
Abstract
Medical students are trained to maintain the health of patients, but such training may have undesirable effects on medical students’ personal health. This study therefore aimed to assess the health-related quality of life (HRQOL) of medical students and to determine the factors that are associated with the students’ HRQOL. The target population included all students enrolled at the Saint Louis University School of Medicine in Baguio City, Philippines, during school year 2012-2013. The measurements included the 36-Item Short Form Health Survey (SF-36) questionnaire for HRQOL, Beck Depression Inventory, abbreviated Maslach Burnout Inventory, Perceived Stress Scale, Holmes and Rahe Stress Scale, and self-report items for other exposure variables. A total of 527 medical students participated in the study. The mean scores in all of the eight domains of HRQOL ranged from 51.36 to 85.83. The highest mean scores were along the areas of physical functioning (85.83) and bodily pain (69.20), whereas the lowest mean scores were in the areas of vitality (51.72) and role limitations due to emotional problems (51.36). Depression, stress, and burnout were associated with lower scores in most of the domains of HRQOL. Medical students in our school are generally in a satisfactory state of functional health and well-being, but have a lower level of mental health as compared with physical health.
Introduction
Medical students are trained to maintain the health of individual patients and of populations. Such training is physically and mentally demanding and may have undesirable effects on medical students’ personal health (Dyrbye, Thomas, & Shanafelt, 2005). According to Weil (n.d.), medical schools foster unhealthy lifestyles; medical students suffer from sleep deprivation, poor nutrition, lack of exercise, and are placed under a considerable amount of stress. In one study, medical students were shown to have a poorer status of physical and mental health, and more anxiety, depression, and negative lifestyle changes as compared with non-medical students (Al-Dabal, Koura, Rasheed, Al-Souwielem, & Makki, 2010). Physicians are health professionals who play a vital role in a country’s health care system. It is therefore essential that physicians-in-training maintain their own well-being to better care for their patients in the future.
Assessing the overall health of individuals and populations is of public health importance. According to the Center for Disease Control and Prevention (2011), one approach to this is to make use of an expansive concept known as health-related quality of life (HRQOL). It is a multidimensional measure for evaluating physical functioning, psychological well-being, and social functioning (Calvert & Skelton, 2008). As it is multifaceted, HRQOL is in agreement with the definition of health of the World Health Organization (2013), which is “a state of complete physical, mental, and social well-being, and not merely the absence of disease or infirmity.” HRQOL has been applied to studies of various populations such as those with chronic diseases or debilitation, as well as to groups of healthy adults and health professionals.
A search for published research articles that primarily assessed the HRQOL of medical students revealed studies conducted in Canada (Raj, Simpson, Hopman, & Singer, 2000), Brazil (Paro et al., 2010), and Iran (Jamali et al., 2013), and none in the Philippines. This study therefore aimed to assess the HRQOL of medical students at the Saint Louis University in Baguio City, Philippines. Specifically, it sought to determine the status of the HRQOL of the medical students along the domains of physical functioning, role limitations due to physical health, bodily pain, general health perceptions, vitality, social functioning, role limitations due to emotional problems, and mental health; it also sought to determine factors associated with the medical students’ HRQOL.
Method
Study Design
A cross-sectional study design was used. In this design, the outcome variable, which is the HRQOL, as well as the exposure variables were assessed at a particular point in time using a questionnaire. A descriptive cross-sectional design was used to determine the status of the medical students’ HRQOL. An analytical cross-sectional design was used to determine the factors that are associated with the medical students’ HRQOL.
Study Population
The target population included all students enrolled at the Saint Louis University School of Medicine in Baguio City, Philippines, during school year 2012-2013. The total population of the students was 608. As all students were included in the study, no sampling techniques were employed.
Data Collection
Data were gathered using a questionnaire consisting of the following parts:
Assessment of HRQOL
HRQOL was measured using the 36-Item Short Form Health Survey (SF-36) questionnaire. The SF-36 is a multipurpose, short-form health survey consisting of 36 questions. It measures eight areas of health: physical functioning, role limitations due to physical health, bodily pain, general health perceptions, vitality, social functioning, role limitations due to emotional problems, and mental health. The tool produces scores for each of these eight areas. As a generic measure, this questionnaire has been useful in evaluating the health of general and specific populations as well as assessing HRQOL (Ware, 2003). Thus, it is an appropriate data gathering instrument for this study.
