
Abstract
Breastfeeding, endorsed by religious, cultural, and scientific evidence, experiences divergent rates in Jordan due to substantial sociodemographic and cultural variations. Our aim is to explore the predictors and barriers that affect BF practices among mothers in Southern Jordan, in order to insight the healthcare providers to identify these barriers in order to increase awareness for the initiation and continuation of breastfeeding. A cross-sectional study was conducted among 380 mothers with infant 2 weeks to 6 months old. Data were analyzed using descriptive statistics and multinomial logistic regression. Findings revealed exclusive breastfeeding at 24%, mixed feeding at 57.63%, and artificial feeding at 18.42%. The study illuminated pronounced barriers in socio-environmental factors (1.65 ± 0.32), infant factors (1.63 ± 0.37), and maternal (1.59 ± 0.27). Predictors encompassed maternal age, education, employment, province, income, family member, delivery mode, and prior breastfeeding experience. In South Jordan, mixed feeding was the commonest way. Mothers’ work and lack of nursery at the workplace was the most noticeable factor. This study equips healthcare providers to recognize barriers hampering breastfeeding among Jordanian mothers, enabling informed strategies to enhance awareness and sustain breastfeeding initiation and continuation.
Plain Language Summary
Breastfeeding, endorsed by religious, cultural, and scientific evidence, experiences divergent rates in Jordan due to substantial sociodemographic and cultural variations. Our aim is to explore the predictors and barriers that affect BF practices among mothers in Southern Jordan, in order to insight the healthcare providers to identify these barriers in order to increase awareness for the initiation and continuation of breastfeeding. A cross-sectional study was conducted among 380 mothers with infant two weeks to six months old. Data were analyzed using descriptive statistics and multinomial logistic regression. Findings revealed exclusive breastfeeding at 24%, mixed feeding at 57.63%, and artificial feeding at 18.42%. The study illuminated pronounced barriers in socio-environmental factors (1.65 ± 0.32), infant factors (1.63 ± 0.37), and maternal (1.59 ± 0.27). Predictors encompassed maternal age, education, employment, province, income, family member, delivery mode, and prior breastfeeding experience. In South Jordan, mixed feeding was the commonest way. Mothers’ work and lack of nursery at the workplace was the most noticeable factor. This study equips healthcare providers to recognize barriers hampering breastfeeding among Jordanian mothers, enabling informed strategies to enhance awareness and sustain breastfeeding initiation and continuation. Our study has several limitations. Firstly, its cross-sectional design relies on retrospective reporting of BF practices, potentially introducing bias. Additionally, despite employing random sampling of health centers, the generalizability of our findings is restricted by the use of convenience sampling.
Introduction
Breastfeeding stands as a cornerstone of infant health and well-being, an assertion bolstered by the World Health Organization’s (WHO, 2021a) recognition of it as the paramount means to ensure a child’s health and survival. Nevertheless, despite its paramount importance, diverse impediments exist that undermine the seamless practice of BF. Rooted in its physiological advantages, BF emerges as not only the optimal sustenance for newborns but a practice that bestows enduring benefits upon both infants and mothers. It provides a wide range of benefits for infant growth, immunity, development, and quality of life that extends to adulthood, like reducing the risk of developing obesity (Horta et al., 2015; Pang et al., 2019; WHO, 2021b), in addition to maternal health; it may aid in reducing the risk of postpartum hemorrhage and postpartum depression with the reduction of breast and ovarian cancers and type 2 diabetes mellitus (Chowdhury et al., 2015; UNICEF, 2018).
Aligned with these imperatives, WHO and the United Nations Children’s Fund (UNICEF) underscore the significance of early initiation of BF and exclusive breastfeeding (EBF) for up to 6 months. This commitment has been reinforced through initiatives such as the Ten Steps to Successful Breastfeeding (TSSB) program, advocating for comprehensive breastfeeding practices within healthcare institutions (Ducharme-Smith et al., 2021; UNICEF, 2018; WHO, 2018).
The Ten Steps are a set of recommendations and practices with a strong emphasis on obstetrics hospitals to prevent free and reduced-price milk substitutes in these facilities; inform pregnant women about the importance of BF with early start of skin-to-skin contact; not to introduce any additions of milk or other drinks to the newborn during a stay in the hospital; not to separate the it from his mother by cohabitation within 24 hr; BF on demand and without a schedule. Implementation of these steps will simplify and increase mothers’ insistence on initiation and continuation of BF (WHO, 2018).
Globally, approximately 44% of newborns between the ages of 1 to 6 months are exclusively breastfed, however few have access to safe and nutrient-dense complementary foods (WHO, 2021b). Against this global backdrop, the scope of BF practices in Jordan warrants exploration. Within a nation where over 9 out of 10 infants are breastfed in their first year, exclusive BF remains a practice by only 26% of mothers, stressing the need for deeper insights (Department of Statistics and ICF International, 2018; UNICEF, 2020). Previous research has shown that BF barriers play an important role in mothers’ initiation and continuation of BF at 6 months. The route of birth, as well as the knowledge and attitude of the mother also affect BF (Hasan et al., 2021). Also a suitable place for lactation and breast milk storage are significant factors for facilitating breastfeeding (Elyas et al., 2017; Evangelista, 2020).
