people to be homebound, which consequently decreases their social network size/density. As social network size and density decrease perceived social isolation is expected to increase, which may increase loneliness and depression/poor mental health. As depression and poor mental health increase, the incidence of frailty and cognitive impairment among older people is expected to increase, all things being equal. The reinforcing feedback loop R4 describes how poor physical health can worsen mental health because older people are homebound. Participants talked about how “you will become depressed because you keep thinking about all sorts of things…because there is no one at home to talk to” [participant 19, male, 65 years], and that when one “sits alone, you think, think, and think” [participant 06, male, 72 years] that can even be construed as a form of “mental torture” [participant 17, female, 70 years] and that “having too many negative thoughts (makes older people bodies) become weaker” [participant 21, female, 85 years].
Income and Unemployment
Figure 3 shows the generic causal structure of income and unemployment and its impact on social isolation among older people in Singapore; Table A1 in the Appendix shows the causal pathways of reinforcing feedback loops R5, R6, and balancing feedback loop B1. The reinforcing feedback loop R5 indicates that as unemployment among older people increases, social network size/density is expected to decrease because employment is a form of social engagement that increases the social network of individuals (Gallie et al., 2003). As social network size/density decreases perceived social isolation is expected to increase, which may increase loneliness, depression/poor mental health, and frailty/cognitive impairment among older people. As frailty/cognitive impairment incidence and prevalence increase, unemployment is expected to increase. The reinforcing feedback loop R5 shows the importance of workplace experience in forming social ties. A participant indicated that “…when you are working, you know each other, then you get less stress…” [participant 20, male, 63 years]. Employment allows for establishing social ties with work colleagues that increase social engagement.

Incoming and unemployment structure.
The reinforcing feedback loop R6 suggests that as income increases, the ability to participate in social activities may increase because social activities require resources that most older people do not have. As participation in social activities increases, social network size/density is expected to rise, which may decrease perceived social isolation and loneliness. As loneliness decreases, depression/poor mental health is expected to decrease, which may decrease the incidence of frailty/cognitive impairment, thus increasing the potential for becoming employed to earn income. The reinforcing feedback loop R6 describes the role of income in the dynamics of social isolation among older people. For those who do not have savings and cannot retire, participants talked about how older people needed to maintain some level of work to earn income to meet basic needs. Participants highlighted how government grants were sometimes insufficient for basic needs, and work was needed to supplement this limited assistance. They emphasized how a lower or lack of income greatly limited their ability to participate in activities because of curtailed spending ability. A participant mentioned how for older people, “if they have no money, they cannot leave the house” [participant 19, male, 65 years] because transportation, eating, and other activities were expensive. For activities, even attending events such as a “buffet or birthday or wedding or gathering,”“they will not go, because they find it adds to their financial problem” [participant 03, male, 67 years]. They avoid having a social drink with their friends at the coffee shop, as they “do not want to go… they are scared of not having enough money” [participant 20, male, 63 years]. For older people who want to be occupied with some formal work, many participants frequently described how good physical health was crucial for employment, not only as an essential requirement but as a necessity. They perceive employers as looking for healthy, younger, and more responsive individuals and that they could not quickly meet those requirements. Participants said that they were “unable to work” due to health conditions, such as having a “numbness of … leg” [participant 04, female, 77 years].
The balancing feedback loop B1 shows that as unemployment increases, leisure time is expected to rise, which allows older people to participate in social activities, conditional on their ability to meet the cost of engaging in social activities. As the ability to participate in social activities increases, social network size/density is expected to rise, which may decrease perceived social isolation and loneliness. As loneliness decreases, depression/poor mental health is expected to decrease, which may decrease the incidence of frailty/cognitive impairment, thus increasing the potential for becoming employed to earn income. Older people who are not currently working may have more time, in general, to engage in social activities, while those who are still working have limited time. Some participants mentioned how if they were “all working” [participant 01, female, 81 years] or “busy doing office work… there is no time to socialize” [participant 11, female, 60 years].
