
Abstract
A work environment that boosts nurses’ leadership skills, has adequate resources and staff and collegial nurse–physician relations, and allows nurses to participate in decision-making enhances patient care quality and nurses’ job satisfaction and performance. I used a cross-sectional design and the Practice Environment Scale of the Nursing Work Index among 519 nurses to assess the nursing practice environment in primary healthcare centers (PHCs) across the Kingdom of Saudi Arabia. Respondents’ views varied, and the general mean (2.45) showed that most nurses thought their work environment has a fair number of staff and resources. The general standard deviation (0.924) indicated that a significant variation exists between the composite score values, and there were no significant differences in the other factors. It was concluded that most PHCs have poor staff and resource adequacy, which shows the significant influence of nurses’ job satisfaction and performance on the quality of their work environment.
Saudi Arabia’s healthcare system is transforming owing to a rapidly growing population and the economic influence of Vision 2030 (Al Mutair, 2015). Notably, there is an acute shortage of nurses, and the healthcare system is endeavoring to address this issue while also adhering to Vision 2030. A stable nursing workforce can ensure the quality of care and improve patient satisfaction levels in Saudi Arabia’s hospitals and primary healthcare centers (PHCs). Saudi Arabia is adopting several measures to develop the nursing practice environment and ensure patient safety and staff welfare. It is focusing on achieving four key objectives concerning the nursing environment: transformational leadership, exemplary professional practice, structural empowerment, and new knowledge, innovations, and improvements (Al-Dossary, 2018). To achieve these goals in the healthcare system and those of Vision 2030, a healthy work environment that attracts nurses is required.
Currently, Saudi Arabia’s healthcare system is focusing on redesigning traditional management models to address nursing shortages stemming from a high staff turnover while also attempting to reduce costs and improve efficiency and results (Alkorashy & Al-Hothaly, 2022).
Literature Review
Studies have shown that a healthy nursing work environment is satisfying, empowering, and safe (Wei et al., 2018). Such work environments contribute to increasing job satisfaction, performance of nurses, and the quality of patient care (Moisoglou et al., 2020). Notably, the quality of care provided to patients is directly linked to the quality of the nurse’s working environment (Al-Dossary, 2022). Several studies have emphasized the need to enhance the quality of care provided by nursing professionals to improve patient safety. For example, it has been reported that improving quality of care is necessary to overcome shortcomings that lead to negative patient experiences in Saudi Arabia (Alkorashy & Al-Hothaly, 2022). This finding is also supported by other studies that have asserted that improving nurses’ working environment is an effective strategy for enhancing patient care quality. However, barriers such as burnout and unhealthy work environments can impede accomplishing this goal (L. Y. Kim et al., 2020). Studies have particularly shown that the current nursing shortage is jeopardizing patient care, safety, and the quality of patient care (Alkorashy & Al-Hothaly, 2022). They have also revealed that inadequate staffing and resources are linked to emotional exhaustion and low job satisfaction among nurses (Alharbi et al., 2020). These findings confirm that a hostile work environment leads to many nurses leaving the profession in Saudi Arabia (Alharbi et al., 2020). Therefore, Saudi Arabia’s Ministry of Health (MOH) must prioritize improving nurses’ work environment to increase patient safety and satisfaction.
Other studies have suggested that investing in nursing leadership training and material and human resources is crucial to enhancing nurses’ work environment. One study suggested promoting nursing leadership training to prevent adverse events (Alsufyani et al., 2021). Another study asserted that engaging nurses in the management of healthcare centers improves patient outcomes because nurses feel a part of the organization, which increases their job satisfaction (Cristina Gasparino et al., 2021).
This study also recommended that interventions by nurse managers in primary health care should focus on improving the identified weaknesses to improve the quality of care and health outcomes. Therefore, a shared professional practice environment that integrates governance may serve as a valuable strategy for healthcare institutions to encourage optimum outcomes for patients and nursing professionals.