The SF-36 was authored by John E. Ware Jr. and was developed as a part of the RAND Medical Outcomes Study (MOS): Measures of Quality of Life Core Survey (RAND Corporation, n.d.-a). The utilization of the SF-36 has been cited in more than 4,000 published articles. It has also been acknowledged as the most widely evaluated generic patient assessed health outcome among quality of life measures. It has also been used in the description of more than 200 diseases and conditions. Translations of the instrument have been documented in 22 countries (Ware, 2003). The SF-36 has been reported to have high reliability, with coefficients exceeding .70 and even .80. There is also evidence of the instrument having adequate content validity, concurrent validity, criterion validity, construct validity, and predictive validity. The various studies on the validity of the SF-36 are cited elsewhere (Ware, 2003). A recent study has shown that the instrument is a valid and reliable tool for measuring the health status among Filipinos residing in two cities in the Philippines (Castillo-Carandang et al., 2013).
The SF-36 can be used as a self-administered questionnaire, or can be administered via a computer or personal or telephone interview. It takes only 5 to 10 minutes to complete. In this study, it was given to the medical students as a self-administered questionnaire.
Scoring of the instrument followed the two-step process as recommended by the RAND Corporation (n.d.-b). In the first step, precoded numeric values were recoded using a scoring key. Each item was scored in a range of 0 to 100. The scores represented the percentage of the total possible score achieved. In the second step, items in the same scale were averaged together to yield the eight-area (scale) scores. Missing data were not included when computing for the scale scores.
In this study, norm-based interpretation of the SF-36 was used. In this interpretation strategy, 50 is considered as the average score or norm. Scores higher than 50 are better than the general population average for all the eight scales, whereas scores lower than 50 are worse (Gandek, 2002).
Assessment of depression
Depression was assessed using the Beck Depression Inventory (BDI). This instrument was originally meant to measure depression in patients with mental illness, but it can also be used in a primary care setting. It consists of 21 questions, each question having four possible responses with scores ranging from 0 to 3. The total score of the test is a measure of the severity of depression. In a primary care setting, a score higher than 21 is interpreted as having depression. Studies have provided evidence of the validity of this tool; it is also considered to have high reliability (Encyclopedia of Mental Disorders, n.d.).
The BDI has been validated in some Asian countries such as Indonesia (Ginting, Näring, van der Veld, Srisayekti, & Becker, 2013), Korea (Yu, Lee, & Lee, 2011), and Japan (Kojima, Furukawa, Takahashi, Kawai, & Nagaya, 2002). However, a review of the literature did not reveal any validation studies of the BDI done in the Philippines.
Measurement of burnout
To measure burnout, an abbreviated Maslach Burnout Inventory (aMBI) was used. This inventory is the most widely used measure of burnout (Maslach, Jackson, Leiter, Schaufeli, & Schwab, n.d.). The abbreviated form contains only 12 out of the original 22 questions, but still assesses the same three domains, namely, emotional exhaustion, depersonalization, and personal accomplishment (McManus, Smithers, Partridge, Keeling, & Fleming, 2003). The abbreviated form includes an additional three items regarding “satisfaction with medicine,” which makes it an appropriate tool for the present study of medical students. No validation studies of the aMBI or the Maslach Burnout Inventory in the Philippines were found.
Measurement of perceived stress
Stress was measured using the Perceived Stress Scale (PSS). This is the most commonly employed questionnaire to gauge an individual’s perception of stress (Cohen, n.d.). It consists of 14 items which are easily understood and hence can be used in the general population. It has been validated in studies, particularly those dealing with health status. For example, in Asia, it has been validated among Chinese cardiac patients who are smokers (Leung, Lam, & Chan, 2010). It also has good reliability (Cohen, Kamarck, & Mermelstein, 1983).
Measurement of stressful life events
Stressful life events were assessed using the Holmes and Rahe Stress Scale (MindTools, n.d.). This is a list of 43 stressful life events that have been correlated with illness. Each stressful event corresponds to a value known as a life change unit (LCU), depending on how stressful the event is. The sum of the LCUs yields an estimate of an individual’s stress level and likelihood of illness. For this particular study, life events that were most likely to apply to medical students in the Philippine setting were included in the questionnaire. For example, divorce was not included as divorce is not allowed in the Philippines. However, no formal validation of this instrument has been conducted in the Philippines.