The social-cultural practices and beliefs impact mothers’ knowledge and attitudes toward BF are known to influence infant feeding (Amanya Mutuli, 2016). Introducing pre-lacteal feeds and providing water mixed with sugar are challenges rooted in cultural traditions that have persisted over time (Hamlan et al., 2015; Jarrah & Bond, 2007).According to previous studies, BF former experiences plays a major role in selecting feeding patterns and can add in difficulties impeding BF initiation and continuation later (Asiodu et al., 2016; Hinson et al., 2018; Huang et al., 2019; Khasawneh & Khasawneh, 2017). One of the most common barriers in Arab countries is the embarrassment to breastfeed in a public place which result in early cessation or choosing not to breastfeed at all (Asiodu et al., 2016; Huang et al., 2019; Nguyen et al., 2021); Conversely, insufficient familial support from perspectives such as husbands, grandmothers, and mothers-in-law can overcome barriers and influence initiation and continuity of BF significantly (AL-Sagarat et al., 2017; Joseph & Earland, 2019; Hinson et al., 2018; Okafor et al., 2017). Thus, understanding present BF practices and barriers becomes imperative. This study aimed to explore predictors and barriers that affect breastfeeding practices among mothers in southern Jordan in order to insight the healthcare providers to identify these barriers and to increase awareness for the initiation and continuation of breastfeeding.
Materials and Methods
Research Design
This study used a cross-sectional descriptive design because it is the most appropriate one to explore a large sample from different areas at a certain time to explore the predictors and barriers that affect breastfeeding practice in south Jordan.
Setting and Relevant Contexts
This study was conducted in the southern region of Jordan, encompassing five comprehensive governmental health centers situated within four distinct rural and semi-rural provinces: Al-Karak, Al-Tafila, Ma’an, and Al-Aqaba. The demography of these provinces encompasses women of reproductive age (aged 18–49 years), and the health service infrastructure includes comprehensive governmental health centers that cater to maternal and child health needs. These centers offer services such as vaccination, infants, and children growth and developmental assessments. The study conducted by Altamimi et al. (2017) reported that within the Al-Karak province, 71.2% of participants had attempted BF, yet only 51 (20.9%) had exclusively breastfed during the first 6 months.
Sample
Mothers seeking healthcare services at comprehensive health centers situated within the southern region of Jordan, whose infants age is between 2 weeks and 6 months were selected during their routine visits for infant’s vaccination, growth, and development clinics, utilizing a convenience sampling approach. Convenience sampling was chosen due to its practicality and accessibility in our specific research context, allowing us to efficiently gather data from a readily available population.
Inclusion criteria encompassed Jordanian nationality, maternal age exceeding 18 to 45 years, absence of chronic medical conditions, residency in the designated cities, with healthy singleton infants, and willingness to actively participate in the research. Exclusion criteria involved mothers who delivered infants prematurely, with multiple gestations, and those with newborns admitted to neonatal intensive care or hospitalization. These exclusions aimed to mitigate potential factors that could impact the standard breastfeeding practices.
The determination of the sample size was conducted utilizing the model proposed by Steven Thompson, resulting in a sample size of 380 participants. This calculation was predicated on the volume of visitors to comprehensive health centers in the southern region of Jordan throughout the year 2020.
Data Collection
Face-to-face structured questionnaires to verifying participant eligibility was performed in a private setting to ensure confidentiality and was in the Arabic language. Data collection occurred from February 2022 till May 2022 by the researchers. A written consent was secured from all participating mothers and were informed that the duration of the questionnaire is about 15 to 20 min.
Measurement
The study questionnaire developed by the researcher constructed in alignment with prevalent BF barriers identified in previous literature for both maternal demographic details, a comprehensive assessment of BF barriers including maternal, infant, and socio-environmental factors. A total of 22 items were identified (Balogun et al., 2015; Nguyen et al., 2021) across three distinct dimensions, each offering two response options including maternal-related barriers (12 items), infant-related barriers (4 items), and socio-environmental-related barriers (6 items). To ensure face validity, the questionnaire items underwent rigorous review by three experts. The internal consistency assessment was undertaken by calculating Cronbach’s alpha coefficient, yielding a value of 0.846 for BF-associated barriers.
Ethical Consideration
Ethical clearance from the Ministry of Health under reference number 2022/1557 was taken.
Data Analysis
Statistical analyses were conducted Utilizing IBM SPSS Statistics (version 26). Using descriptive statistics were employed to synthesize the sociodemographic characteristics of the participants, alongside detailing the prevalence of artificial, BF, and mixed feeding practices.