Finally, some studies have revealed different institutional, organizational, individual, and patient level factors that act as facilitators for Nurses and barriers for Registered Nurses (RNs). For example, Abou Malham et al. (2020) found that these factors include facilities and staffing arrangements, which equate to the supply and availability of human resources. Other factors include politics and legislation, interprofessional fellowship, and organizational policy support (leadership and strategies to support nurses’ practice change, professional boundaries, patient perceptions, knowledge, and capabilities). Therefore, Brofidi et al. (2018) recommended that hospital administration should focus on developing a work environment that supports continuous education and nurses’ participation through continual evaluation procedures and improving human resources management. Thus, nurses’ participation in hospital affairs and nursing foundations for quality of care are critical contributors to a healthy nursing work environment.
Thus, assessing nurses’ work environments is integral to obtaining baseline data that will help the MOH formulate policies to improve nurses’ working conditions. This study examines the work environment of nurses working in Saudi Arabia’s PHCs by using the most common instrument to measure the nursing practice environment: the Practice Environment Scale of the Nursing Work Index (PES-NWI). This scale measures “factors that enhance or attenuate a nurse’s ability to practice nursing skillfully and deliver high quality care” (Lake, 2002; Swiger et al., 2017).
Methods
Study Design and Sample
A cross-sectional design was used to assess the quality of the nursing practice environment from the perspective of nurses working in PHCs across the Kingdom of Saudi Arabia using the PES-NWI (Alkorashy & Al-Hothaly, 2022). In order to collect the data used in the study, convenience sampling was employed. Nurses were selected based on their easy reachability across the country. I received 519 (83.98%) fully answered questionnaires, and they were considered fit for analysis.
Ethical approval (approval number 113) was obtained from the Institutional Review Board of the MOH, where the study was conducted. A consent form was distributed along with the electronic survey stating that filling out the survey would be considered informed consent. No identifiable data were collected. Confidentiality of data and participants’ privacy were maintained, and subjects’ right to withdraw from the study was also ensured.
Instrument
The PES-NWI comprises 31 items across five subscales: (1) staffing and resource adequacy (SRA), (2) collegial nurse–physician relations (CNPR), (3) nurse manager ability, leadership, and support of nurses (NMALS), (4) nurse participation in hospital affairs (NPHA), and (5) nursing foundations for quality of care (NFQC). A 4-point Likert scale ranging from 1 (strongly disagree) to 4 (strongly agree) was used to identify the subscale(s) that support nurses’ abilities to deliver a high level of patient care. PES-NWI scores above the midpoint of 2.5 indicated a favorable practice environment for nurses, while scores below the midpoint indicated an unfavorable practice environment (Swiger et al., 2017). The five subscales provide insight into the key structures of the nursing practice environment (Lake, 2002; Swiger et al., 2017). The Cronbach’s alpha of the entire questionnaire (.962) indicated very good reliability. The correlation coefficients of all items were .735, and the correlation coefficients were significant at the .05 level, as shown in Table 1.
Cronbach’s Alpha of the Constructs.

Statistical Analysis
The data were coded and entered in the Statistical Package of Social Science (SPSS) version 23. Descriptive statistics were generated for all variables to understand the nature of the data in this study. Pearson correlations and polyserial correlations were computed to examine inter-correlations among the subscales of PES-NWI (SRA, CNPR, NMALS, NPHA, and NFQC).
For each item, respondents could rate strongly agree (4), agree (3), disagree (2), or strongly disagree (1). The scoring of the PES-NWI was done by creating categorical references for poor, mixed, and favorable practice environments, as suggested by researcher (Lake, 2002; Swiger et al., 2017). A score more than 2.5 on all or four of the five subscales indicated a favorable environment. A score more than 2.5 on two or three of the five subscales indicated a mixed environment. Finally, a score more than 2.5 on one or none of the five subscales indicated an unfavorable environment.
The significance level of each independent variable depends on its correlation with another independent variable (Field, 2005). The correlation coefficient must be a value greater than zero. Moreover, it is necessary to prove that the variable contributes in a statistically significant manner in predicting factors in a population under study (Field, 2005). Correlation matrices were plotted to display the correlation coefficient (r) of each variable in relation to another, as shown in Table 2.