Relationships With Family and Friends
Figure 4 shows the causal structure of the relationship with family and friends and its impact on social isolation among older people in Singapore; Table A1 in the Appendix shows the causal pathways of reinforcing feedback loops R7, R8, R9, and R10. The reinforcing feedback loop R7 stipulates that as the relationship with neighbors and social activity center friends increases, mutual help is assumed to increase, leading to a sense of community. As the sense of community among older people in neighborhoods increases, relationship with neighbors and social activity friends is expected to increase further. This relationship is assumed to increase social network size/density over time. Likewise, the reinforcing feedback loop R8 suggests that as the relationship with neighbors and social activity center friends increase, older people that engage in social activity center activities are expected to increase, which may create a sense of community among older people, thus further increasing relationship with neighbors and social activity center friends. Participants frequently expressed how the quality of relationships mattered a lot, sometimes more than the number of friends one has; as a participant said, in “life, you should have one or two very good friends where you have things you … pour (out) to him or her” [participant 02, female, 77 years]. They mentioned that “having good friends is good, (and in life) you do not need so many” [participant 19, male, 65 years] and “with a good friend you can go out and have a meal, drink coffee, go out for a walk” [participant 15, male, 84 years], and the ability to spend leisure activities with other friends improved one’s relationship. Participants also mentioned how having good neighbors was important. Some had very good relationships with neighbors, contributing to a sense of community. Participants mentioned how older adults who were neighbors helped each other, and some would “go to their neighbour…to collect groceries” [participant 01, female, 81 years], with one elderly who “ha[s] been helping their neighbour, for 7 years” [participant 05, female, 72 years]. Helping each other to run errands increased their sense of community. It strengthened neighbors’ relationships with each other, creating a positive cycle of mutual care and reinforcing the propensity to help others. One participant mentioned that “real neighbors can help … with anything.” [participant 05, female, 72 years]. A sense of community was also generated by participation in SAC activities. When older people participate in SAC activities, they “come down and see everybody” [participant 20, male, 63 years]. The familiarity of seeing neighbors regularly creates a sense of community. These relationships encourage them to go for further activities at the SAC.

Relationships with friends and family structure.
The reinforcing feedback loop R9 shows that as self-isolating behavior among older adults increases, relationships with neighbors and SAC friends are expected to decrease, which may eventually decrease social network size/density. As social network size/density decreases perceived social isolation and loneliness are assumed to increase, which may intend to increase depression/poor mental health, further exacerbating self-isolating behaviors. Participants talked about how there were still many isolated older people. Self-isolating behavior refers to older people who would rebuff invitations from their neighbors for contact, to communicate, and to take part in outside activities. Those who are isolated would “all close their doors…” [participant 13, male, 79 years], and even their neighbors “had never talked to them before” [participant 15, male, 84 years].
The reinforcing feedback loop R10 suggests that as the use of technology among older people increases, the gap between current technology levels is reduced, increasing older adults’ familiarity with their environment. This is particularly important given the rapid deployment of technology in everyday life in Singapore—especially for communication, payments, and access to government services. As older people become more comfortable with their environment, it is assumed that perceived social isolation will decrease further, encouraging older people to adopt more technology to facilitate their engagement in the community. We asked participants how they gauged technology, namely mobile technology, and its usefulness as a social intermediary to facilitate communication. For those older people who already use technology relatively frequently and know how to use it, they found these mobile platforms to be useful in sustaining contact with family and friends. Participants talked about how the “phone is very important for old people” [participant 17, female, 70 years] as “In the past, [they] did not have mobile phones… but now one can make phone calls when not visiting, have long chats, keep in touch, and chat with each other” [participant 09, female, 58 years]. They tended to be on the phone “all the time nowadays… always with the telephone now” [participant 18, female, 83 years] to talk with their friends. Messaging apps such as WhatsApp can be used for “communicating with children” [participant 21, female, 85 years] and other family members, especially cousins, and siblings living further apart. They would “every time contact my brother, my sister, they WhatsApp me and I WhatsApp them” [participant 11, female, 60 years]. Increased connectivity strengthened relationships that otherwise would not have been possible. On the other hand, there is also a knowledge gap where some participants talked about how they or older people are unfamiliar with using technology. According to the participants, some older people “do not know how to press…the number” [participant 05, female, 72 years], “for some older people, learning computers is extremely difficult for them; it is like a barrier for them,” and “if it is too complicated, we will not know how to use (it)” [participant 21, female, 85 years]. The lack of familiarity was a source of stress that may “brood a sense of pressure.”“Now science is so advanced, you do not know how difficult… [it is] for older people…” [participant 04, female, 77 years], and they express their frustration, “but for us …sometimes it is there but I do not know how to use” [participant 10, male, 62 years] especially in “cashless place like Singapore.”
