
Abstract
This study aimed to design and validate a professional development environment model based on a task-centered approach in medical education. Accordingly, a mixed research design was used, and a qualitative content analysis was performed using a synthesis research method to identify the elements and components of the proposed model. Furthermore, a descriptive survey method was employed to validate the model from the point of view of experts. For the purposeful selection of resources considering the identification of the components of the professional development environment model based on the task-centered approach, authentic scientific documents indexed in databases, such as Scopus, Science Direct, Springer, Google Scholar, ProQuest, Emerald, and PubMed from 2000 to 2022 were reviewed, and 48 documents were selected. Then, they were analyzed using open coding and axial coding. To validate the proposed model, 20 specialists in radiology, medical education, and educational sciences were selected as a sample. The data were collected through an 8-item researcher-made questionnaire the content validity of which was confirmed by calculating S-CVI and CVI. According to the analysis, 4 main components and 14 sub-components were extracted, which led to the design of the desired model. The findings in the quantitative part also showed that the presented model has high internal validity in the field of medical education. Therefore, it is suggested to use this model as an innovative strategy and guidance for medical professionals.
Plain language summary
Professional Development Environment Model Based on Task-Centered Approach
The attainment of a model for designing the learning environment in the field of medicine is of significant importance. Therefore, this study aimed to design and validate a professional development environment model based on a task-centered approach in medical education. The development of a professional development environment model based on a task-centered approach including four components of process factors, contextual factors, content factors, and learning outcomes. The findings of content validation indicated that the provided model had the necessary validity in medical education. The proposed model of the professional development environment based on the task-centered approach has content validity and can be a guide for educational designers and specialists in the medical field.
Introduction
One of the goals of medical education and its broad term, professional development, is to train students with the capabilities needed for lifelong learning which requires an effective learning environment (Silva et al., 2012). Clinical learning environments are not always ideal for education; however, in order to get maximum benefits from clinical training and improve the learning environment, professors can create favorable opportunities and use various strategies and different teaching styles (Dent et al., 2021). Dornan (2012) in a study showed that the learning environment affects the professional development of students, and a poor learning environment is associated with increased burnout and student anxiety. When medical students move from the classroom to clinical practice environments, their roles and learning challenges change dramatically from a formal curriculum approach to an informal learning model in the workplace. These informal opportunities are strongly influenced by the working environment and conditions (Dornan, 2012). The increase in the number of students, the small number of clinical instructors, the varieties of talents and abilities of individuals in acquiring skills, and the lack of clinical cases for observation and practice make fewer learning opportunities available for students (Butler et al., 2009). The purpose of professional development is to improve competencies in the field of clinical skills and medical knowledge to provide the best patient care, which includes expanding and strengthening existing actual knowledge and practical skills. Moreover, the professional development environment plays an important role in the process of transferring knowledge and skills. People need to learn and then apply what they have learned in the real environment (Anshu & Singh, 2017). Accordingly, one of the effective criteria of clinical education is empowering students, followed by developing knowledge, attitude, and skills. These three components are of significant importance in complex learning and professional roles. Therefore, education can create necessary and needed competencies (MB Janssen-Noordman et al., 2006).