Sample Correlation Matrix of Staffing and Resource Adequacy.

Results and Discussion
Of the respondents, 410 (79%) were women, and 109 (21%) were men, showing that most nurses in Saudi Arabia are women. A total of 270 (52%) participants had bachelor’s degree, 190 (35.6%) had a diploma, while only 59 (11%) had a master’s degree, as shown in Table 3.
Distribution of Respondents Based on Demographic Variables.

Staffing and Resource Adequacy
In a nursing environment, staffing adequacy is when the nurse-to-patient ratio does not overwork any of the nurses or put patients in jeopardy (Griffiths et al., 2018). It simply means to have enough nurses. Resource adequacy is when a medical institution has everything it needs to perform daily activities, such as enough time, supplies, and patient beds (Cimiotti et al., 2014). The findings and debates on personnel and resource sufficiency show that Saudi Arabian PHCs confront significant issues. Many nurses feel they need more time for care talks, and the low mean score for RN staffing indicates a resource deficit. These results support L. Y. Kim et al. (2020), which found that staffing affects nurses’ work satisfaction. These resource shortages must be addressed to improve the work environment and patient care. The overall mean of this construct was 2.45, and the standard deviation (SD) was 0.924, as shown in Table 4.
Mean and Standard Deviation of the Items and the Construct of Staffing and Resource Adequacy.

The mean score shows that, on average, most items had a score of 2. This indicates that most nurses believed that their work environment has a fair number of staff and resources. The SD indicates that a great variation existed between the composite score values, suggesting that respondents’ views varied.
The highest mean was of the variable “Enough staff to get the work done.” This variable had a mean score of 2.51 and a mode of 3.271 (52%). Moreover, it recorded a score of 3 or 4, scores above a fair score; thus, most respondents viewed their work environment as being adequately staffed with nurses. Staffing adequacy mainly depends on the number of patients admitted, the number of unit beds, the case mix index, and patient acuity (Mark et al., 2002). Therefore, I concluded that most PHCs in Saudi Arabia employ sufficient staff in relation to the number of patients admitted and the services to be provided.
The variable “Enough time and opportunity to discuss patient, client, or resident care problems with other nurses” had a mean score of 2.46 and a mode of 2.53%. Most nurses (274) scored it as 1 or 2, indicating that most nurses do not have adequate time to discuss the provision of care with other nurses. That is, most PHCs do not provide their employees with enough time to discuss care provision.
“Adequate support services allow me to spend time with my patients” had a mean score of 2.44 and a mode of 2. Notably, 279 nurses (54%) reported that they do not get adequate support services. This is one of the main factors limiting the time nurses get to spend with their patients.
“Enough RNs on staff to provide quality patient, client, or resident care” had a mean score of 2.40 and mode of 2. Two hundred and ninety (56%) nurses scored this item 1 or 2 and it had the lowest mean score, indicating that this is the biggest issue concerning staffing and resource adequacy in PHCs. It can be inferred that most medical institutions in Saudi Arabia do not employ an adequate number of nurses, which leads to subpar quality of services.
In conclusion, most PHCs have poor staffing and resource adequacy. L. Y. Kim et al. (2020) assessed the association between job satisfaction and the components of nurses’ working environment. They found that SRA is strongly linked to nurses’ emotional exhaustion, which, in turn, affects their job satisfaction.
Collegial Nurse–Physician Relations
Schmalenberg and Kramer (2009) described collegial nurse–physician relations as nurses collaborating with physicians to ensure that they deliver good quality patient-care services. This relationship is mainly built by the communication between the two parties (Schmalenberg & Kramer, 2009). The mean of this construct was 2.48 and the SD 0.937, as shown in Table 5.
Mean and Standard Deviation of the Items and the Construct of Collegial Nurse–Physician Relations.

The overall mean shows that, on average, nurses gave a score of two to the items of this construct. This implies that nurse–physician relations are not considerably collegial. The SD shows that a great variation exists between the composite score values, indicating that respondents held different views.