Descriptive statistics, in the form of mean ± SD, were applied to both individual item scores and the aggregated mean score. Subsequently, the scale scores underwent classification into two discrete categories based on their mean values representing either low perceived barriers or high perceived barriers. This categorization was presented in terms of both frequency and percentage, enhancing the clarity of interpretation.
Following the identification of breastfeeding barriers, a multinomial regression model was deployed, integrating nine sociodemographic variables. These variables were treated categorically, with the highest category within each variable serving as the reference point. Marital status was purposefully excluded from this analysis due to singularities in the matrix. The aim of this selective reporting was to streamline the presentation of results, highlighting solely those predictors that bore statistical significance within the context of the outcomes table.
Operational Definition of Study Variables
The concept of BF practice encompasses the classification of infants based on their feeding regimen, which includes exclusive BF, formula feeding, or a combination of both. This classification is determined by the proportions of infants exclusively breastfed, those solely formula-fed, and those on mixed feeding regimens.
The breastfeeding barriers are defined as the factors restricting the mother’s breastfeeding behaviors. The barriers measured by 22 items covered infant, maternal, and socio-environmental factors adopted by previously published studies (Balogun et al., 2015; Nguyen et al., 2021).
Breastfeeding predictors from demographic data refer to characteristics or factors related to a mother’s background or socio-economic status that are believed to influence her likelihood or ability to breastfeed her infant (Khasawneh & Khasawneh, 2017).
Results
Participant’s Socio-demographic Characteristics
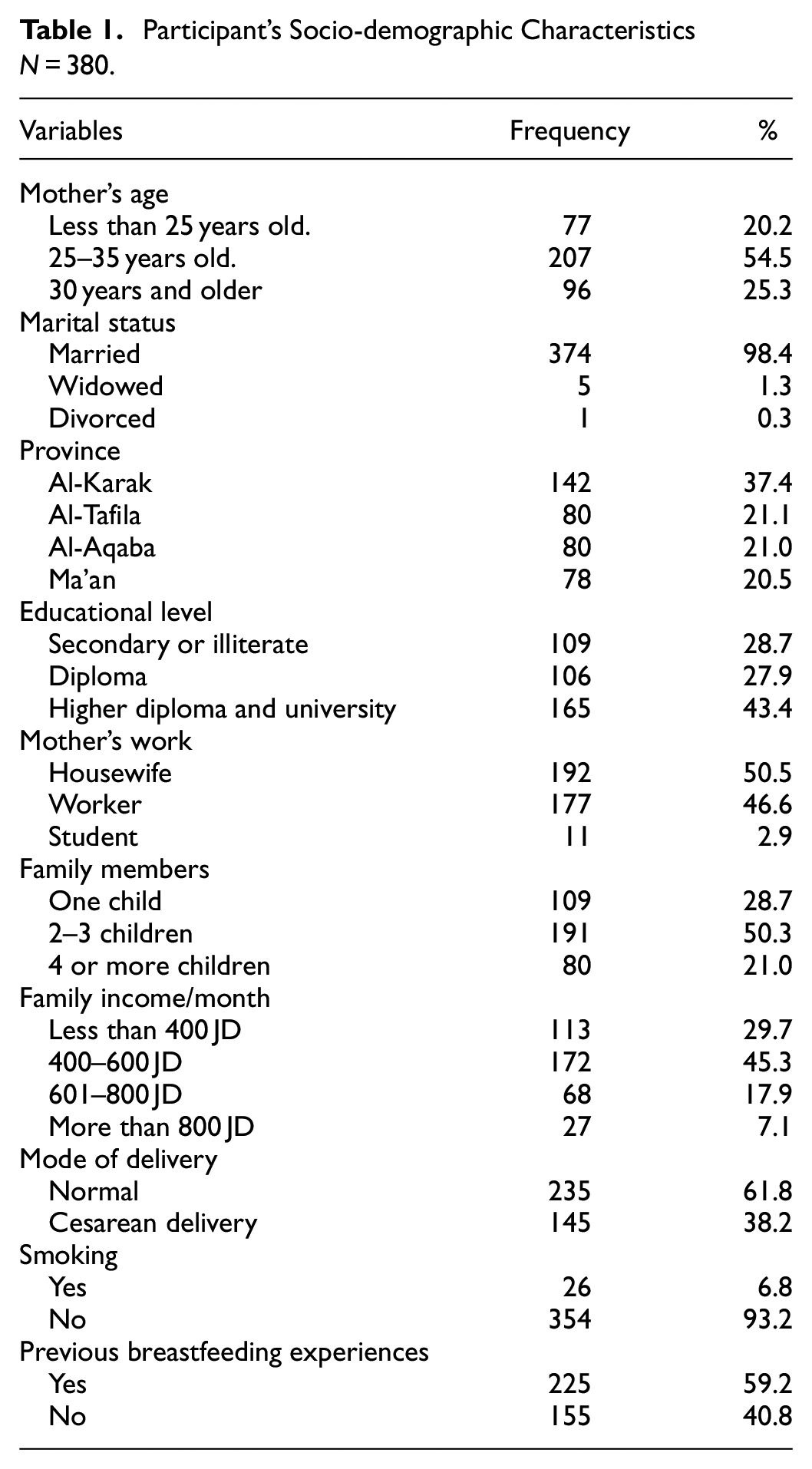
A total of 380 mothers from four provinces in Southern Jordan participated in the current study. More than half of the sample, specifically 207 (54.5%), fell within the age range of 25 to 35 years. The vast majority of participants, precisely 374 (98.4%), reported their marital status as married. Among the mothers, 354 (93.2%) identified as non-smokers, and approximately 142 (37.4%) resided in the Al-Karak province.