Measurement of other variables
The instrument also contained self-report items related to the other exposure variables. These variables were age, sex, civil status, year level, academic performance, pre-medical course, and socioeconomic status.
Data Management
The questionnaires were administered personally by the researcher accompanied by a research assistant. The questionnaires were administered at the middle of the second semester. Questionnaires were administered during regular class days and not during major examination periods.
To extract the data from the questionnaires, the responses were coded, using number codes to make the data suitable for analysis.
Microsoft Excel was used for data entry. Only one database was created. The database had one variable for each item in the questionnaire and one record for each respondent. Each participant had a unique identifier in the form of an identification number. The Microsoft Excel file was then exported to Epi Info 7 for data analysis.
Data Analysis
The main outcome variable was the HRQOL scores (continuous quantitative). Exposure variables included age (quantitative), sex (binary), civil status (unordered categorical), ethnicity (unordered categorical), year level (ordered categorical), academic performance (ordered categorical), pre-medical course (unordered categorical), socioeconomic status (ordered categorical), depression (continuous quantitative), burnout (continuous quantitative), stress levels (continuous quantitative), and stressful life events (continuous quantitative).
Prior to actual analysis, the data were checked for missing values. These were appropriately coded, so that the computer will recognize them as missing and thus exclude them from the analysis.
In the analysis of the data, the following were carried out: basic descriptive analysis in the form of means and standard deviations of the HRQOL scores along the eight scales; measures of association between the HRQOL scores and the exposure variables, t test, and null hypotheses and p values for the association between the HRQOL scores and binary variables, that is, sex, one-way ANOVA and null hypotheses, and p values for the association between the HRQOL scores and unordered and ordered categorical variables. In addition, Bartlett’s test for inequality of population variances was performed. If the p value from Bartlett’s test was less than .05, non-parametric tests such as the Mann–Whitney/Wilcoxon two-sample test or the Kruskal–Wallis test were used instead of the t test or ANOVA, respectively. Pearson’s correlation coefficient and null hypotheses and p values were used to determine the association between the HRQOL scores and quantitative variables, that is, age, depression (BDI score), burnout (aMBI score), stress levels (PSS Score), and stressful life events (Holmes and Rahe Stress Scale score).
Ethical Considerations
The research protocol was reviewed and approved by the Institutional Review Board (IRB) of the university prior to the conduct of the study. The review considered both scientific and ethical aspects of the research. The questionnaire had a cover letter that provided information on the research objectives as well as the significance and importance of the study. Participation in the study was voluntary and it was explained to the students that they had the option not to answer the questionnaire. Students were not compensated for their participation. Complete anonymity of the research participants was observed as the participants were asked not to write their names or any identifying marks on the questionnaires. Thus, specific information on the questionnaires could not be linked to specific individuals. Access to the data was limited only to the researcher and two research assistants.
Results
Characteristics of the Study Participants
A total of 527 medical students participated in the study representing a response rate of 86.7%. Most were between the ages of 19 and 24 years old (78.8%). Most were female (61.1%) and single (96.77%). The highest percentage of respondents were in first year (30.4%). In terms of academic performance, the most common grade point average range was 80 to 84. Most of the medical students studied nursing as their pre-medical coursework (55.6%). The most common combined annual income range was between PhP (Philippine pesos) 100,000 and PhP 499,999 (40.5%; Table 1).
Demographic Characteristics of the Participants.