Ideally, students should learn professional skills in a robust professional development environment where complex assignments can be completed and practiced as integrated units. When students learn complex tasks in an integrated manner, it will be easier for them to transfer what they have learned to the reality of work environments. Therefore, a real learning environment is needed that focuses on the integration of all aspects of competencies. However, most training programs offer separate modules for knowledge and skills. Although students have acquired considerable knowledge and individual skills, they have not learned how to integrate them into simple performances. Most students state that different aspects of complex skills were addressed in a discrete and piecemeal manner and that they had little opportunity to master the coordinated performance of knowledge and skills related to complex assignments. Despite the learning research results and guidelines that support the effectiveness of integrated learning environments, systematic models for this type of instructional design are scarce (Van Merriënboer, 1997). According to Gillespie et al. (2009), assistant programs must be designed in such a way that they can implement what they have learned during their studies in reality. For this purpose and the efficiency of assistants’ performance, attention should be paid to providing conditions for their presence in clinical environments since what they learn as students is often different from what they experience directly from beginner patient care (Ginsburg, 2014). If learning is transferred correctly, it not only has no negative burden but also promotes flexibility and improves skills (Benbassat, 2014). When the acquisition of knowledge and transfer of skills is important, it leads the instructional designer or instructor to use the task-based instruction. In the task-based learning, students must apply their knowledge in a course or designed learning experience (Francom, 2017). There are many examples of educational design models that are designed for complex learning. Due to the emphasis of complex learning on problem-solving, these models can respond to this aspect of learning, and holistic educational design models take steps to achieve this goal through complete meaningful learning tasks that are based on reality and are one of the basic components for professional development in the field of health (Van Merriënboer & Kirschner, 2017). In order to design internship programs and teach complex subjects, Van Merriënboer et al. (1997) introduced the educational design model under the title of the four-component model (4C/ID). In addition, among the studies conducted, task-centered learning has been able to increase transfer learning strengthening communication and collaborative skills, as well as the ability of students to adapt to professional conditions and the real environment, and create the integration of learners’ learning and deeper learning (Rajab & AL-Dabbagh, 2011; Vakani et al., 2014).
In this learning strategy, instructional goals are based on tasks set by the health team, and learning is achieved through doing assignments by students in real clinical situations. In interacting with the real environment and people, they find an opportunity to communicate between theoretical knowledge and clinical experience (Koh et al., 2014). Previous research conducted in the field of task-centered educational environments shows a strong relationship with increasing student learning. In a study conducted by Frerejean et al. (2021), the results indicated that task-centered instructional design models, such as the four-component model, led to a rich knowledge base, and created harmony between performance and learning through the combination of learning in the educational environment and learning in the work environment (Frerejean et al., 2021). Other studies also show that task-centered learning has increased the level of knowledge and skills and improved the attitude toward the learning environment (Frerejean et al., 2021; Maggio et al., 2015; Rosenberg-Kima, 2012; Shenoy et al., 2022). The results of a study conducted by Costa et al. (2022), suggest that the use of educational programs developed with 4C/ID has a high impact on performance, regardless of the academic area, the design of the study, and the outcome. Their results also suggest that the use of the 4C/ID model should be prioritized as an instructional model in college and university learning environments (Costa et al., 2022).
Additionally, Argelagós et al. (2022), conducted a quasi-experimental study on the effects of an online task-centered course on the Information Problem Solving (IPS) skills development and self-efficacy perception of 80 graduate students in educational sciences. The IPS and four-component instructional design models have been applied for course design and development. The results indicate that after the course, the students in the experimental group outperformed those in the control group on planning and search activities (Argelagós et al., 2022) The findings of a study by Salary et al. (2022), showed that the educational intervention based on the four-component instructional design led to the effectiveness and promotion of assistants’ performance due to its realistic learning assignments in the clinical learning environment (Salary et al., 2022). Furthermore, Postma and White (2015), revealed that the four-component instructional design model provides conditions for measuring cognitive feedback considering the content and the development of the learner’s cognitive strategies, and finally, it is recommended that the model of four-component design should be considered a basis for teaching and learning in the classroom to develop abilities in clinical reasoning among dental students and in medical education (Postma & White, 2015). Yusup and Musharyanti (2022), aimed to compare the knowledge and skills in medication safety of nursing students after the medication-safety training using the 4C/ID. Training in medication safety using the 4C/ID approach could improve the medication-safety knowledge and skills of the nursing students. Moreover, it can be continuously given to nursing students in their preclinical education to better prepare nursing students to be competent in medication administration and patient safety (Musharyanti et al., 2021).