Conversely, a notable proportion, 165 (43.0%), held higher diploma and university degrees. In terms of maternal occupation, almost half of the sample, 192 (50.5%), identified as housewives. Family size distribution revealed that 191 (50.3%) of the mothers had 2 to 3 children in their households. Furthermore, 172 (45.3%) reported a monthly income falling within the range of 400 to 600 Jordanian Dinars.
Regarding childbirth, the majority, 235 (61.8%), delivered their infants through vaginal route, 225 mothers (59.2%) had prior BF experience. A detailed overview of the study participants’ characteristics is presented in Table 1.
Participant’s Socio-demographic Characteristics N = 380.
Breastfeeding Practices in Southern Jordan
The findings presented in Figure 1 depict the distribution of feeding practices among the participants. From the total participants, 91 individuals (23.95%) exclusively practiced BF, while 70 of them (18.42%) opted for artificial feeding. The majority of the sample, encompassing 219 (57.63%), embraced mixed methods.

Pattern of feeding.
Barriers to Breastfeeding Items Analysis
The barrier items were divided into three dimensions with two answer options (yes or no): Specifically, these dimensions comprised maternal-related barriers, comprising 12 items; infant-related barriers, comprising 4 items; and socio-environmental barriers, comprising 6 items. The scale scores were divided based on the mean score into two categories (perceived low and high barriers) and expressed in frequency as a percentage.
The Maternal-Related Barriers
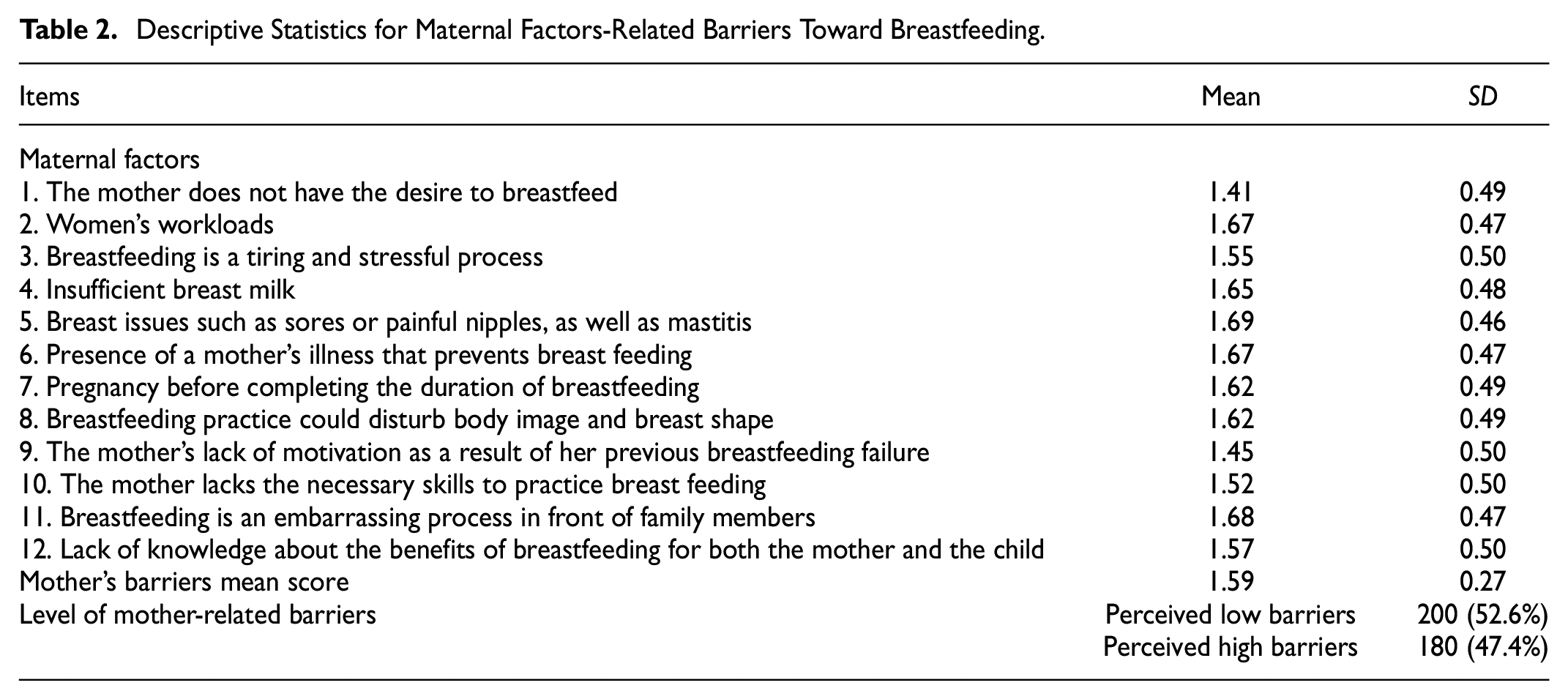
As shown in Table 2 result shows that the mother’s related factors dimension had the lowest mean (1.59 ± 0.27). Perceiving breast problems like sores or painful nipples and mastitis and shying from feeding in front of others were a mother’s barriers to breastfeeding with a mean of (1.69 ± 0.46) and (1.68 ± 0.47), respectively. In contrast, mothers who did not get the desire to BF, had the least barrier (1.41 ± 0.49); after categorizing the scale mean score, the results showed that more than half of the sample, 200(52.6%), had low perceived barriers compared with 180(47.4%) who perceived a high barrier.