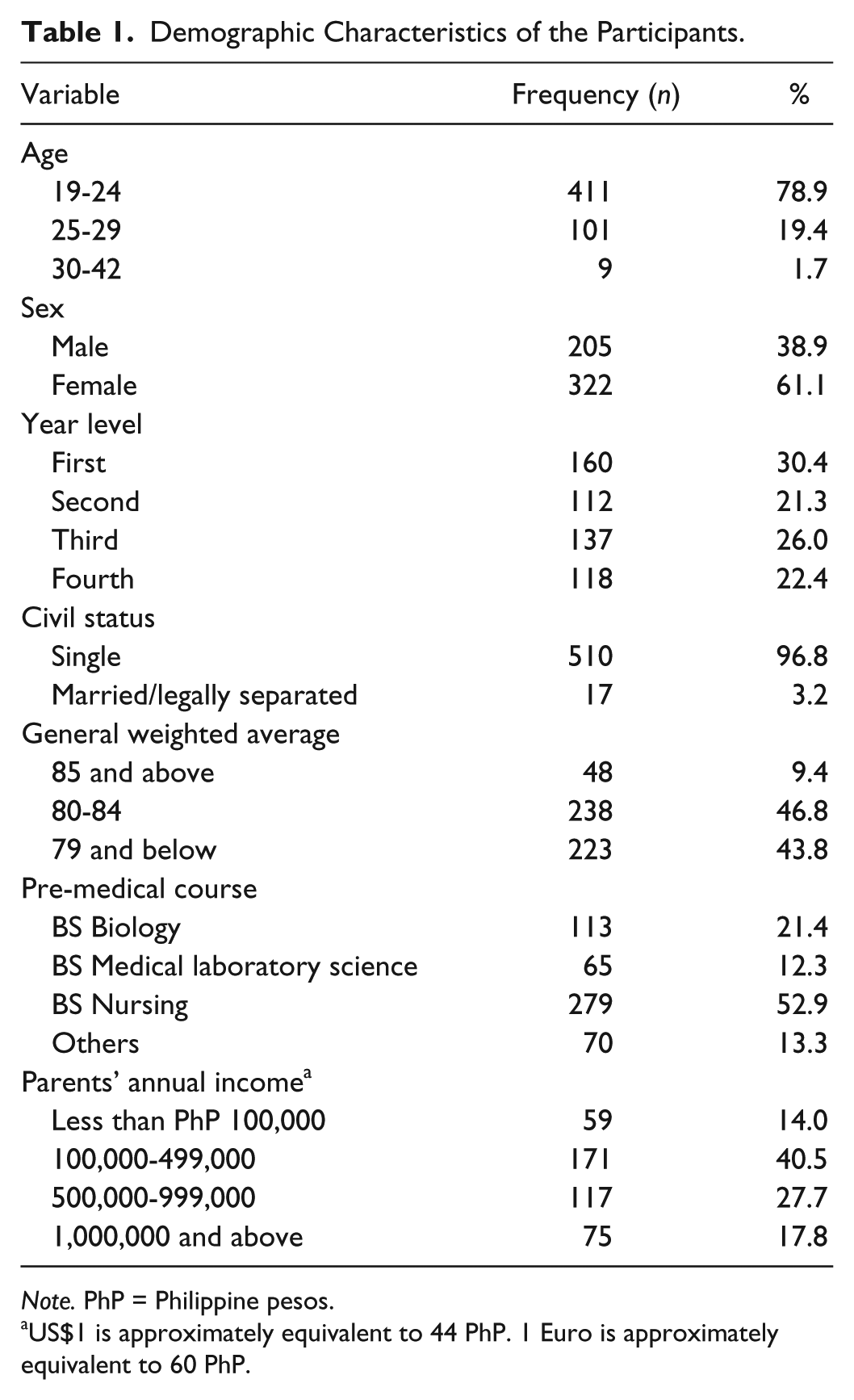
Note. PhP = Philippine pesos.
US$1 is approximately equivalent to 44 PhP. 1 Euro is approximately equivalent to 60 PhP.
The response rate in this study was 86.7%. Among the non-responders, there was an almost equal number of males and females; 40 were males and 41 were females, with a male to female ratio of approximately 1:1. The male to female ratio in each year of the medical school was as follows: first year—1:1.4, second year—1:1.4, third year—1:1.6, and fourth year—1:1.5. The overall male to female ratio in the medical school is 1:1.5. Further analysis revealed that there was no significant difference between the non-responders and responders according to sex (p = .10; see Table A1 in the appendix). Although it is possible that some students who refused to participate were symptomatic, for example, with depression, the high response rate makes non-response bias less likely.
In all, 45 students (8.5%) had manifestations of clinical depression, whereas 182 students (34.5%) had features of moderate to major stress. The medical students had a low tendency for burnout along the domains of personal accomplishment and depersonalization, but had a high tendency for burnout along the domain of emotional exhaustion. They scored relatively high in terms of satisfaction with medicine (Table 2).
Psychological Characteristics of the Participants.

Note. BDI = Beck Depression Inventory.