Behavior and Personality
Figure 5 shows the causal structure of behavior and personality and its impact on social isolation among older people; Table A1 in the Appendix shows the causal pathways of reinforcing feedback loops R11, R12, and R13. The reinforcing feedback loop R11 suggests that as inferiority complex/low self-esteem among older people increases, it is assumed that these older people are more likely to refuse help from social services. Older people who refuse needed help tend to engage in self-isolating behavior, which is expected to decrease social network size/density. As social network size/density decreases perceived social isolation may increase, which may increase loneliness, depression/poor mental health, and the feeling of inferiority complex/low self-esteem. Participants frequently mentioned how a person harboring an ‘inferiority complex or a low self-esteem could lead to a self-perpetuating cycle of social isolation. Self-isolating behavior is when an individual deliberately declines to interact with others and tries not to connect or chooses not to when others try to engage them. Some participants referred to this as “feeling embarrassed” about their situation or “feeling scared” that others will come to know about their circumstances. When probed further, participants suggest how an “Inferiority complex” can arise from such factors as needing to use social services for poor mental health. Older people may not want to engage because “they feel inferior due to money-related issues because they do not have the ability” [participant 16, male, 63 years]. For those with family conflicts, participants indicated how older people “do not want people to ask, ‘where are your children, where is your wife?” [participant 20, male, 63 years]. They may feel embarrassed that they are in an undesirable situation, blame themselves, and compare themselves to others, leading to feelings that they are much worse off than their peers. Participants observed that those with an inferiority complex tend to refuse help, even if there are outreach services that appeal to them. When asked about social services, they claim it is “not necessary” and “they do not want to trouble anyone” [participant 09, female, 58 years].

Behavior and personality structure.
The reinforcing feedback loop R12 shows that as inferiority complex/low self-esteem increases among older people, it eventually leads to self-isolating behavior and decreased social network size/density. As social network size/density decreases, social services needs are expected to increase, which may reinforce the feeling of an inferiority complex/low self-esteem. From our interviews, 4 contributing factors (i.e., distrust of others, communication barriers, unsocial personality, and poor mental health) were associated with self-isolating behavior. Participants mentioned how older persons might not want to engage with others due to fear or past negative experiences. More specifically, they fear that others might take advantage of them. Likewise, communication barriers were mentioned as many of the older persons spoke dialect and had lower literacy levels, so finding a common medium for cordial communication may be challenging. Disparity existing between those who “cannot speak English” and those “who do not understand… (and are) scared” [participant 17, female, 70 years] leads older persons to spend more time alone. Some participants suggested that some older people may have developed a habitual avoidance of social contact and need to be integrated gradually. Participants also talked about how poor mental health may lead to persistent negative thoughts causing older people not to want to leave the house and engage with others. A participant discussed how one could “feel like do not want to wake up, do not want to work, just want to sleep only” [participant 06, male, 72 years].
The reinforcing feedback loop R13 shows that as self-isolating behavior increases, social network size/density is expected to decrease, which may increase perceived social isolation and loneliness. As loneliness increases, depression/poor mental health is assumed to increase, which may further cause older adults to self-isolate.