Descriptive Statistics for Maternal Factors-Related Barriers Toward Breastfeeding.
The Infant-Related Barriers
Table 3 result shows the presence of a congenital infant abnormality such as cleft lip or palate had the highest infant barrier to feeding (1.67 ± 0.47). At the same time, babies rejecting breast milk accounted for the lowest perceived infant barrier (1.59 ± 0.49) after categorizing the scale mean score; the results showed that more than half of sample 216 (56.8%) have high perceiving barriers compared with 164 (43.2%) perceiving a low barrier.
Descriptive Statistics for Infant Factors-Related Barriers Toward Breastfeeding.

Socio-Environment Related Barriers
The results in Table 4 show that mothers’ work and lack of nursery at the workplace had the highest two barriers (1.79 ± 0.41) and (1.79 ± 0.40), respectively, while vigorous promotion of infants’ formula milk, powder, and other breast milk substitutes had the lowest socio-environment barriers for breastfeeding (1.52 ± 0.50). After categorizing the scale mean score, the results showed that 140(36.0%) participants had low perceived barriers compared to 240 (63.2%) participants who perceived a high barrier.
Descriptive Statistics for Socio-Environment Factors Related Barriers Toward Breastfeeding.

The Predictors Associated With BF Practices Among Mothers in Southern Jordan
The study investigated the predictors associated with breastfeeding practices among mothers in Southern Jordan. Nine socio-demographic variables were included in the multinomial regression model, treating them as categorical variables with the highest category as the reference. Marital status was excluded from the analysis due to singularities in the matrix, aimed at enhancing the interpretability of the output. Only significant predictors are presented in Table 5. The results demonstrate that the model with the complete set of predictors outperforms the null model (X2[10] = 536.064, p < .001). Approximately 21.2% of the variance in the dependent variable is collectively explained by mother’s age, education level, work status, province of residence, family income, family size, mode of delivery, smoking status, and previous breastfeeding experience.
The Predictors Associated With Breastfeeding Practices.
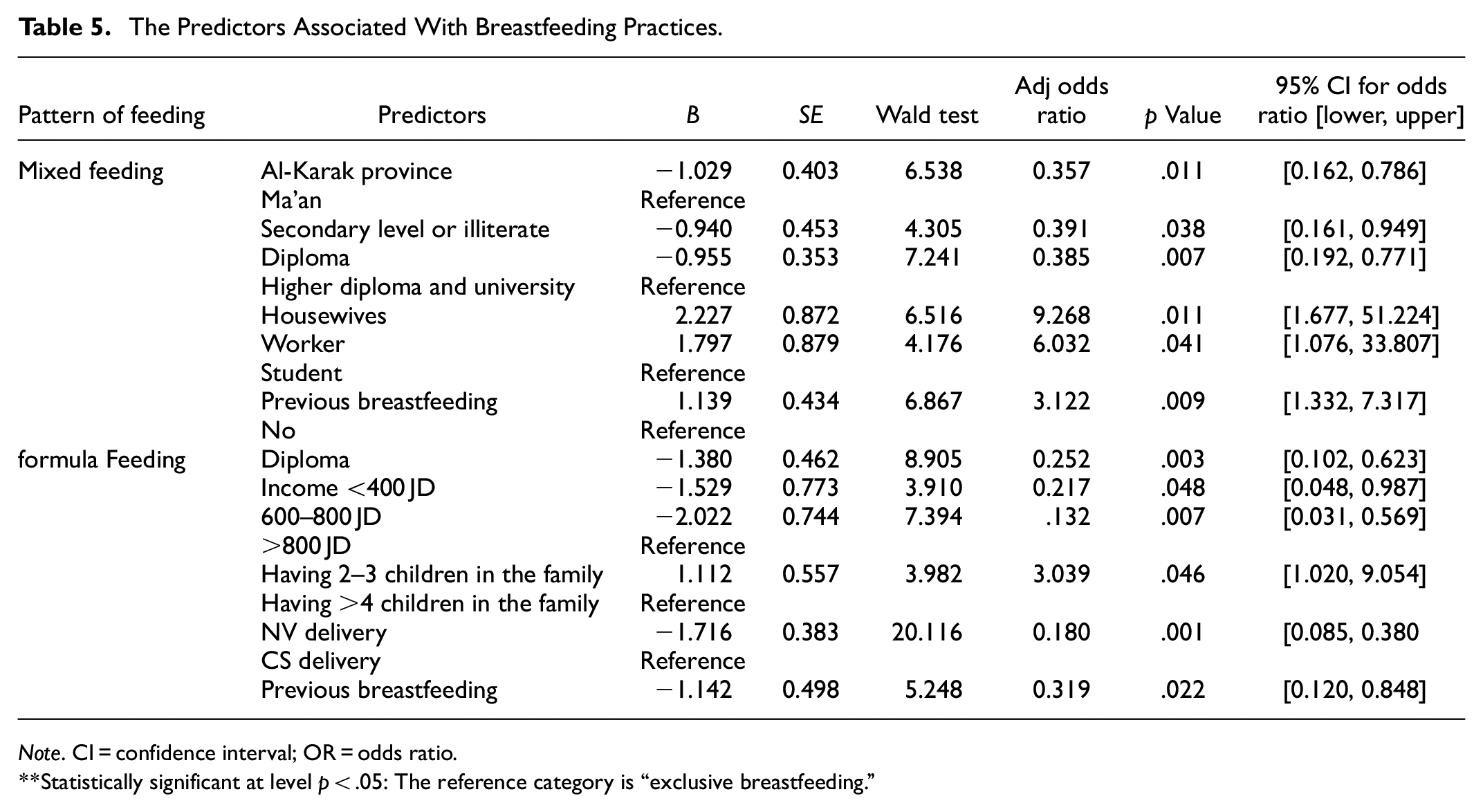
Note. CI = confidence interval; OR = odds ratio.
Statistically significant at level p < .05: The reference category is “exclusive breastfeeding.”
The findings in Table 5 reveal that individuals residing in the Al-Karak province were 64.3% less likely to opt for mixed feeding methods compared to those in the Ma’an province (Adjusted Odds Ratio [AOR] 0.357, 95% Confidence Interval [CI] [0.162, 0.786]). Additionally, individuals with secondary or lower educational levels (AOR 0.391, [0.161, 0.949]) and diploma holders (AOR 0.385, [0.192, 0.771]) were 60.9% and 61.5% less likely, respectively, to choose mixed feeding methods over breastfeeding when compared to those with a higher diploma or university education.