“Collaboration between nurses and doctors” had a mean score of 2.47 and a mode of 2. A total of 251 (46%) nurses scored it 3 or 4, and this variable received the highest percentage of good scores in the construct CNPR. Most nurses disagreed that nurses and physicians collaborated. Studies have shown that optimum patient experience is not provided in hospital where doctors do not interact well with the nurses (Friese, 2005). Based on these statistics, most patients in Saudi Arabia do not get good quality care owing to poor collegial relations between nurses and physicians.
“Physician and nurses have good working relationships” had a mean score of 2.50 and a mode of 2, indicating that most nurses did not have a good relationship with doctors. Of these nurses, 53% (278) disagreed with having a good relationship with physicians. This item is correlated with “Collaboration between nurses and doctors” (0.68), indicating that one of the main reasons behind a poor working relationship is the lack of collaboration between nurses and doctors.
“A lot of teamwork between nurses and doctors” had a mean score of 2.45 and a mode of 2. It had the lowest mean score in this construct, demonstrating that poor teamwork is the main cause of poor collegial nurse–physician relationships. More than half of the nurses (54%) reported having poor teamwork with physicians in their PHC.
Overall, collegial nurse-physician interactions in Saudi Arabian PHCs, the research finds tension. Poor cooperation, working relationships, and teamwork may impair healthcare delivery (Y.-B. Kim & Lee, 2023).
It can be inferred that all of its variables contribute to the lack of collegial nurse–doctor relationships in Saudi Arabia’s PHCs because most nurses are women and most physicians are men. This supports Schmalenberg and Kramer’s (2009) nurse-physician teamwork emphasis. To improve patient outcomes and work harmony, these ties should be prioritized
Nurse Manager Ability, Leadership, and Support of Nurses
Al-Dossary (2018) and Alsufyani et al. (2021) showed that investing in nursing leadership is crucial to improving the work environment’s safety for nurses. Another study focused on how management, supervision, and consultancy affect nurses’ working environment (Cristina Gasparino et al., 2021). The mean of this construct was 2.44 and the SD 0.898, as shown in Table 6.
Mean and Standard Deviation of the Items and the Construct of Nurse Manager Ability, Leadership, and Support of Nurses.
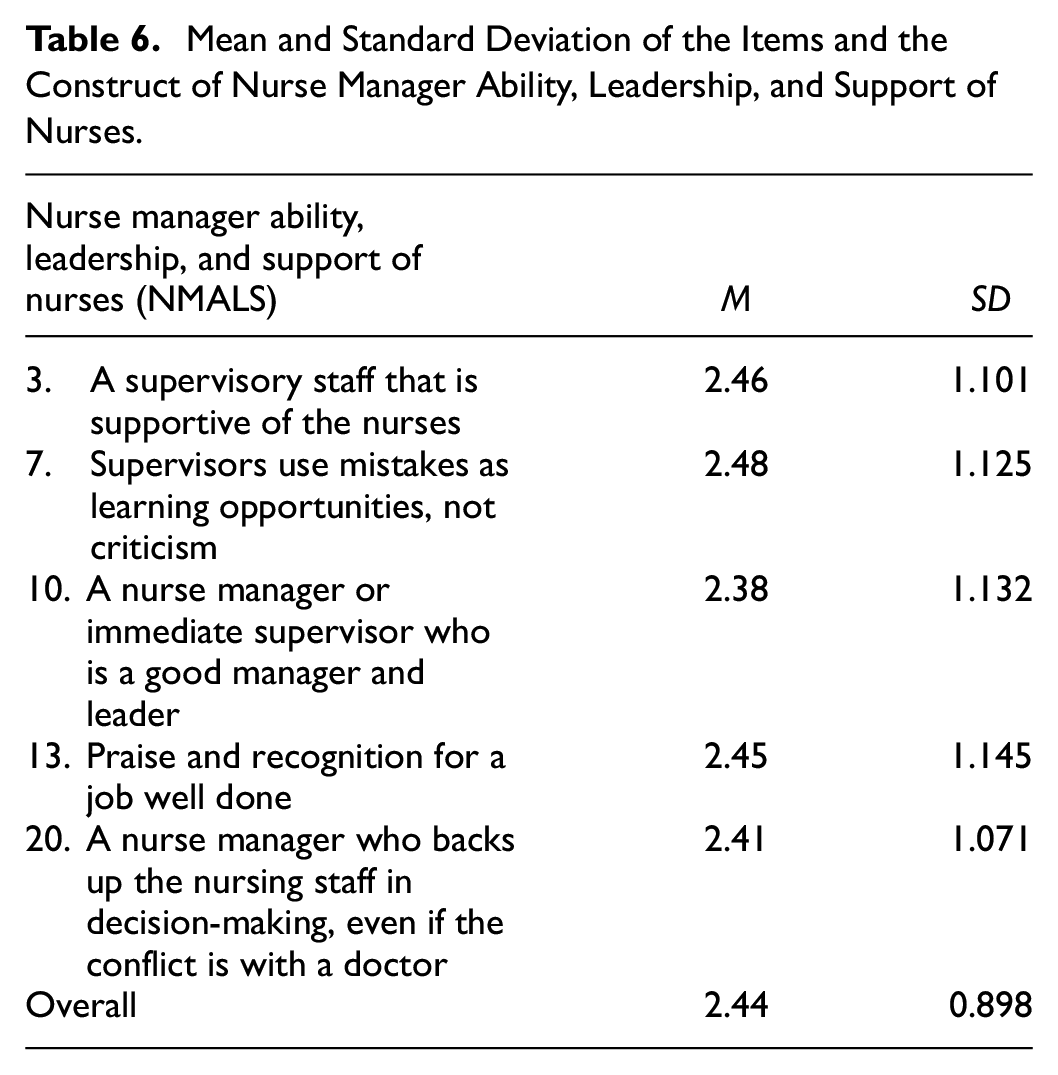
“Supervisors use mistakes as learning opportunities, not criticism” had a mean score of 2.48. This item had the most positive responses in this construct. However, most respondents (264 or 51%) said that their supervisors criticized them for their mistakes.