HRQOL of the Medical Students
The mean scores in all of the eight domains were above 50, ranging from 51.36 to 85.83. The highest mean scores were along the areas of physical functioning (85.83) and bodily pain (69.20), whereas the lowest mean scores were in the areas of vitality (51.72) and role limitations due to emotional problems (51.36; Table 3).
HRQOL of the Medical Students.
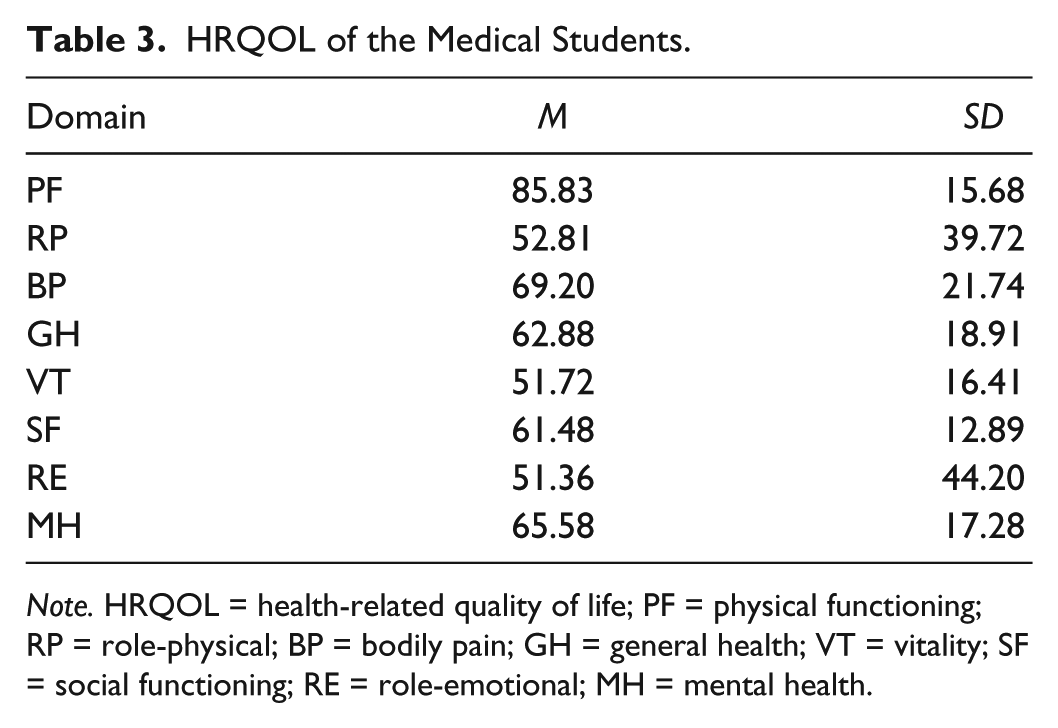
Note. HRQOL = health-related quality of life; PF = physical functioning; RP = role-physical; BP = bodily pain; GH = general health; VT = vitality; SF = social functioning; RE = role-emotional; MH = mental health.
Associations Between HRQOL and the Exposure Variables
Male students tended to have higher scores than female students along the domains of general health (p = .001), vitality (p = .014), and role limitations due to emotional problems (p = .004). There were no significant differences in the HRQOL scores among the four year levels except for the area of social functioning, where fourth-year students had lower scores as compared with the other three year levels (p < .001). There were also no associations between the HRQOL scores and academic performance, except in the domain of role limitations due to physical health where those with lower weighted averages had lower HRQOL scores than those with higher weighted averages (p = .015; Table 4).
Associations Between HRQOL and Categorical Variables.

Note. No associations were observed between the HRQOL scores and age, civil status, and parents’ combined annual income. HRQOL = health-related quality of life; PF = physical functioning; RP = role-physical; BP = bodily pain; GH = general health; VT = vitality; SF = social functioning; RE = role-emotional; MH = mental health; ns = not significant; BDI = Beck Depression Inventory.
In the Philippines, students admitted to a medical school should be holders of a baccalaureate degree, which is termed as their pre-medical course. Those who studied nursing as their pre-medical course had higher scores in the area of bodily pain (p = .046), whereas those who studied medical technology as their pre-medical course had higher scores in the area of social functioning (p = .008). No associations were observed between the HRQOL scores and age, civil status, and parents’ combined annual income (Table 4).