Furthermore, housewives (AOR 9.268, 95% CI [1.677, 51.224]) and working mothers (AOR 6.032, [1.076, 33.807]) were more likely to select mixed feeding methods over breastfeeding when compared to mothers who are students. Additionally, mothers with prior breastfeeding experience were 3.12 times ([1.332, 7.317]) more likely to choose mixed feeding methods. Conversely, neither maternal age, family income, family size, mode of delivery, nor smoking status emerged as significant predictors (p > .05).
On a different note, the likelihood of opting for artificial feeding over breastfeeding showed a 74.8% decrease for diploma holders (AOR 0.252, 95% CI [0.102, 0.623]) compared to those with a higher diploma or university education. Similarly, individuals with a monthly income of <400 JD (AOR 0.217, [0.048, 0.987]) and 400 to 800 JD (AOR 0.132, [0.031, 0.569]) were 78.3% and 86.8% less likely, respectively, to choose artificial feeding compared to those with an income >800 JD.
Regarding family size, mode of delivery, and previous breastfeeding experience, the results indicate that mothers with 2 to 3 children in the family were 3.03 times (95% CI [1.020, 9.054]) more likely to opt for artificial feeding over breastfeeding compared to those with >4 children. Mothers who had a vaginal delivery were 82.0% less likely to choose artificial feeding (AOR 0.180, [0.085, 0.380]) compared to those who underwent a cesarean section. Similarly, mothers with breastfeeding experience were 68.1% less likely to opt for artificial feeding (AOR 0.319, [0.120, 0.848]) compared to those without. However, maternal age, work status, province of residence, and smoking status did not emerge as significant predictors (p > .05).
Discussion
Our study delves a comprehensive discussion for the observed BF practices and the array of factors influencing these practices among mothers in Southern Jordan. The significance of BF as the optimal source of infant nutrition is widely acknowledged, and our findings further underscore the importance of understanding the barriers that impact the prevalence of BF.
In our study, we identified several key associations. BF prevalence was positively linked with prior BF experience and family size, but inversely correlated with cesarean delivery, maternal education level, maternal employment, and family income. Notably, approximately 23.9% of mothers exclusively breastfed their infants during the study period, mirroring the national average of 25.5% in Jordan. This aligns closely with WHO guidelines for favorable exclusive BF rates (Department of Statistics and ICF International, 2018).