“A supervisory staff that is supportive of the nurses” had an average score of 2.46, and 251 nurses disagreed with this item. This indicates that most supervisors in PHCs do not support their nurses.
“A nurse manager who backs up the nursing staff in decision making, even if the conflict is with a doctor” had a mean score of 2.41. A little more than half of the nurses (51%) did not view their manager as someone who always supports them, especially when the conflict is with a doctor.
“A nurse manager or immediate supervisor who is a good manager and leader” had the lowest mean score (2.38), indicating that this is the main cause of poor NMALS.
“A supervisory staff that is supportive of the nurses” and “A nurse manager or immediate supervisor who is a good manager and leader” had the highest correlation with a correlation coefficient of .6647. The items in this construct had very similar scores; it shows that one aspect contributes to the poor performance of another. Overall, nurse manager skills, leadership, and support indicate a need for PHC management improvements. The low mean score for nurse managers supporting their employees in decision-making and that many nurses see their supervisors as critical rather than helpful indicate poor leadership. Al-Dossary (2018) and Alsufyani et al. (2021) stressed the importance of nursing leadership in workplace safety.
Nurse Participation in Hospital Affairs
A good nurse should be involved in the affairs of the hospital (Sellman & Snelling, 2016). However, a related study showed that this might not be a decision nurses could make since some health centers have policies that do not support nurse participation. The mean score of this construct was 2.40 and the SD 0.866. The mean score shows that, on average, the respondents gave a score of 2 to the items in this construct, as shown in Table 7.
Mean and Standard Deviation of the Items and the Construct of Nurse Participation in Hospital Affairs.

The correlation matrix of NPHA showed that all variables are positively and statistically correlated with each other.
“Nurses are involved in the internal governance of the hospital” and “Nurses have the opportunity to serve on hospital and nursing committees” had the highest correlation coefficient (r) (.7424) among the coefficient of the items in the other four constructs. This means that many PHCs in Saudi Arabia have policies that support these two aspects. The mean of these two items was 2.277 and 2.380, respectively, and they both had a mode of 2. However, stronger leadership and support systems may improve workplace morale (Sellman & Snelling, 2016). While nurse engagement in hospital affairs may be improved, many Saudi Arabian PHCs favor nurse involvement in governance and committees. However, increasing nurses’ involvement in hospital matters may enhance decision-making and patient care.