In general, this educational method is an instructional strategy for medical students who learn knowledge and practical skills in the clinical environment and alongside patients. In addition, an effective professional development program focuses on inclusive learning (Diaz-Maggioli, 2003). Medical education increasingly emphasizes acquiring complex theoretical knowledge, integrating this knowledge and skills, and applying them to new clinical situations. Although it is essential to provide students with diverse clinical practice opportunities, this is not always possible due to the lack of suitable patients, a gap between theoretical knowledge and practical skills, and a greater focus on patient safety. Also, there are many types of research related to the issue of how to teach to understand and transfer learning, as well as multiple learning methods; however, there is still a big gap between the design and implementation of instructional programs that cannot replace teaching in authentic situations. Medical students face many problems in clinical training; therefore, regarding the importance of the role of clinical training in the formation of the students’ professional competence and capability, and because the development of any clinical training model requires accurate knowledge and awareness of the existing context, much research on the effective implementation of task-centered education in learning situations and its effectiveness as a method of education is needed.
It seems that task-centered learning is an alternative framework for creating a set of learning activities designed to provide facilities for medical students and assistants to be able to use them in multiple situations leading to improved performance (Paul Griffin, 2011). Therefore, in order to facilitate learning transfer, integrate the professional competencies of the assistants, and make the design of the learning assignments real in the clinical educational environment, this study can lead to effectiveness and improvement of the assistants’ performance quality. With this background in mind, this study was conducted to design a professional development environment based on a task-centered approach, followed by investigating the content validity of the developed model.
Method
The present study was carried out in two stages. In the first stage of the research, the synthesis research approach was used to determine the components of the professional development environment based on the task-centered approach. Synthesis research, which in some cases is equivalent to qualitative meta-analysis, includes the combination of specific features and factors of research literature. Synthesis research tries to analyze the research, covers and resolves conflicts in its literature, and identifies the main topics for future research (Cooper et al., 2019). The value of this type of research is in creating a match among knowledge, needs, and skills with which combined processes are performed. This is more than putting together a bunch of information. What is emphasized is the integration of various contents in a special perceptual framework that establishes the emergence of new perspectives or relationships (Short, 1991). Therefore, the synthesis research method was used as a suitable method to design the professional development environment based on the task-centered approach. This study utilized the Roberts Synthesis Research Model using six stages on 48 qualitative studies related to the research topic in the following order: (1) Identifying the need, conducting a preliminary search, clarifying the need; (2) Conducting research in order to retrieve information; (3) Selecting, refining, and organizing studies; (4) Determining the perceptual framework and adapting it to the information obtained from the analysis; (5) Processing, synthesis, and interpretation in the form of concrete products; and (6) Presentation of results (Short, 1991). The statistical population of the model design section consisted of written sources, including books, articles, and authoritative scientific documents indexed in such databases as Scopus, Science Direct, Springer, Google Scholar, ProQuest, Emerald, and PubMed. After identifying the components of the professional development environment based on the task-centered approach and designing the initial template, the validity of the content of the template was investigated from the point of view of specialists and experts using a questionnaire survey method. The sampling was conducted in a purposeful manner, which was used for the purposeful selection of documents related to the elements of the professional development environment based on the task-centered approach from the available sources between 2000 and 2022. After collecting the sources and checking the titles and content, irrelevant sources were removed, and then, the selection and refinement of studies and selection of relevant sources were done. Accordingly, the investigation process is as follows:
Totally, 230 studies related to the keywords were selected, and 150 cases of unrelated studies were removed after examining the titles. Following that 80 abstracts of the studies were examined, and 23 studies were removed due to unrelated abstracts. Afterward, 9 cases of unrelated studies were removed after the full-text examination, and finally, 48 documents were included in the study. In the second stage, content validation of the model was done using the opinions of experts in the fields of medical education and educational sciences, which included 20 people using a survey method, CVI, and S-CVI. The minimum acceptable value for CVI was 78% or higher, and at the total level of the instrument, S-CVI/Ave was considered 0.8 and 0.9 or higher (Shi et al., 2012). The questions related to evaluating the validity of the content of the model were designed and formulated by experts in the form of a questionnaire. This questionnaire had eight questions that were graded on a Likert scale from 1 (very little) to 5 (very much). The content validity of this tool was confirmed by the opinion of experts, and its reliability was calculated by Cronbach’s alpha test of .7. SPSS software was also used to analyze the data through descriptive and inferential statistics (one-sample t-test).