There was a striking association observed between the HRQOL scores and depression; those who were depressed had significantly lower scores in seven out of the eight domains, as compared with those without depression (p < .001). In terms of stress, those with moderate to major stress had lower scores in the areas of role limitations due to physical health, general health, and role limitations due to emotional problems (Table 4). Similar findings were observed in terms of perceived stress, presented in Table 5, where negative correlation coefficients in all areas of HRQOL except bodily pain and social functioning, indicated that higher stress levels were related to lower HRQOL scores.
Associations Between HRQOL and Numerical Variables.

Note. HRQOL = health-related quality of life; PF = physical functioning; RP = role-physical; BP = bodily pain; GH = general health; VT = vitality; SF = social functioning; RE = role-emotional; MH = mental health; ns = not significant.
As for burnout, emotional exhaustion and depersonalization were negatively correlated with HRQOL scores in six out of the eight areas. The relationships were stronger for emotional exhaustion as compared with depersonalization. There were slightly positive correlations between satisfaction with medicine and HRQOL in five out of the eight areas (Table 5).
Discussion
The results of this study showed that overall, medical students had an average to above average HRQOL. It also revealed that students had a higher HRQOL in the scales related to physical health, that is, physical functioning and bodily pain, but scored lower in scales related to mental health, that is, vitality and role limitations due to emotional problems. Depression, stress, and burnout were associated with lower scores in most of the domains of HRQOL, whereas sex, pre-medical course, academic performance, and year level were associated with fewer of the HRQOL domains.
The lowest scores were in those domains related to mental health. This means that medical students have a tendency to encounter problems with work or other daily activities as a result of emotional problems and that they may experience feelings of nervousness and depression (Ware, 2003). These are likely related to the nature of the medical school experience, which has been often described as stressful. Medical students have to undergo frequent periods of adjustment, which may affect them emotionally. For instance, first-year students have to adjust to medical school itself, which is more rigorous and intellectually challenging as compared with their pre-medical course. Students in third year have to adjust to clinically oriented courses, from the basic science courses of lower years, not to mention the issue of academic overload typical of third year. Students in fourth year have to adjust to clinical clerkship, wherein full-time clinical training in the hospital is an entirely different experience from teaching and learning in the classroom setting. Moreover, this study also showed that psychological conditions such as depression, stress, and burnout are inversely related to HRQOL scores.
There are other issues that might stress medical students. Although family members are generally supportive, due to the cultural norm of close family ties in the Philippines, they can also be a source of stress, especially for students who have family problems, or who are married and/or with children, who may be struggling to balance family life and medical school training. Financial problems can also be a source of stress, as medical education is expensive and scholarship grants for medical education are very limited in the Philippines.
The findings of the current study are consistent with those of Voltmer, Rosta, Aasland, and Spahn (2010) who, as a part of their article, studied the HRQOL of medical students in Germany and discovered that the students had lower scores in the domain of mental health as compared with physical health. The results are also in agreement with those of Dyrbye et al. (2007) who, also as a part of their article, determined the quality of life of medical students in the United States. Their students also had relatively low mental quality of life scores.
However, medical students are able to perform all types of physical activities, even the most vigorous, without limitations due to health, and that they do not experience pain or there are no limitations due to pain (Ware, 2003). A possible explanation for this might be that the great majority of medical students are apparently physically fit young adults, as attested by their annual medical-physical examinations. Students have to undergo these physical examinations together with basic laboratory tests prior to enrollment. Moreover, chronic diseases which may bring about pain and physical limitations are uncommon in this age group.
Our study also showed that males had significantly higher scores than females in the domains of general health and vitality. This means that males have a tendency to evaluate their personal health as excellent and that they always feel energetic, as compared with females. This is in keeping with the cultural norm in the Philippines where men are generally considered to be the stronger sex, thus men perceive themselves to be so. The present study also revealed that male medical students had significantly higher scores in the domain of role limitations due to emotional problems as compared with female medical students. A higher score means that there are less interferences with work or daily activities as a result of emotional problems. This is again consistent with the cultural norm in the Philippines where men are supposed to be less emotional than women. Thus, male medical students in general do not let emotions or emotional problems hinder their performance in their studies and training. These findings are similar to those of the study of Paro et al. (2010) that female students had lower HRQOL scores than males. Jamali et al. (2013) also established that male gender was significantly associated with higher HRQOL scores as compared with females.