Nursing Foundations for Quality of Care
Rigolosi (2012) asserted that most PHCs lack nursing foundations and highlighted their importance in healthcare organizations. I analyzed NFQC to check whether this assertion is true. The mean of NFQC was 2.41 and the SD 0.850. The mean shows that, on average, the respondents gave a score of two to the items in this construct. The high SD shows that there was a great variation in the composite score values, as shown in Table 8.
Mean and Standard Deviation of the Items and the Construct of Nurse Foundations for Quality of Care.

The correlation matrix of NFQC showed that all variables are positively and statistically correlated with each other. “An active quality improvement program” and “Written, up-to-date nursing care plans for all patients/clients/residents” had the highest correlation coefficient (r) (.6950). Analyzing the mean of these two items confirms that the similar scores were either high or low. The mean of these two items was 2.505 and 2.478, respectively, and they both had a mode of 2. Thus, most respondents gave a score of two, indicating that most nurses work in an environment where “physicians and nurses have good working relationships” and there is “collaboration between nurses and doctors.” To further analyze the correlation, I plotted a scatter chart and inserted a trend line (Figure 1) to see the trend in the least and most correlated variables. The more correlated values show a line of higher gradient, indicating a growth in the scores of the two factors. This means that nurses’ working environment is better when both factors are considered. Finally, the research identified a fair nursing foundation for excellent treatment in Saudi Arabian PHCs, with a mean score of 2.41. An active quality improvement program and current nurse care plans are linked. In healthcare literature, quality improvement and documentation are stressed (Rigolosi, 2012). However, this part may be improved.
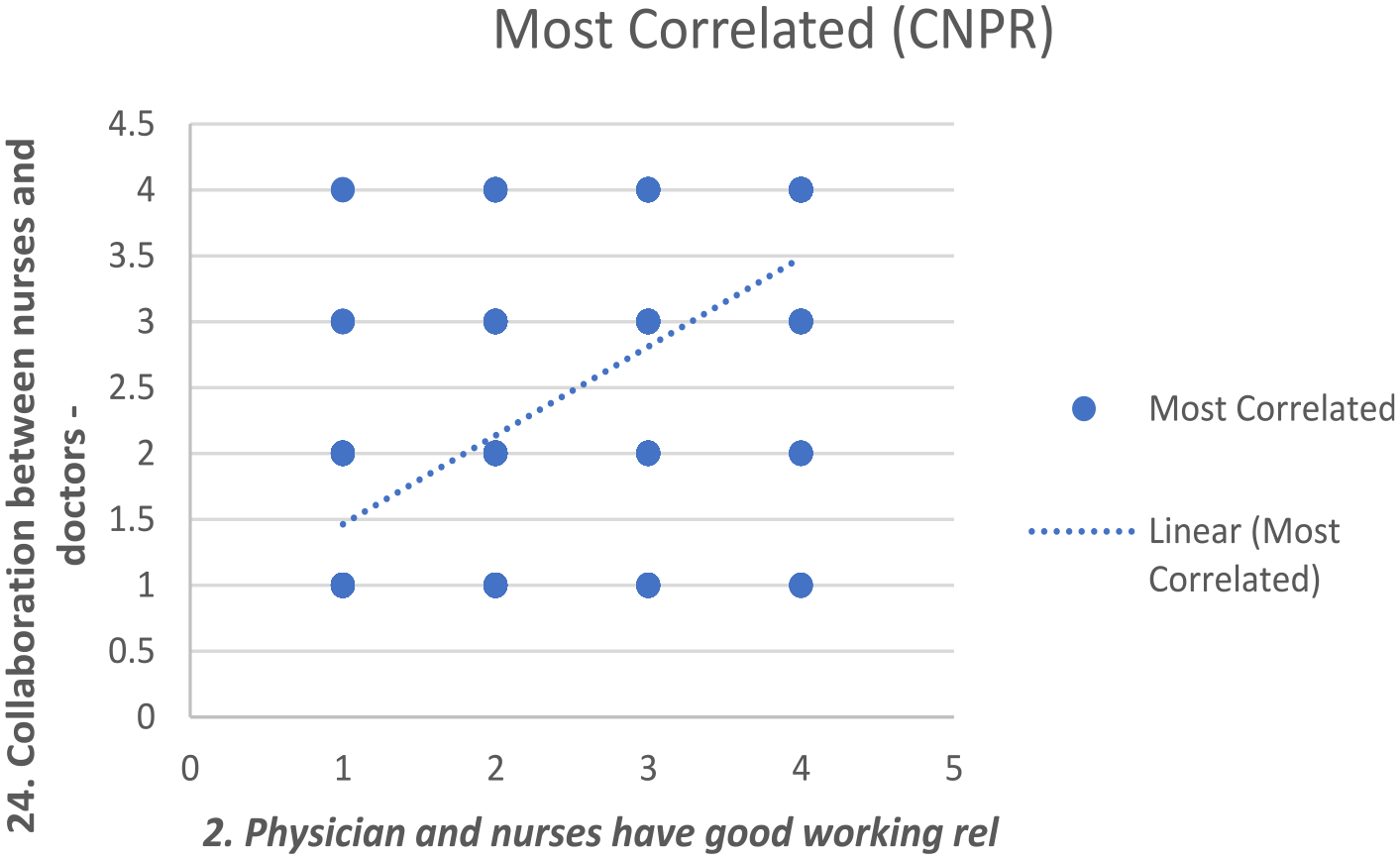
Scatter plot and trendline.
The composite score of the PES-NWI was less than 2.5 (mean = 2.4, SD = 0.75), as shown in Table 9. This indicates that most PHCs in Saudi Arabia have an unfavorable nursing practice environment.
Mean and Standard Deviation of the Subscales of the PES-NWI and the Composite Score.
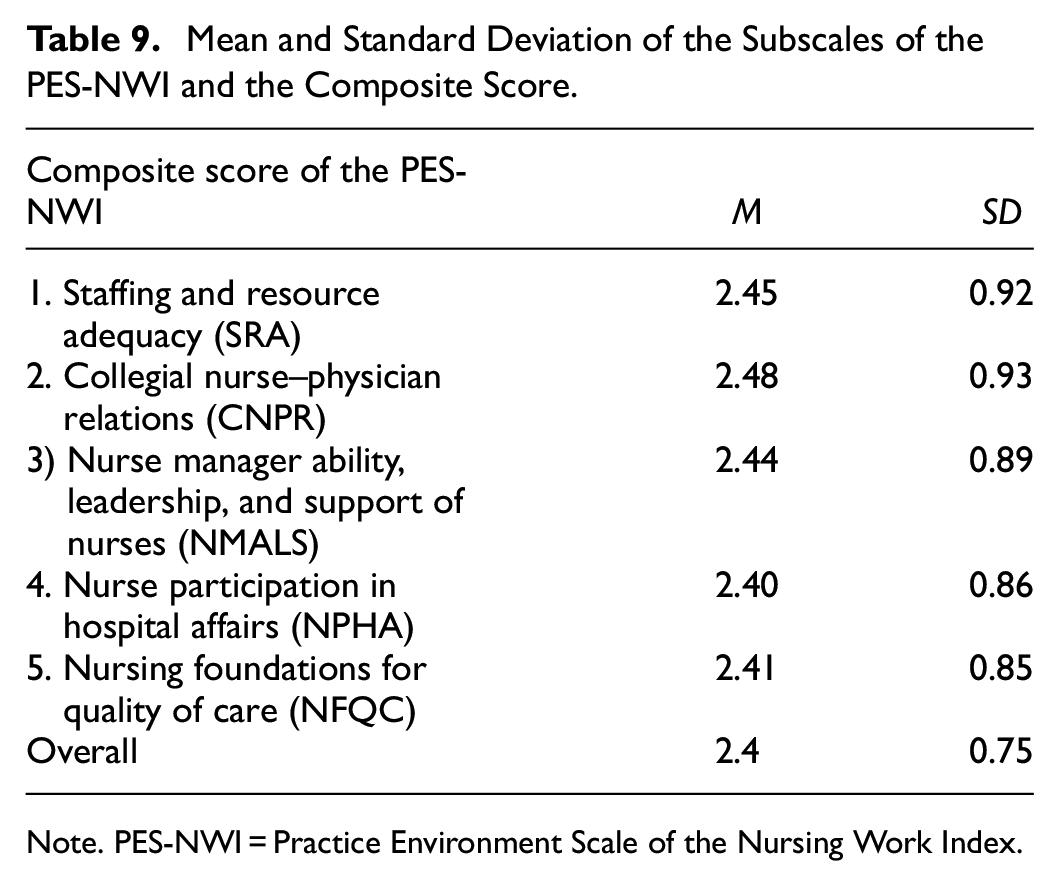
Note. PES-NWI = Practice Environment Scale of the Nursing Work Index.