Results
The thematic analysis method used to analyze and classify the findings resulted in 4 main themes and 14 sub-themes (Table 1). In the following, each component of the model of the professional development environment based on the task-centered approach is presented.
Thematic Analysis Coding Schemes.

After categorizing the results and comparing them with one another, the results were synthesized using the aggregation approach, and finally, the themes were created in Table 1. According to the themes, the most significant components of task-centered learning were identified in 4 main categories and 14 related sub-categories, including (1) Context factors, (2) Content factors, (3) Process factors, and (4) Learning outcomes. According to the elements of the professional development environment based on the task-centered approach, the proposed model was drawn, which is presented in Figure 1.
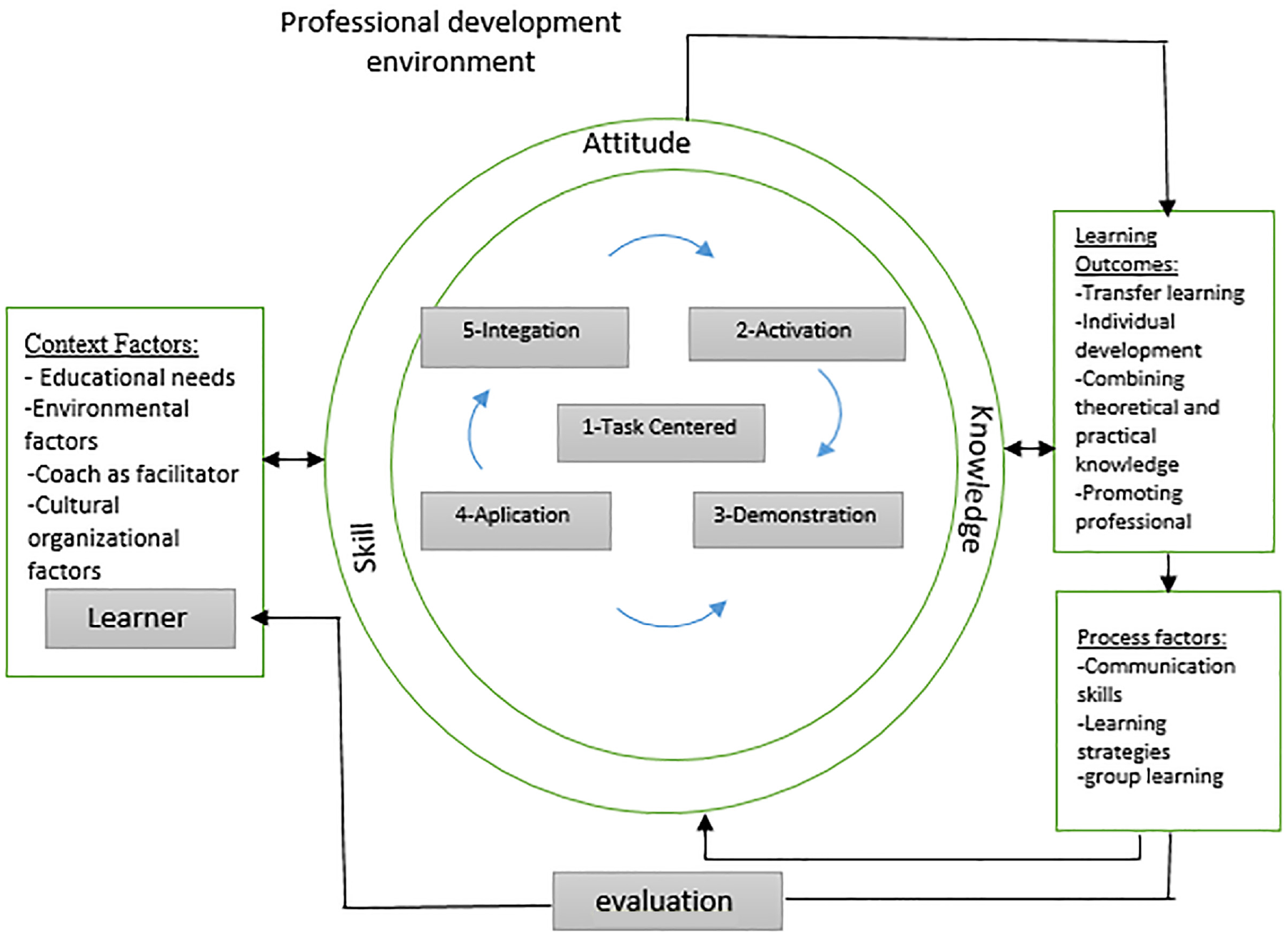
Professional development environment model based on the task-centered approach.