Discussion
Firstly, the insight that deteriorating physical health and poor mental health induce fear of falling and limit the mobility of older people, which consequently increase the incidence of social isolation, is consistent with findings from other studies. Vellas and colleagues (Vellas et al., 1997) found that older community-dwelling individuals who express fear of falling may be making a rational assessment of their risk of sustaining injurious falls, and those who have poor self-assessed physical and cognitive health are most afraid to fall. Another study by Pegorari and Tavares (2014) concludes that depression (linked to poor mental health) affects behavior and performance, reduces social participation, leads to poor physical health, and increases frailty among older people. Likewise, a bivariate correlation analysis by Burholt et al. (2017) shows that greater disability is associated with greater levels of loneliness. Lastly, Qiu and colleagues (Qiu et al., 2010) found a significant association between poor mobility and being homebound. The Qiu et al. (2010) study found that three out of four subjects unable to walk were homebound, while only one out of every five subjects who could walk at least 5 m was homebound. This insight has policy implications. Policymakers concerned with social isolation among older people should focus on interventions that increase the physical and psychological health of older people. This is important because the likelihood of older people becoming socially isolated increases with poor health. When mobility is compromised due to poor health (frail/cognitively impaired), social engagement is expected to be limited, likely leading to social isolation. The hallmark of successful aging is a sustained ability to interact physically, socially, and psychologically with the environment late into the life course. This attribute is determined by functional ability modulated by features of the surrounding environment. Hence, policies and interventions that facilitate the ability of older people to interact physically, socially, and psychologically with their environment should be prioritized.
Secondly, from the perspective of older people who frequently attended Senior Activity Centres (SAC), the ability of older people to be financially self-sustaining is closely tied to one’s ability to engage socially to reduce the risk of being socially isolated. According to Rözer et al. (2020), older people lose social contact after short- and long-term unemployment; that is, network size, contact frequency, and network support decline when they become unemployed. Evidence from Stewart et al. (2009) shows that lack of employment seems to influence people’s experience of social isolation. Further analysis showed that gender, age, educational attainment, and employment status were all significantly associated with a sense of belonging. This insight emphasizes the importance of ensuring that older people have adequate resources to meet the basic needs of life. Policy interventions that provide older people with resources or ensure that older people who are healthy and want to remain employed in appropriate industries are supported have the potential to reduce social isolation among older adults. In addition, policies that promote seamless connection/integration of older people with families and educate the population about the need to support older people have the potential to reduce social isolation.
Thirdly, insights from the interview suggest that family members are the most important ties that help older people engage physically, socially, and psychologically with their environment. This important relationship, however, is not guaranteed and may not suffice if the relationship between older people and family is strained. Older people without children and immediate family are vulnerable to limited social engagement, which can lead to social isolation. However, it was clear from our discussion with older people that friends play an important role in helping them be socially engaged. In our study, older people who frequently attended Senior Activity Centres (SAC) tend to make friends, which helps them stay socially active and avoid being isolated. Donaldson et al. (2015), found that improving relationships with children and grandchildren or having people one can rely on for help may make a significant difference in alleviating social isolation. According to Lim and Ng (2010), living alone was associated concurrently with a lack of a confidant, both of which predict loneliness; and loneliness predicts more depressive symptoms. A study by Bachrach (1980) shows that childlessness has a particularly powerful effect on the probability of social isolation. However, this effect is strongly conditioned by the health and occupational class of the older person. Litwin and Stoeckel (2014) conclude that better well-being among older European adults was found to be associated with network types with greater social capital and that accessible family ties are a strong correlate of well-being in this population. According to Wu and Chan (2012), for older people living in Singapore, living alone and residing with adult children are predictors of social isolation. The risk of social isolation is greatly reduced by public apartment neighborhood, and daily participation in public neighborhood events and contact with friends alleviates isolation more than contact with non-co-residing relatives for older people. This insight brings to bear the need to implement family-friendly policies to help older people connect with family and friends. Policies promoting the creation of centres and programs to engage older people via social interactions, memory, and physical rehabilitation can potentially reduce social isolation. In addition, programs that help older people bridge the technological gap can potentially increase social connectedness.