This research illuminates numerous crucial elements of Saudi Arabian PHC work environments. Fair circumstances include nursing foundations for treatment quality, but staffing, resource sufficiency, nurse-physician interactions, nurse administration, and nurse engagement in hospital affairs are difficult (Y.-B. Kim & Lee, 2023). These results and previous research emphasize the need for focused interventions to improve the work environment, benefitting healthcare personnel and patients. Resolving these issues is necessary to improve Saudi Arabian PHCs' work environments.
Conclusion
Improvement in nurses’ working environment contributes to better outcomes for not only patients but also healthcare centers and nursing professionals (Alsufyani et al., 2021). Mugenda and Mugenda (2009) state that in correlation analyses, it is important to compare sample results with opposite ones to measure the magnitude of influence. So as to analyze the correlation further, a scatter chart was plotted and a trend line inserted to show the trend in the least and most correlated variables. The more correlated values show a line of higher gradient indicating growth in the scores of the two factors. This shows that when both factors are considered, the nurses’ working environment is better.
The initial analysis was on the first construct (SRA), and it acted as a benchmark for analyzing the data in the other categories. Armstrong (1995) explains that all assumptions to be used should be proved using at least one group when one is working with different groups of similar data. The other categories also showed similar results where all the variables were positively correlated. This means that increasing one variable in a construct would increase all other variables in the construct. This shows that the work environment greatly influences nurses’ work. Based on the results of this study, all factors (variables) in one aspect (construct) of nurses’ work environment have a positive influence on each other. The strength of one aspect of an organization will positively affect the other aspects and increase nursing productivity if PHCs in Saudi Arabia have adequate staff and resources to hire and retain nurses. The conclusion to be drawn from this is that the quality of a PHC’s services can be improved by addressing this issue.
The main limitation of this study is its cross-sectional design. Using this design is subject to the incidence-prevalence bias, also known as the Neyman bias, which might influence the findings. Another limitation is that it does not investigate any external factors that can impact nursing performance; all the factors of PES-NWI were internal factors. External factors not included in a certain construct may have a negative correlation with a variable, but this was not analyzed.
Relevance for Clinical Practice
This study can benefit decision-makers and nursing leaders in healthcare centers in different ways. First, it shows the reality of the nursing practice environment in Saudi Arabia’s PHCs. Second, it shows the importance of improving nurses’ performance and increasing their medical knowledge. The results of this study can benefit nursing researchers because they extend the knowledge on different areas of nurses’ performance: caregiving, administration, clinical research, teaching, and counseling/advisory services. The results may also benefit clients because they show the most important factors that affect the nursing practice environment, such as participation in decision-making, the relationship between healthcare providers and managers, and the development of professional communication.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The author expresses her gratitude to Princess Nourah bint Abdulrahman University Researchers Supporting Project number (PNURSP2023R347), Princess Nourah bint Adulrahman Univerity, Riyadh, Saudi Arabia.