The First Component: Context Factors
According to the synthesis of different sources, any component that helps learners achieve professional development can be categorized as a sub-theme under a more general category called Context Factors. Although these sub-themes have previously been considered independent components in different models or as important components in task-centered learning and professional development, they can be integrated into the Context Factors component. One of the important and key factors in designing a professional development program is context factors. According to Table 1, the organization, culture, and environment in which learning takes place determine the characteristics of the context under what conditions, when, who, where, and why it takes place. The context factors identified in the present study include the analysis of educational needs, environmental factors, the role of the clinical instructor, organizational-cultural factors, and the role of the learner.
In this regard, Guskey and Sparks’ (1996) model indicate that the content of the program and the context characteristics are skills that the continuing professional development program aims to present to the learners. The program content variables are “how,” “design,” and “implementation” of the content of the professional development curriculum, and the characteristics of the context related to “who,” “when,” “where,” and “why” of the professional development program. The professional development program originates from the awareness of a professional need that directly affects the relationship between continuous professional development and progress (Guskey & Sparks, 1996). Another context factor is coaching and guidance to complete tasks for better learning transfer (Van Merriënboer & Kester, 2008). In task-centered teaching, the teacher serves as a facilitator by explaining the learning task and showing how to complete parts of the task or helping the learners. It also plays a role by recommending appropriate resources and providing coaching and feedback while learners are completing learning tasks. The role of the learners also changes to a self-directed and cooperative learner (Reigeluth & Karnopp, 2013). Another factor is the organizational-cultural component in instructional strategies in the design of professional development, which is consistent with the results of a study by Loucks-Horsley et al. (2009). They regarded context factors, such as teachers, learners and their learning needs, organizational culture, and instructional strategies effective in the design of the professional development environment (Loucks-Horsley et al., 2009).
The Second Component: Content Factors
Professional development cannot succeed without strong content. To be effective, professional development should be based on curricular and instructional strategies that have a high probability of affecting student learning (Joyce & Showers, 2002). In addition, professional development should (1) deepen the knowledge of the subjects being taught, (2) sharpen teaching skills in the classroom, (3) keep up with developments in the individual fields and in education generally, (4) generate and contribute new knowledge to the profession, and (5) increase the ability to monitor students’ work in order to provide constructive feedback to students and appropriately redirect teaching (Harwell, 2003). The content of professional development should be connected with the professional development needs of learners who are in different career stages and with the goals of professional development, in accordance with the criteria and curricula that the learners use (Alzahrani, 2008). Content represents the subject knowledge, skills, and competencies to perform professional tasks that must be acquired through participation in professional development activities (Hassel, 1999). In general, the content and effective professional development activities should include educational strategies and lead to the improvement of learners’ performance, as seen in Figure 1.