In 2017, Altamimi et al. reported a 20.9% exclusive BF rate up to 6 months. Meanwhile, the Aqaba region showcased a 19.8% rate for exclusive BF for the same period (Dabbour, 2019). Notably, the northern part of Jordan demonstrated a higher rate, with 33% of infants being exclusively breastfed at 6 months (Khasawneh & Khasawneh, 2017).
When assessing breastfeeding (BF) practices across the Middle East, our findings reveal a notable alignment with rates observed in Iraq and Egypt, while simultaneously uncovering distinctions of significance. In particular, our results mirror global trends, as demonstrated by the parallel rates found in countries like Iraq, which reported a rate of 26.47% (Kandeel et al., 2018; Sdeeq & Saleh, 2021). It is imperative to underscore the variances within this regional context. For instance, Iran boasts the highest rate at 56.4%, a phenomenon potentially attributable to its extended maternity leave policy, affording mothers a generous 6 months compared to Jordan’s 3 months, supplemented by 2 weeks of paternity leave (Alzaheb, 2017; Behzadifar et al., 2019). Conversely, Abu Dhabi reported the lowest rate at 16.9%. This divergence could be attributed to shorter paid maternity leave periods during the study; however, it is noteworthy that recent legislation in the United Arab Emirates has introduced extended fully paid maternity leave periods, ranging from 2 to 3 months (Al Ketbi et al., 2018).
From a global perspective, the exclusive breastfeeding rate in Ghana has seen an encouraging increase, with 66.0% of infants under 6 months benefitting from exclusive breastfeeding (Asare et al., 2018). This upswing signals progress and emphasizes the dynamic nature of breastfeeding practices on a global scale.
Examining the spectrum of feeding practices, we observed an 18.42% prevalence of artificial feeding in our sample group, a figure lower than previous studies, which was less than that reported by Khasawneh et al. (2017), who found that (24%) of infants received artificial feeding, and 25.4% in Aqaba, Jordan (Dabbour, 2019). However, in a recent study conducted in Erbil city, the rate of artificial feeding was 10.1% (Sdeeq & Saleh, 2021).
In contrast, mixed feeding, a customary practice in many Arab nations, was observed among 57.63% of mothers in our study. This prevalence demonstrated slight deviations when compared to rates reported in Iraq (63.4%) and Saudi Arabia (51%) (Orabi et al., 2017; Sdeeq & Saleh, 2021). Conversely, in Egypt, a significantly lower proportion (12.7%) resorted to mixed feeding, with a preference for exclusive breastfeeding among mothers (Kandeel et al., 2018).
Crucially, our study identified various barriers affecting BF initiation and continuation. Cultural perceptions and societal norms play a pivotal role. Mothers’ reluctance to breastfeed in public or in the presence of family members stems from deeply ingrained beliefs. This finding resonates with similar studies conducted among different cultural groups like a previous study among African-American women (Hinson et al., 2018). In addition, Jordanian culture discourages BF in a public places (Altamimi et al., 2017; Hamlan et al., 2015). In China, some people found it acceptable to breastfeed in public places; however, others consider women’s breasts as sexual organs and should be hidden from public view (Zhao et al., 2017).
Breast-related issues, including sores, painful nipples, and mastitis, emerged as frequently reported barriers by mothers in southern Jordan in the current study, which is consistent with previous studies (Elyas et al., 2017; Hamlan et al., 2015; Hinson et al., 2018). Surprisingly, even with access to medical assistance, mothers still encounter difficulties. This highlights the need for enhanced post-discharge support and adherence to the Ten Steps to Successful Breastfeeding (WHO, 2018).
Regarding infant-related barriers, the primary obstacle identified by mothers in Southern Jordan, based on their perception and with the highest score, is the presence of congenital abnormalities, such as cleft lip or palate, which can hinder breastfeeding. This finding aligns with a study conducted in Vietnam, where it was similarly observed that infant illness is strongly associated with suboptimal breastfeeding practices (Nguyen et al., 2021).
It is evident that a cultural myth regarding breastfeeding exists among mothers in southern Jordan. This myth revolves around the belief that infants feel hungry after breastfeeding and do not gain sufficient weight from it. Such misconceptions stem from the perception that breast milk might lack adequate nutrition, leading to concerns about the adverse effects on the mother’s health and subsequently prompting the initiation of artificial feeding. These findings align with previous studies conducted in the United Arab Emirates, Iraq, and Jordan, which also identified these misconceptions as the primary reasons for discontinuing breastfeeding (Al Ketbi et al., 2018; Hamlan et al., 2015; Sdeeq & Saleh, 2021). To address this issue, step 8 of successful breastfeeding emphasizes training mothers to identify the signs of their children’s desire for nourishment, cuddling, and rest, and enables them to respond according to the child’s needs (WHO, 2018).