Lastly, the insight that some older people tend to self-isolate due to social fears that prevent social participation in activities and refusal of help from social services emphasizes the importance of implementing programs that focus on breaking down stigma through education and counseling. According to Aw et al. (2017), for older people in Singapore, attitudes about expanding their social network depended on the psychosocial adjustment of the older person to the prospect of gossip and the “trouble” of managing social relations. Mistrust was characterized by the phenomenon of “closed doors” by these older people living in housing estates, who often rejected help and felt imposed on by others interacting with them. Their mistrust extended to suspicion toward others. Interventions that focus on providing trusted familiarity, regularity of contact, and the cultivation of a conducive environment for older people who do not want to engage with other people have the potential to reduce social isolation.
The limitations of this study are that, first, only 21 older persons who frequently attended Senior Activity Centres (SAC) were included in the study, which is not representative of older persons in Singapore. Second, individuals with depression diagnoses were excluded from the study. Third, SAC members included in the study are older persons living in public housing estates and did not include older individuals living in private housing in Singapore. Future research should focus on expanding the number of older people included in the study. In addition, a study that explores the role of Senior Activity Centres (SAC) in coordinating support services for older people to alleviate social isolation will be valuable. Likewise, future studies that examine the causalities hypothesized in the resultant qualitative model will help to increase confidence in the causal map.
Conclusion
This study describes an exercise that aims to develop a deeper understanding of the dynamic of social isolation among older people in Singapore, leveraging the insights of older people living in public housing estates in Singapore who frequently attended Senior Activity Centres (SAC) with personal and societal knowledge of social isolation among older people. The qualitative system dynamics model developed herein helps to bring a feedback perspective to understanding the dynamics and complexity of social isolation among older people. The feedback perspective helps in identifying systemic issues that drive social isolation among older people, which has the potential to inform system-wide interventions and policies to improve the societal engagement of older people.
Supplemental Material
sj-docx-1-sgo-10.1177_21582440241241371 – Supplemental material for Mapping the Dynamic Complexity of Social Isolation Among Older Adults in Singapore
Supplemental material, sj-docx-1-sgo-10.1177_21582440241241371 for Mapping the Dynamic Complexity of Social Isolation Among Older Adults in Singapore by Emma Min Shuen Toh, Aloysius Wei-Yan Chia and John P. Ansah in SAGE Open
Footnotes
Appendix
Causal Pathways.
| Loop reference | Loop name | Loop pathway |
|---|---|---|
| R1 | Social isolation and loneliness loop | 1→2→3→1 |
| R2 | Levels of mobility loop | 4→5→7→8→4 |
| R3 | Fear of falling loop | 4→6→7→8→4 |
| R4 | Physical-mental health loop | 4→5/6→7→1→2→3→9→4 |
| R5 | Unemployment feedback loop | 11→1→2→3→9→4→11 |
| R6 | Income feedback loop | 10→12→1→2→3→9→4→11→10 |
| B1 | Leisure time loop | 11→13→12→1→2→3→9→4→11 |
| R7 | Community loop | 24→25→27→24 |
| R8 | Activities loop | 24→26→27→24 |
| R9 | Isolated neighbors loop | 35→24→22→1→2→3→9→35 |
| R10 | Use of technology loop | 28→30→31→2→28 |
| R11 | Inferiority complex loop | 33→34→35→1→2→3→9→33 |
| R12 | Social services loop | 33→34→35→1→32→33 |
| R13 | Depression loop | 35→1→2→3→9→35 |
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Data Availability Statement
Data that support the findings of this study are not openly available due to potentially identifiable information of the participants and will be available from the corresponding author upon reasonable request.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.