The indicators related to the content factors identified in this research are competencies, which include knowledge, skills, and attitudes. The content factors are designed based on the task-centered approach, and learning tasks are the central aspect of this approach. The four principles of activation, modeling, application, and integration are related to the application of learning tasks. Activation of prior knowledge means the activation of cognitive structures that are related to subjects and tasks that must be studied and performed. Modeling in task-centered teaching includes showing learners how to perform a learning task and also providing working and supporting information related to the learning task. The amount of modeling provided to learners gradually fades over time as learners gain expertise (Francom & Gardner, 2014). Application in task-centered education occurs as a part of the real experiences of the learning period. The application must be aligned with the desired skills for learning; therefore, the learning tasks must be designed to support the learners to perform the desired skills in order to achieve the learning goals (Van Merriënboer & Kirschner, 2017). Integration also happens as a part of the task-centered learning experience. It is a stage of learning in which learners use their new knowledge and skills in everyday life or discover new ways and ideas for using new knowledge and skills (Francom & Gardner, 2014).
The Third Component: Process Factors
The process shows the way of acquiring new knowledge and skills. Process variables are related to professional development. The methods and processes are the ways of creating and improving the amount of knowledge, attitude, skills, and behavioral changes that are appropriate to the goals of the program and are related to the level of information, as well as the experiences of the learners and the content.
Since the professional development program stems from an awareness of a need, effective assessment plays an important role in supporting learners and enhancing their ability to take on new responsibilities in other learning environments (Badri et al., 2017). Regarding the group learning component, Eraut (2004) describes three types of work activity in the professional development environment that give rise to the acquisition of knowledge and skill, namely participation in group activities (including team-work), working alongside others (and gaining a new perspective from colleagues), and tackling challenging tasks (which can increase confidence and problem-solving abilities). The next component is related to communication skills. Sharifah et al. (2009) has shown students’ positive perception of the effect of task-centered learning on acquired skills, such as interpersonal communication. Our findings are consistent with the results of many previous studies that show students’ understanding of the learning method as an important factor in strengthening their interpersonal skills, which are essential for clinical practice.
The Fourth Component: Learning Outcomes
Task-centered learning environments are the most suitable alternative for developing professional skills and facilitating learning transfer (Francom & Gardner, 2014). Moving toward the development of core competencies can help determine whether an assistant in training is practically prepared as a physician. These competencies are developed into six general areas, including the patient, medical knowledge, performance-based learning, personal and communication skills, professional ethics, and system-based performance (Hoff et al., 2004). On the other hand, complex learning seeks the integration of knowledge, skills, and attitudes, as well as the coordination of different constituent skills, and the transfer of what has been learned to daily life and the work environment. Therefore, a supportive clinical environment plays an important role in the transfer of learning, and the goal of clinical education is to provide scientific and practical experiences in an environment that facilitates the student’s learning, as well as personal and professional development.
The topics of learning transfer, personal development, integration of theoretical knowledge and practical knowledge, and promotion of professional competencies are among the outcomes of designing the learning environment based on the task-centered approach, which is an instructional strategy for subjects in education. Therefore, a supportive clinical environment plays an important role in the transfer of learning, and the goal of bedside education is to provide scientific and practical experiences in an environment that facilitates the student’s learning, as well as personal and professional development (Francom & Gardner, 2014).
The purpose of validating the content of the model is to reflect the opinions of experts and modify and improve the proposed model. In this research, the expert panel method was used for validation. In this way, the initial version of the conceptual model along with the internal validation questionnaire of the model was sent to 20 experts in the field of educational sciences and medical education in order to check the adequacy of the components. In order to statistically analyze the answers given to the questionnaire questions, one-sample t-test was used. The model’s content validity questionnaire measures eight dimensions of validity, coherence, consistency, comprehensiveness, acceptability, comprehensibility, applicability, and scalability which can be seen in Table 2.
Content Validation Questionnaire of the Professional Development Environment Model Based on the Task-Centered Approach.

The results of the one-sample t-test to evaluate the content validity of the professional development environment model based on the task-centered approach are reported in Table 3.