When considering the socio-environmental aspect, the primary reason for discontinuing breastfeeding is mothers’ work obligations, coupled with the absence of workplace nurseries. These findings align with several studies conducted on the subject (Al Ketbi et al., 2018; Hamlan et al., 2015).
In our study, the barrier of “Mothers who do not have the desire to breastfeed” was reported the least. This finding is consistent with a previous study conducted in California, where mothers expressed feelings of shame and guilt for being unable to breastfeed their infants (Asiodu et al., 2016).
A small percentage of the mothers in our study highlighted the lack of family or partner support as a barrier to breastfeeding. This finding mirrors those observed in developed countries (Asiodu et al., 2016; Hinson et al., 2018) and Middle Eastern countries such as Jordan, Saudi Arabia, and Iraq (Khasawneh et al., 2020; Orabi et al., 2017; Sdeeq & Saleh, 2021). Consequently, it is essential to provide instructions and interventions that encourage husbands and grandmothers to actively support breastfeeding.
Our study identified some demographic characteristics that predict success or act as barriers to BF. The mode of delivery is one of the main factors affecting breastfeeding. Mothers who gave birth vaginally used less artificial feeding than mothers who gave birth via cesarean section, which is consistent with previous research conducted in China, Iran, and Jordan (Behzadifar et al., 2019; Chen et al., 2018; Khasawneh & Khasawneh, 2017 was the main barrier to initiation and continuation of BF among these mothers. Therefore, these mother’s needs help and advice after delivery (Kim et al., 2017).
In our study, mothers with previous BF experience were less likely to choose artificial feeding than BF explained by previous practice and their ability to balance the family’s needs with the infant’s need; which was one of the main predictive factor for the success BF. This finding is inconsistent with other studies (Huang et al., 2019; Khasawneh & Khasawneh, 2017).
Mothers with diplomas and secondary levels are less likely to select mixed feeding and artificial feeding methods as opposed to BF compared with mothers with higher diplomas and university degrees. This is consistent with findings from studies conducted in Iran and Ghana (Asare et al., 2018; Behzadifar et al., 2019). And in contrast with a study conducted in China which revealed that higher education levels are associated with a high prevalence of breastfeeding (Li et al., 2021). This guides us to focus on mothers with higher educational levels to increase their ability to breastfeed and to identify the barriers that prevent them from practicing breastfeeding. Mothers with lower educational levels can be educated by conducting workshops and health education programs on breastfeeding benefits and techniques.
Finally, our study explains the complex interplay of factors shaping breastfeeding practices among mothers in southern Jordan. It highlights the need for targeted interventions that consider cultural, social, and economic determinants. Our findings offer valuable insights for policymakers, healthcare professionals, and researchers, emphasizing the importance of comprehensive support systems to foster optimal breastfeeding practices.
Limitation
Our study has several limitations. Firstly, its cross-sectional design relies on retrospective reporting of BF practices, potentially introducing bias. Additionally, despite employing random sampling of health centers, the generalizability of our findings is restricted by the use of convenience sampling.
Conclusions
In summary, this study has yielded valuable insights into the breastfeeding practices and barriers faced by mothers in four Provinces of South Jordan. The prevalence of different feeding methods was examined, with a specific focus on identifying predictors and barriers associated with not exclusively breastfeeding.
The findings indicate that mixed feeding is the predominant method of feeding in South Jordan. The decisions made by mothers to not exclusively breastfeed are influenced by various barriers that hinder this practice. It is crucial to address these barriers in order to promote breastfeeding.
The implications of this research extend to healthcare professionals, policymakers, and stakeholders. Healthcare providers, such as nurses and midwives, can utilize these findings to recognize the barriers that impede exclusive breastfeeding and tailor their educational efforts accordingly. We recommend implementing prenatal and early postpartum education programs that enhance maternal knowledge about breastfeeding.
Additionally, integrating regular lactation consultant counseling sessions, particularly for new mothers, is highly recommended. Creating a supportive work environment that provides clean, private, and safe spaces for lactation is a critical aspect of promoting exclusive breastfeeding. Policies that enable and encourage breastfeeding within workplaces should be emphasized.
To ensure continuous skilled lactation support, we advocate for the development of seamless systems that connect hospitals and community healthcare settings. This collaboration can significantly contribute to enhancing breastfeeding practices and support.
In essence, our study highlights the importance of addressing barriers to exclusive breastfeeding in South Jordan. By promoting education, supportive policies, and continuous lactation support, we can foster a culture that prioritizes optimal infant nutrition and maternal well-being.
Footnotes
Acknowledgements
I greatly appreciate the advice and encouragement of my chairperson, Professor Hala Obeidat. Appreciation is expressed to Mu’tah University, Al-Karak, Jordan, Jordanian Royal Medical Services (JRMS), and Princess Muna College of Nursing.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Statement
This study was approved by Ministry of Health (Reference Number 2022/1557).
Data Availability Statement
The datasets generated during and/or analyzed during the current study are available in the Zenodo repository 10.5281/zenodo.14052087.
References
 ]
]