Regarding the factors associated with HRQOL, our findings are similar to those of Paro et al. (2010) who found out that female medical students and those with depression had lower HRQOL scores. Dyrbye et al. (2007) likewise reported that burnout and depression were major factors that influenced medical students’ quality of life. In addition, Swami et al. (2007) observed that in Malaysia, life satisfaction, which is used interchangeably with quality of life, was inversely related to depression. Arslan, Ayranci, Unsal, and Arslantas (2009) also reported that in Turkey, the scores of the SF-36 scale were lower for those with depression as compared with those without depression.
However, the results of the current study differ from those of Naseem and Iqbal’s (2010) study. Among Pakistani medical students, physical functioning, general health perception, vitality, and social functioning for second-year students were significantly less than the other classes. In the present study, social functioning was highest among third-year students and lowest among fourth-year students. This is because students in the third year have already adjusted to life in medical school and have already established friendships among classmates. Thus, they are able to interact with each other and socialize on weekends. However, fourth-year students are in clinical clerkship wherein they spend most of their time in the hospital. There is little time for socialization with friends and after work they would rather rest and sleep in preparation for the next hospital duty the following day. This is similar to the findings of Paro et al. (2010) and Jamali et al. (2013) where students in the highest year level had lower HRQOL scores as compared with lower year levels.
It is interesting to note that 45 medical students (8.5%) had depression based on the BDI score. Further analysis of Item Number 9 on the BDI, which assesses suicidal thoughts, revealed that 54 students checked the response “I have thoughts of killing myself, but I would not carry them out”; 3 students responded that “I would like to kill myself”; and 2 students responded that “I would kill myself if I had the chance.” This has implications for counseling services in a medical school. Such services are available at our university’s Guidance Center, and the head of the center personally attends to medical students who seek consultation. However, very few medical students avail of these services, most probably due to lack of time owing to their heavy class schedule and busy hospital rotations.
The strength of this study is that it made use of well-established and validated data gathering instruments such as the SF-36, BDI, aMBI, PSS, and Holmes and Rahe Stress Scale. The use of such tools minimized information bias. This study also had a relatively high response rate, which could have minimized selection bias. To the best of our knowledge, this is the first study on the HRQOL of medical students in the Philippines.
However, this study also had certain limitations. As in other studies employing questionnaires, recall bias is a possibility. In determining the factors associated with HRQOL, confounding was not assessed as the main objective of the study was to describe the status of the medical students’ HRQOL. Furthermore, the present study only involved students from just one medical school in the Philippines. This limits the study’s generalizability. The results may not necessarily be extrapolated to students from other medical schools in the country or to those from other countries. It is important to bear in mind that medical schools vary in terms of the nature of their curricula, for instance, traditional versus problem-based learning, duration of the medical course, as well as school and hospital atmosphere and environment. Medical students from different schools may also vary according to sociodemographic characteristics such as age and sex distribution, and other personality characteristics. All these may influence their HRQOL.
In conclusion, medical students in our school are generally in a satisfactory state of functional health and well-being, but have a lower level of mental health as compared with physical health. Depression, stress, and burnout reduce the medical students’ state of health. The results of this study have implications for medical educators in our school. It could provide a basis for the development of student wellness programs and activities. It is imperative that counseling services and mentoring programs for medical students be strengthened and enhanced. Improving the well-being of future physicians will hopefully translate to better quality of care for the patients they are meant to serve.
Future research on the HRQOL of medical students is needed. This study may be replicated by other medical schools in the country. Further investigations could utilize a longitudinal design rather than a cross-sectional design to trace changes in the students’ health and well-being over time.
Footnotes
Appendix
Differences Between Non-Responders and Responders According to Sex.
| Sex | Non-responders | Responders | Total |
|---|---|---|---|
| Male | 40 | 205 | 245 |
| Female | 41 | 322 | 363 |
| Total | 81 | 527 | 608 |

Note. Fisher’s exact test p value = .10 (not significant).
Acknowledgements
The author would like to thank Carl Froilan D. Leochico, MD, for his invaluable assistance in data collection, data management, and data analysis; and to Joshua H. Gaboy, MD, and Rodel J. Banggiacan, MD, for their help with data management.
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author disclosed receipt of the following financial support for the research and/or authorship of this article: This study was funded through a University Research Grant (URG No.12.3.SoM.1) from Saint Louis University, Baguio City, Philippines.