Results of One-Group t-Test to Evaluate the Content Validity of the Professional Development Environment Model Based on the Task-Based Approach.

The results of the one-sample t-test comparing the average of each question with the hypothetical average of the community, which is equal to 3, show that the views of experts on each question designed based on the extractive model are higher than the average, and this difference is significant at all levels of the questions related to the model (p < .001). Moreover, the model of the professional development environment based on task-centered learning has a significant positive status considering the eight criteria.
Content validity is the degree to which an instrument has an appropriate sample of items for the construct being measured and is an important procedure in scale development. The content validity index (CVI) is the most widely used index in quantitative evaluation. There are two kinds of CVI: I-CVI and S-CVI. Researchers recommend that a scale with excellent content validity should be composed of I-CVI of 0.78 or higher and S-CVI/Ave of 0.8 and 0.9 or higher. The characteristics and qualifications of the experts, process, and main results of content validity evaluation should be reported in scale-related manuscripts (Shi et al., 2012). The CVI and the overall appropriateness of the S-CVI indicate the comprehensiveness of judgments about the validity or feasibility of the final instrument. Considering that the minimum acceptable value for the CVI is 0.79, the Table 4 indicates the content validity of the model and the whole scale. In order to calculate the overall appropriateness of S-CVI, the average approach was used, and its value was calculated at 0.88 for the proposed model. Therefore, it can be concluded that the experts have evaluated the mentioned model as suitable and the model of the professional development environment based on the task-centered approach has the necessary validity.
Descriptive Indicators of the Characteristics of the Professional Development Environment Model Based on the Task-Based Approach, CVI, and S-CVI.

Discussion and Conclusion
This study was conducted to design and validate a professional development environment model based on the task-centered approach in medical education. Furthermore, the characteristics of the professional development environment were identified; accordingly, specialists and managers in the medical field could utilize this model to make decisions in the educational program design and implementation of this model. The remarkable feature of the first part of the research is to provide a comprehensive structure of the characteristics of the professional development environment, which has not been presented comprehensively and in a synthesis method in previous studies, as well as for the training of assistants. Therefore, the synthesis method was used to identify the components of the professional development environment. At this stage, theoretical foundations were collected from various sources and texts, including books, articles, research conducted on internet sites related to the subject under study, and necessary information. The data were analyzed by repeatedly reading texts and documents and using the combined analysis method. Finally, by examining the sentences and their meanings, 4 main components and 14 sub-components were obtained.
Considerations related to each of the four elements of the professional development environment model based on the task-centered approach of context factors, content factors, process factors, and learning outcomes were obtained. Considering the key role of context factors, the considerations of this component in the developed model include the analysis of educational measures, environmental factors, the role of the clinical instructor, organizational-cultural factors, and the role of the learner. Studies performed by Coffie et al. (2019), de Villiers (2016), Harwell (2003), Machado (2019), and Nawab and Bissaker (2021) also confirmed the same features. Along the same line, Gess-Newsome et al. (2003) pointed to the characteristics of the instructor, cultural and structural context, educational materials, as well as the students, and teaching topic as the field of professional development that is effective in changing knowledge and performance. The content factors are competencies (knowledge, skills, and attitude), and the content should be specific and teachable; moreover, the development of various aspects of personality should be regarded. The importance of the mentioned features has been shown in the studies conducted by Harwell (2003) and Villegas-Reimers (2003). In this regard, Garet et al. (2001) found that focusing on content knowledge is effective in increasing teachers’ knowledge and skills, and changing the classroom style (Garet et al., 2001). Additionally, Ingvarson et al. (2005) showed that focusing on content has significant direct effects on professional development (Ingvarson et al., 2005).
According to Villegas-Reimers (2003), the components of professional development include professional development goals; the context in which professional development takes place; the personal and professional characteristics of the participants; models, techniques, and implementation of processes; evaluation and measurement of the effectiveness of professional development; and infrastructure support for professional development (Villegas-Reimers, 2003). Considerations related to process factors are communication skills, designing appropriate instruction strategies, educational evaluation, and collaborative learning. In the studies carried out by Harwell (2003), Rollins (2003), and, the importance of the process dimension has been expressed as one of the dimensions of professional development.
Regarding the component of learning outcomes, the following features were stated: learning transfer, personal development, integration of theoretical knowledge and practical knowledge, and promotion of professional competencies. The results of studies by Van Merriënboer and Kester (2008), O’Halloran (2001), MB Janssen-Noordman et al. (2006), and Balapala et al. (2014) are consistent with the findings of this section. After presenting the model of the professional development environment based on the task-centered approach, the validity of the proposed model was investigated. Due to the specialized nature of the research topic, one of the best ways for validation is to use the opinions of experts, which is considered to be more of an aspect of sharing efforts and aligning with the collective wisdom of scientists in the relevant scientific field, and it is a way of enjoying their suggestions and technical opinions. In this regard, the results of the validation of the model showed that the observed T at the confidence level of 88% for all questions was significant; accordingly, the average answers of the experts were significantly higher than the average scores. According to experts, the model of the professional development environment based on the task-centered approach has sufficient validity, and the elements related to it are correctly selected. Considering that this educational model was presented for the first time in the assistantship course, much research is needed to validate the current model. Based on the results obtained from this study, it is expected that those learners who use the task-centered approach in their educational program will have many abilities, will be able to apply their learning in real environments, and use it outside the work environment since in the majority of the conventional teaching methods, there is a dispersion among what the learners learned.
Medical students learn each type of skill and knowledge separately; however, it is difficult to coordinate and apply them practically. On the other hand, by using task-centered education, the concern of student learning in different courses can be reduced, and education in medicine can be more effective. The findings of this study indicated the effectiveness of the task-centered environment, compared to traditional and common environments. Due to the emphasis on real assignments, the amount of practical participation is more than that in traditional methods; as a result, it causes the integration of theoretical and practical learning of learners, acquisition of clinical reasoning skills, improvement of skills and competencies, optimal performance and learning, and deeper learning. Educational design models can be used to teach skills and qualifications in assistants’ training programs. The four-component design model is of crucial importance in order to develop the competencies of doctors, and according to this model, sufficient attention is paid to the coordination and integration of knowledge, attitude, and skill; moreover, it is possible to transfer learning to real situations. As the findings show, each of the identified components and sub-components is crucial in the process of education and learning of learners in the field of medicine.
Limitations and Future Research Directions
In any research, due to time and setting restrictions, the researcher cannot examine all the variables or methods. Since the current study is focused on the design of the professional development environment of doctors and is extracted from documents and articles, future studies are suggested to use the interview method with experts as a source of data, and in other communities, such as teachers and students, to be able to generalize the research results to a larger statistical population and draw a more comprehensive concept of the effectiveness of the model. Furthermore, policy-makers, educational program executives, medical education specialists, and other researchers should not only review and modernize learning strategies but also all the elements involved in the professional development process and improvement of the effective learning environment, and consider them in the planning and educational design of different courses.
Supplemental Material
sj-pdf-1-sgo-10.1177_21582440231217824 – Supplemental material for Design and Validation of Professional Development Environment Model Based on Task-Centered Approach in Medical Education
Supplemental material, sj-pdf-1-sgo-10.1177_21582440231217824 for Design and Validation of Professional Development Environment Model Based on Task-Centered Approach in Medical Education by Somayeh Salary, Ali Akbar Amin Beydokhti, Morteza Karami, Parvaneh Layegh, Masoud Mahdavi Rashed and Mozhgan Mahmoudian in SAGE Open
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
Our study was approved by Semnan University of Medical Sciences and Health Services (approval no. 1398.244).
Informed Consent
All informants provided written informed consent prior to enrollment in the study.
Data Availability Statement
Data sharing not applicable to this article as no datasets were generated or analyzed during the current study.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.